
This is my no politics Twitter account. I need some sanity occasionally. Physician & Meta-Physician #Theology #Philosophy #Oncology #Statistics #Investing
Joined March 2019
- Tweets 1,792
- Following 284
- Followers 449
- Likes 7,113
308 Photos and videos











Pinned Tweet

May 21
Reminder Bayesian methods do not assign true or ontological probabilities to events such as the objective chance of a fair coin landing heads or a dice producing a six. Bayes treats probability as a measure of uncertainty or degree of belief that is through mathematical distributions like the beta, gamma, or normal curves, thus in the Bayesian framework, what is called “probability” is not the truth but a numerical representation derived from integrating areas under these curves being called "probability." Remember they depend on the chosen prior, thus changing the prior will alter the resulting “probabilities,” highlighting that they are not properties of the real world, but artifacts of the modeling assumptions. Theoretically they are just representations of your beliefs, which is why Bayes has been resisted as a foundation for stats.
May 21

@PhilosopherMD1 Cute concern. Meanwhile p-values gave us a replication crisis, p-hacking, and 50 years of irreproducible medicine. Bayes gives actual probabilities. Fix your own house first.
1
3,022
PhilosopherMD retweeted

I’ve seen this quote from Dr Glatstein before but TBH I did not understand what it meant. Here @DrewMoghanaki explains that we as ROs, a tiny profession, need to be prepared to advocate fiercely for our patients (and specialty)…even if that means walking into tumor board like a black-hat cowboy in a 1980s Western: unsettling, but impossible to ignore.

2
1
10
2,598
PhilosopherMD retweeted

Totally agree with you @NiuSanford. The problem with Bayesian analyses is that our “priors” are often TOTALLY wrong, but they factor into the conclusions.
We might have said the RTOG0617 74 Gy arm was 80% likely to win, and that guess could have led to a different conclusion when the trial was read out. Same with PARTIQoL, stem cell transplants for breast cancer, and other trials with surprise negative results.
3
1
6
526
PhilosopherMD retweeted

What a day it has been!!!
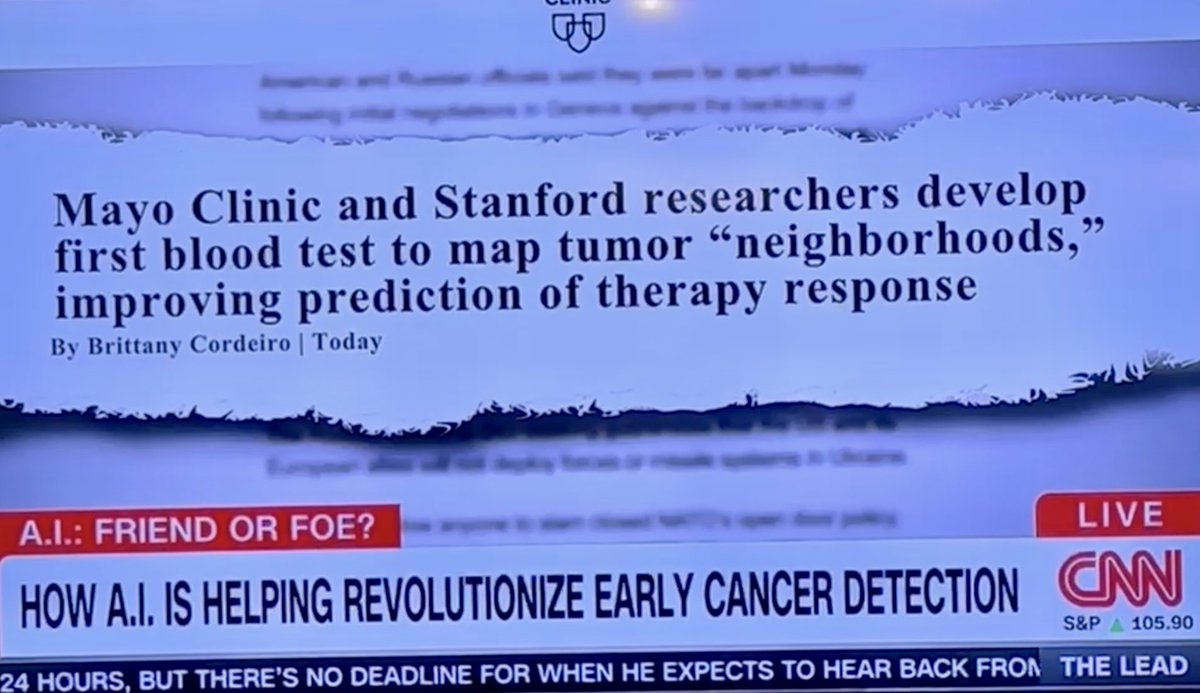
@AaronNewmanLab and I started this journey years ago back when we were both junior faculty. A difficult question — Can we perform liquid biopsy of the tumor microenvironment?
Spoiler alert. We finally did it! In @Nature & on @CNN today w/ @jaketapper!!

10
34
180
10,760
PhilosopherMD retweeted

Apr 6
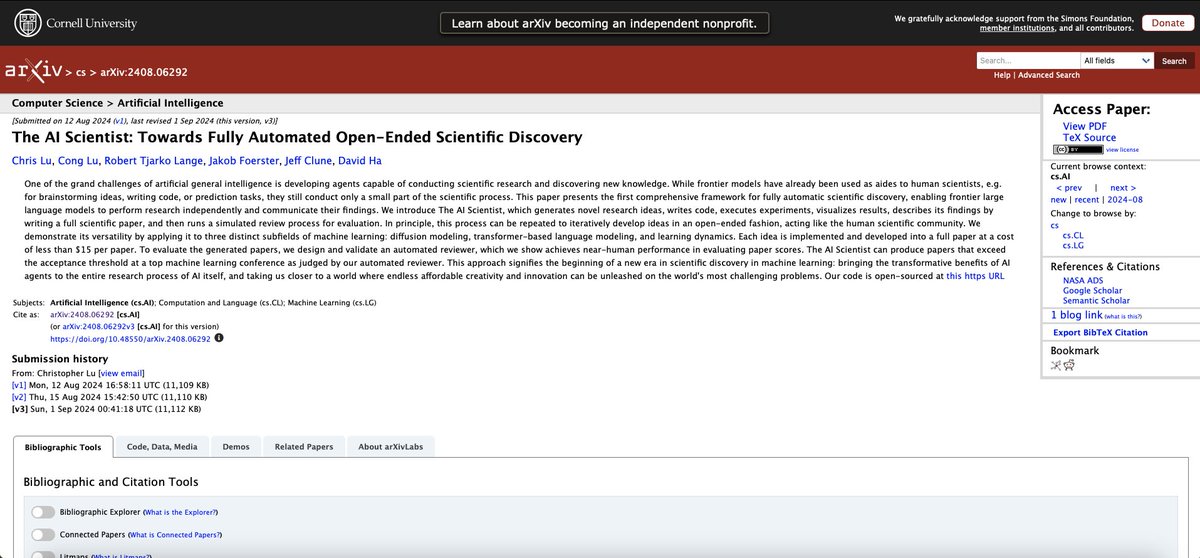
BREAKING: An AI just wrote a research paper. Submitted it to a top science conference. Passed peer review. Nobody on the review panel knew it was AI.
The paper is called "The AI Scientist." Published last week in Nature. Built by Sakana AI in Tokyo, with researchers from Oxford and UBC.
Here is what it did — completely on its own.
It read existing scientific literature. Formed a hypothesis. Designed an experiment. Ran the experiment. Analyzed the results. Wrote the full academic paper. Then peer-reviewed its own work.
No human at any stage.
They submitted three fully AI-generated papers to a top ML conference under blind peer review. Human reviewers were told some might be AI, but not which ones.
One was accepted. It scored higher than 55% of human-authored papers at that same conference.
The accepted paper cost $15 in compute to produce.
Fifteen dollars.
Now here is the part nobody is talking about.
The team found a clear scaling law: stronger foundation models produce higher-quality research outputs. Better base model in, better science out.
Which means this gets dramatically better — automatically — every time a new model drops.
Right now it is limited to computational ML experiments. No biology. No chemistry. No physical labs.
For now.
What happens when the thing that discovers new science... is itself?
65
148
485
122,572
Apr 1
Free access (given by the author herself🤩) to an amazing book by @learnfromerror! It's one of my favorite books on science and has deeply shaped how I think about medical studies and the use of statistics. You will not regret reading it and will be helpful during this time we are discussing statistical methods in medicine. errorstatistics.com/2026/04/…
1
1
353
PhilosopherMD retweeted

Mar 29
I don't see where intentions come in, but whenever we talk of the capabilities of an instrument, we're talking about how it would behave in applications other than this one. Yet we can use that information about its capabilities to make inferences about the case at hand. Only Bayesians think warranting an inference must mean assigning a Bayesian belief in its truth..
1
1
2
181
PhilosopherMD retweeted
Mar 25
Any replies from my frequentist friends @learnfromerror @predict_addict ? Bayes is not a cure all (poison?) and has well known flaws and as the article notes good reasons why it has not been used. From the article quoted that rightly states “On the contrary, currently used methods that preserve objectivity and benefits of randomization are not outdated, old school, or closed-minded. They are principled, based on scientific fundamentals for protecting integrity and ensuring robustness of scientific conclusions.” tinyurl.com/296jsfmf
4
2
2
1,323
PhilosopherMD retweeted

Starting to see a number of these "No True Scotsman" rationalizations for negative TORPEDO results. It's easy to make this sort of argument especially with respect to procedural interventions. At some point though one has to admit the possibility that protons just didn't perform as well as expected with respect to extent of late toxicity risk reduction in definitive HNSCC treatment.

A critical point in proton therapy is "how the sausage is made". Passive scatter is not PBS, SFO is not MFO, spot size, layer numbers, setup margins (which drives robustness opt), IGRT, ease of verification scans/adaptive replanning. All matter more than whats on a nominal plan
5
2
13
2,397
PhilosopherMD retweeted

Mar 21
🧵 Just published in @TheLancet: TORPEdO – the first phase 3 RCT designed specifically to test whether IMPT (proton beam) improves late function & QoL vs modern IMRT in oropharyngeal SCC.
Short answer: It doesn’t.
Long answer (with the numbers that matter) 👇
7
33
80
20,650
Mar 18
I hope I’m not the only one confused by the MARCAP prostate data that flies in the face of what I was taught in residency. Shout out to @zklaassen_md for the best summaries I’ve seen here urotoday.com/conference-high… & urotoday.com/conference-high…
1
2
502
PhilosopherMD retweeted

Feb 26
Academics using less AI than me are inefficient luddites that might as well be writing with quill and ink. Academics using more AI than me are committing research misconduct.
1
11
2,251
Mar 1
Heavy hitters going at it! Great discussion.
Feb 26

Great work @DrSpratticus and @AmarUKishan ! For me, a clear MFS benefit for 6 mos ADT in the salvage setting is certainly worth recommending it for most patients. And that benefit looks to hold for PSAs >= 0.20. Although, the NRG data showing DECIPHER is predictive of MFS benefit in this setting is quite helpful for further triage. #GU26

1
255
PhilosopherMD retweeted

Jan 24
This paper is just...glorious. It's the distilled, concentrated version of the decay of academia.
It's actually the tip of darker iceberg, but I need more time to put that together.
For now, let's enjoy the following:
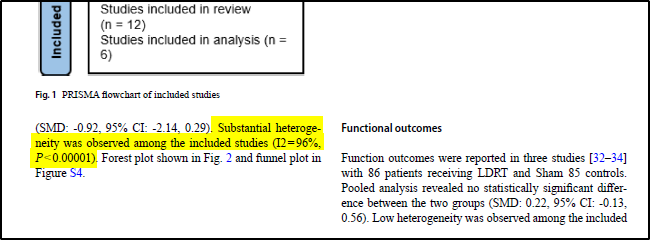
First, the calculated I² for their included studies was...96%. That's...insane. I would not expect anyone to submit a meta-analysis with this level of heterogeneity. If someone did, I would expect a desk rejection and/or peer review rejection.
It also doesn't tell us anything about the effect size or direction. Simply put: the reason this value is so high is because the most modern and well-designed LDRT trial included (Fazilat-panah et al, 2025) showed a massive/significant benefit to LDRT, which washed out the older/poorly designed studies.
(My charitable hypothesis here is that the meta-analysis was submitted in March 2025 but not accepted till July 2025. The Fazilat-panah paper was published online in March 2025 and could not have been included in the original submission. My assumption is that the original version of the meta-analysis had a much lower/more reasonable I². When undergoing peer review, someone asked for this new study to be included. Of course, the question then becomes why the meta-analysis was accepted after revision, but I only have non-charitable hypotheses for that explanation.)
Second, while I don't think this meta-analysis was ENTIRELY crafted using an AI ChatBot, I suspect AI was...heavily relied on.
The most glaring evidence is in the "References" section.
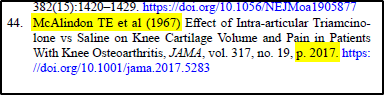
The McAlindon JAMA paper is given a publication year of 1967 and a page number of 2017.
In reality, this paper was published in 2017 on page number 1967.
This is a classic, super annoying LLM problem called "metadata transposition hallucination".
LLMs see everything as tokens, and knows (predicts) what tokens are likely to (or should) occur together. In this case, an LLM "knows" that the McAlindon paper citation string contains "2017" and "1967".
But it doesn't understand the MEANING of these numbers (tokens), so it swapped them.
I would bet a lot of money that this wouldn't have happened if the page number was 3004, for example, because that would be a date a thousand years in the future, and the LLM would therefore be unlikely to predict that token in that location.
Of course, it's possible for a human to make an error like this but...unlikely.
Anyway, this paper is a beautiful example of the collapse of civilization.
Jan 24

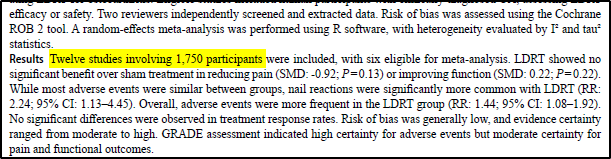
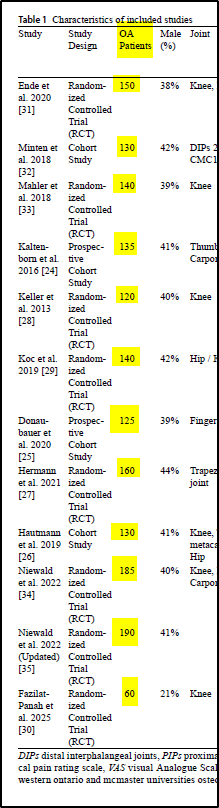
I have questions about basic math skills in this paper, considering the body of the text states multiple times their pool had 1,750 patients but Table 1 only sums to...1,665 patients.
Hilariously, that discrepancy is a p value ≤ 0.05...strong work kids!
1
8
25
4,672
PhilosopherMD retweeted

Jan 17
Update! My brilliant colleague and frequent coauthor, @MikkoPackalen writes with a different take about AI use in science and scholarship. His take is persuasive but contrary to mine. Perhaps he's right that I'm not fully appreciating the culture change that AI portends for science. Here's what he wrote to me:
Non-Dinosaur NIH AI Policy: "AI is an important opportunity for advancing and accelerating science. Applicants are encouraged to use AI as they best see fit. NIH understands that AI is deeply integrated in the workflows of many researchers, and NIH does not want to discourage the use of AI in any way. Of course, every researcher continues to be responsible for every aspect of their grant application submission, whether developed and written with AI or not."
8
10
66
11,221
Jan 14
None to happy about the FDA opening up
to Bayesian stats. I agree with @predict_addict

My new post 'The Lunatics Have Taken Over the Asylum'
Has been published on Medium
valeman.medium.com/the-lunat…
#FDA #pharma #bayesianism

1
3
5
1,037
PhilosopherMD retweeted

My new post 'The Lunatics Have Taken Over the Asylum'
Has been published on Medium
valeman.medium.com/the-lunat…
#FDA #pharma #bayesianism
1
3
8
2,146