
Proud to be Puerto Rican, mother, wife and oncologist, representing community oncologist @ASCO BOD 21-25, @TheStartcenterforcancercare. Opinions are my own.
Joined June 2019
- Tweets 7,045
- Following 603
- Followers 713
- Likes 18,311
89 Photos and videos












Pinned Tweet

8 Dec 2020
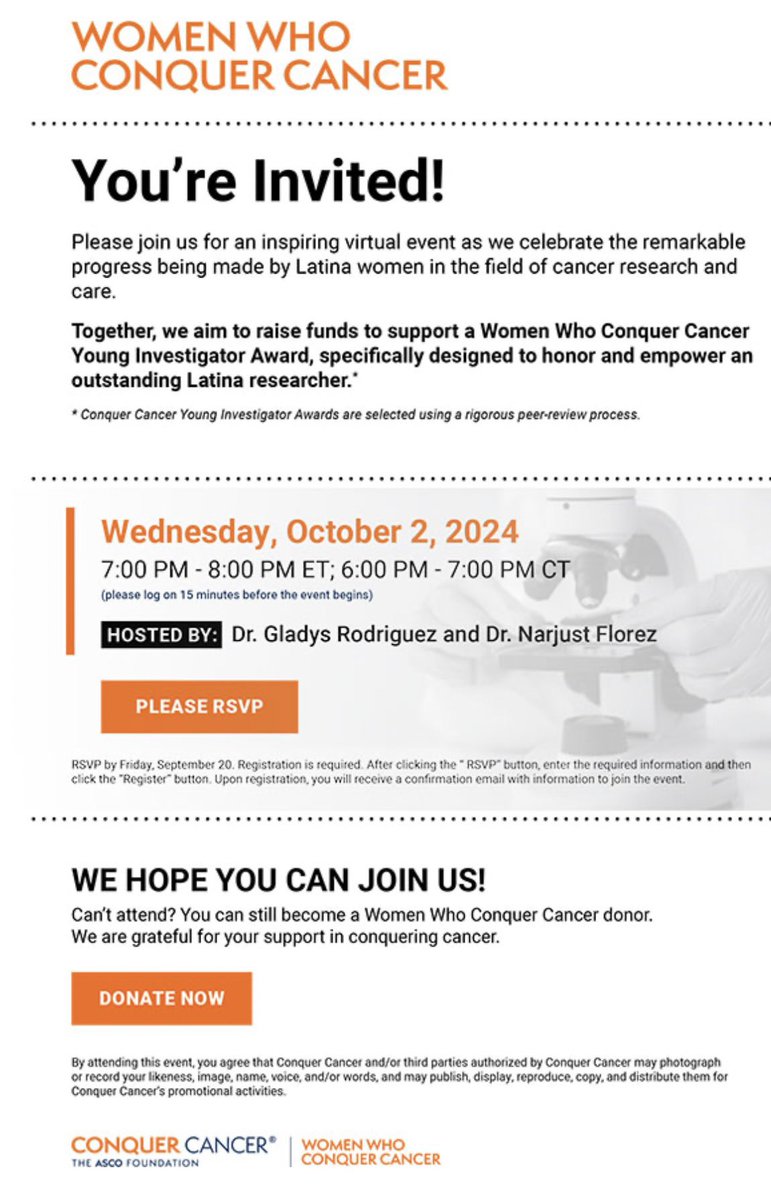
I am honor to join @NarjustDumaMD and @ASCO @ConquerCancerFd to fund a YIA for Latinas in oncology conquer.org/WWCCGIFT @SandraSwainMD @EdithPerezMD @ASCOPres Please help us reach the goal! @HemOncWomenDocs
1
15
30
Gladys Rodriguez,MD, FASCO retweeted

I wouldn't say that was my big takeaway of this paper or trial. The takeaway I got was there is a giant overall survival benefit for our youngest breast cancer patients to ovarian function suppression over tamoxifen. Sure, there are some low risk patients, where Tam alone is fine, but the majority of super young breast cancer patients present at later stage. If you’re going to give chemo then do not give tamoxifen alone, this needs to be more widely accepted in the community, as it’s been 15 years and the uptake is still too low. Too many oncologists do not give the youngest patients ovarian suppression, as they don't like dealing with how unpopular it is with patients, and difficult it is for patients. Yes it is hard, but it saves lives and it’s our duty to our patients to work with them on side effect management and not just abandon so easily when things get tough, as this is likely our most effective weapon in premenopausal ER breast cancer. We are failing our very young breast cancer patients who have the highest mortality from breast cancer when we do not strongly recommend this and then HELP patients with their side effects so they can stay compliant. This often take a lot of time and extra visits, but it really is so important. #Breastcancer #SOFT #TEXT
Jun 3

SOFT/TEXT 15-year final results: tamoxifen remains reasonable for low-risk premenopausal HR disease; in young, HER2−, high-risk patients, OFS—and especially exemestane OFS—provides a stronger endocrine backbone.
annalsofoncology.org/article…

7
25
95
19,448
Gladys Rodriguez,MD, FASCO retweeted

Jun 6
Powerful and poignant #asco2026 President’s Address by Eric Small: “The Science and Practice of Translation: Improving Cancer Outcomes Worldwide” @asco connection.asco.org/do/2026-…
1
8
21
1,200
Gladys Rodriguez,MD, FASCO retweeted

#asco26: 1) if patients with 4-9 ln are reluctant to get chemo get prosigna; 2) please enroll pts to ofset. Seems ofs is all we need in low genomic premen; 3) denosumab can be spaced out; 4) geda doublet in pik3m should be considered but watch tox; 5) no 1st line serd for now
20
75
10,901
Gladys Rodriguez,MD, FASCO retweeted

The #ASCO26 learning continues! Excited to join an outstanding faculty at #BestofASCO in 🌴☀️ Puerto Rico 🇵🇷 on June 13-14 Looking forward to great discussions, collaboration, and bringing the latest oncology advances to our community. @TotalHealthConf

1
8
23
1,167
Gladys Rodriguez,MD, FASCO retweeted

Jun 5
Amazing 🤩
Congratulations Dr. Meza! 🎊🎉🎉

Beyond grateful for being selected for Excellence Award from the Academy of Resident and Fellow Educators. This goes to my amazing mentors and attendings to show me what great educators look like 🎉
@marthamims @Elkhanany @BCMDeptMedicine 🕊️

1
1
6
616
Gladys Rodriguez,MD, FASCO retweeted
Love working at a place where people work hard, care, and know how to have fun along the way. Great #MiamiNights at #ASCO26 with our formidable @SylvesterCancer MedOnc Chair, @GlopesMd.

2
7
46
1,633
Gladys Rodriguez,MD, FASCO retweeted

Wow- 🤯 I thought summarizing one #ASCO26 presentation with character limits was a challenge.
@VKaklamani with a pretty good attempt to summarize all of breast into one tweet 😂 👏 🤩

#asco26: 1) if patients with 4-9 ln are reluctant to get chemo get prosigna; 2) please enroll pts to ofset. Seems ofs is all we need in low genomic premen; 3) denosumab can be spaced out; 4) geda doublet in pik3m should be considered but watch tox; 5) no 1st line serd for now
1
8
37
6,434
Gladys Rodriguez,MD, FASCO retweeted

Jun 1
What % of patients with HER2 eBC and residual disease are eligible for T-DXd according to the DB-05 criteria?
👉48%
👉the majority of patients (lower risk) remain eligible for T-DM1
👉T-DM1-only eligible patients experienced favorable real-world outcomes, despite having RD
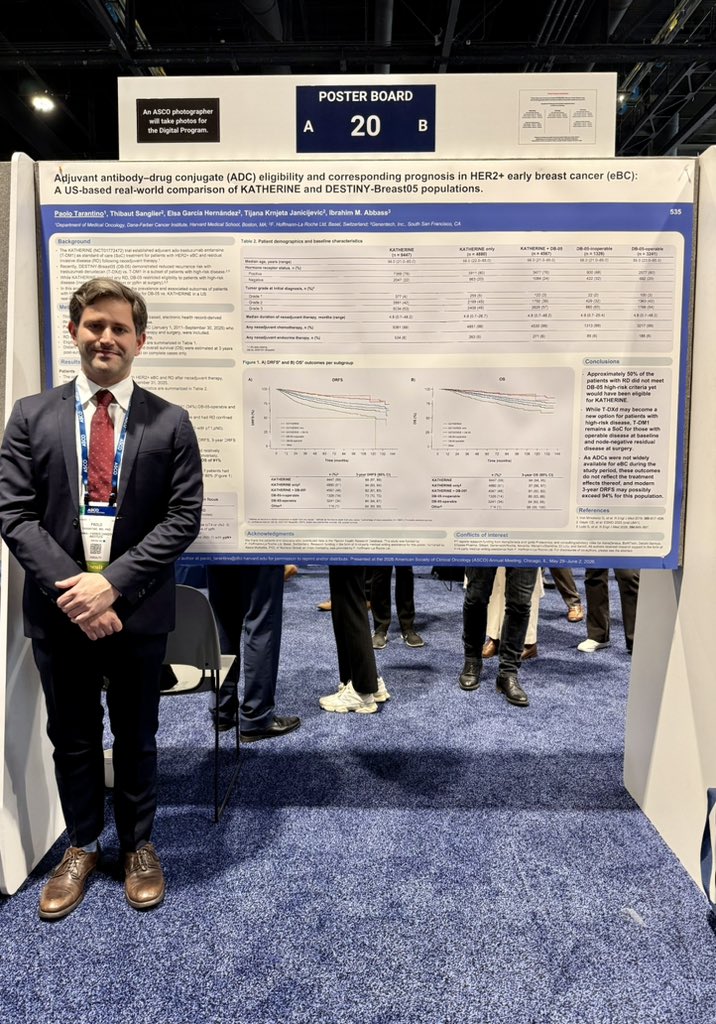

#ASCO26 Poster Session | Poster #20 | Adjuvant antibody-drug conjugate (#ADC) eligibility and corresponding prognosis in HER2 early #BreastCancer: A US-based real-world comparison of KATHERINE and DESTINY-Breast05 populations. @PTarantinoMD

1
20
74
10,791
Gladys Rodriguez,MD, FASCO retweeted

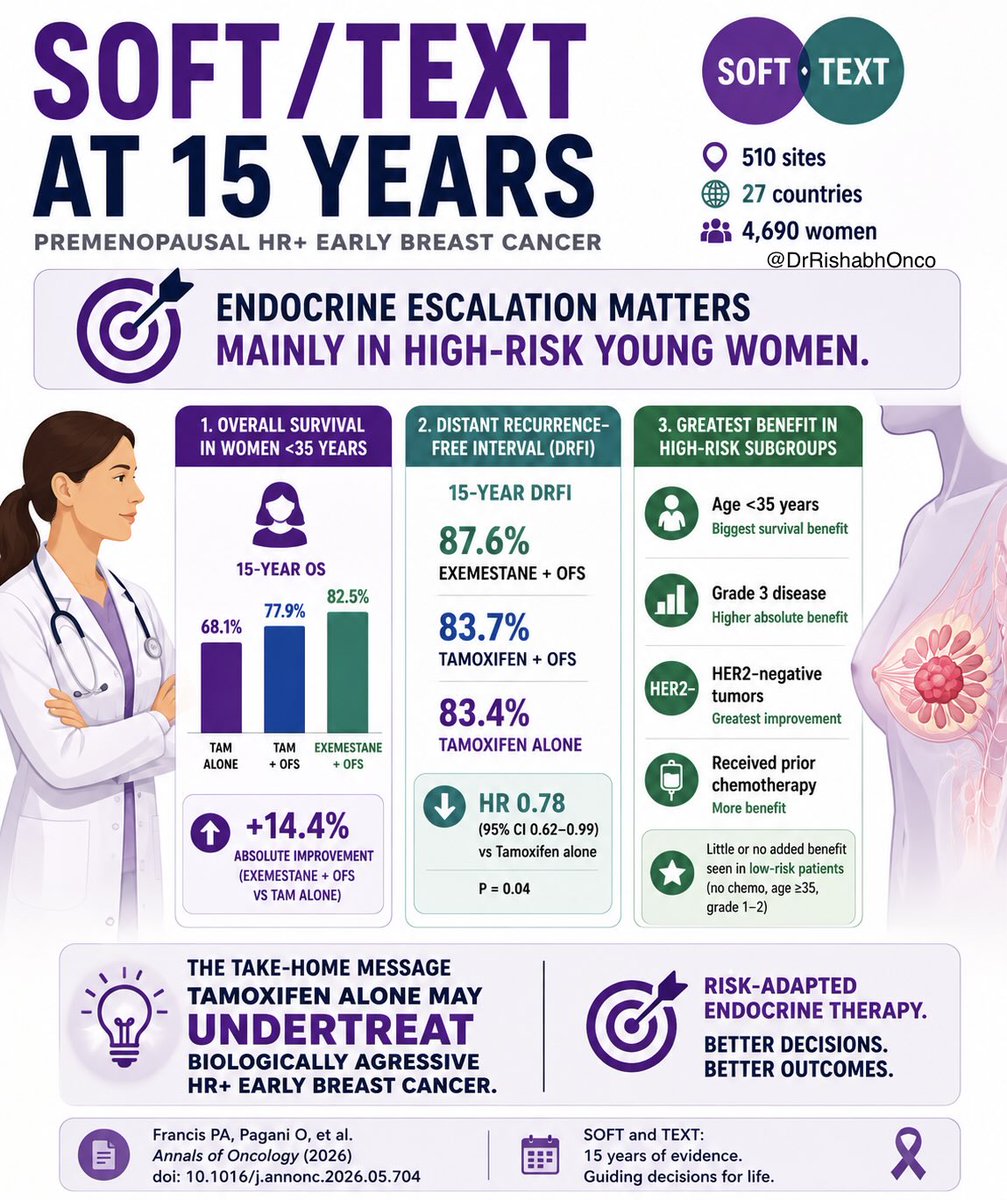
15-year SOFT/TEXT update confirms what many of us already sensed in clinic:
Not every premenopausal HR breast cancer needs endocrine escalation.
But the youngest, highest-risk patients absolutely do. 🎯
🔹 Exemestane OFS continued to reduce distant recurrence vs tamoxifen OFS
🔹 Biggest absolute benefit seen in:
• Age <35
• Grade 3 disease
• HER2-negative tumors
• Prior chemotherapy cohorts
In women <35 years with HER2-negative disease:
15-year OS:
➡️ 82.5% with exemestane OFS
➡️ 68.1% with tamoxifen alone
That is not a marginal difference.
The real message from SOFT/TEXT in 2026:
Risk-adapted endocrine therapy matters more than ever. 📈
#ASCO26 #bcsm #OncoTwitter @OncoAlert @myesmo @esmo_open @ASCO
43
101
4,126
Gladys Rodriguez,MD, FASCO retweeted

The most trusted voice in cancer care @ASCOPost It is an honor for me to be appointed as the Senior Deputy Editor of @ASCOPost The voice of @ASCO ! Grateful to the very talented editorial board, leadership of Dr. Jim Armitage EIC, @caraglynn01 and Angela Cochran!


12
14
90
8,472
Gladys Rodriguez,MD, FASCO retweeted

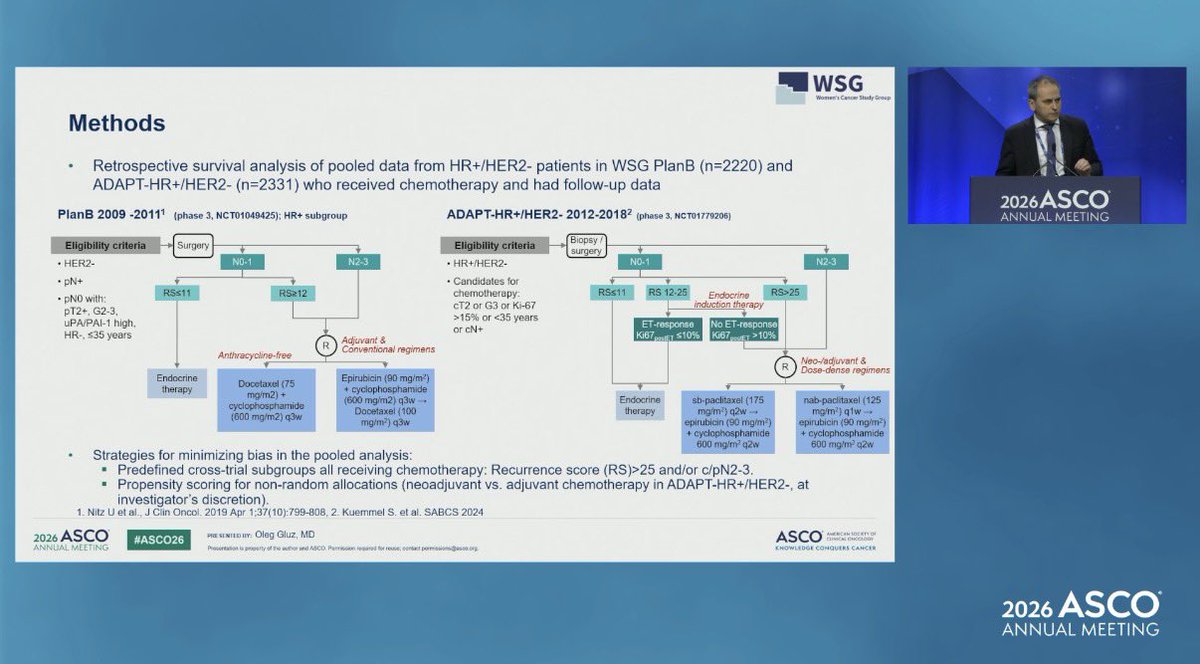
sometimes just giving patients a choice between what kind of chemo and letting them know this is better than none at all is more important that what type of regimen. This trial supports patient centric decisions

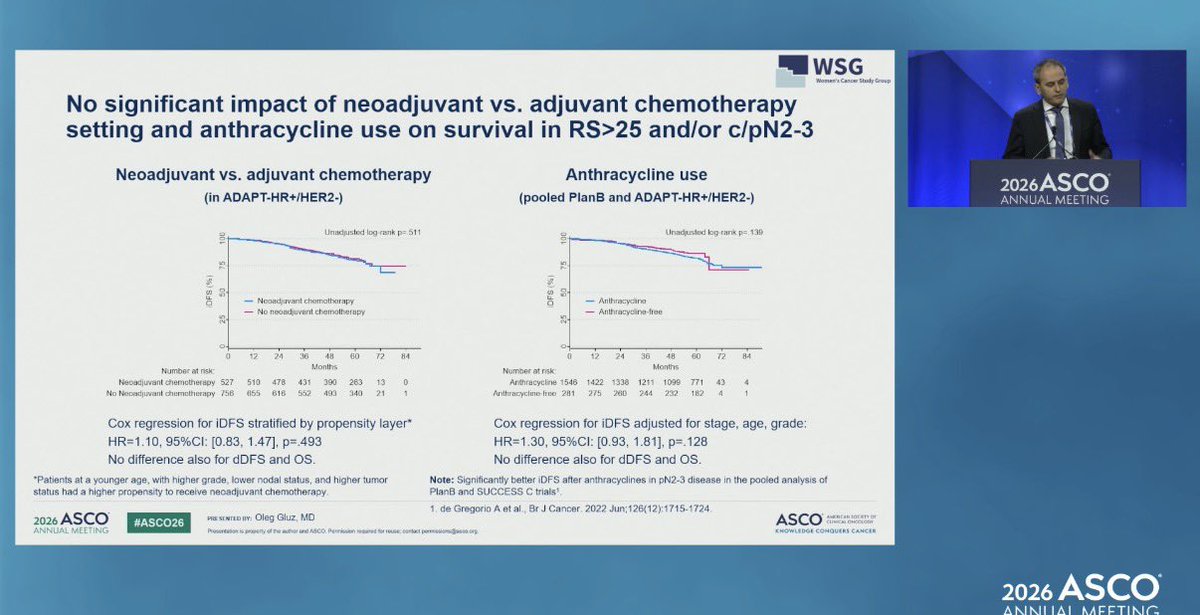
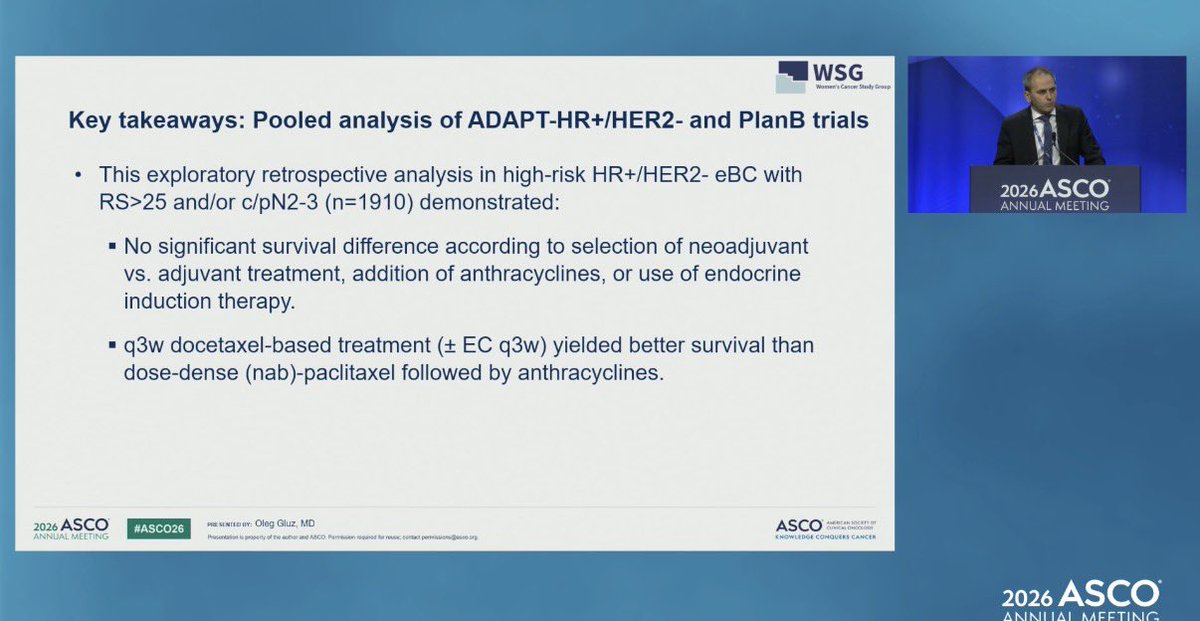
Pooled analysis of the WSG ADAPT-HR /HER2− and PlanB trials (n=1910) showed no survival differences according to neoadjuvant vs adjuvant chemotherapy, anthracycline use, or endocrine induction therapy in biologically high-risk HR /HER2− early breast cancer.
#ASCO26
2
2
691
Gladys Rodriguez,MD, FASCO retweeted

Jun 2
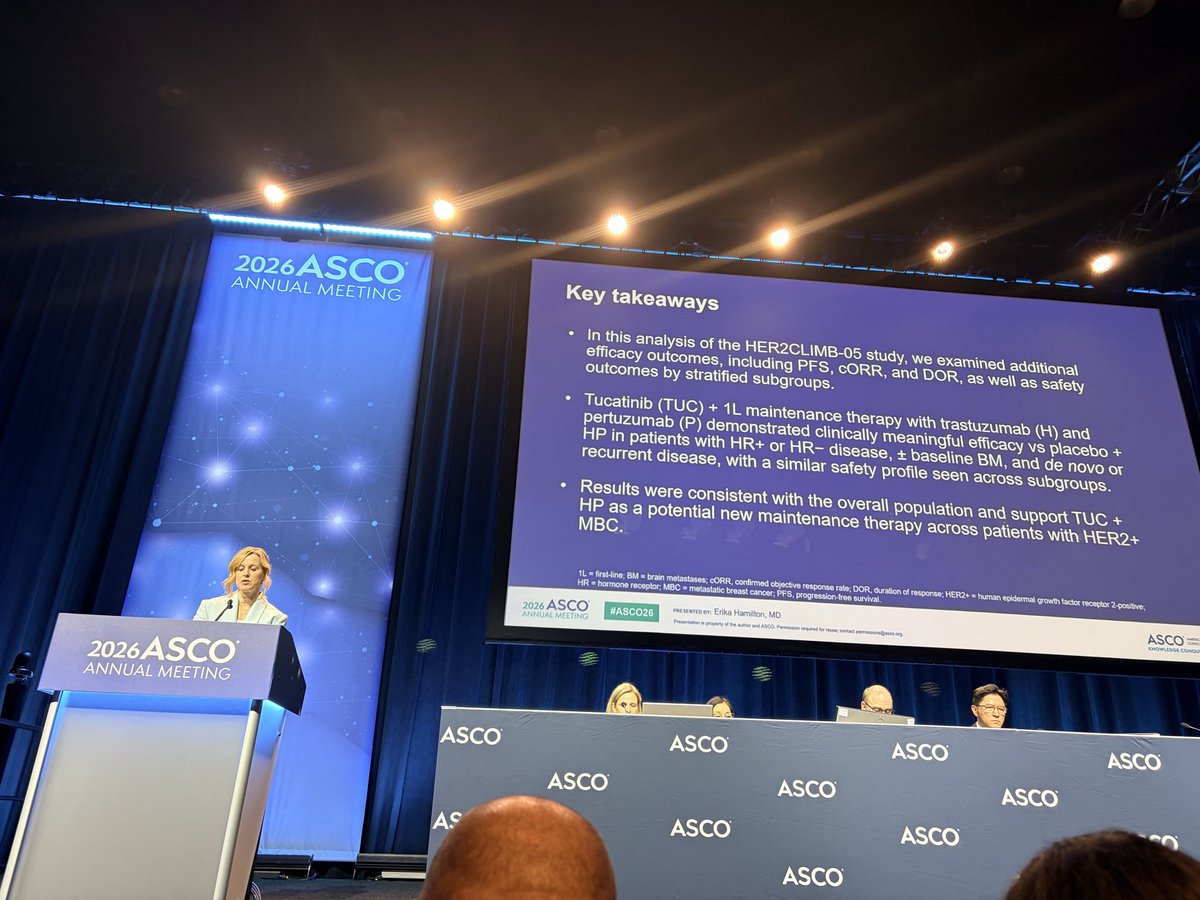
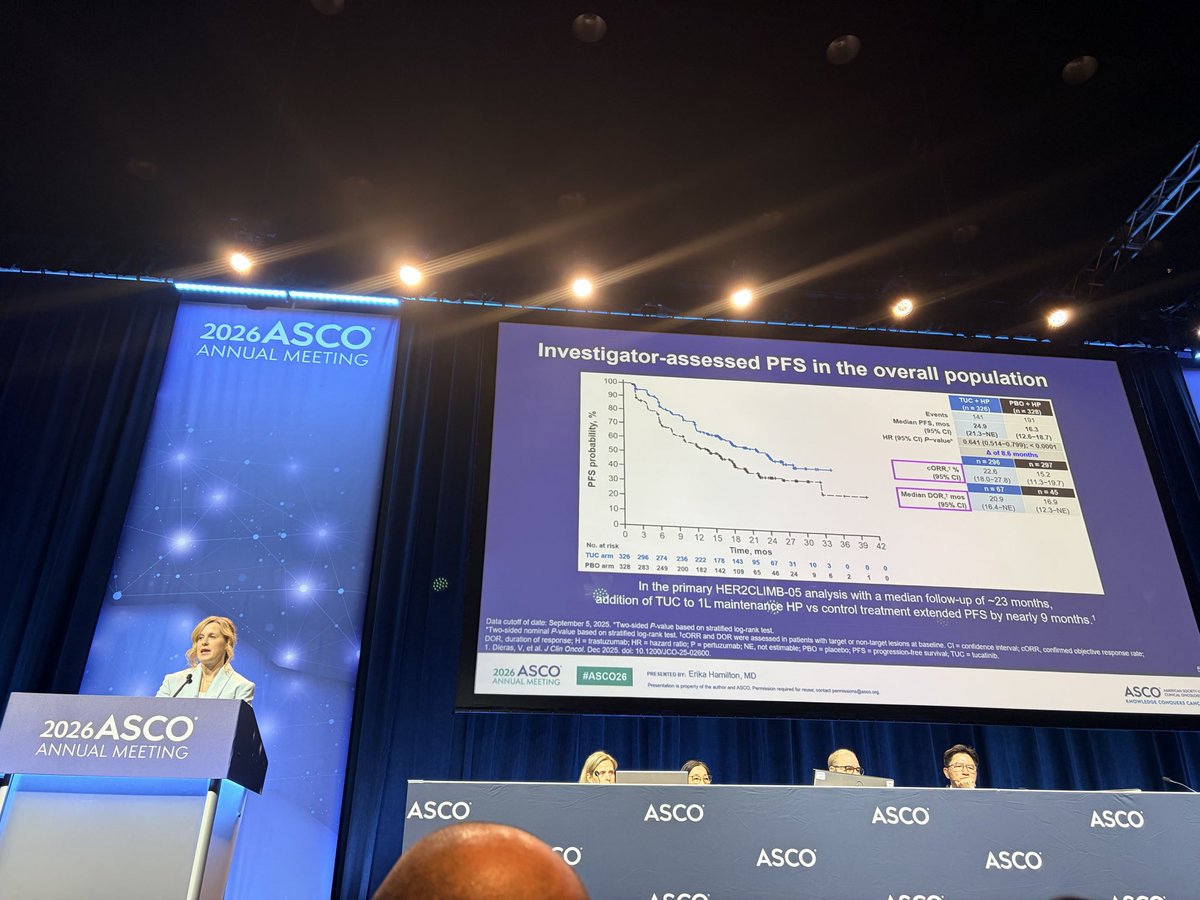
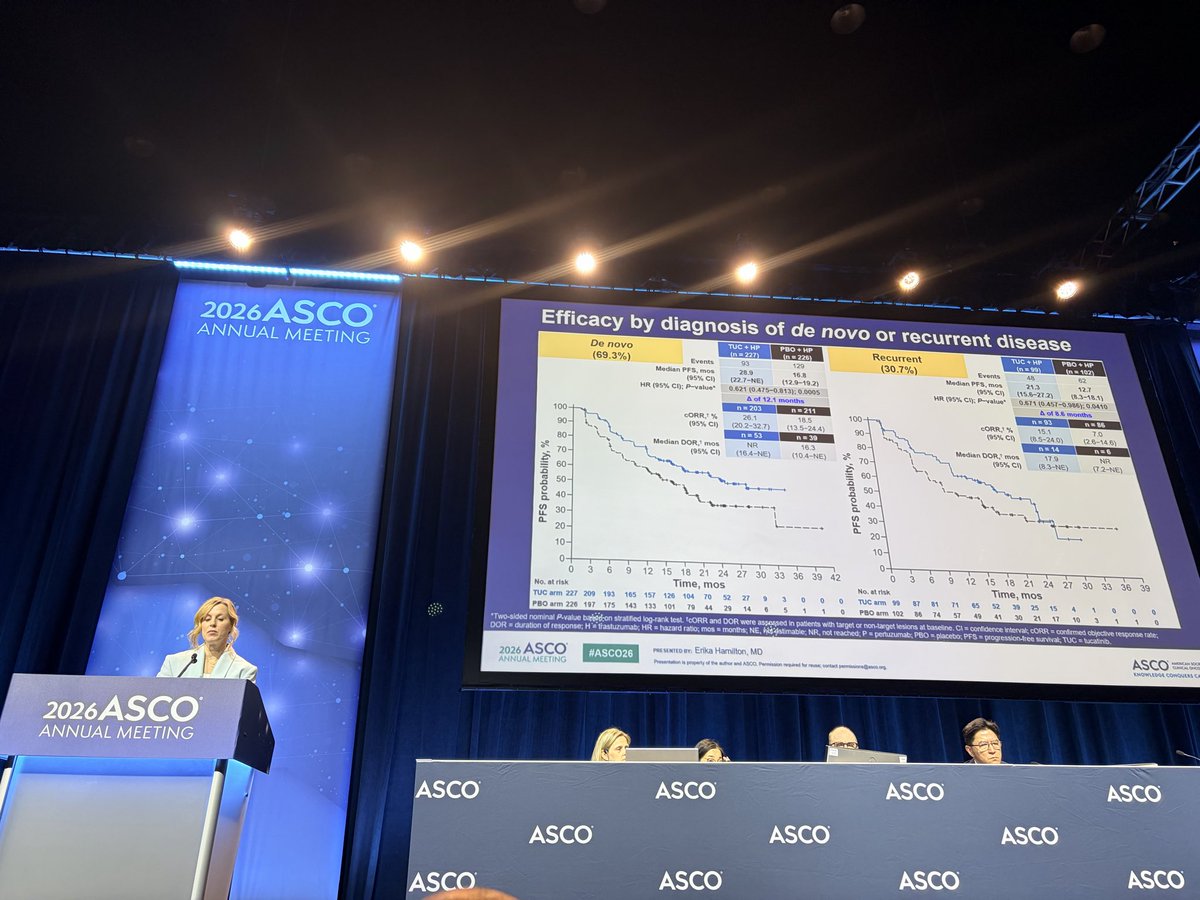
@ErikaHamilton9 beautifully presents additional efficacy and safety from HER2CLIMB05, at median follow up of 23 months mPFS was prolonged by 9 month. In HR- mPFS 12.6 mo improved to 24.9 mos, in HR , mPFS improved from 18.1 mo to 25 mo, those with and without baseline brains mets still derived benefit, and denovo and recurrent disease also still derived benefit. No new safety signals. @OncoAlert
@SCRIOncology @SarahCannonDocs

1
8
19
954
Gladys Rodriguez,MD, FASCO retweeted

These are really clinically relevant and practice changing data on how to optimize #denosumab use in patients with bone metastases: induction with 4 monthly administrations then every 3 months
#ASCO26 @ASCO @OncoAlert @valeguarneri
Jun 2

Dear Colleagues at #ASCO26
A great way to end this final day of the meeting that with a presentation straight from the Podium to your feed.
@OncoAlert proudly presents Dr. Roger Von Moos 🇨🇭who just presented Abs 1004 at ASCO:
Prevalence of symptomatic skeletal events (SSE) with reduced denosumab (Dmab) dose density (every 12 weeks versus every 4 weeks): A randomized phase III non-inferiority trial SAKK 96/12 REDUSE.
The phase III SAKK 96/12 REDUSE trial randomized 1,380 patients with bone-metastatic breast cancer or castration-resistant prostate cancer to denosumab 120 mg every 4 weeks or, after a 3-month loading phase, every 12 weeks. The reduced-frequency schedule was non-inferior for preventing symptomatic skeletal events, with similar efficacy and lower rates of hypocalcemia and osteonecrosis of the jaw. These findings support every-12-week denosumab as a new standard of care, reducing toxicity, treatment burden, and costs.
@Silke_Gillessen
@RothschildSacha
@DrChoueiri 🇺🇸 @hoperugo 🇺🇸 @matteolambe 🇮🇹 @TiansterZhang 🇺🇸 @CathyEngMD 🇺🇸 @stolaney1 🇺🇸 @montypal 🇺🇸 @tompowles1 🇬🇧 @brian_rini 🇺🇸 @cdanicas 🇪🇸 @NiuSanford 🇺🇸 @amerseburger 🇩🇪 @GlopesMd 🇺🇸 @Icro_Meattini 🇮🇹 @PGrivasMDPhD 🇺🇸 @DrYukselUrun 🇹🇷 @nataliagandur 🇦🇷 @ElisaAgostinett 🇧🇪 @HHorinouchi 🇯🇵 @realbowtiedoc 🇺🇸 @to_be_elizabeth 🇮🇹 @UOzkerim 🇹🇷 @p_ciracimd 🇮🇹 @DrVilmaPBarcia 🇪🇸 @DraMartinezLago 🇪🇸 @DrMirallas 🇺🇸 @GaiaGriguolo 🇮🇹 @MarioBalsaMD 🇪🇸 @scocmem 🇬🇧 @AmandaNizamMD 🇺🇸 & @weoncologists 🇺🇸 @APCCC_Lugano @AOmlin
11
29
2,794
Gladys Rodriguez,MD, FASCO retweeted
#ASCO26 Great dinner with Women in Thoracic Oncology. Grateful to share ideas, mentorship, and friendship with such an inspiring group of leaders. @ASCO is not only about science and innovation, but also about lifting each other up and building community. #WomenInOncology #LungCancer #SheforShe

3
17
711
Gladys Rodriguez,MD, FASCO retweeted

Jun 2
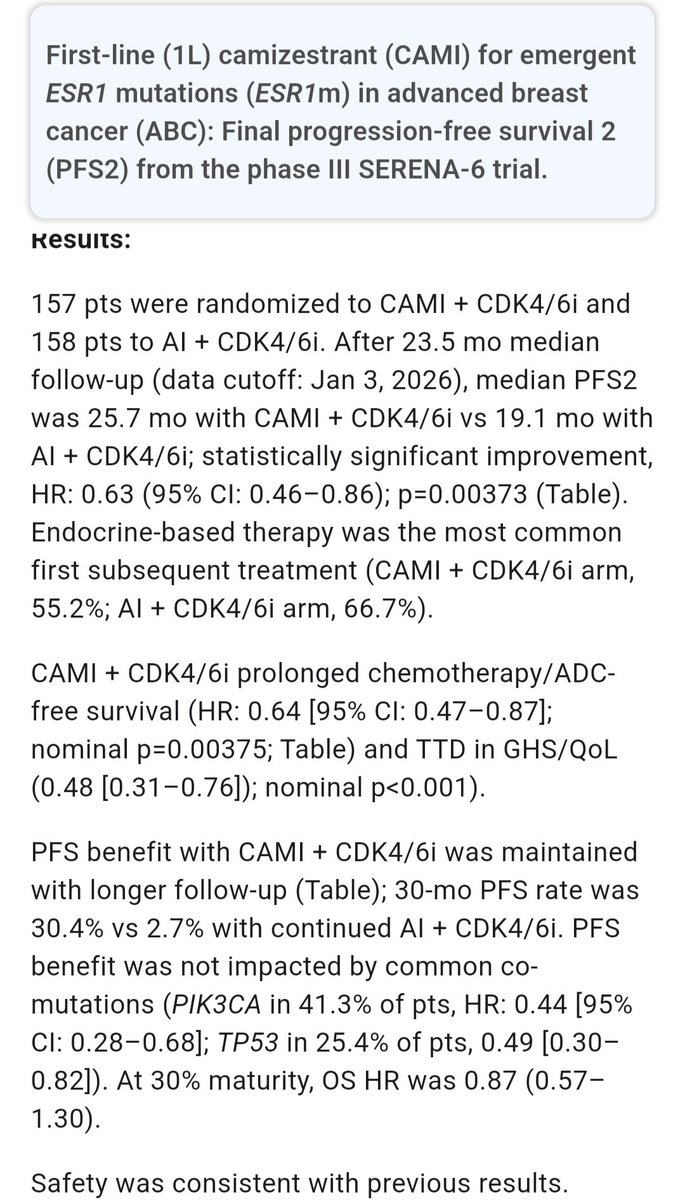
#ASCO26 | SERENA-6
Early switch to camizestrant CDK4/6i at the emergence of an ESR1 mutation also improved PFS2 versus continuing AI CDK4/6i.
PFS2: 25.7 vs 19.1 months✅️
HR 0.63, p=0.0037
The strategy is reasonable: intervene with ctDNA before waiting for radiologic progression.
But there is a design issue: if crossover to camizestrant at radiologic progression had been mandatory, we could have understood the true value of early switching at molecular relapse much more clearly.
Looking forward to the discussion.
1
10
24
5,305
Gladys Rodriguez,MD, FASCO retweeted
Jun 2
This excellent #asco26 ed session on Time to Trial Activation featuring @FDAOncology @NCIDirector @KimrynRathmell & @Dee_Anna_Smith is available around the paywall - scroll down in this link: (and watch opening ceremony and @ASCO Voices talks as well!)
asco.org/annual-meeting/prog…

4
5
21
884
Gladys Rodriguez,MD, FASCO retweeted

My #ASCO26 #FitCheck: spent Day 4 PM & Day 5 AM streaming sessions in my PJs from my hotel room while catching up on clinical work. I'm happy to have phenomenal colleagues who help cover for small acute issues but in the last 24 hrs I've had 8 plans due. 😅☢️🛠️⚡️🩻#ASCOFashion

1
24
815
Gladys Rodriguez,MD, FASCO retweeted
#ASCO26 I never imagined that in the middle of my career I’d be reporting on cancer research advances and helping make them understandable for the lay public—in both English and Spanish. Grateful for the opportunity. @Lung_Cancers @sylvestercancer #CancerResearch #MedTwitter

3
25
1,213
Gladys Rodriguez,MD, FASCO retweeted
I've waited all #ASCO26 to finally spend time with Dr @NarjustFlorezMD and now it's TIME. 🤜⚡️🤛

4
31
1,094
Gladys Rodriguez,MD, FASCO retweeted
Jun 2
As #asco26 comes to a close, I think the highlight for me was connecting w/3 of my prior @ConquerCancerFd @asco IDEA mentees: Nico from Romania, Yanin from Mexico, & Anyur from Kazakhstan. All 3 have become amazing oncology leaders & are improving cancer care globally. So proud!

10
49
1,813