
Medical Oncologist focused on GI & Endocrine Malignances. Vall Hebron University Hospital. Vall Hebron Institute of Oncology (VHIO). Teknon Cancer Institute.
Joined May 2017
- Tweets 3,983
- Following 301
- Followers 2,655
- Likes 8,556
311 Photos and videos











Jaume Capdevila retweeted

Jun 12
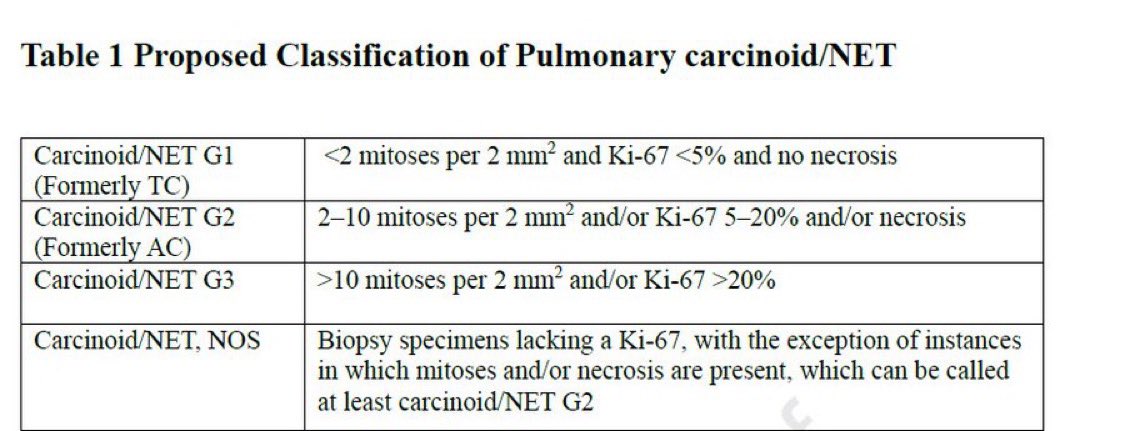
🫁 Actualización clasificación de TNE pulmonares (IASLC)
🔹 Incorpora Ki-67 como criterio diagnóstico
🔹 Reconoce NET G3 pulmonar
🔹 Transición de “carcinoide” hacia “NET”
🔹 Integra de nuevos conocimientos moleculares
🎯 Más precisión diagnóstica y mejor estratificación
🔗 doi.org/10.1016/j.jtho.2026.…
5
10
345
Jaume Capdevila retweeted
Jun 10
Save the date!
📅 25 de junio | Madrid
🔬 Actualización práctica sobre ZANOSAR® en tumores neuroendocrinos
👥 @GCarboneroLab , @JHernando3 y @DrAngelaLamarca
🤝 Con nuestro aval científico @GrupoGetne

4
7
506
Jaume Capdevila retweeted

Jun 10
See a new #neuroendocrinetumors activity via @PeerView @Ja_Capdevila #MedEd lrn.peerview.com/150211587_1…
1
2
112

#Neuroendocrine carcinoma (NEC) care is advancing. Learn how emerging evidence around DLL3-directed therapies and DLL3/CD3 BiTEs may help shape precision-driven treatment strategies and improve patient outcomes: bit.ly/40m8aY9
#Oncology #MedEd @Ja_Capdevila
4
7
185
Jaume Capdevila retweeted

Jun 8
The RAS revolution continues!
Tango Therapeutics' new results date back to the discovery of a synthetic lethal interaction, in 2016: PRMT5 inhibition selectively kills cancer cells deficient in MTAP — about 40% of pancreatic cancer — while ~sparing normal cells
This mechanism itself is probably independent of RAS, but given RAS inhibition is the likely future foundation of therapy, Tango's PRMT5 inhibitor, Vopimetostat, was tested in combination with RevMed's RAS inhibitor, Daraxonrasib — in MTAP-deficient pancreatic cancer
Today's data come from a small number of patients, but the 6-month progression-free survival was 90% (compared, cross-trial, with Daraxonrasib alone, ~56%)

June 2026 is the biggest month in drug development in PDAC ever in human history. Any objection?
5
48
206
32,410
Jaume Capdevila retweeted

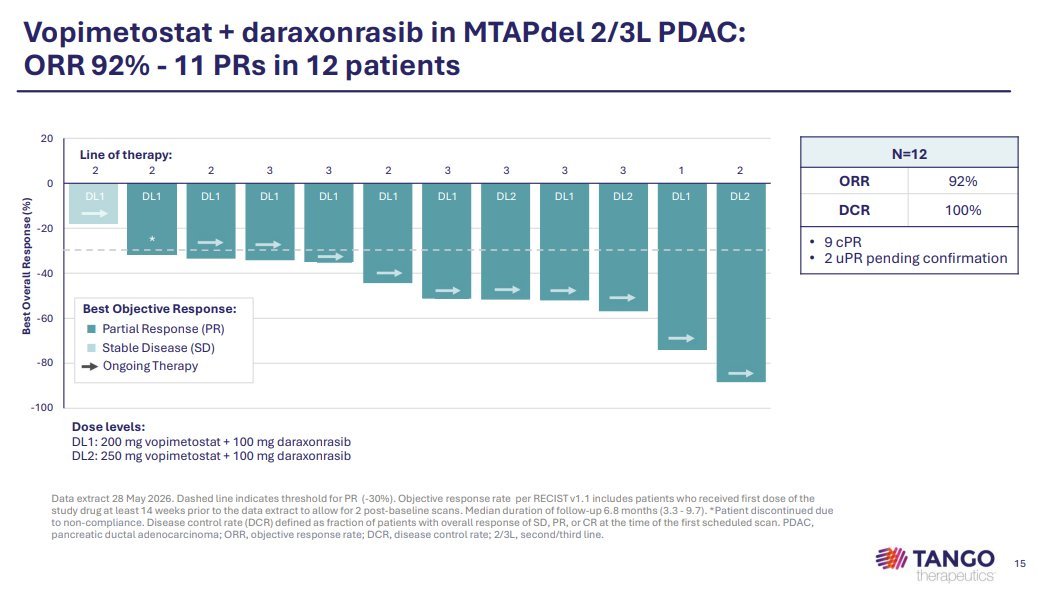
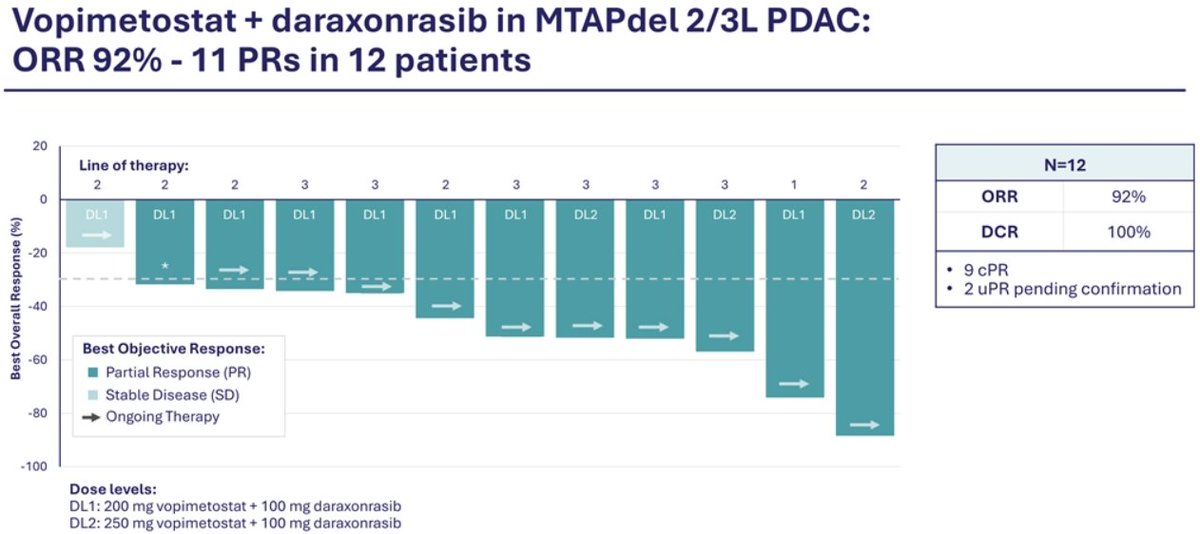
Last year, we reported that KRAS PRMT5 is synergistic in MTAP-null PDAC (doi.org/10.1158/0008-5472.CA…). Today, the first clinical data for a KRAS/PRMT5 combination was reported, with an incredible 92% ORR.
RAS inhibitors are the present, but combinations are the future!!
$TNGX $RVMD
24 Jul 2025

Happy to have contributed to this new work from @KathleenMulvan4 and @TheSellersLab, showing that KRAS and PRMT5 inhibitors synergy, out now in Cancer Research. KRAS/PRMT5 combos ($RVMD/$TNGX) are now in clinical trials, and results couldn't come sooner!
doi.org/10.1158/0008-5472.CA…
2
42
149
35,534
Jaume Capdevila retweeted

Jun 5
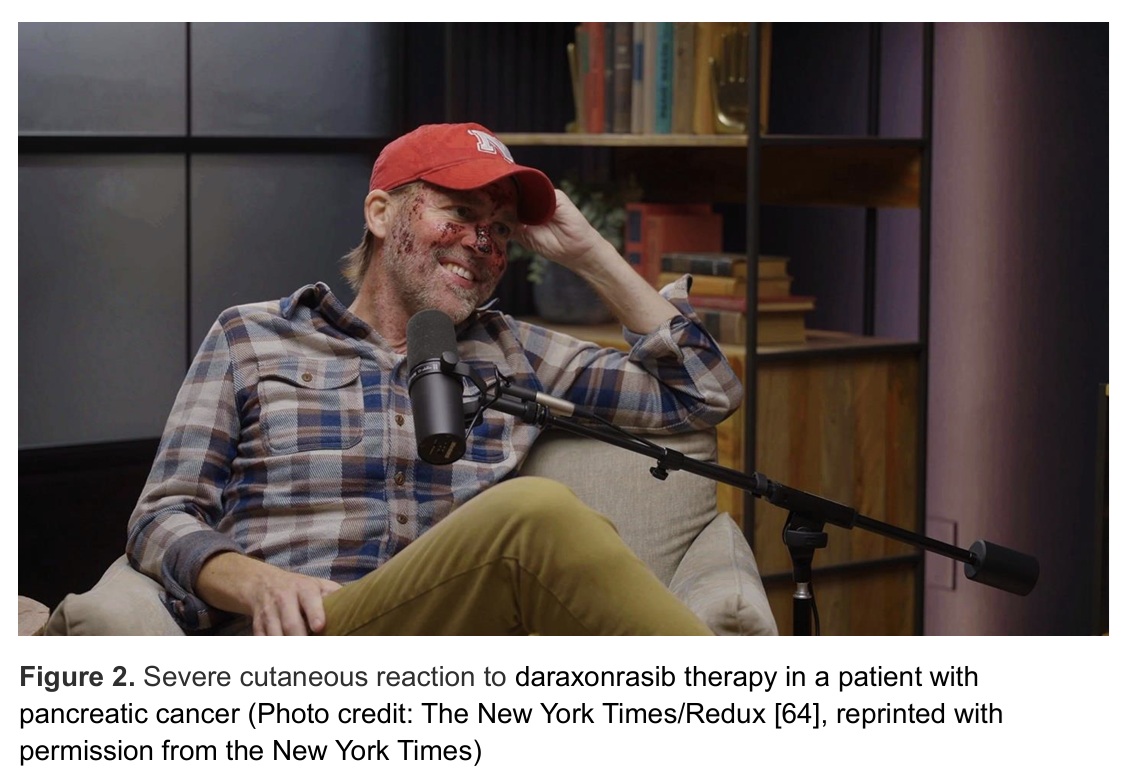
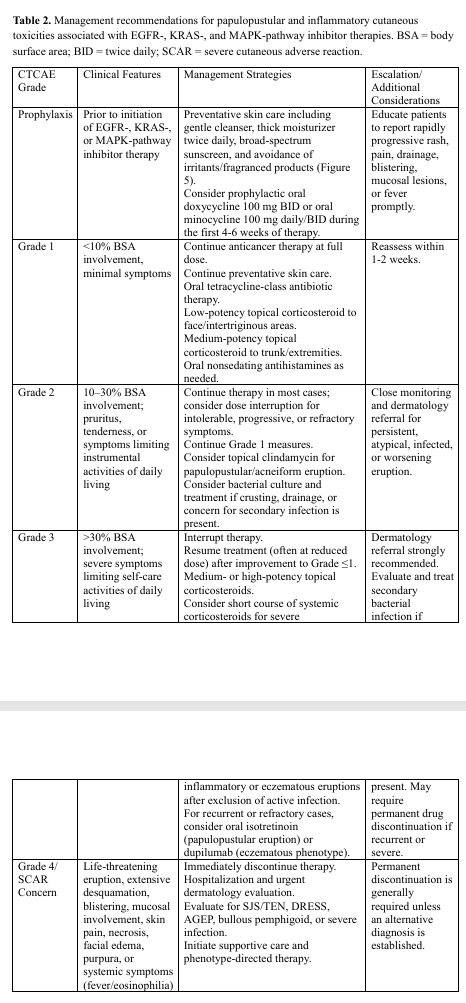
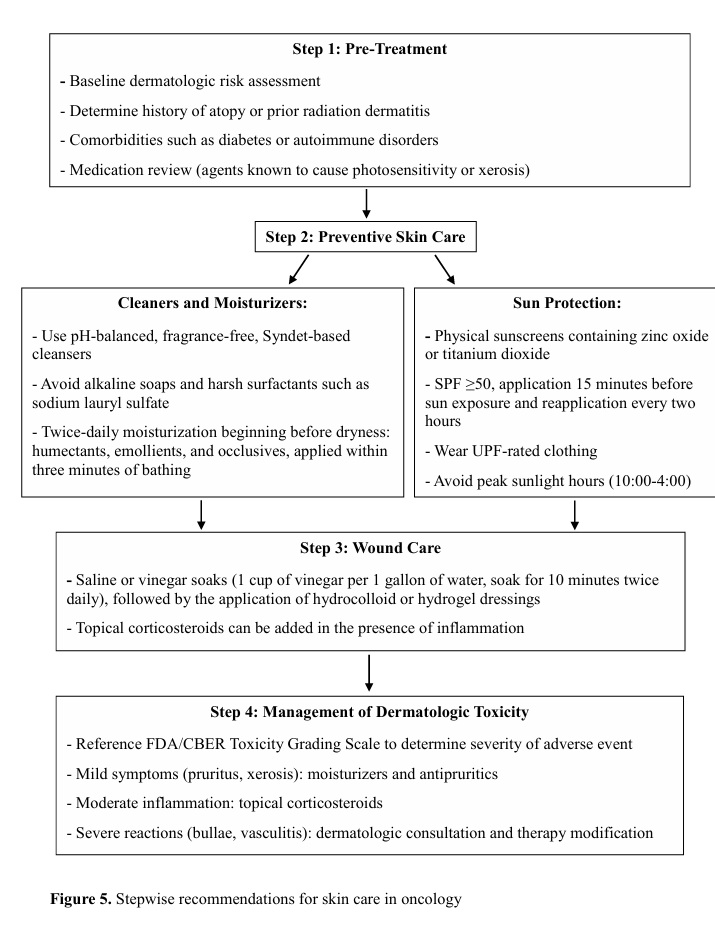
Daraxonrasib #PancreaticCancer data is a major step, but skin toxicity limits dosing.
Timely 4-step algorithm in @OncJournal protects patient QoL & treatment continuity.
academic.oup.com/oncolo/adva…
#OncoTwitter #PancreaticCancer #Oncology #SupportiveCare
ALT https://academic.oup.com/oncolo/advance-article/doi/10.1093/oncolo/oyag194/8699602
4
22
40
4,737
Jaume Capdevila retweeted
Jun 2
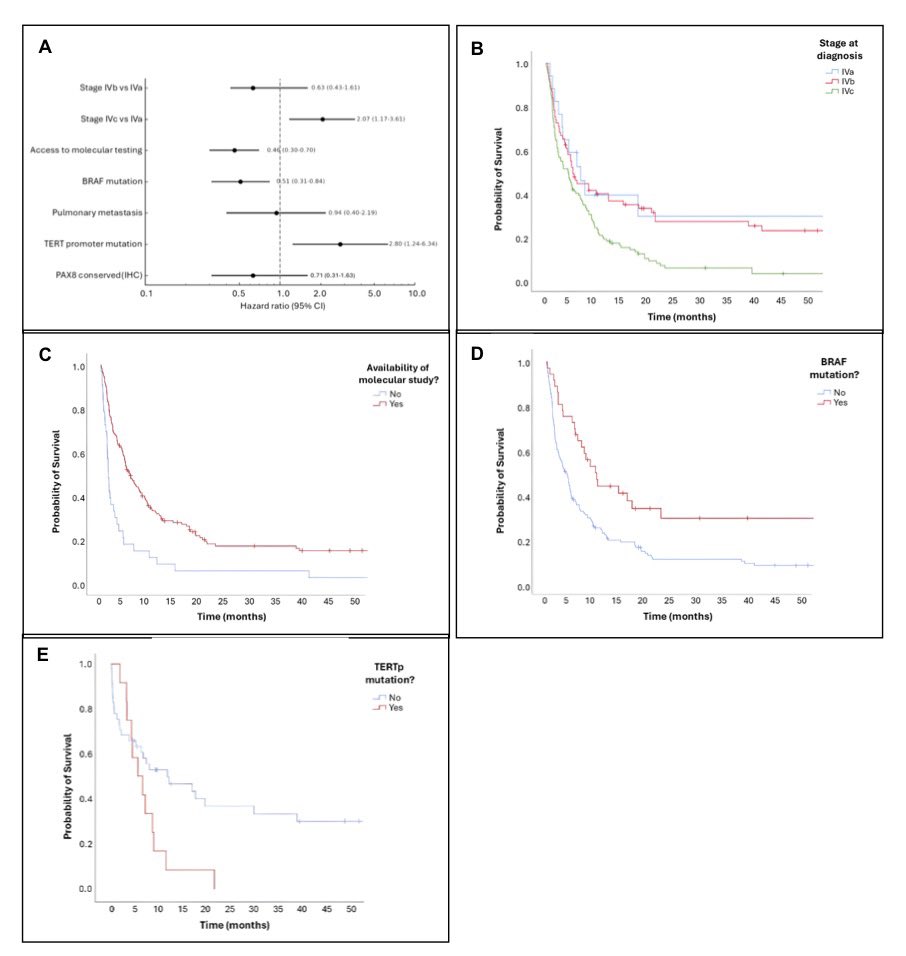
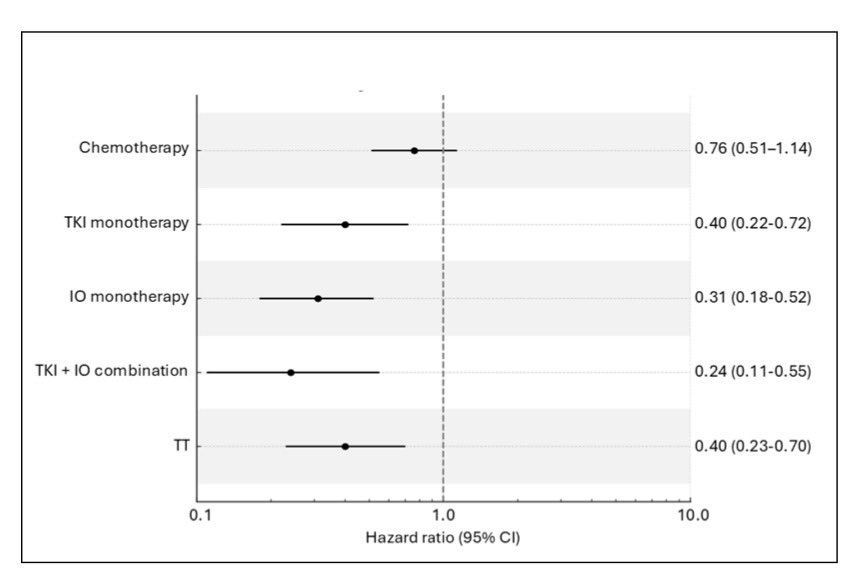
🧬 REGETNE-tiroides: RWE en CAT (n=214)
📈 mOS: 4.5 meses
🧪 Perfil molecular: mejor SG
🧪 BRAF V600E: mejor pronóstico
🧪 TERTp: peor pronóstico
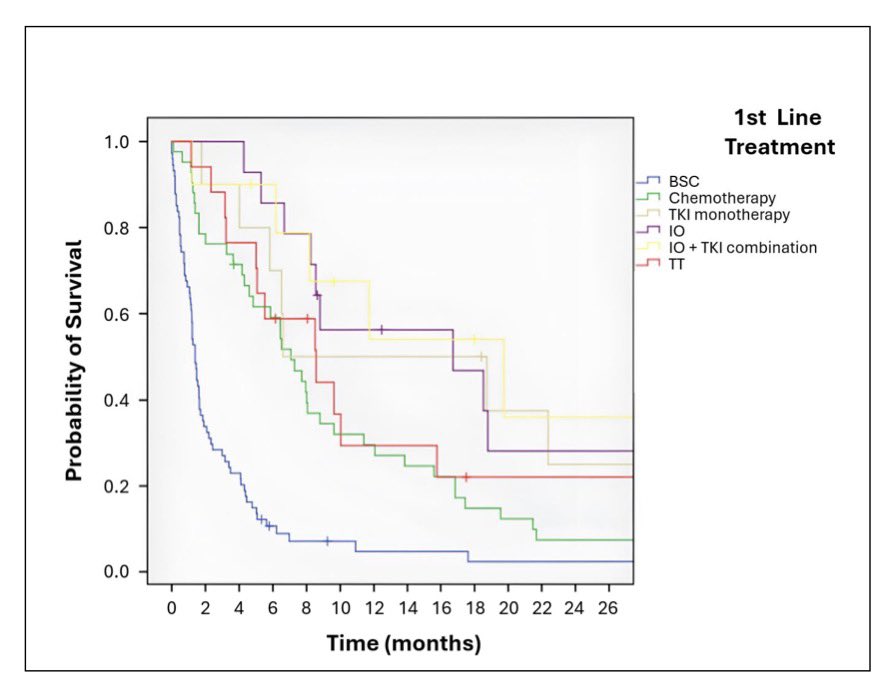
🎯 IO, TKI, IO TKI y terapias dirigidas: mayor supervivencia.
⚠️ Tratamiento local: impacto pronóstico, incluso en enfermedad M1
🔗 doi.org/10.1093/oncolo/oyag1…
9
11
1,749
Jaume Capdevila retweeted

Honored to have participated in the Revolution RAS-302 clinical trial that demonstrated 60% overall survival for patients who received the KRAS on inhibitor #Daraxonrasib compared to chemotherapy.
Our team @panoncology participated in this practice changing clinical trial in 🇵🇷 Puerto Rico. We are grateful to @RevMedicines and their leaders, scientists Dr Jan Smith, Dr. Wang, Dr. Salman, and oncologists Miguel Colon Donate, Karina Arocho, Luis Velazquez, Rafael Perez Casellas, Santa Merle, Radiologist Dr. Rafael Vicens and All PanOncology team members. Thank you to our partners Doctor’s Center Hospital Orlando Health and IGM Oncologic Hospital in 🇵🇷
We are privileged to have the trust of our patients, their, families and our colleagues who work together and support clinical trials to advance the science and cure cancer #RAS302 #ClinicalTrials #ASCO26 #PancreasCancer

4
18
87
7,549
Jaume Capdevila retweeted

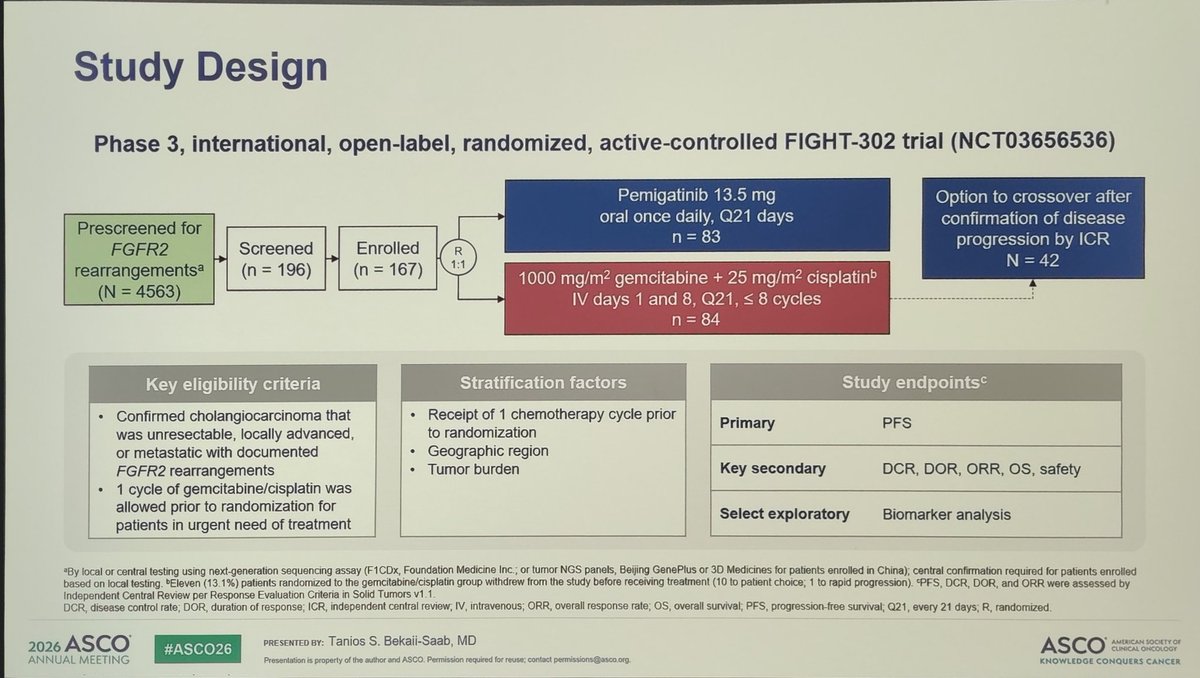
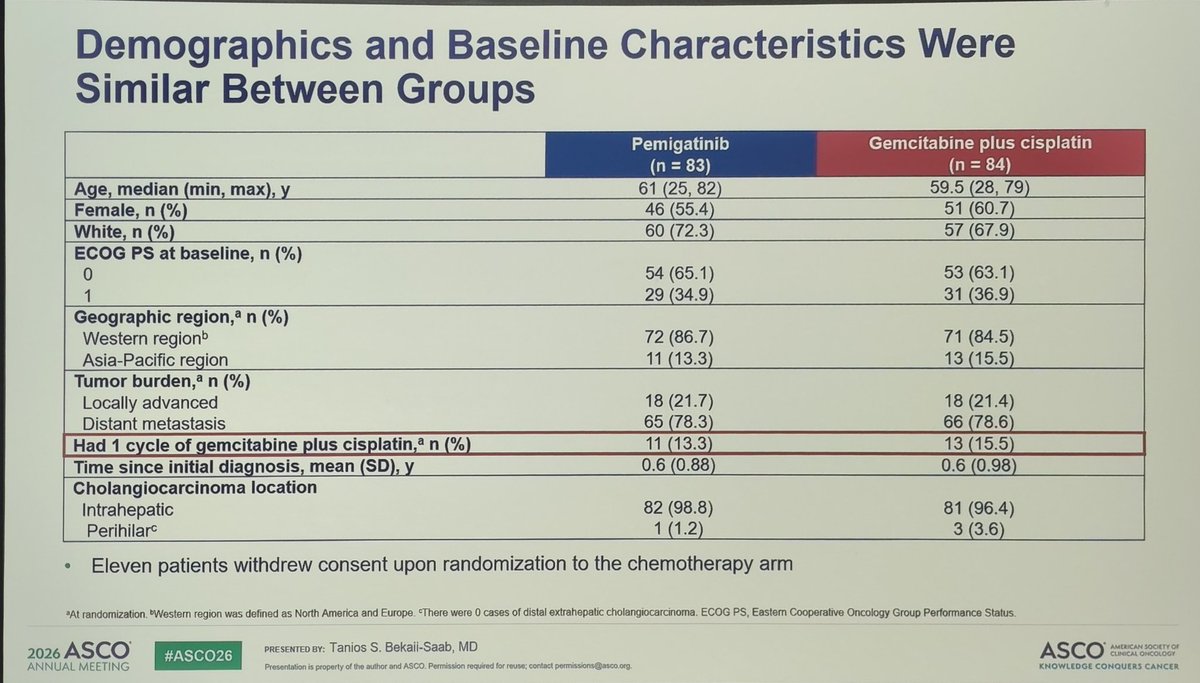
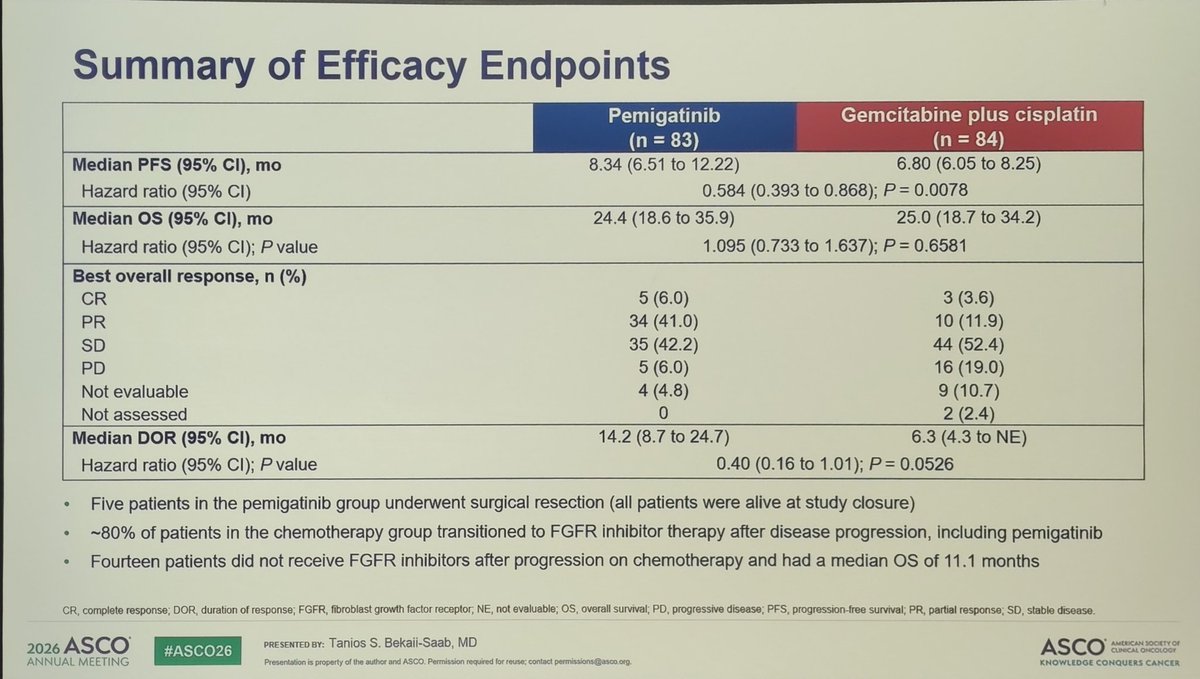
🚨 FIGHT-302 at #ASCO26
Pemigatinib vs CisGem in 1L FGFR2 rearranged BTC
• PFS 8.3 vs 6.8 mo
• ORR 47% vs 15%
• OS 24.4 vs 25 mo
🤔 Does this change the algorithm or lack of evidence given no IO CisGem?
😯 An option for pts who need response?
@_SEOM @atuvibi @GrupoTTD
10
12
697
Jaume Capdevila retweeted
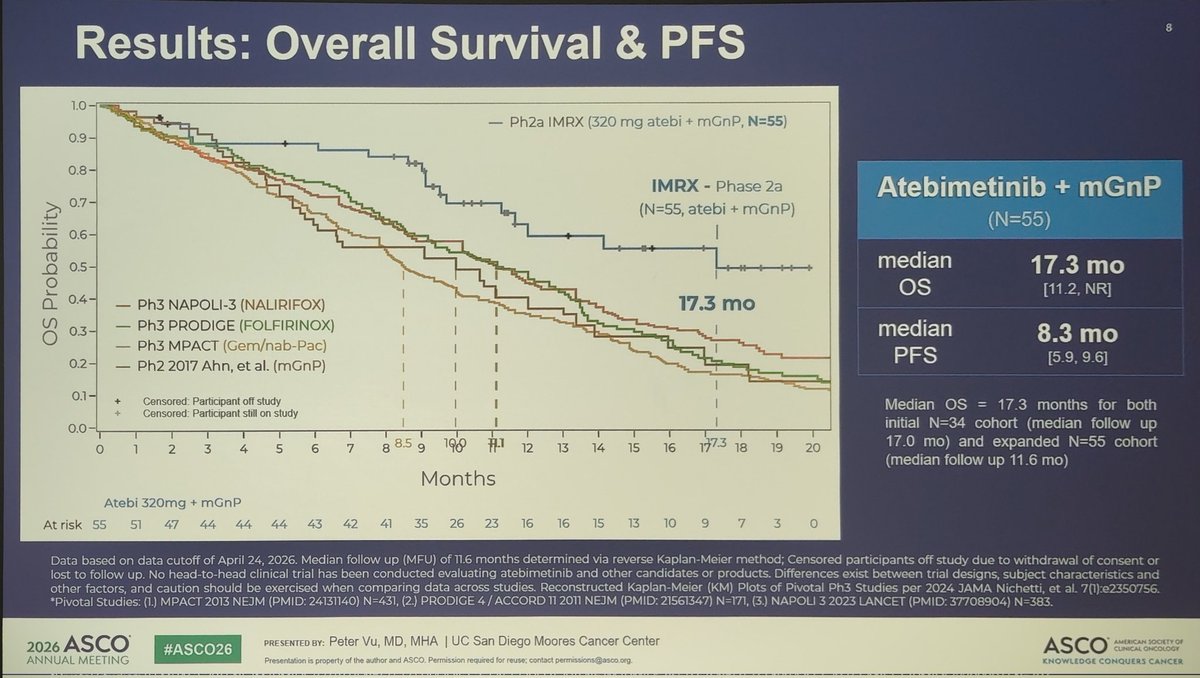
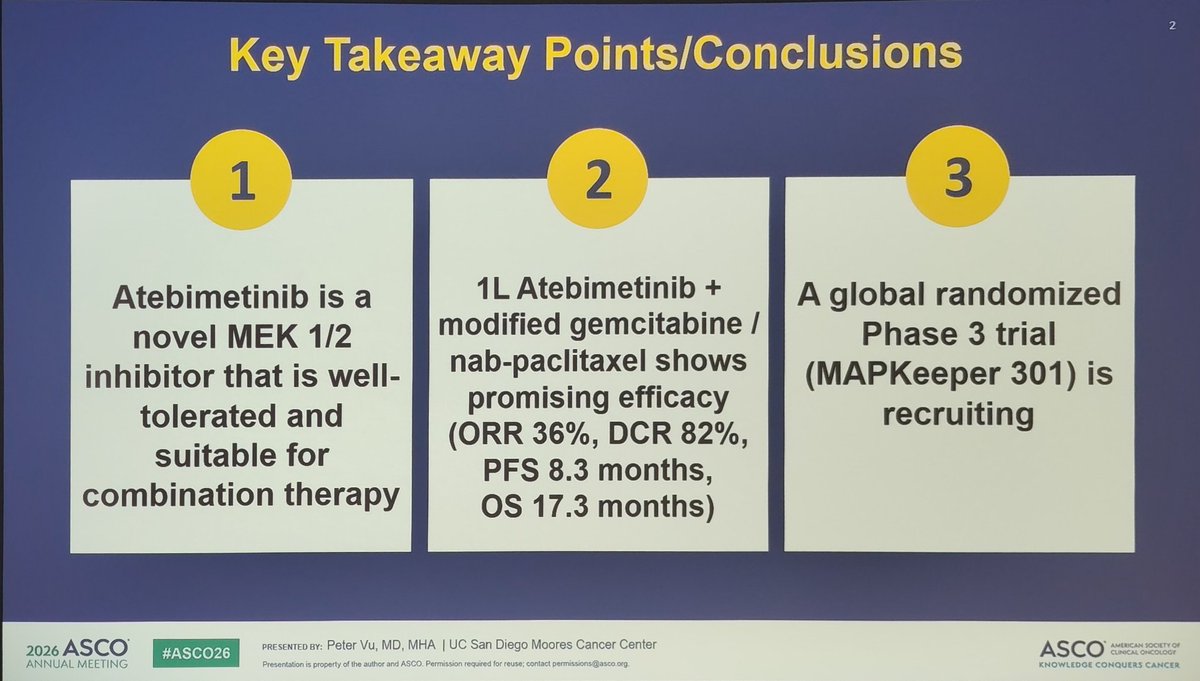
🚨 PDAC Mini-oral time at #ASCO26
Key takeaway points:
• Pembrolizumab does not add efficacy to Olaparib maintenance for gBRACA mutant PDAC.
• MEK inh QT (modified GnP) showed promising efficacy (OS 17 mo) -> Will they play a role with KRAS inh?
@_SEOM @GrupoTTD @myESMO

1
3
9
464


Jaume Capdevila retweeted
Key posters on FGFR2 in BTC:
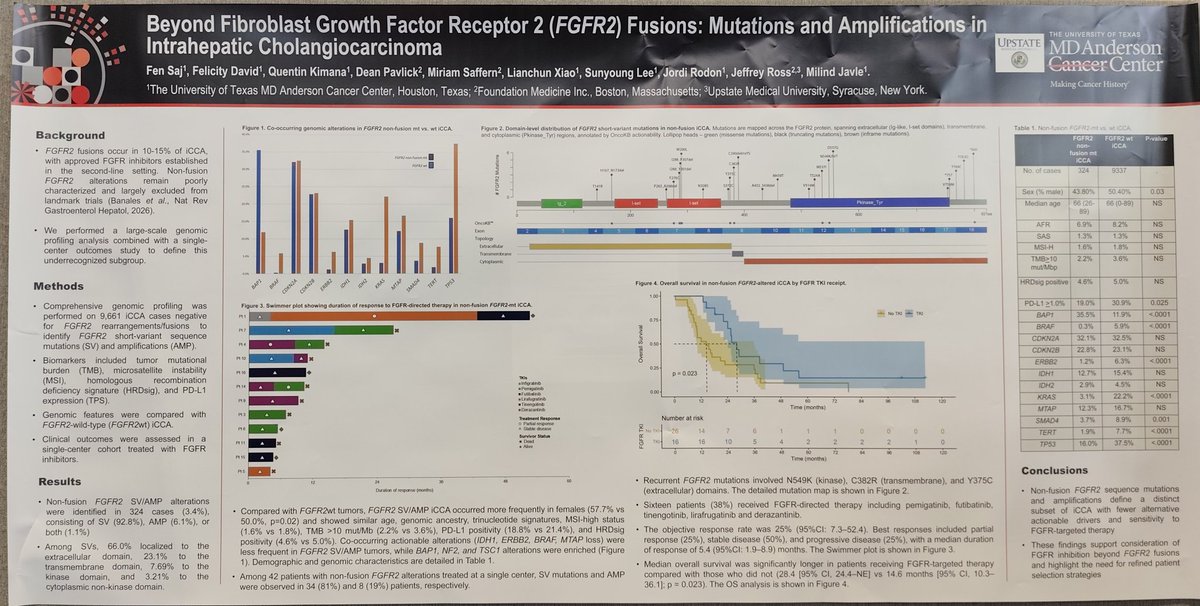
• Mut or ampl seen in ~3% of cases → eligible for targeted FGFR2inh
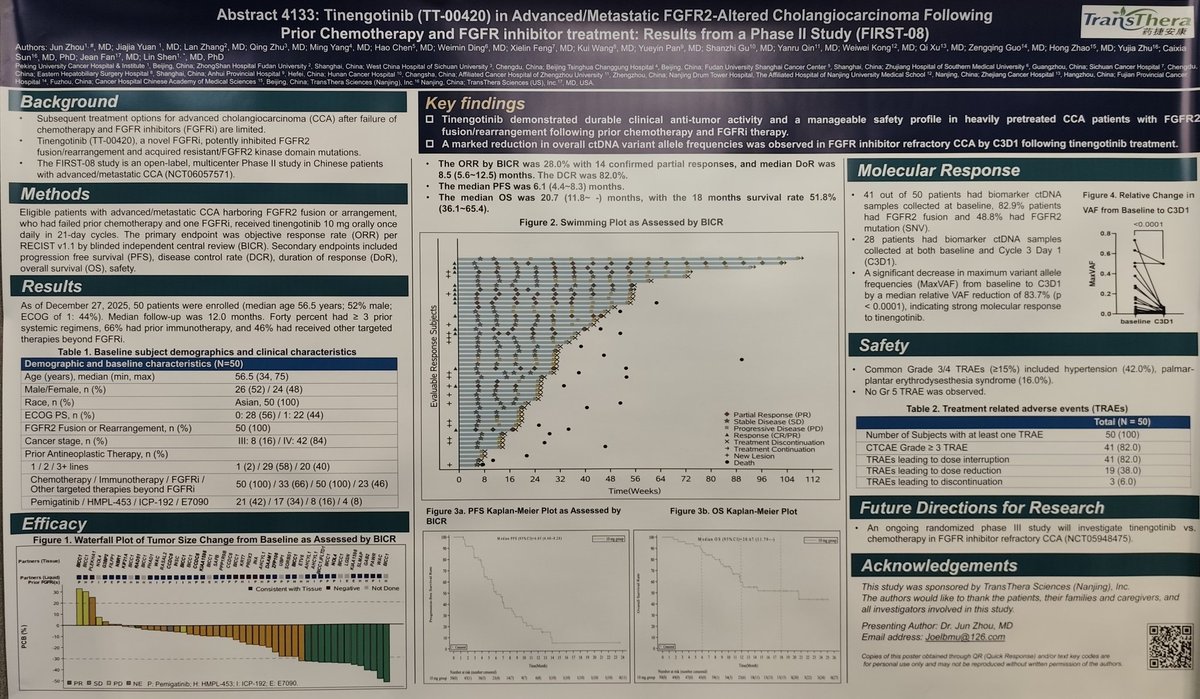
• Tinengotinib shows efficacy in pts pretreated with FGFR2inh
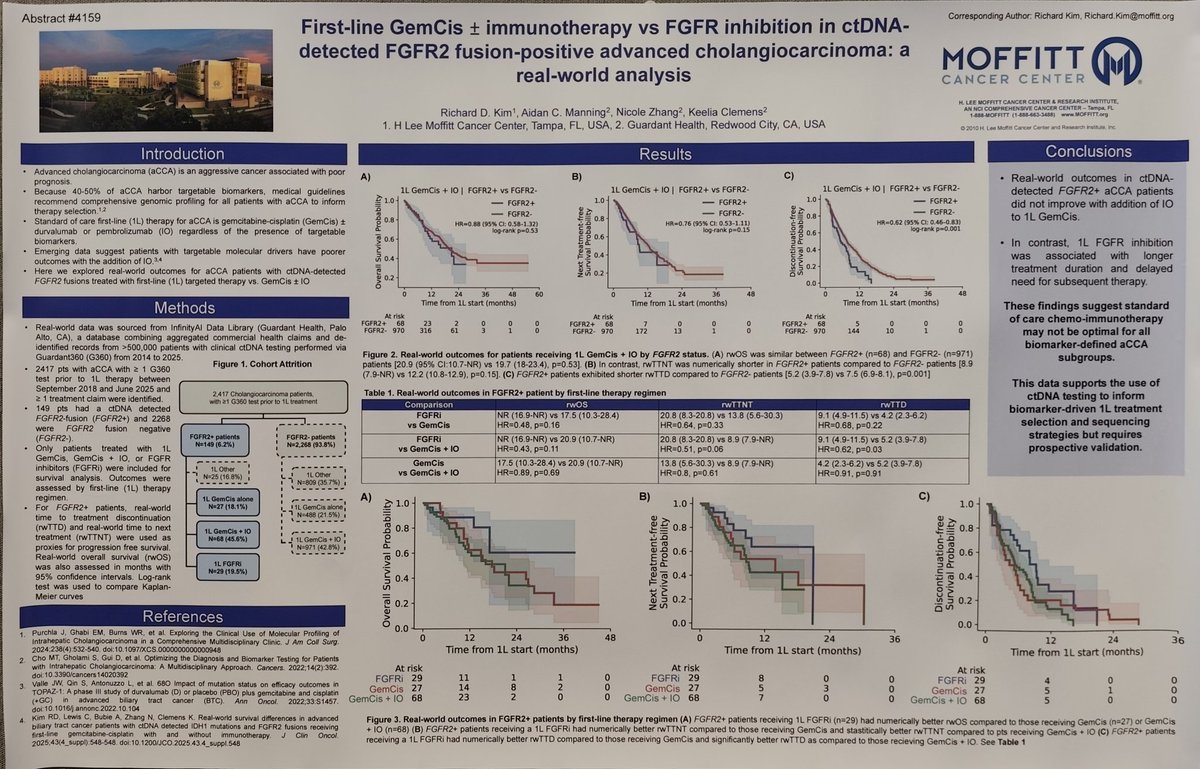
• RWD suggest FGFR2inh 1L may deliver better PFS vs CisGem IO.
🕵️♂️ results from FIGHT-302.
@GrupoTTD #ASCO26
1
4
9
362
Jaume Capdevila retweeted

May 31
This is not simply a new pancreatic cancer drug.
It is a reminder that even “undruggable” biology can become treatable with persistence.
Daraxonrasib doubled median OS vs chemotherapy in RAS G12 metastatic pancreatic cancer: 13.2 vs 6.6 months.
A remarkable ASCO moment.
#ASCO26
@DrChoueiri @TiansterZhang @CathyEngMD @montypal @tompowles1 @brian_rini @cdanicas @GlopesMd @PGrivasMDPhD @nataliagandur @yekeduz_emre @neerajaiims @ASCO @ONCOassist @OpenMedicineHQ @MedwatchKate @scserendipity1 @CParkMD @urotoday @OncLive @crisbergerot @urologysummit @SuyogCancer @Larvol @IMG_Oncologists
24
277
1,351
192,077
Jaume Capdevila retweeted
Prime time at #ASCO26 ❗ Daraxonrasib improves PFS and OS in second-line PDAC treatment compared to QT. Grateful to be part of this important moment for patients. Audience on its feet applauding, fully aware of this historic milestone.
6
14
389

Presented at #ASCO26:
Among patients with previously treated metastatic pancreatic ductal adenocarcinoma, the RAS(ON) inhibitor daraxonrasib led to significantly longer overall survival and progression-free survival than chemotherapy. Full phase 3 RASolute 302 trial results: nej.md/4nWaxvM
@ASCO
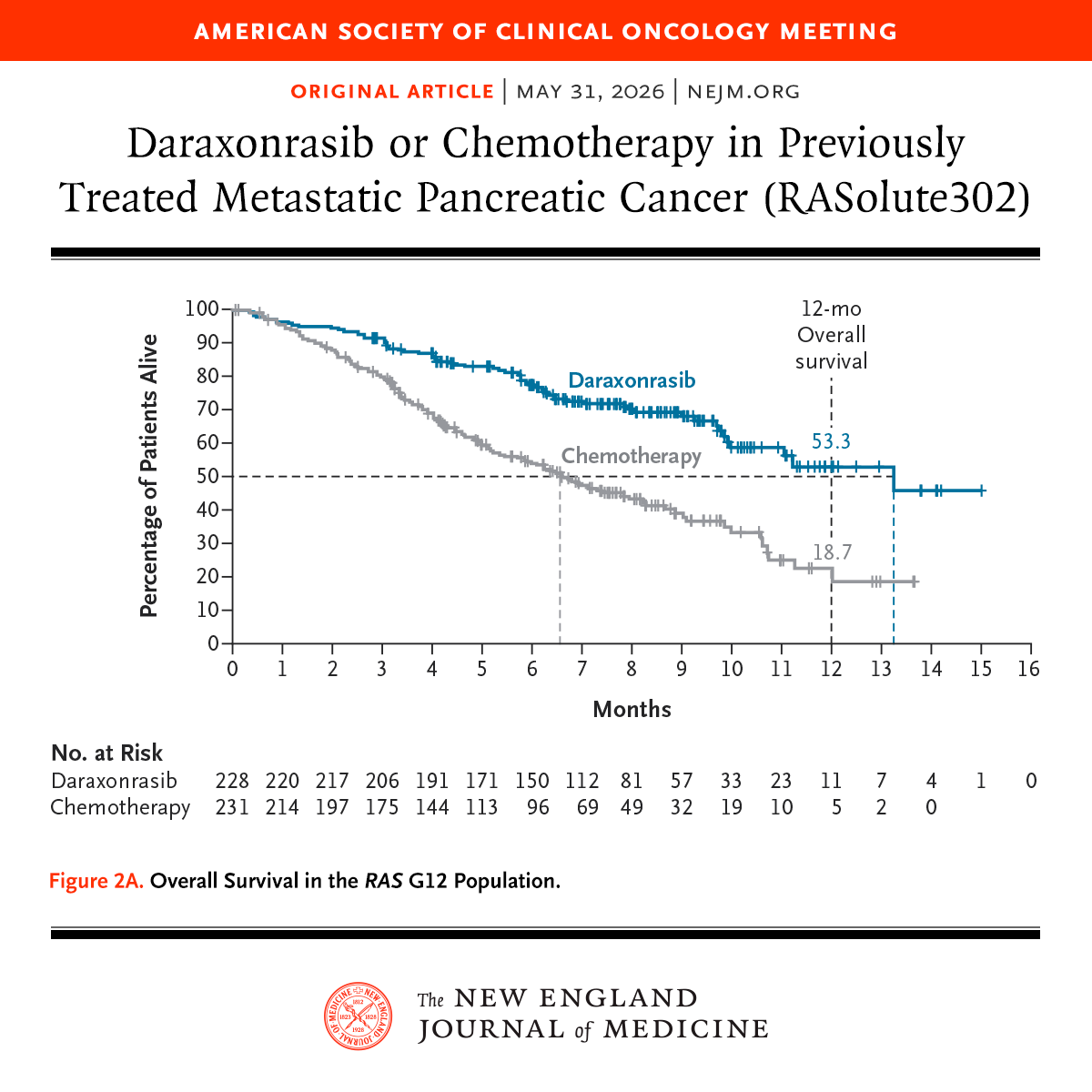
ALT Graph from a study published in the New England Journal of Medicine on daraxonrasib versus chemotherapy for metastatic pancreatic cancer. The x-axis represents months, and the y-axis shows the percentage of patients alive. Two lines indicate survival rates: daraxonrasib (blue) and chemotherapy (gray). The bottom section lists patients at risk over time. Title and journal logo are included.
52
2,054
5,574
2,463,857
Jaume Capdevila retweeted
May 31
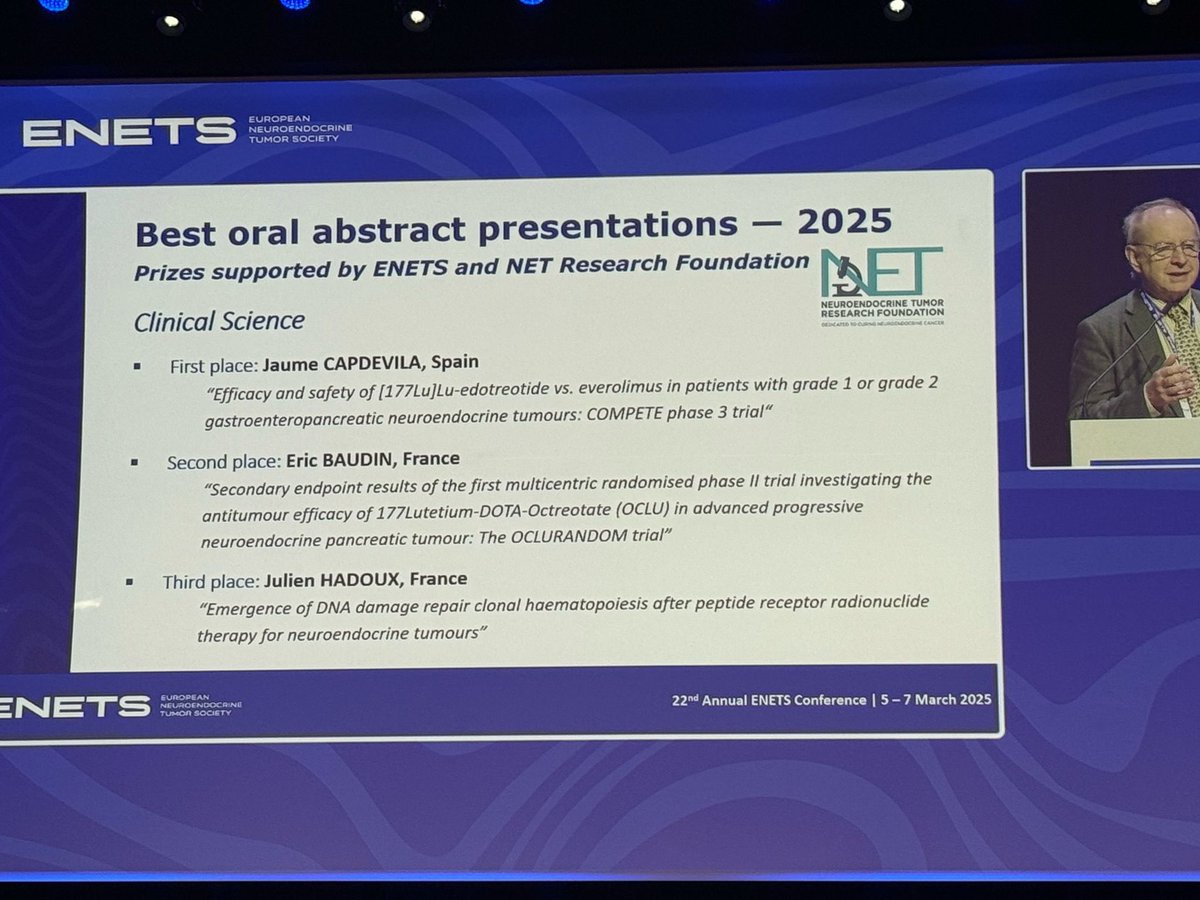
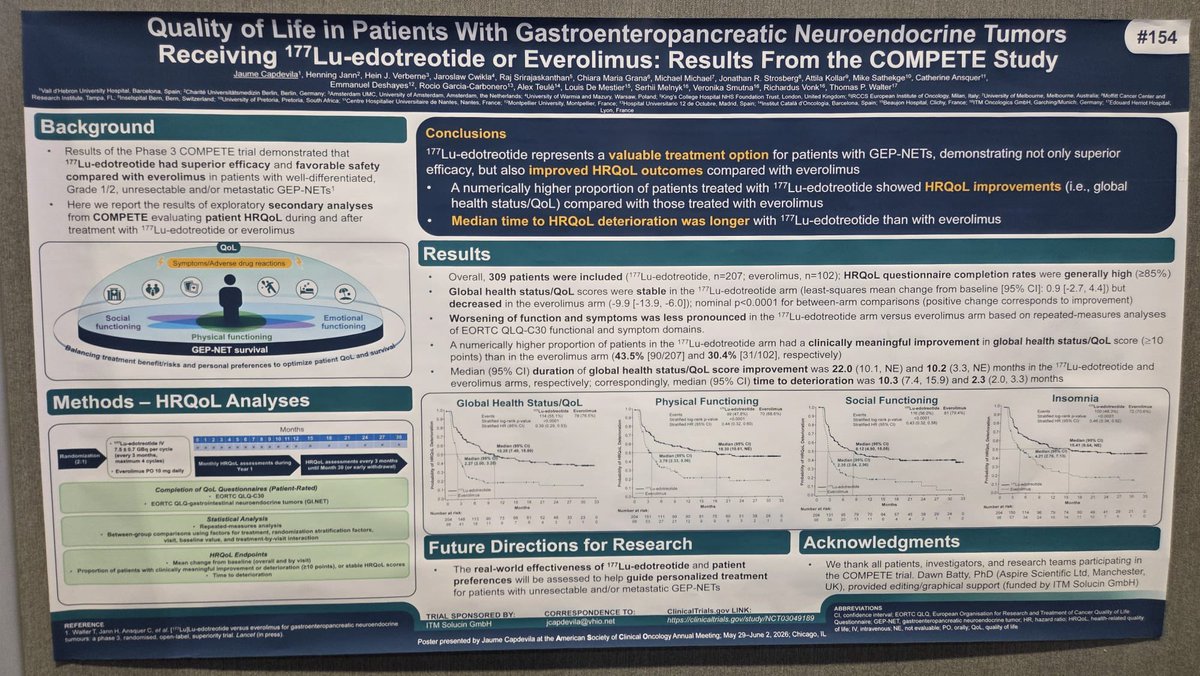
🔵 #ASCO26 | El Dr. Jaume Capdevila presenta los datos de calidad de vida del estudio COMPETE.
✔️ 177Lu-edotreotide vs everolimus
📈 Mejor HRQoL
📈 Más pacientes con mejoría clínica
📈 Mayor tiempo hasta deterioro
🎯 PRRT mejora la calidad de vida de los pacientes con TNE-GEP.
1
6
11
489
Jaume Capdevila retweeted

May 31
#ASCO26
This one is special.
This is the hottest paper of 2026 and potentially in the history of pancreatic cancer.
Let’s dive in.
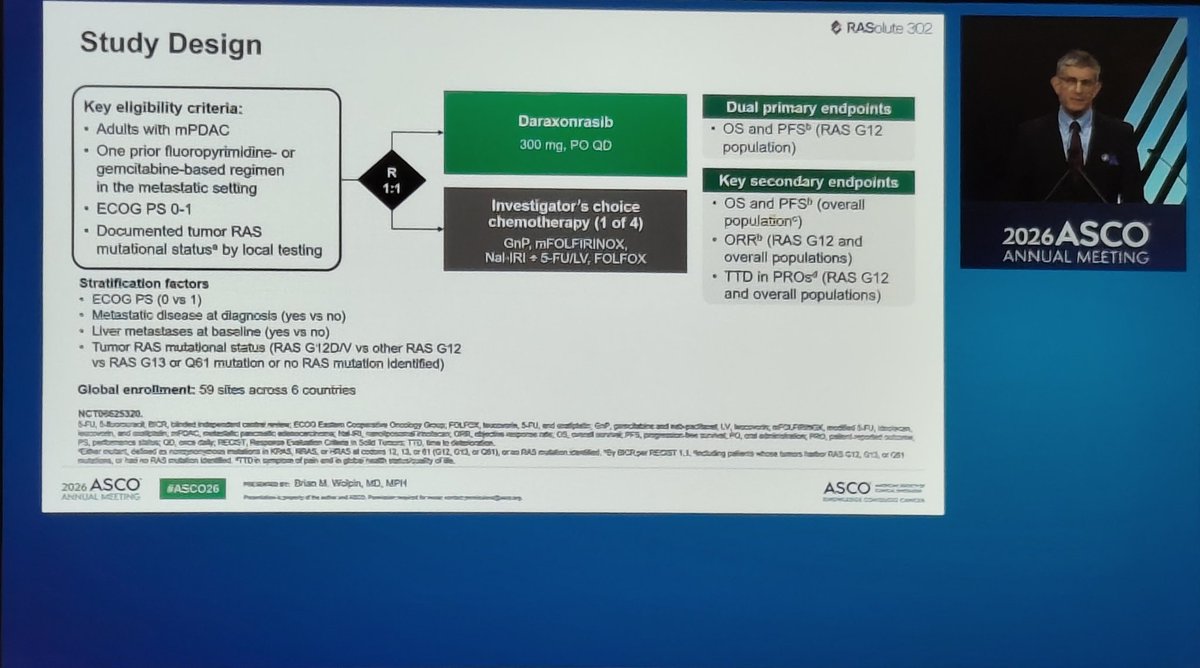
RASolute 302: Daraxonrasib vs investigator’s choice chemotherapy in previously treated metastatic pancreatic cancer
Abstract LBA5 (soon!)
Presentation: May 31, 2026, 3:21-3:33 PM CDT
For decades, pancreatic cancer has been where good ideas go to die.
We have optimized chemotherapy. We have sequenced chemotherapy. We have celebrated modest gains.
But the central driver of PDAC has always been sitting there in plain sight:
RAS.
More than 90% of pancreatic cancers have oncogenic RAS mutations, and until recently, we had essentially nothing direct to do about it.
Daraxonrasib is an oral RAS(ON) multiselective inhibitor targeting the active GTP-bound state of mutant and wild-type RAS.
And in RASolute 302, it delivered.
Quick hits:
📌 Phase 3 international randomized trial 500 patients with previously treated mPDAC Daraxonrasib vs investigator’s choice chemotherapy
🧬 RAS G12 population
91.8% of patients had RAS G12 mutations
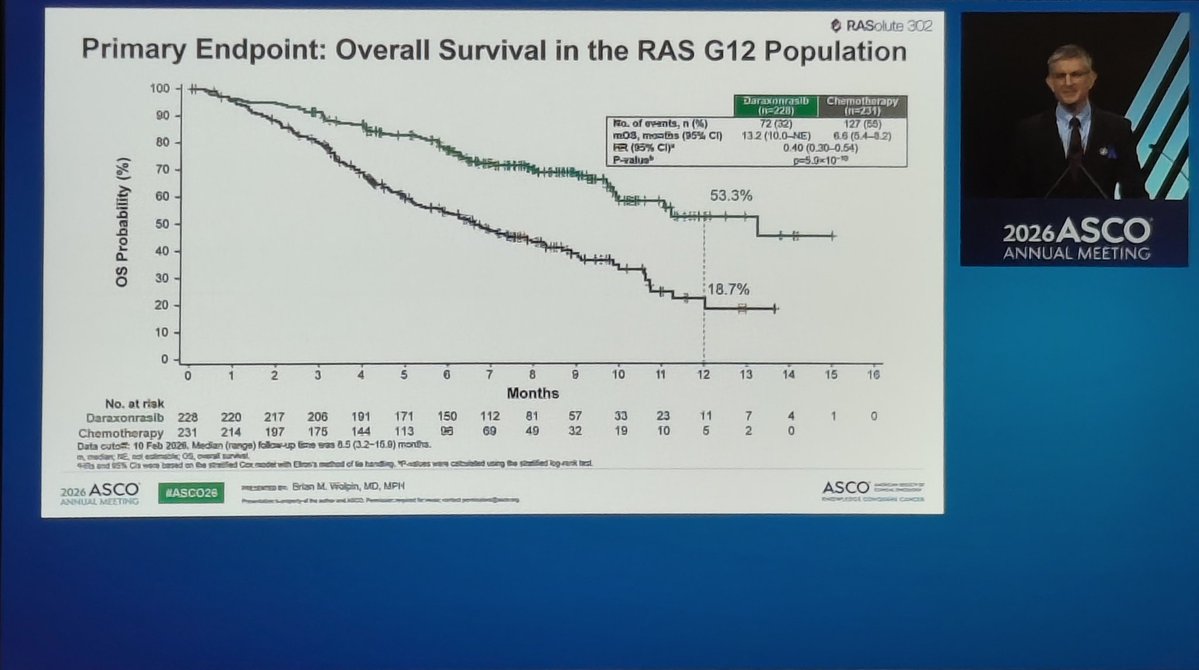
📈 OS in RAS G12 population
13.2 vs 6.6 months
HR 0.40
P<0.001
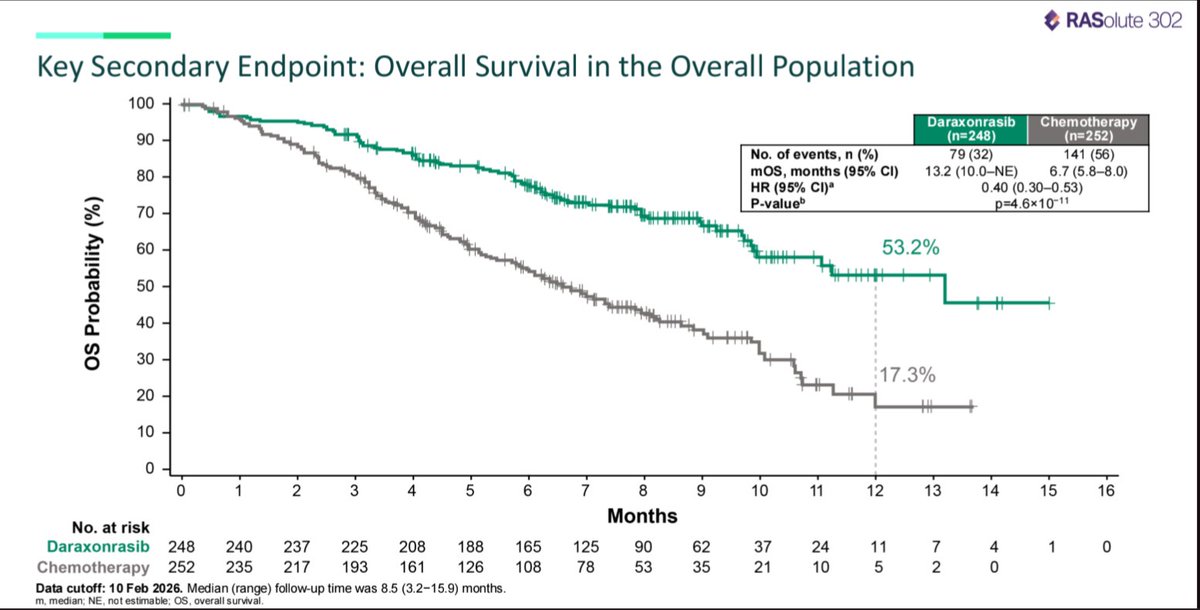
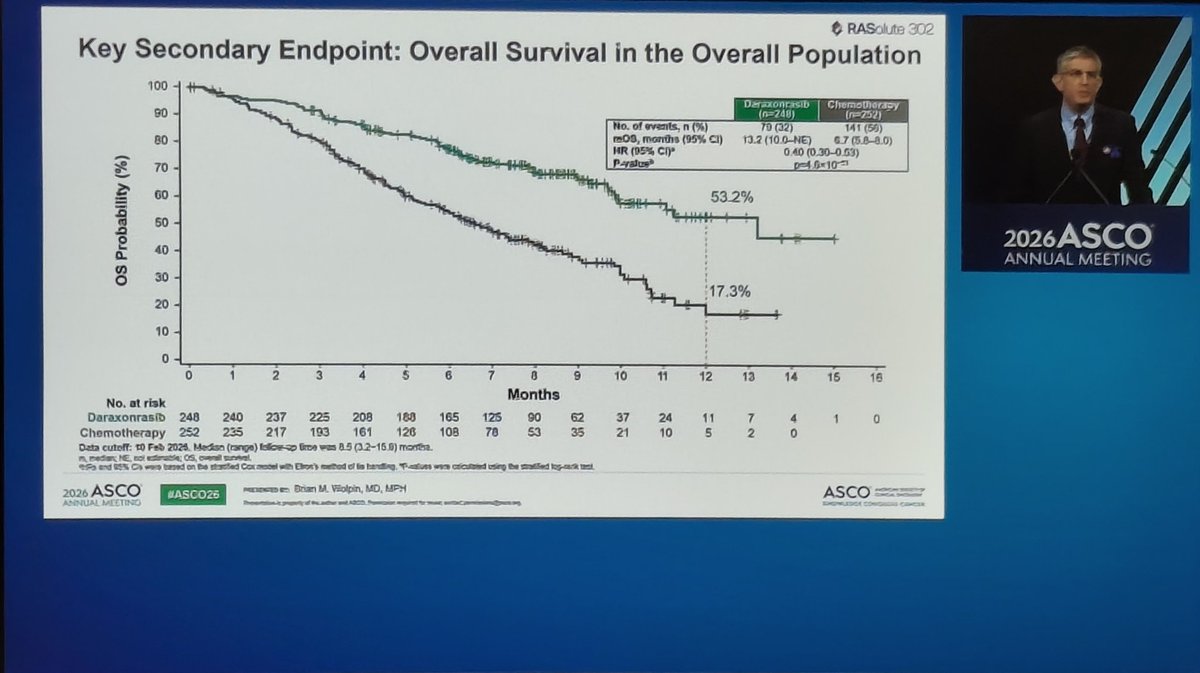
📈 OS in overall population
13.2 vs 6.7 months
HR 0.40
P<0.001
📊 PFS in RAS G12 population
7.3 vs 3.5 months
HR 0.45
P<0.001
📊 PFS in overall population
7.2 vs 3.6 months
HR 0.49
P<0.001
🔥 12-month OS
Overall population: 53.2% vs 17.3%
⚠️ Toxicity matters, but this was not just more efficacy for more toxicity
Grade ≥3 AEs: 61.8% vs 69.6%
TRAEs leading to discontinuation: 1.2% vs 11.2%
This is the kind of survival curve we almost never get to see in pancreatic cancer.
This validates RAS(ON) inhibition in the most RAS-addicted major cancer. It takes a target we have talked about for decades and turns it into a clinically meaningful survival benefit in a randomized phase 3 trial.
The next questions come fast: 1L combinations, maintenance, perioperative disease, sequencing, resistance, toxicity management, and whether this becomes a new backbone.
RAS is here, and it couldn’t have come sooner.
nejm.org/doi/full/10.1056/NE…
@TheGutonclab @UGrewalMD @TimothyJBrownMD @OncoAlert @Onco_Nexus @ASCO
@NazliDizman @LauraAlderMD @DVAraujoMD @DrBarbiOnc @LauraEsfeller @FunchainMD @YGaritaonaindia @DrSAHaddad @jgong15 @iandresmeraz @SakditadMD @RamilaShilpakar @RohitBanwar @lungoncdoc

12
269
911
85,161

