
Hepatologist & Therapeutic Endoscopist @VCUHealth🏫| EBM snob |Coffee☕️ Afficionado| Views my own, not of my employer| youtube.com/@sahajrathi
Joined September 2009
- Tweets 2,867
- Following 852
- Followers 3,105
- Likes 6,993
493 Photos and videos










Pinned Tweet

21 Sep 2023
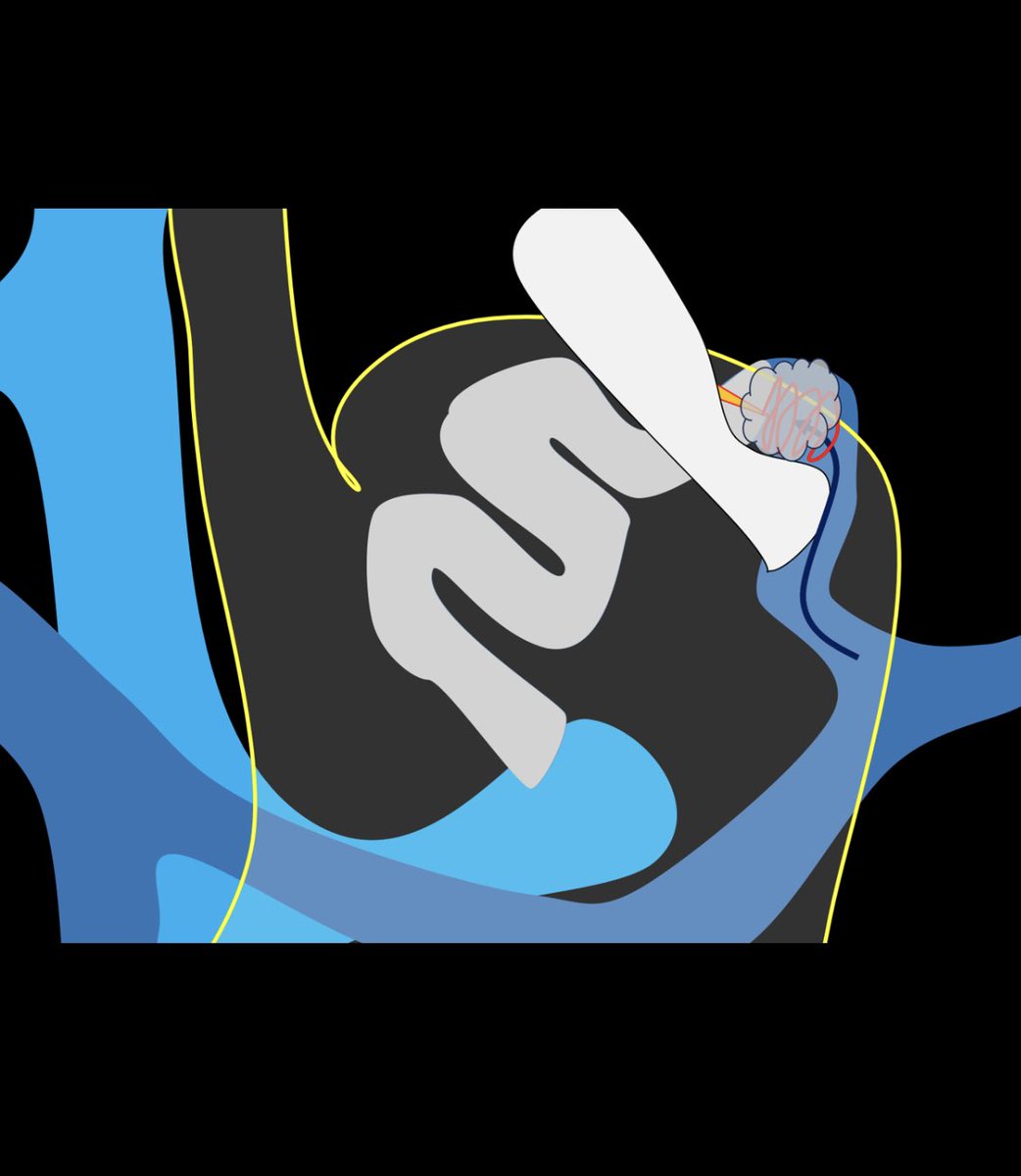
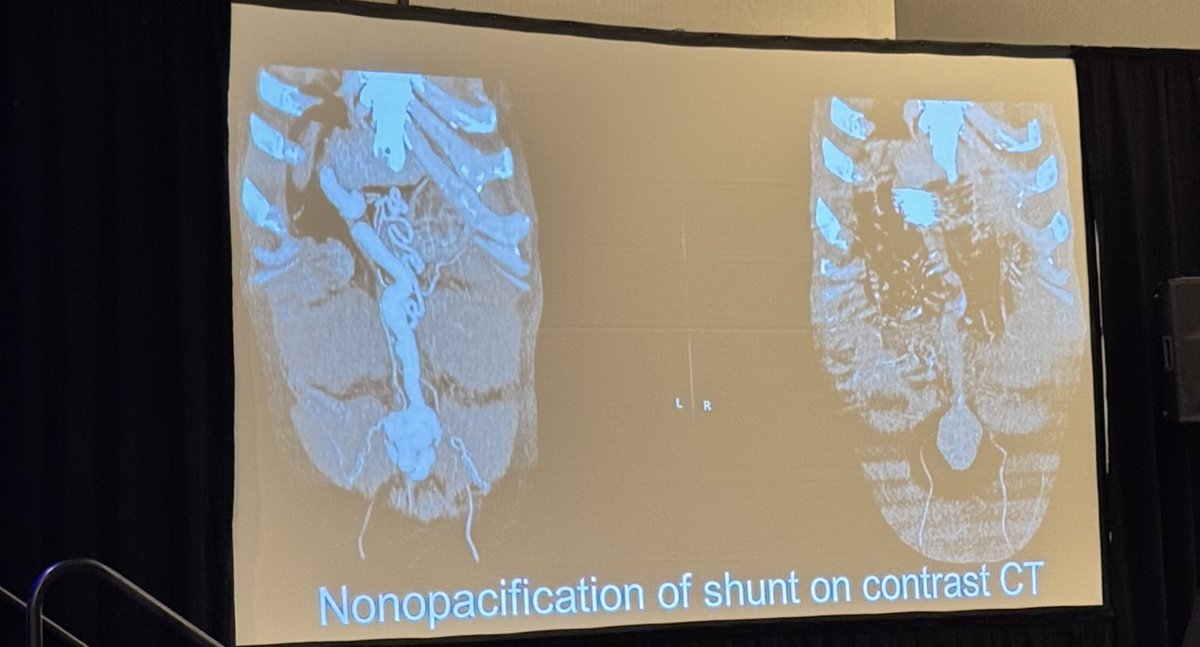
#EUS guided Transgastric Shunt Obliteration- a novel technique to block shunts for difficult to treat Hepatic Encephalopathy
Supplementary data out now, contains:
👉Video of the technique
👉Case details
👉EEG data
Video link:cdn-links.lww.com/permalink/…
#Endohepatology #GITwitter
18 Aug 2023

🔥Hot off the press🔥
Excited 🤩to share our novel technique - EUS guided Transgastric Shunt Occlusion (#ETSO) is out now
An excellent alternative to BRTO for portosystemic shunts, ETSO is
👉 Faster
👉 Less expensive
👉 No need for fluoroscopy suite
doi.org/10.14309/ajg.0000000…
11
18
85
26,206
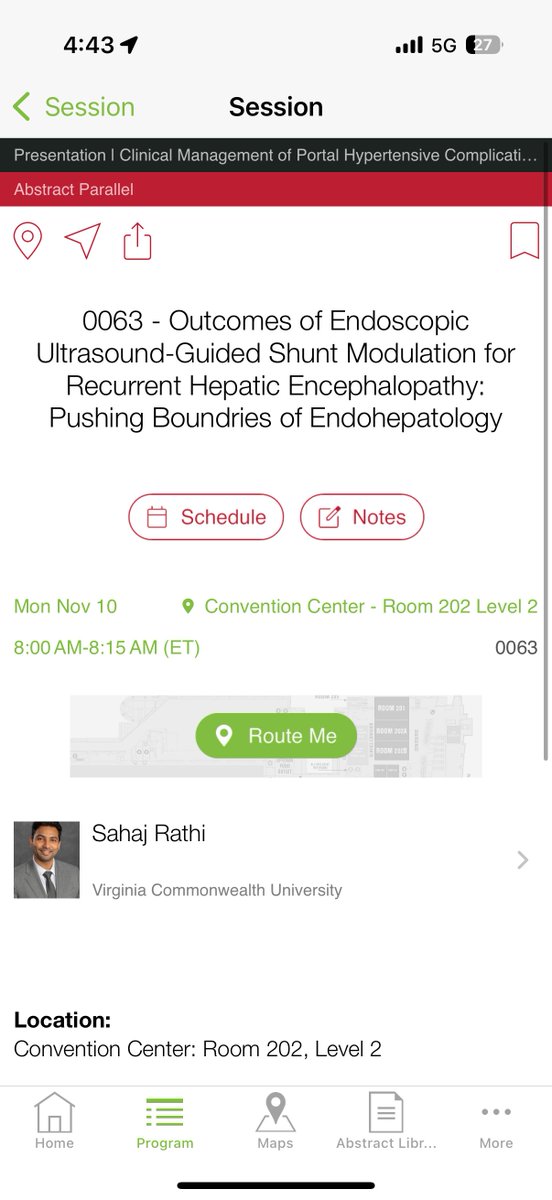
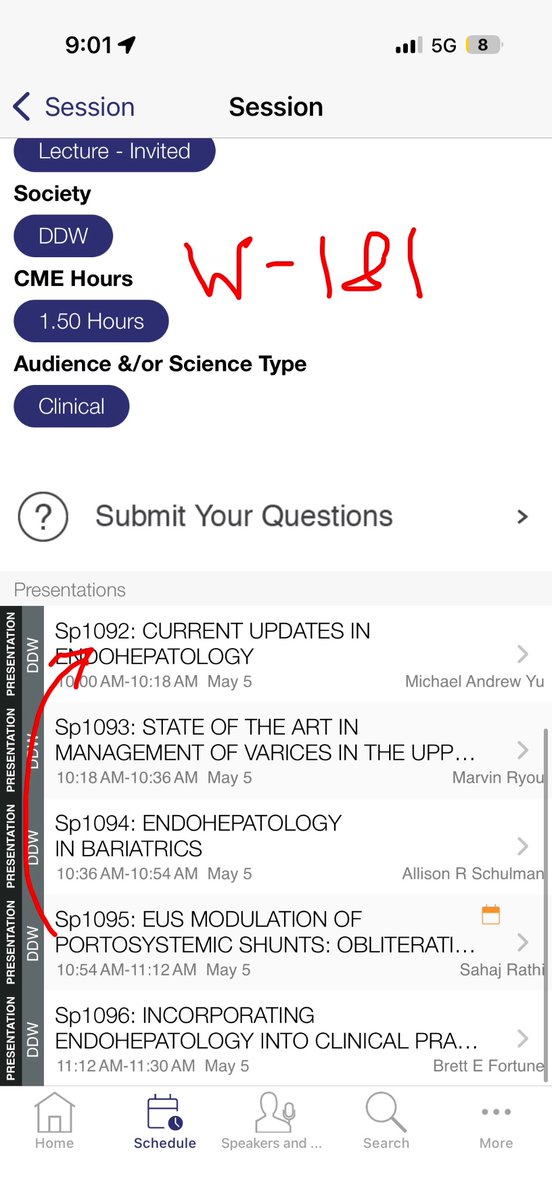
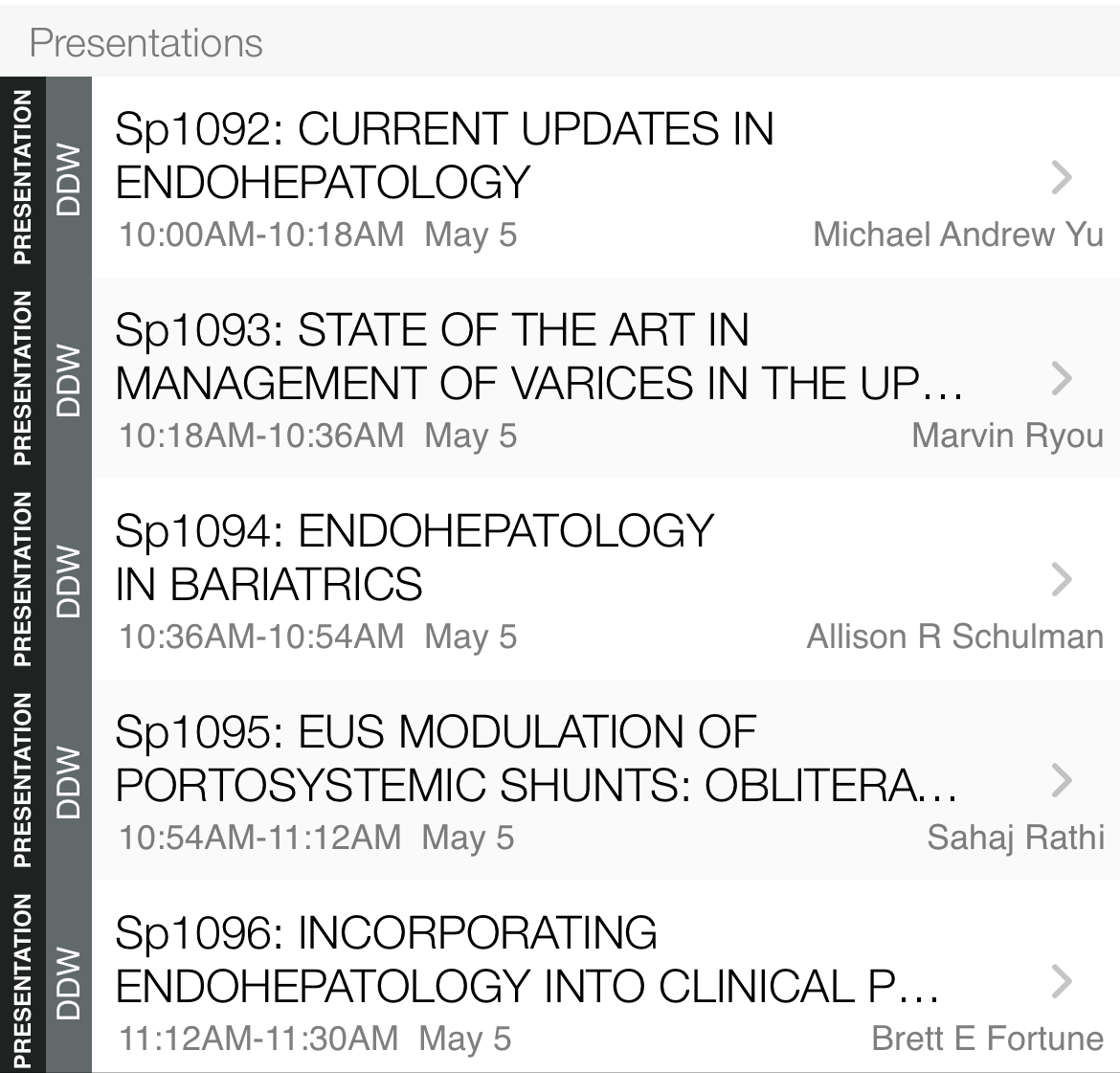
At #DDW2026? Interested in Gastric Varices and Portosystemic Shunts?
Swing by these halls. I shall try to cover the nuances of how #EUS can maage both these complications of portal hypertension! #EndoHepatology
Note the change in time:
10am, W181(ASGE)
EUS guided shunt modulation in cirrhosis
10.40am, W194(AGA)
EUS guided Gastric variceal obliteration
Biliary focus? Check this out:
11.45am, ASGE learning center
Cholangioperitoneoscopy in complex biliary injury
#GITwitter #Endoscopy

2
39
1,289
Sahaj Rathi MD, DM, MRCP retweeted

Looking forward to moderating tomorrow's @ASGEendoscopy endohepatology SIG-sponsored symposium titled "Endohepatology: Current Updates and Future Directions" alongside @AlyssaChoiMD . This has historically always been a packed room with audience. We have a great lineup tomorrow with outstanding speakers/talks. Hoping to see many of you there! @DDWMeeting
@allie_schulman @SahajRathi @BrettEFortuneMD @michaelandrewyu
1
4
17
2,385
Sahaj Rathi MD, DM, MRCP retweeted

Mar 21
30th Virginia Liver Symposium and Updates in Gastro by @VCUHealth:
@tariqraseen discussing managing IBS in IBD
📌 IBS like symptoms common in IBD remission
🚫 Exclude ongoing inflammation (FC, CRP)
🧀 Food is most common trigger of IBS: dairy, gluten, wheat, high FODMAP, ☕️, 🍻
💊 Treat with IBS related pain: antispasmodics, peppermint oil
🔍 Recognising IBS-IBD overlap avoids escalation of biologics
@VCU_Liver @AmCollegeGastro @AmerGastroAssn @CrohnsColitisFn


5
20
1,468
Sahaj Rathi MD, DM, MRCP retweeted
Mar 21
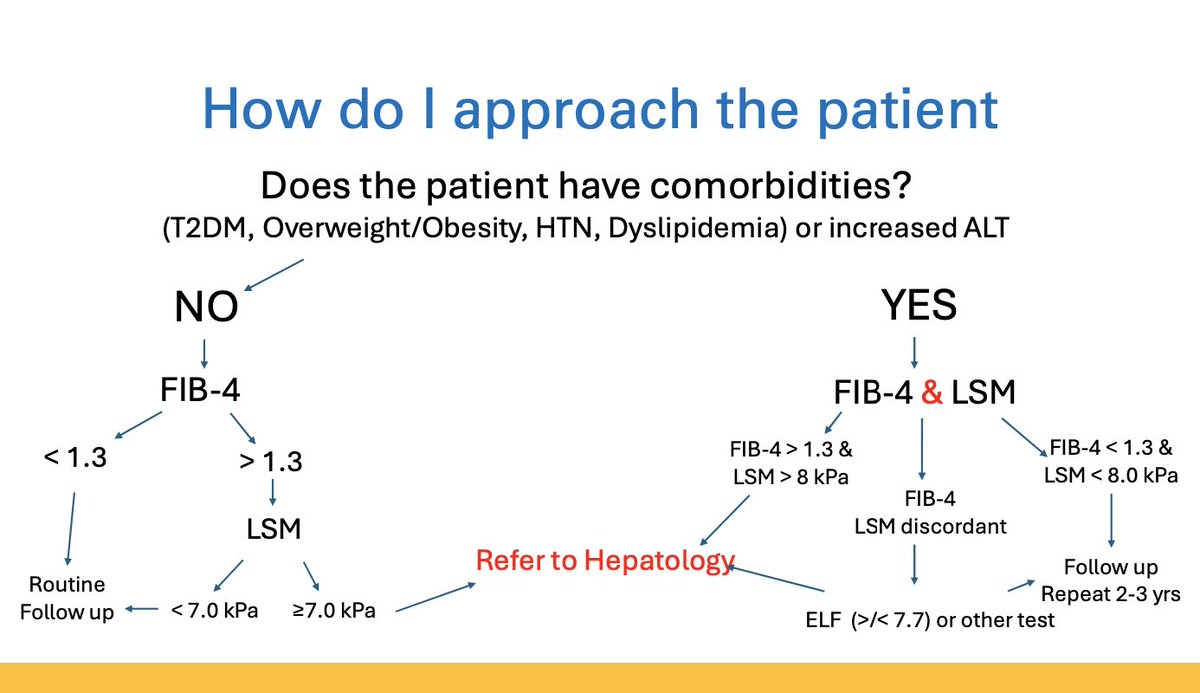
Prof @RichSterlingMD with pro-tips for non-invasive liver disease assessment (NILDA) tools at @VCUHealth Liver Symposium
🩸Blood based NILDA good at ruling out advanced fibrosis (FIB-4, ELF, APRI etc)
👎 However they’re suboptimal at identifying F2-F3
📌 Up to half of those who need Rx (F2-F3) missed if you use FIB-4<1.3 to decide who needs Rx
➕ Use combination of NILDA for assessment (blood based imaging)
📌 in age>65, use FIB-4 threshold of 2 (instead of 1.3)
@VCU_Liver @AmCollegeGastro @AmerGastroAssn @AASLDtweets @EASLedu @INASL_Liver @LiverFellow

7
23
1,795
Sahaj Rathi MD, DM, MRCP retweeted
Mar 21
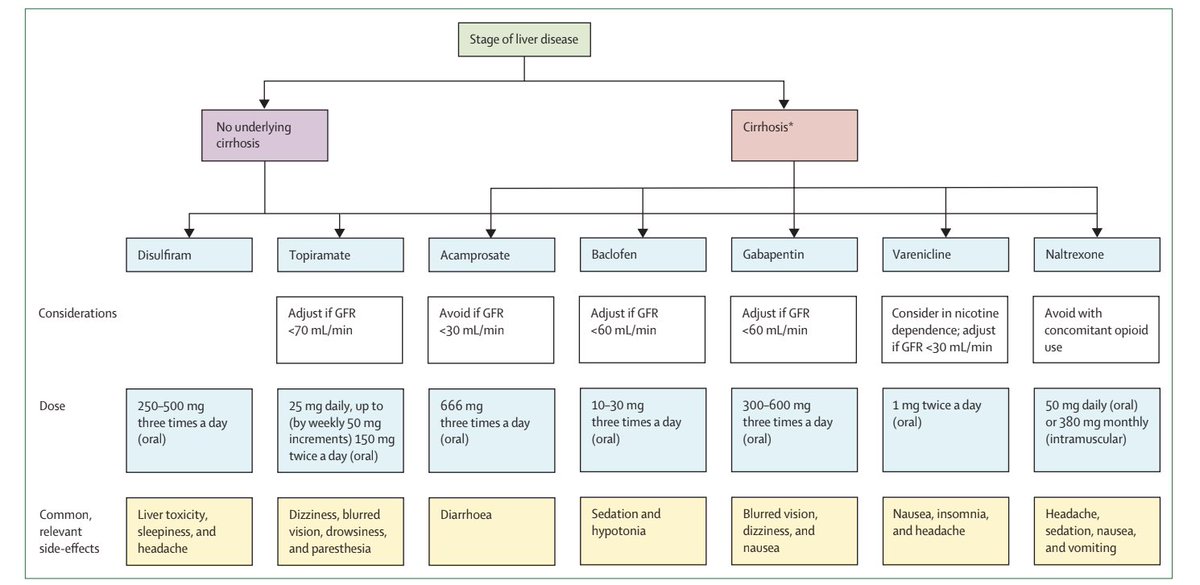
Prof @juanpabloarab shedding light on ALD at @VCUHealth Liver Symposium
🥃 Risk of liver decompensation ALD>MASLD for same fibrosis stage
☠️ Alc-hepatitis 3-month mortality is 40%
💊 Best benefit for steroids in alc-hep with MELD 25-39. MELD outperforms MDF for steroid response
👍 Acamprosate NNT for AUD is 12 (for reference, NNT with PPI for PUD bleeding is 15)
@VCU_Liver @AASLDtweets @liverUSA @AmCollegeGastro @AmerGastroAssn @EASLedu @INASL_Liver @ASRG_Liver @LiverFellow

2
8
27
1,982
Sahaj Rathi MD, DM, MRCP retweeted
Mar 21
All eyes on the screen for @SahajRathi giving us a glimpse into the realm of endohepatology at @VCUHealth Liver Symposium and GI updates!
Gastric variceal management…Shunt obliteration…Gall bladder drainage…Liver bx…Tumor ablation…Abscess and cyst drainage…nasobiliary drainage…
Skill innovation 👏
@VCU_Liver @ASGEendoscopy @AmCollegeGastro @AmerGastroAssn @AASLDtweets @EASLedu @LiverFellow @INASL_Liver
1
3
25
1,471
27 Dec 2025
#POCUS for HPB medicine/therapeutic endoscopy
Quick and effective focused assessment for key 🔑 clinical questions
A Tweetorial 📹🧵
#GITwitter #endoscopy #ERCP #EUS
2
6
25
2,914
27 Dec 2025
5⃣ Is there a bleed? Assessing hepatogastric interface after EUS liver biopsy
Especially if
❗️Cirrhotic liver
❗️Suboptimal coag profile
❗️>1 pass
I personally feel reassured assessing this at 3-4hr mark.
This is where a hematoma would show up
x.com/i/status/1816821793681…
26 Jul 2024
Cirrhosis - Identifying irregular liver outline on ultrasound
I believe all GI units should have at least one bedside ultrasound
Trainees should try to learn #POCUS and use it as an extension of their clinical evaluation
Views #LiverTwitter #GITwitter?
1
1
607
27 Dec 2025
That’s a wrap!
There are multiple other nifty applications of #POCUS in therapeutic endoscopy, but these are the ones I find most useful
Any other uses #GITwitter?
5
292
Sahaj Rathi MD, DM, MRCP retweeted

16 Dec 2025
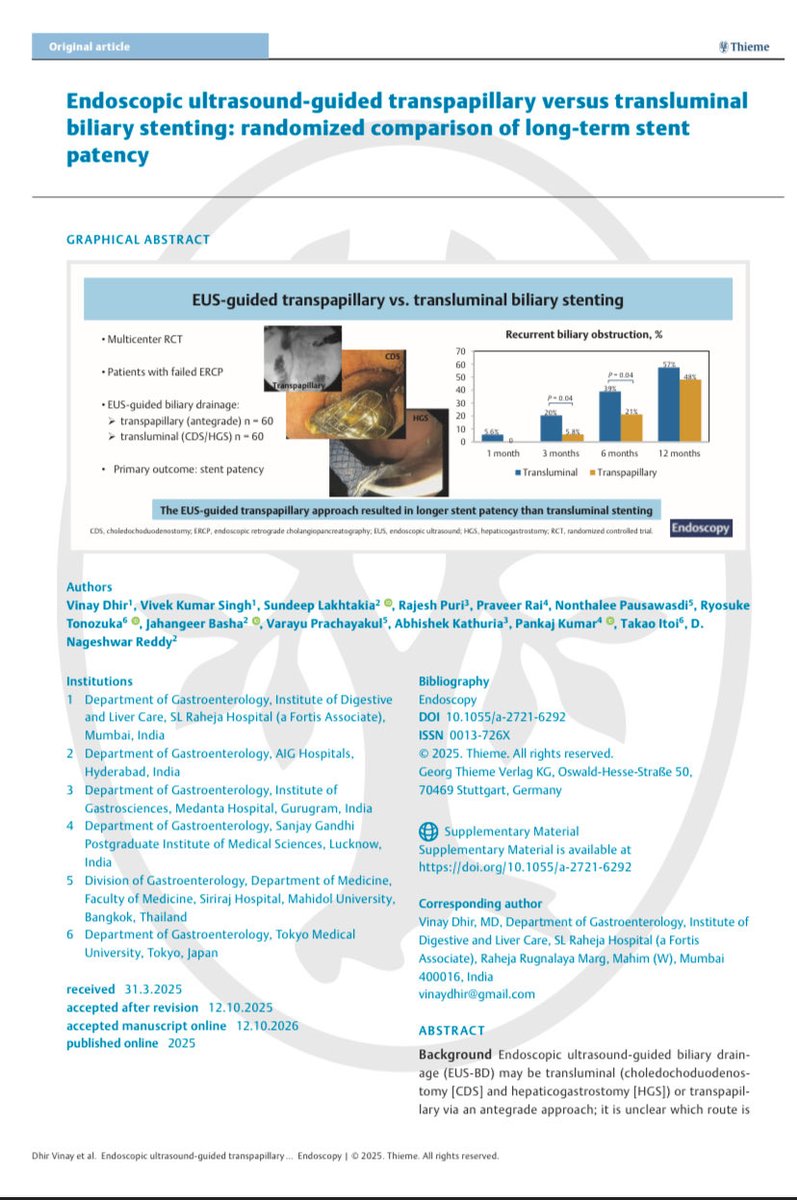
Published online in endoscopy
1
6
45
2,675
Sahaj Rathi MD, DM, MRCP retweeted

6 Dec 2025
🌟 Exciting 4 days at ISGCON 2025, Amritsar wrapped up 🌟
👉🏻 Power-packed academic sessions & brilliantly delivered lectures
👉🏻Excellent clinical discussions
👉🏻Strong focus on DM/DNrB training challenges and changing landscape of women in GI 🔥
Won 🏆 in Endoscopy clinics 🙌🏻
@ajay_duseja @DrMaheshgoenka @drsuniltaneja @docMPK @drnipunverma @doc_arka @RoyAHep @HepatologyPGI @DrHarpreet20210


9
3
24
1,091
4 Dec 2025
Many many congratulations @RoyAHep and @AnandVKulkarni2 !! 🤩🤩

Humbled to be awarded the OP Memorial Rising Star Award at ISGCON 2025. Moments like these rekindle why the journey is worth it.
Grateful to all my mentors, colleagues and patients
🥂 to @AnandVKulkarni2 for winning the SR Nayak Researcher Award
🎗️Award twinning mode on✨




11
839
Sahaj Rathi MD, DM, MRCP retweeted
29 Nov 2025
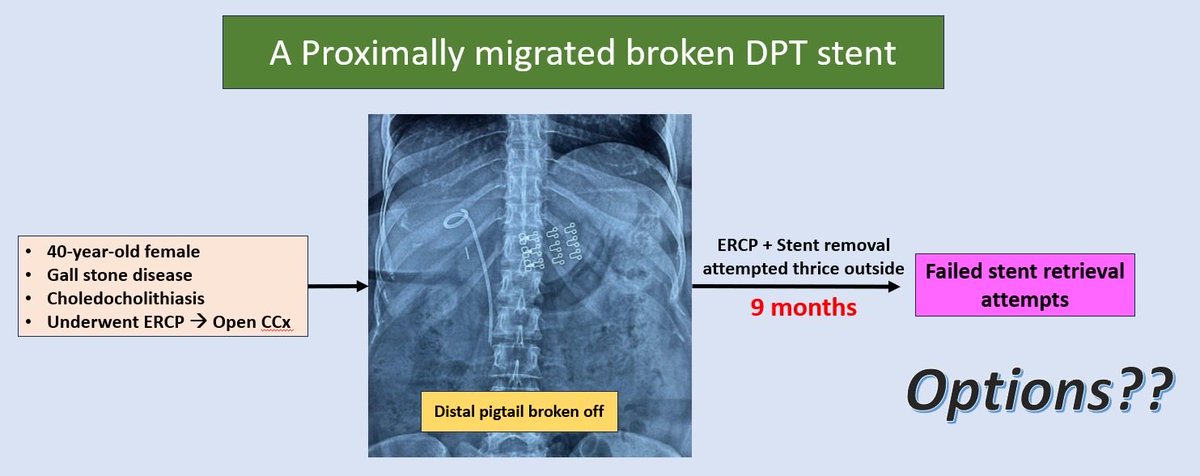
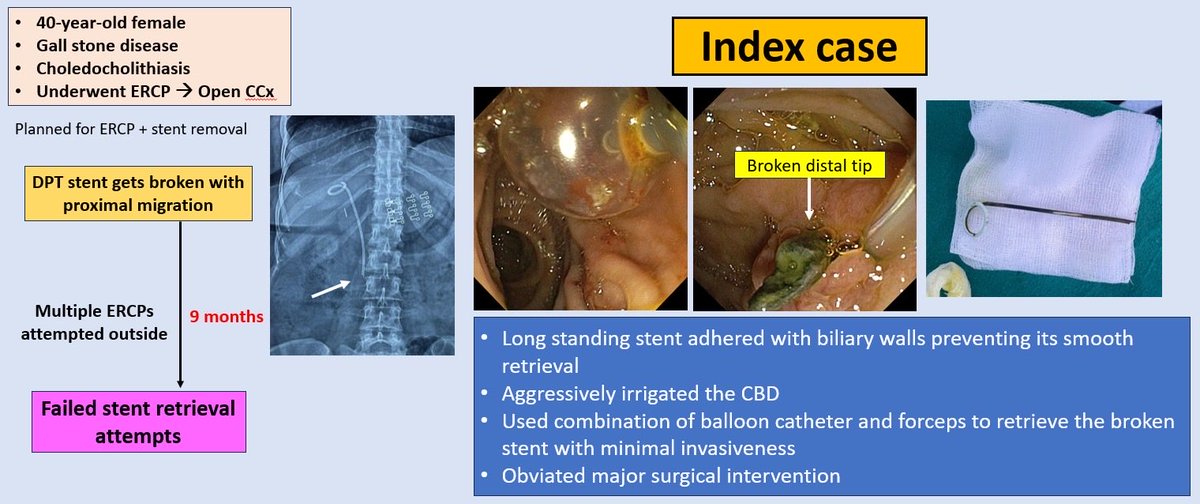
❌ PROXIMALLY MIGRATED BROKEN BILIARY STENT ❌
👉🏻A 40 year old female post-cholecystectomy was planned for stent removal.
👉🏻Xray showed broken distal pigtail with proximally migrated stent
🎈 Failed multiple attempts outside
🎈 Challenging scenario 🔥
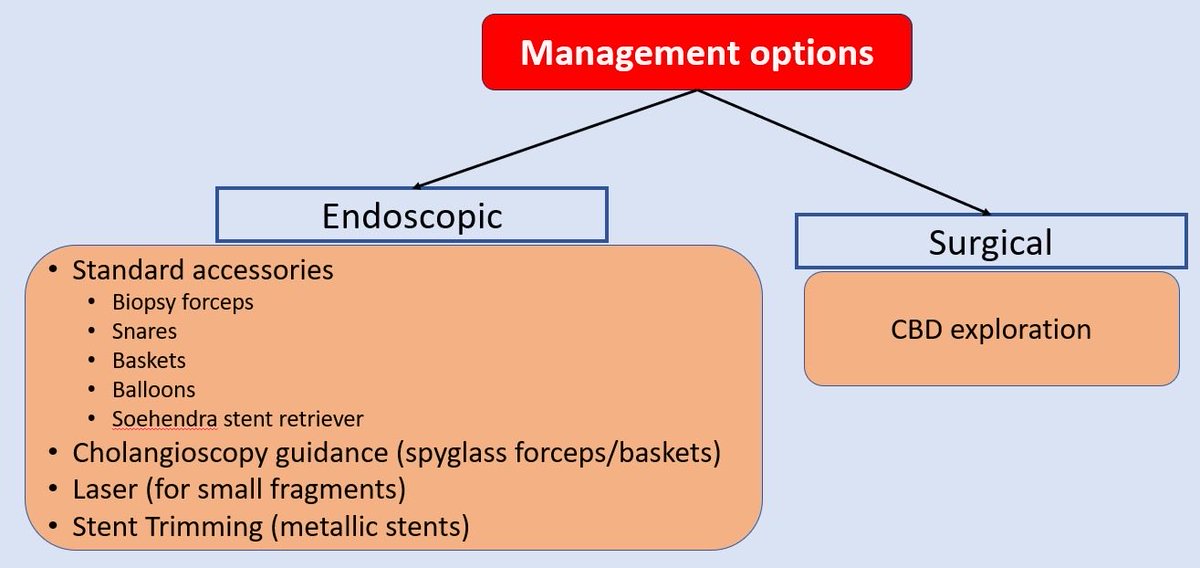
🎈 Advised surgical CBD exploration
🎈 Patient distress 😪
What your experience and possible salvage methods??
2
7
13
1,257
Sahaj Rathi MD, DM, MRCP retweeted

17 Nov 2025
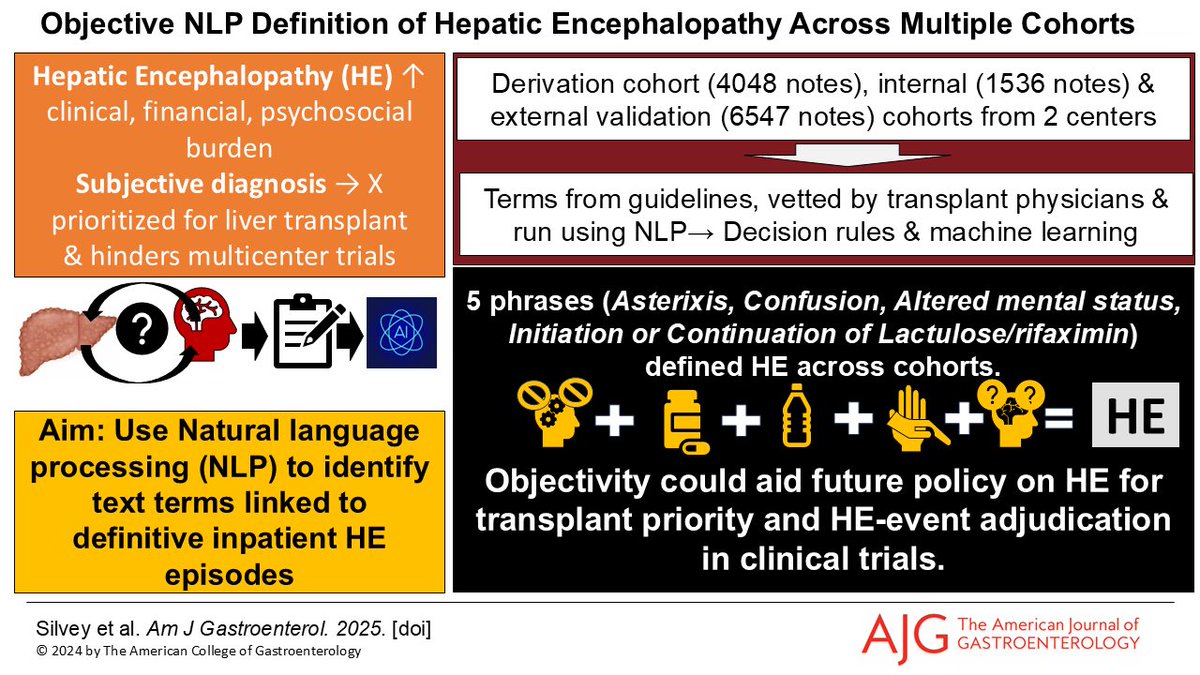
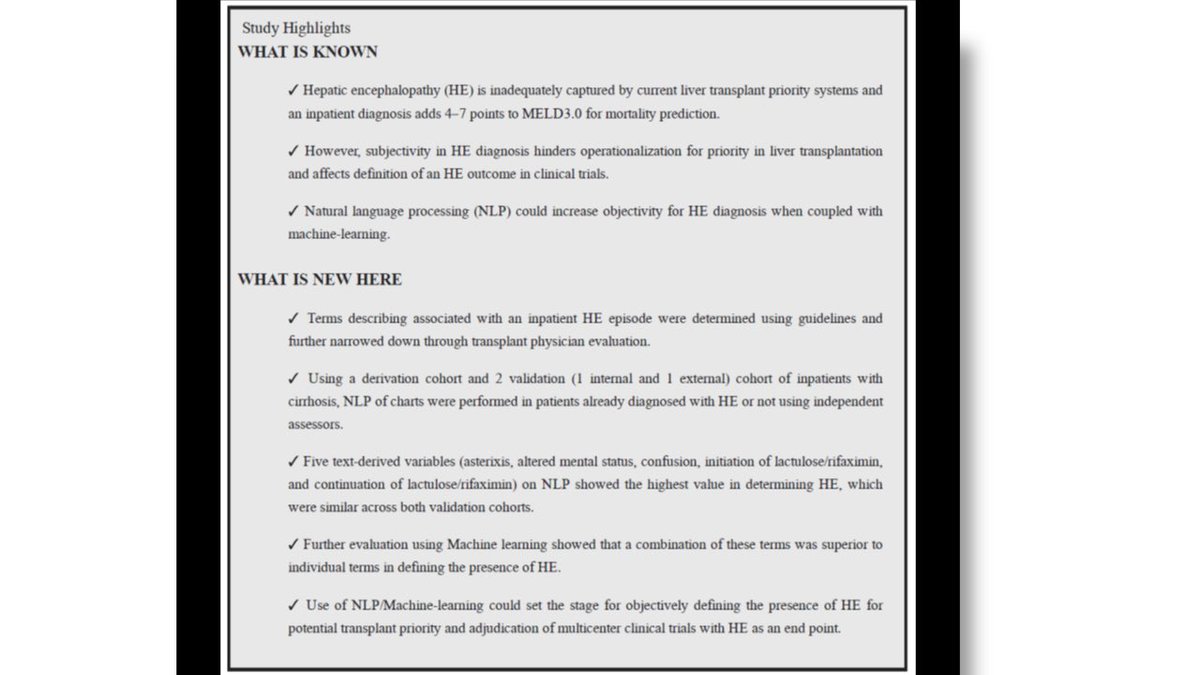
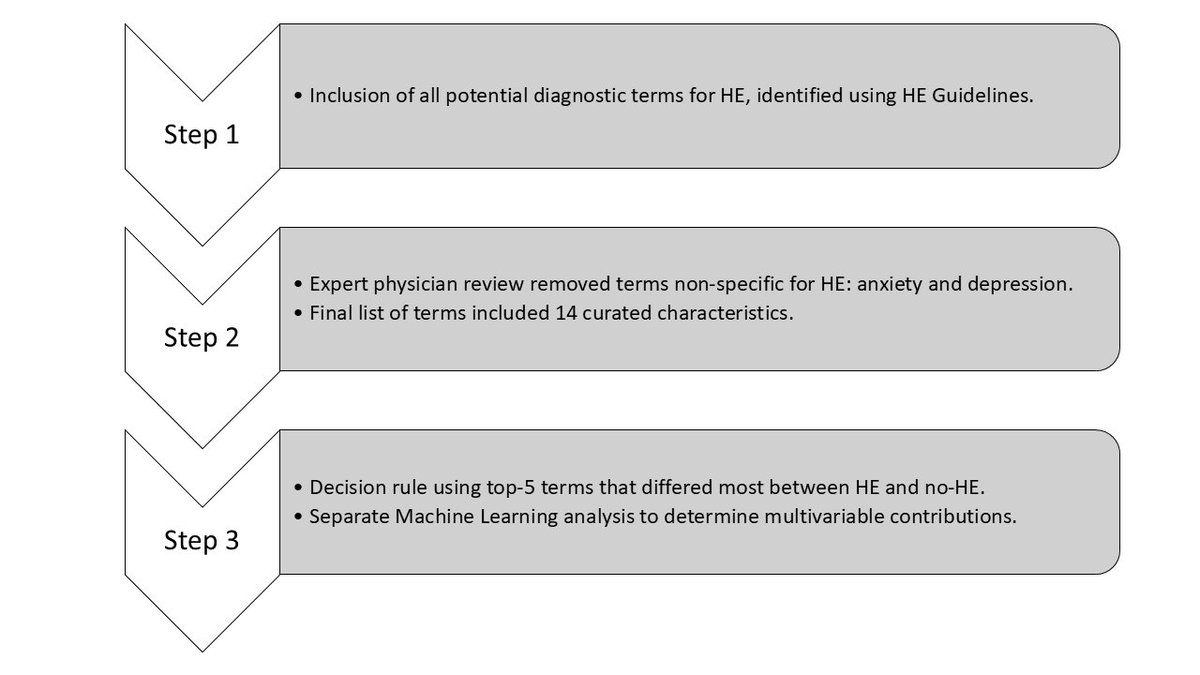
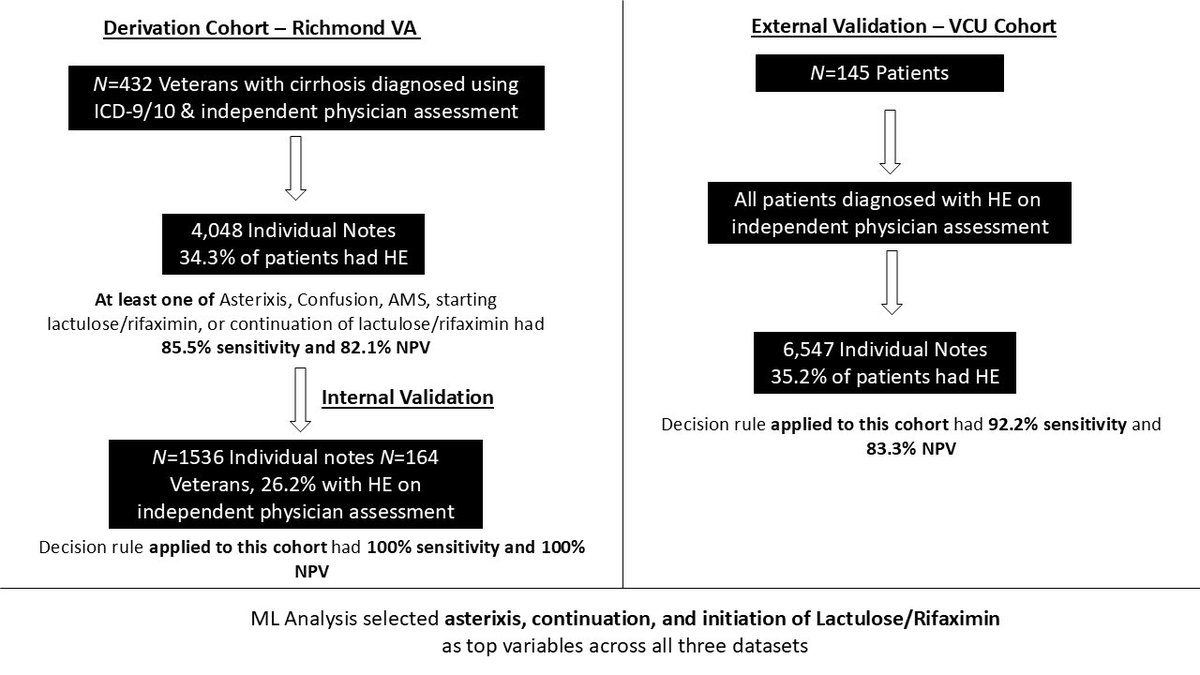
Can we use NLP #AI to ⬆️objectivity of #Hepaticencephalopathy diagnosis?
Yes! 3 cohorts (@RichmondVAMC @VCU_Liver #NACSELD) showed 5 phrases w ⬆️value
Implications for
🔑 #Transplant priority
🔑 remote adjudication of clinical trials
pubmed.ncbi.nlm.nih.gov/4119… @AmJGastro
1
14
45
3,029