
Head of the Dept. of Minimally Invasive and Robotic Urology, University Center of Excellence in Urology, Wroclaw Medical University, 'Views are on my own'
Joined May 2017
- Tweets 418
- Following 361
- Followers 252
- Likes 572
12 Photos and videos


Bartosz Malkiewicz retweeted

24 Dec 2025
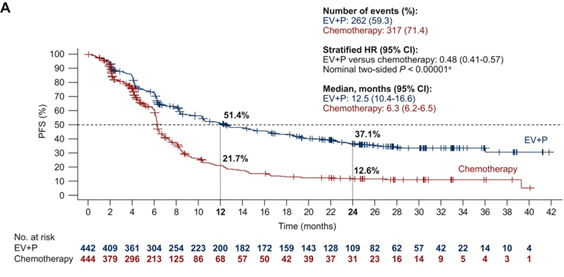
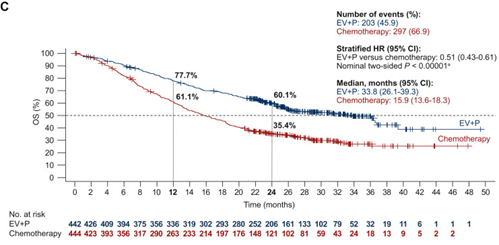
2/ Updated EV-302 (2.5-yr f/u). EV pembro as 1L SOC in la/mUC. PFS 12.5 vs 6.3 mo (HR 0.48); OS 33.8 vs 15.9 mo (HR 0.51) vs chemo. Durable benefit with no new safety signals.
@tompowles1 @shilpaonc
annalsofoncology.org/article…
2
13
47
4,907
Bartosz Malkiewicz retweeted
24 Dec 2025
IT IS THIS TIME OF THE YEAR AGAIN!
TOP 10 GU clinical trials in 2025!
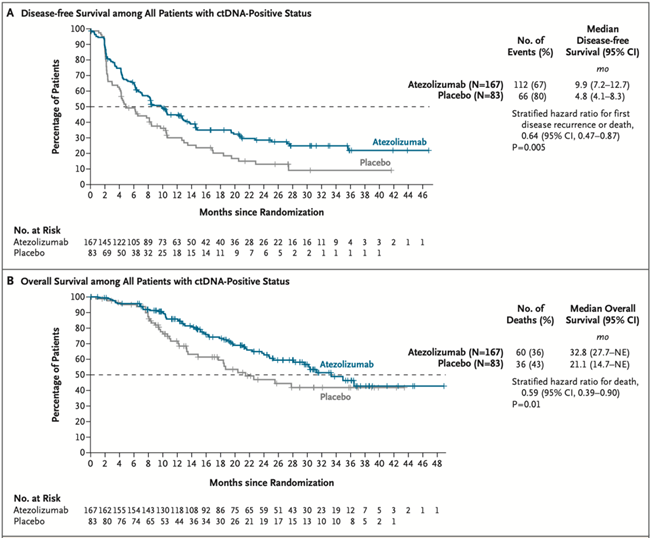
1/ Practice-changing IMvigor011: In ctDNA MIBC post-cystectomy, adjuvant atezo improved DFS (HR 0.64) & OS (HR 0.59) vs placebo. ctDNA- pts spared therapy w/ 2-yr DFS ~88%.
@tompowles1 @DrYukselUrun @OncoBellmunt @NEJM #ESMO2025 Plenary @myESMO
nejm.org/doi/full/10.1056/NE…
11
206
562
67,060
Bartosz Malkiewicz retweeted

24 Nov 2025
MRI is a great tool in prostate cancer. The problem is, quality in practice might not be quality we see in studies. Nice study from @dr_coops showing that in the VA, MRI not good enough to rule out biopsy. jamanetwork.com/journals/jam…
2
9
38
3,941
Bartosz Malkiewicz retweeted

24 Nov 2025
Remains one of the cheapest/easiest ways to minimize unnecessary testing, biopsy, diagnosis, or treatment: repeat a newly elevated PSA (without empiric abx)
jamanetwork.com/journals/jam…
4
12
83
13,536
Bartosz Malkiewicz retweeted

Optimal Duration of Androgen Deprivation Therapy With Definitive Radiotherapy for Localized Prostate Cancer: Meta-Analysis
jamanetwork.com/journals/jam…
Meta-analysis of over 10,000 patients from 13 randomized trials found that the survival benefit of androgen deprivation therapy (ADT) combined with radiotherapy is highly dependent on both treatment duration and patient risk profile, with diminishing returns beyond roughly 9–12 months and increasing non–cancer-related mortality with prolonged therapy. Optimal duration varied by disease severity—shorter or no ADT for lower-risk intermediate disease, longer courses for higher-risk groups—highlighting that extended therapy is not universally beneficial.
Because longer ADT improves cancer-specific outcomes but also increases other-cause mortality, the study emphasizes tailoring duration based on individual risk, comorbidities, life expectancy, and patient preference rather than applying uniform treatment lengths. #ProstateCancer
@NicholasZaorsky
@yilun_sun
@StatMatt9
@DrHowardSandler
@drjefstathiou
@Soum_Roy_RadOnc
@DrPaulNguyen
@jeshoag
@PBarataMD
@angela_jia_
@MSteinbergMD
@AmarUKishan
@DrSpratticus
@OncoAlert 🚨
@Silke_Gillessen
@AOmlin
@weoncologists
1
39
106
9,832
Bartosz Malkiewicz retweeted

17 Oct 2025
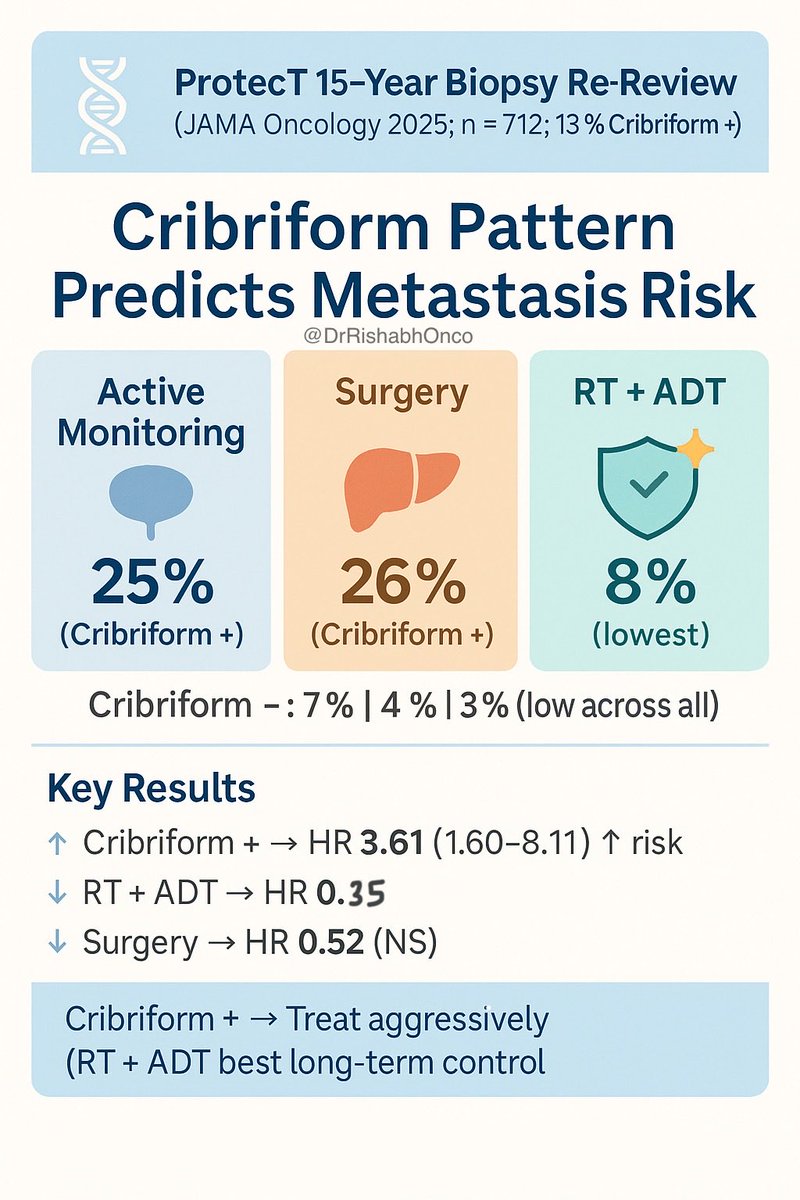
🧬 Cribriform architecture changes the story in localized prostate cancer.
🔥 ProtecT 15-year biopsy re-review shows who really needs treatment vs surveillance.
🎯 n = 712 with available slides (13 % cribriform )
💊 Arms:
▫️ Active monitoring
▫️ Radical prostatectomy
▫️ Radiotherapy neoadjuvant ADT
📊 Key Results
• Cribriform → ↑ metastasis risk (HR 3.61, 95 % CI 1.60-8.11)
• RT ADT → lowest metastasis (HR 0.35 vs active monitoring)
• Surgery → HR 0.52 vs active monitoring (NS)
• 15-yr metastasis (cribriform ): AM 25 % | Surg 26 % | RT ADT 8 %
• Cribriform –: 7 % | 4 % | 3 %
✅ Takeaway:
Cribriform = treat aggressively (RT ADT best long-term control)
Cribriform – = active surveillance still safe for most patients.
📖 Sushentsev et al. JAMA Oncology 2025. 🔗 doi.org/10.1001/jamaoncol.20…
#OncoTwitter #MedTwitter #ProstateCancer #UroOnc
@OncoAlert @myesmo @esmo_open @ASCO @JAMAOnc
2
75
167
16,011
Bartosz Malkiewicz retweeted

13 Jun 2025
Many thanks to my hosts @wojciechpiotrk1 @bartmalkiewicz Jan Łaszkiewicz and the rest of the wonderful Dept of Urology at Wroclaw Medical University observed really cutting edge Endourology and robotics. Also was interviewed by the local TV station as a highlight to my visit. @StanfordUrology



5
5
35
2,095
Bartosz Malkiewicz retweeted

18 Apr 2025
Our new SR and MA published in @EurUrolOncol evaluates focal therapy for localized PCa using prospective data only. Important for patient counselling.
📊 50 studies, 4,615 patients
📊 12-mo csPCa RFS in intermediate-risk: 79% (95% CI 74–83%)
🔗 doi.org/10.1016/j.euo.2025.0…
5
21
66
11,181
Bartosz Malkiewicz retweeted

11 Apr 2025
Histological subtypes/divergent differentiation (HS/DD) in UTUC = worse outcomes.
In a review of 14,407 patients, HS/DD linked to higher stage/grade, more LNI/LVI, and worse CSS, OS, RFS.
Detection should prompt aggressive tx close follow-up.
kwnsfk27.r.eu-west-1.awstrac…
1
2
2
212
Bartosz Malkiewicz retweeted

3 Apr 2025
Smarter staging in prostate cancer?
🙋🏼♂️🙋🏻♂️🙋🏾♂️In patients with intermediate/high-risk prostate cancer and negative PSMA PET (miN0), extended pelvic lymph node dissection (ePLND) remains a clinical dilemma.
🔍 This multi-institutional study (n = 282) externally validated five nomograms to predict lymph node invasion (LNI):
▪️ MSKCC
▪️ Briganti 2017
▪️ Briganti 2019
▪️ Amsterdam-Brisbane-Sydney
▪️ Briganti 2023
Key finding:
✅ The Briganti 2023 nomogram outperformed all others with highest accuracy (C-index: 77%) and spared 47% of unnecessary ePLNDs at a 5% cutoff—while missing only 3.8% of LNI cases!
Clinical implications:
1.Negative PSMA PET ≠ no risk: ~13% still had LNI!
2.Micrometastases matter: PSMA PET may miss them due to spatial resolution limits.
3.Briganti 2023 helps tailor who really needs nodal dissection, balancing risks and benefits.
pubmed.ncbi.nlm.nih.gov/3989…
@GGandaglia @dr_rajwa @ArmandoStabile @Albert0Briganti @alexmottrie
1
23
61
4,293
Bartosz Malkiewicz retweeted

23 Mar 2025
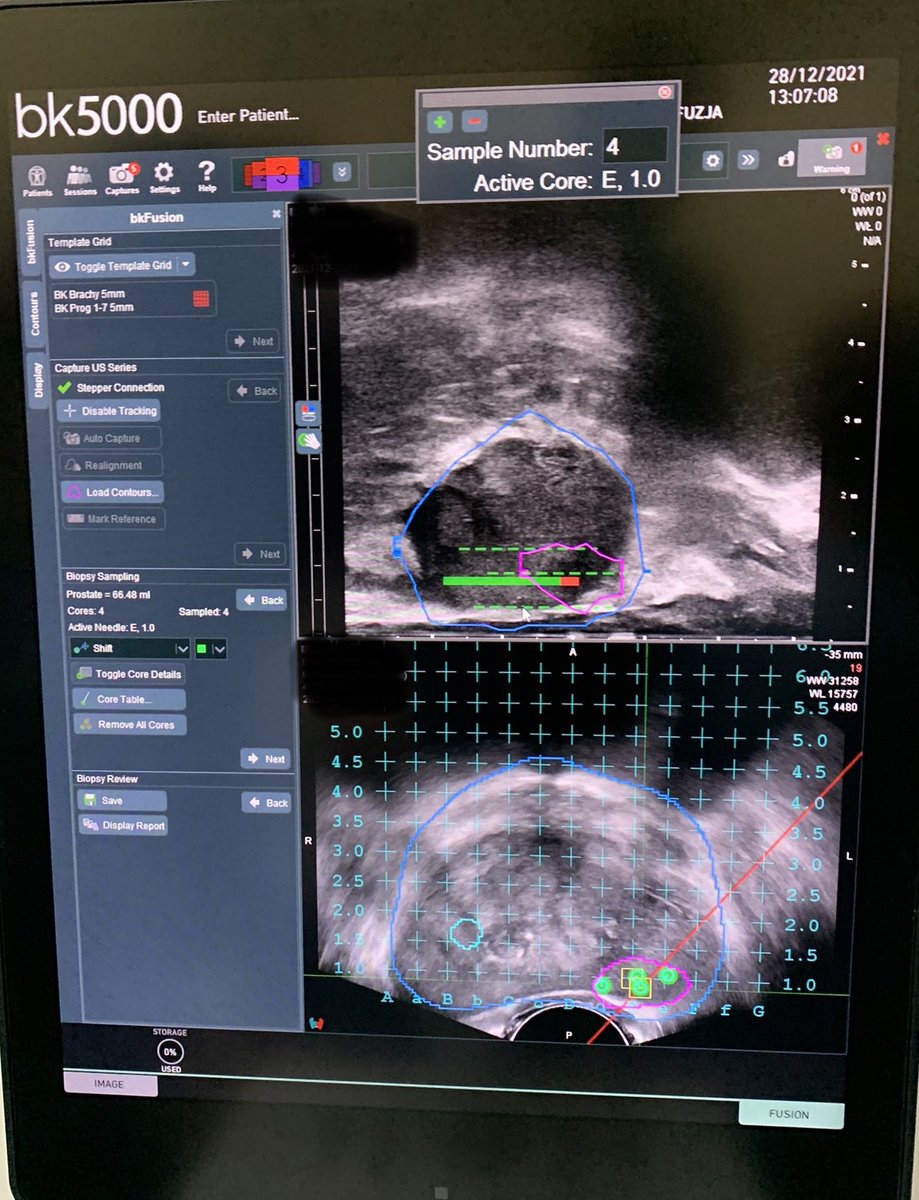
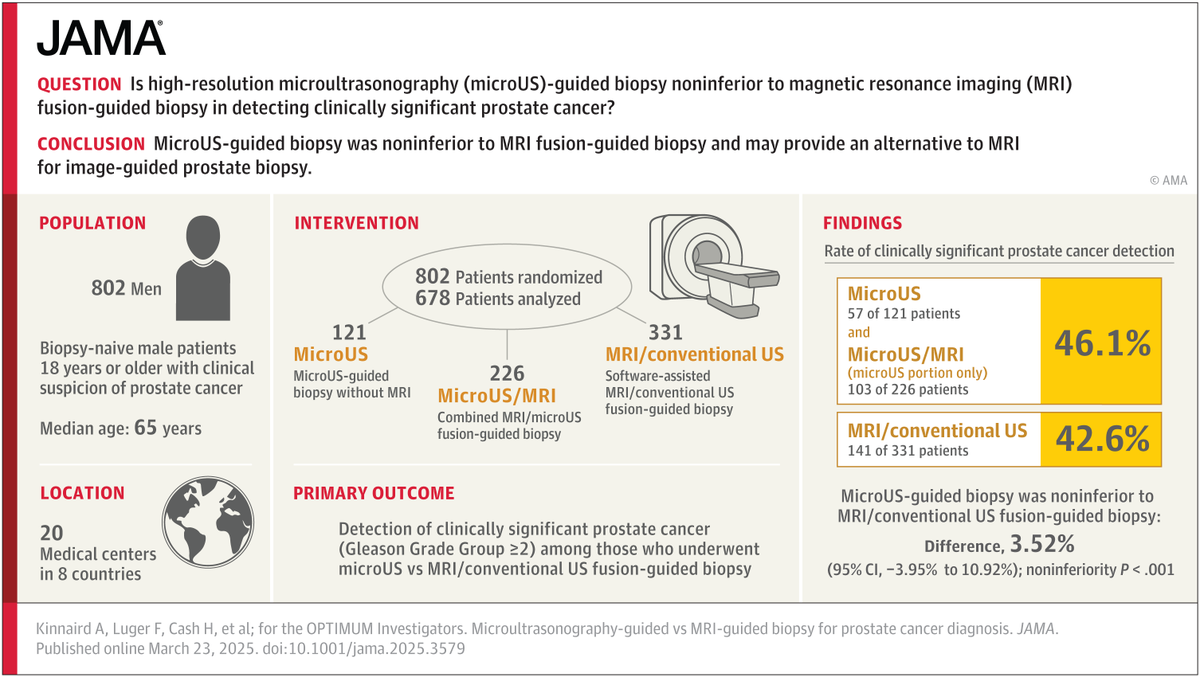
Micro-ultrasonography-guided biopsy is noninferior to MRI-guided fusion biopsy for the detection of clinically significant prostate cancer in biopsy naïve men. ja.ma/4hzTwTo #EAU25 @JulianStruck @moisessocarras @ChrisFungMD @arvinkgeorge @TxetxuPereira
6
43
102
20,856
Bartosz Malkiewicz retweeted

22 Mar 2025
#eau25
What is your advice for a 65yo man with Parkinson and 80ml prostate?
💥Functional session: urodynamics first!
💥BPH surgery session: AEEP first!
💥CaP session: what is his PSA?
💥Patient session: LUTS is not so important to me
1
4
179
Bartosz Malkiewicz retweeted

16 Jan 2025
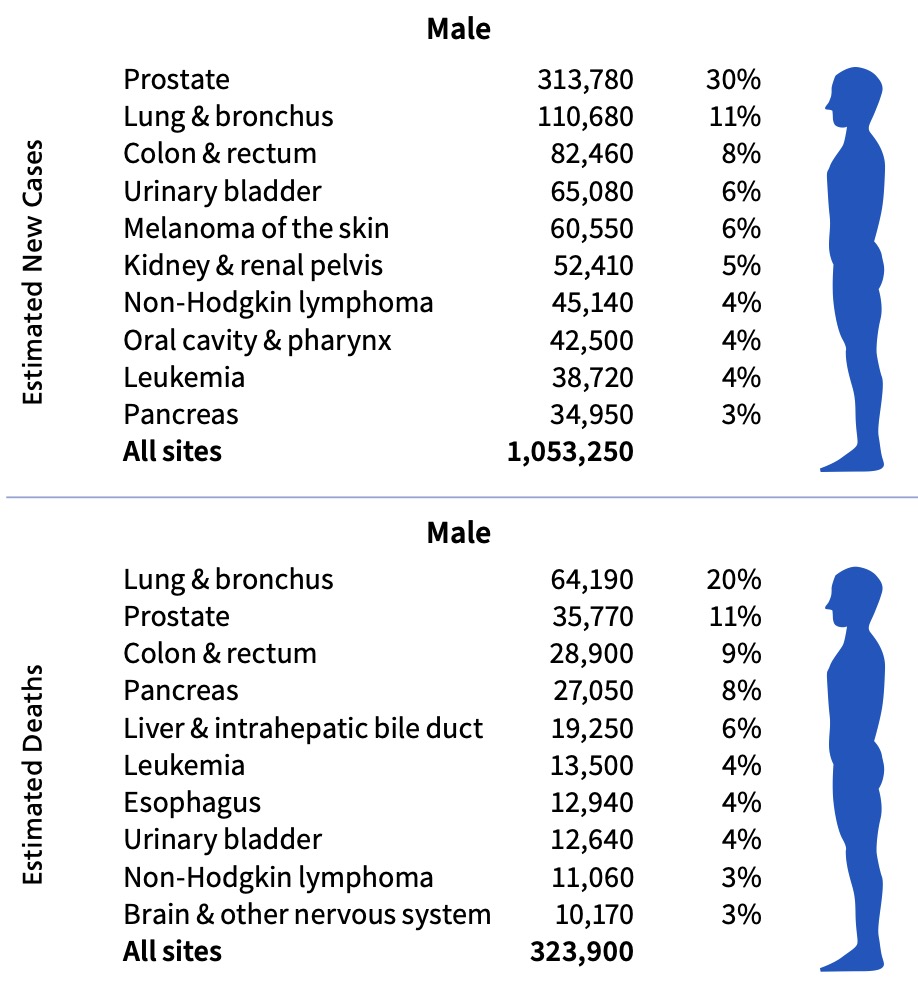
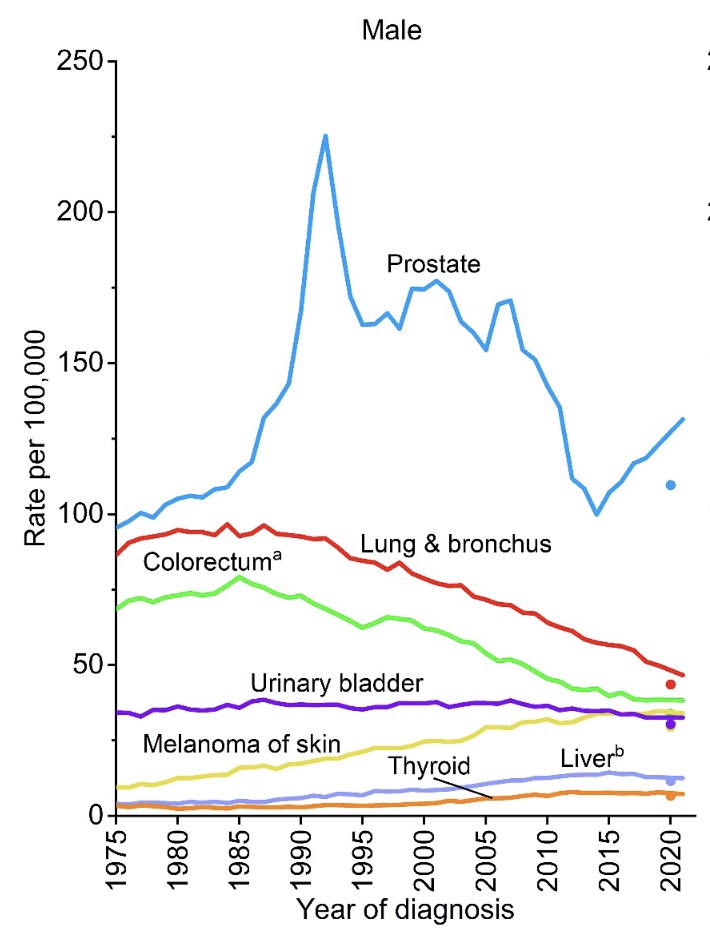
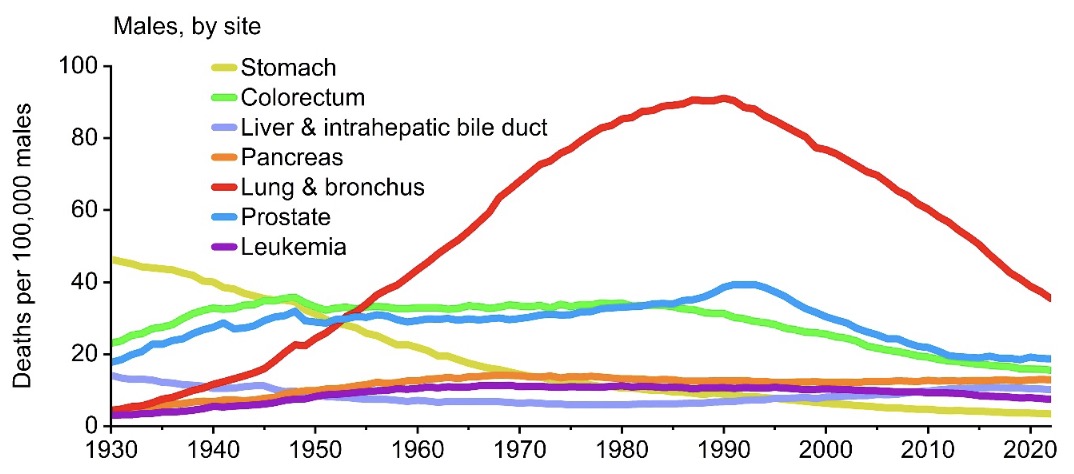
Cancer Statistics 2025 are out! #prostatecancer incidence still on the rise, mortality basically flat. Get screened so you can get treatment _when needed_. #pcsm
acsjournals.onlinelibrary.wi…
8
92
164
24,988
Bartosz Malkiewicz retweeted

4 Jan 2025
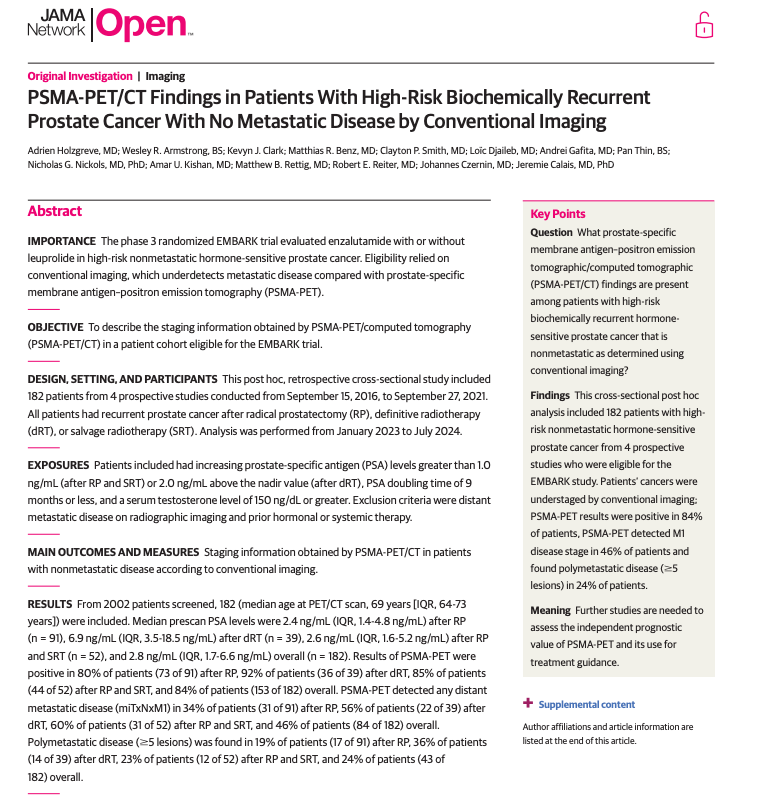
Conventional imaging understages high-risk nonmetastatic prostate cancer.
☢️PSMA-PET was positive in 84% of cases, detecting M1 disease in 46%, polymetastatic in 24%.
#ProstateCancer #PSMAPET #Oncology @OncoAlert @JAMANetworkOpen @APCCC_Lugano
doi:10.1001/jamanetworkopen.2024.52971
1
40
95
7,834
Bartosz Malkiewicz retweeted

5 Jan 2025
Some statistics of the Journal
🌍 Numbers of articles accepted over the past 5 years

3
3
422
Bartosz Malkiewicz retweeted
5 Jan 2025
5-year (2020-2024) acceptance rate :
2
4
246
Bartosz Malkiewicz retweeted

30 Dec 2024
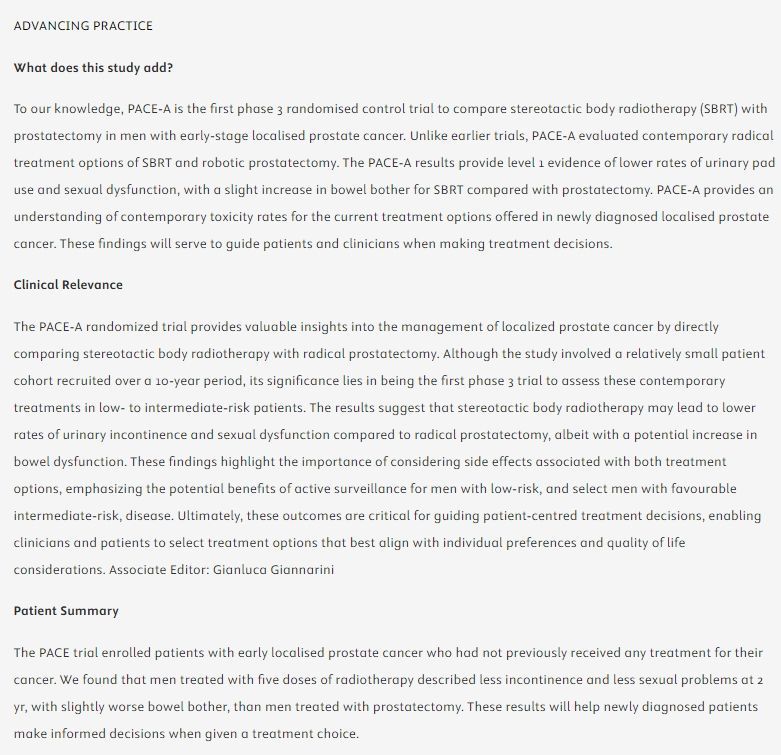
Editor's Choice: Radical Prostatectomy Versus Stereotactic Radiotherapy for Clinically Localised Prostate Cancer: Results of the PACE-A Randomised Trial by @nickva1 et al
Read the full article here: buff.ly/3OSVsu6
Come back to read the Editorial!
#UroSoMe #MedTwitter #eururol #EditorsChoice #ProstateCancer #PCa #Spotlight
@GGiannarini

1
30
65
8,249
Bartosz Malkiewicz retweeted
28 Dec 2024
And NOW, TOP 5 PROSTATE CANCER trials of 2024!
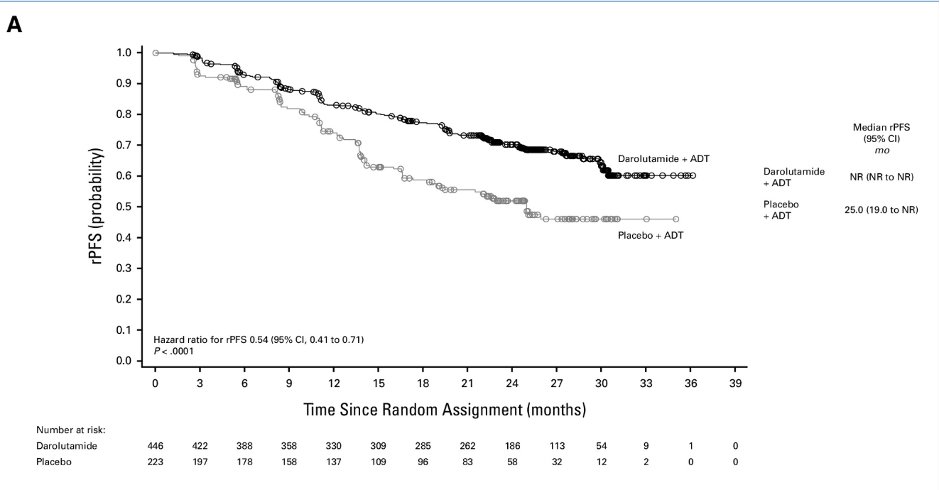
1) The ARANOTE trial shows darolutamide ADT improves rPFS in mHSPC by 46%,--Benefits seen across all subgroups with a favorable safety profile.
⛹🏼♂️A new player for doublets in mHSPC!
#ESMO24 Dr. Fred Saad @Silke_Gillessen @neerajaiims @umangtalking @DrRanaMcKay @JCO_ASCO
doi.org/10.1200/JCO-24-01798
5
169
370
45,519
Bartosz Malkiewicz retweeted

14 Dec 2024
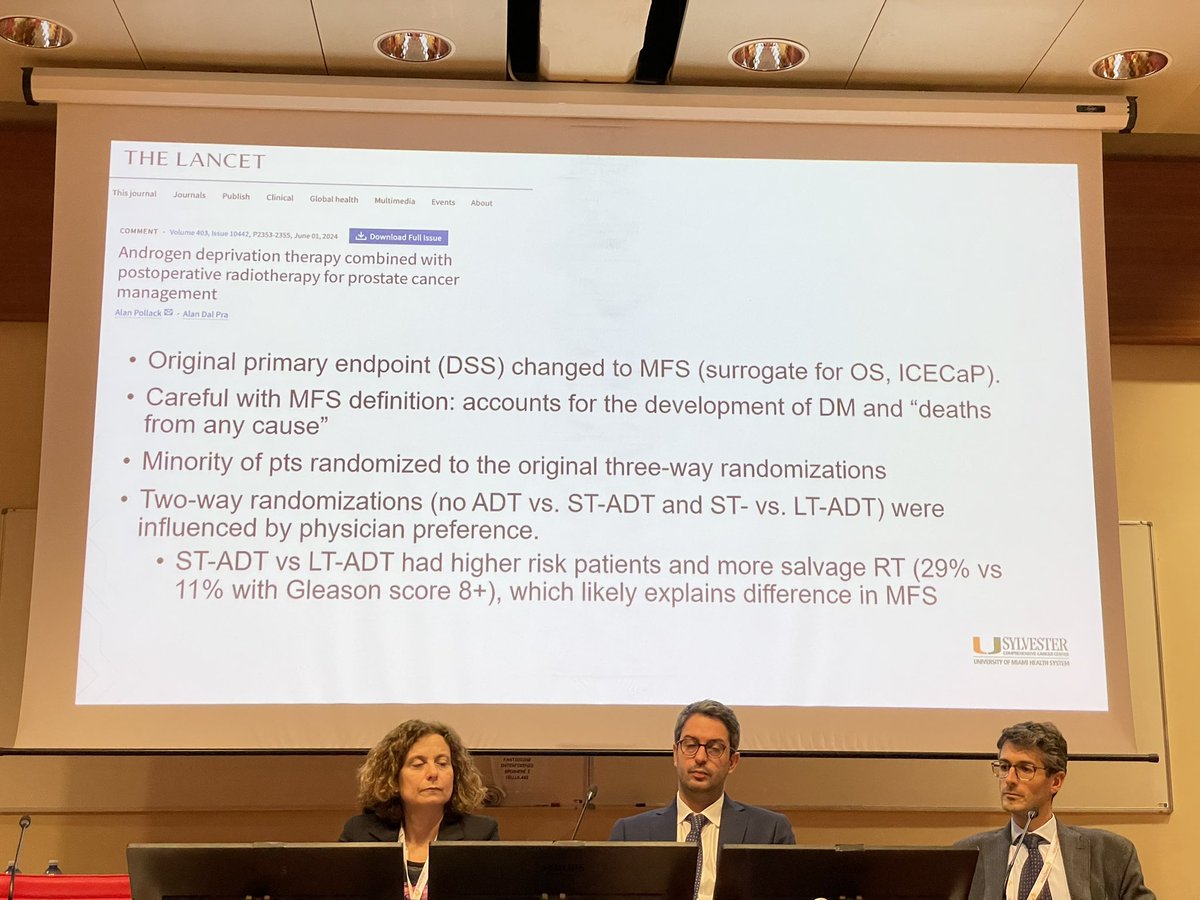
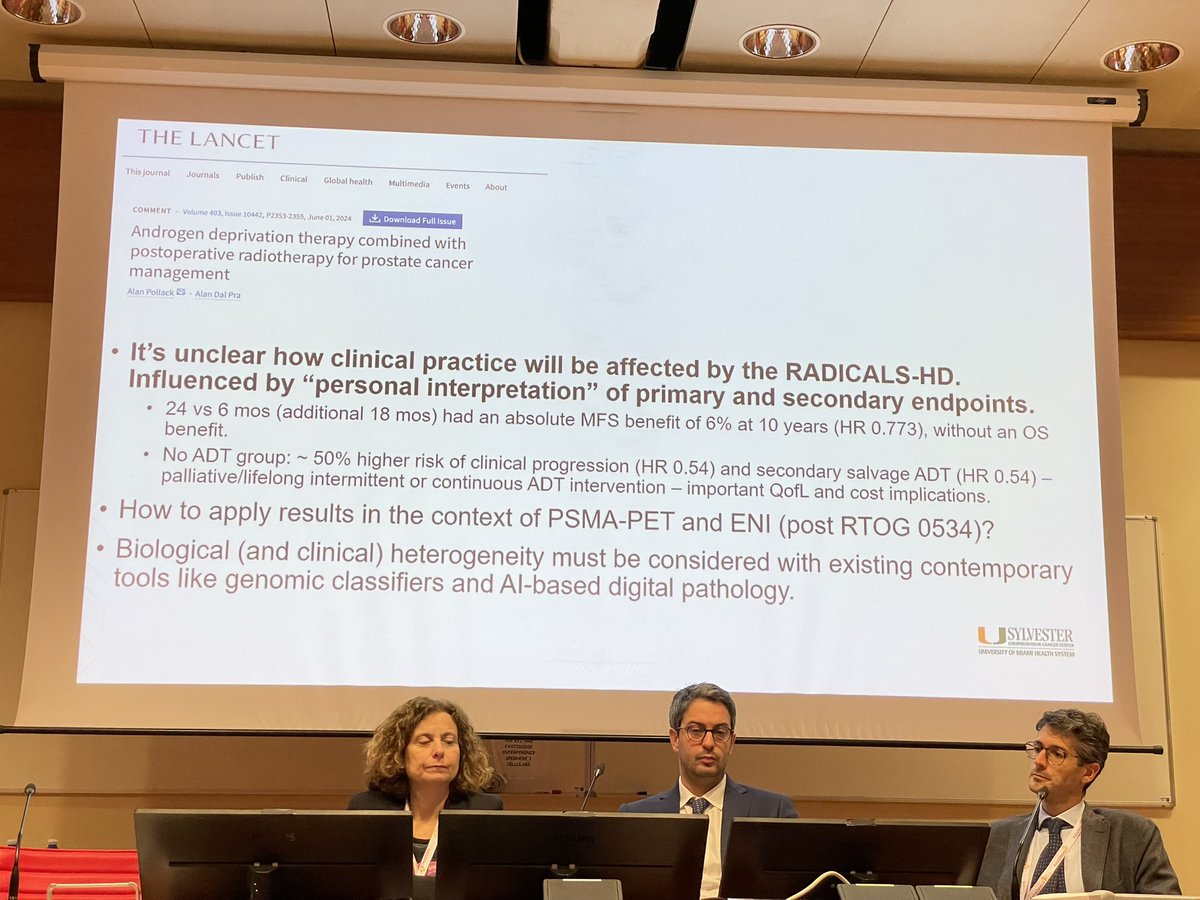
Insightful interpretation of the RADICALS-HD trial by @a_dalpra at yesterday’s PCa masterclass. Kudos to my friends @paolo_gontero, @oderdam, @GMarra_MD, and @peppinoiorio for organizing such a stellar event!
7
28
2,535
Bartosz Malkiewicz retweeted
14 Dec 2024
Great insights from @TaimurShah on @TouijerKarim’s trial comparing limited vs. extended PLND at yesterday’s #TOP24 prostate cancer masterclass in Turin. Congrats to organizers @paolo_gontero, @oderdam, @GMarra_MD, and @peppinoiorio!

1
4
11
1,591