
73 Photos and videos









Pinned Tweet

6 May 2025
Launch Day!
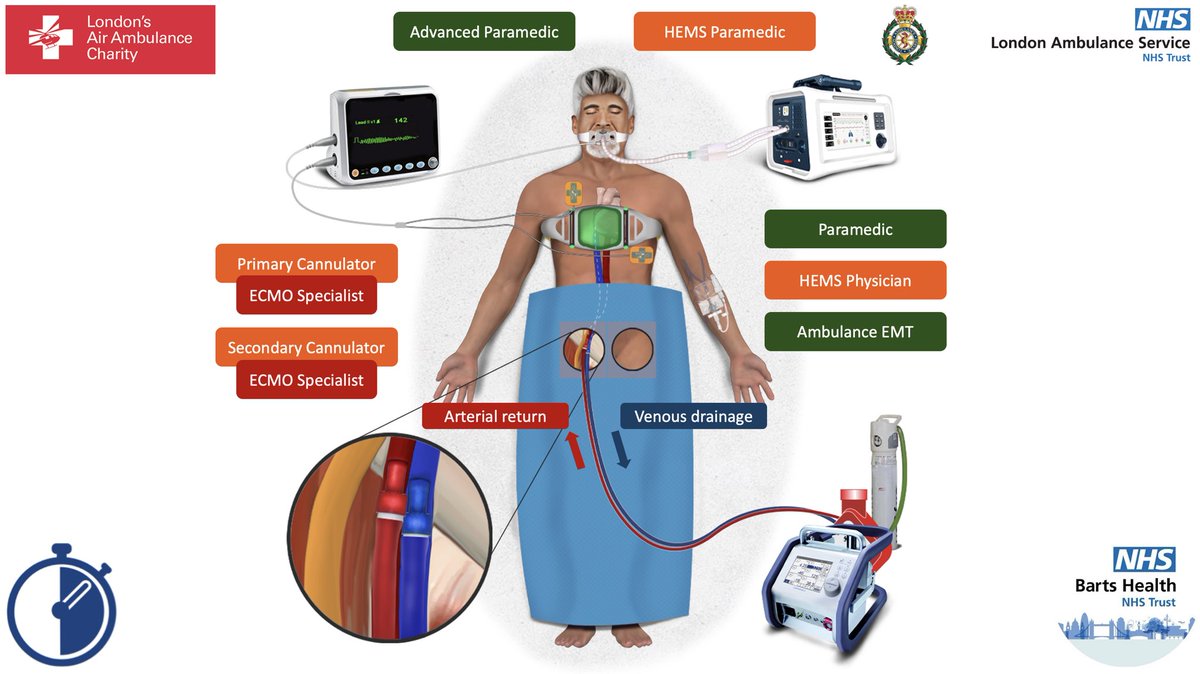
Endovascular Cardiac Arrest Team (ECAT) @LDNairamb in collaboration with @NHSBartsHealth & @Ldn_Ambulance - #ECMO-CPR #Resuscitation
6 May 2025

For the first time ever in the UK, we are bringing ECMO to the streets of London, offering hope to patients in cardiac arrest.
londonsairambulance.org.uk/n…


3
11
85
10,481
Mamoun retweeted

Apr 29
What happens when you remove the hospital as the boundary?
Advanced, targeted interventions & diagnostics can be delivered in the field enhancing cardiac arrest care
Reframing resuscitation as precision critical care @cliffreid @PrecareSyd @SydneyHEMS
sciencedirect.com/science/ar…
17
43
3,447
Mamoun retweeted

Apr 24
I have changed my practice because of this gem!
If you think it’s worthy - please give it a RT & a like!

3
18
51
5,782
Apr 1
Tough to operate with success in current #NHS environment, yet, ACCESS London do it 24/7 all year round. Thousands of patients conveyed on complex life support and given access to lifesaving procedures! Proud you @ACCESS_London1 Team x.com/access_london1…

🚑 3 years of ACCESS London
Supporting critical care transfers across London and beyond
📷 130,000 km travelled
📷 Supported by over 500 healthcare professionals
#CriticalCare #NHS

1
6
13
1,917
Mar 30
What a beautiful piece on clinical physiology in septic shock and various haemodynamic profiles 🫀

🤓🫀We keep asking: “What’s the cardiac output?”
But maybe the better question is:
“How efficiently is the heart working?”
In septic shock, we often focus on:
Preload
Cardiac output
MAP
But we forget something fundamental:
👉 The heart doesn’t work alone.
👉 It works against the arterial system.
1. The missing concept: Ventriculo–arterial coupling (LVAC)
LVAC = interaction between:
Ees → contractility
Ea → arterial load
👉 Expressed as Ea / Ees
This ratio reflects:
How efficiently the heart converts energy into forward flow
2. What is “normal”?
LVAC ≈ 0.5 → optimal efficiency
LVAC ≈ 1 → maximal stroke work
LVAC > 1 → uncoupling (inefficient system)
But here’s the twist:
👉 In septic shock, LVAC is often >1
👉 Not just due to vasodilation—but also myocardial dysfunction
3. Why this matters clinically
Two patients can have:
Same MAP
Same CO
But completely different physiology:
✔ One → efficient coupling
❌ One → energy wasted, poor flow generation
4. The key insight
Septic shock is NOT just:
❌ “low preload”
❌ “vasodilation”
It is:
👉 A mismatch between heart and arterial system
5. Therapy changes the balance
Fluids → may improve coupling (↓ LVAC)
Norepinephrine → can improve OR worsen coupling
Inotropes → target Ees
Important:
👉 Increasing MAP ≠ improving flow
👉 Increasing pressure can worsen afterload
6. The most interesting part
From the data:
LVAC >1 can predict response to norepinephrine
But improving LVAC ≠ guaranteed tissue perfusion and outcomes follow a U-shaped curve
👉 Both too high AND too low LVAC can be harmful
7. The limitation we must respect
Even if you “optimize” LVAC:
👉 Microcirculation may still be impaired
👉 Lactate may still rise
👉 Shock may persist
Because: Macro ≠ micro
🤓Final message
We need to move from:
❌ “Fix the blood pressure”
To:
✅ “Optimize the interaction between heart and vessels”
LVAC doesn’t replace hemodynamics.
It completes it.
📃Reference
Caicedo Ruiz JD et al. Journal of Critical Care, 2026. doi.org/10.1016/j.jcrc.2026.…

ALT
1
17
70
15,598
Mar 26
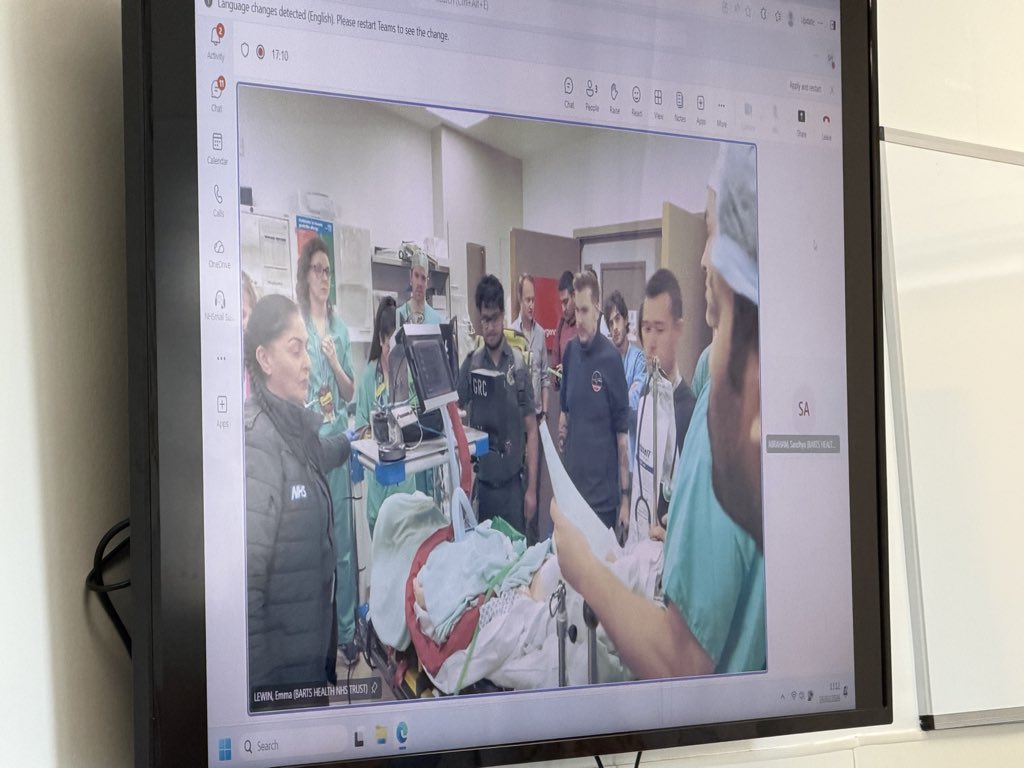
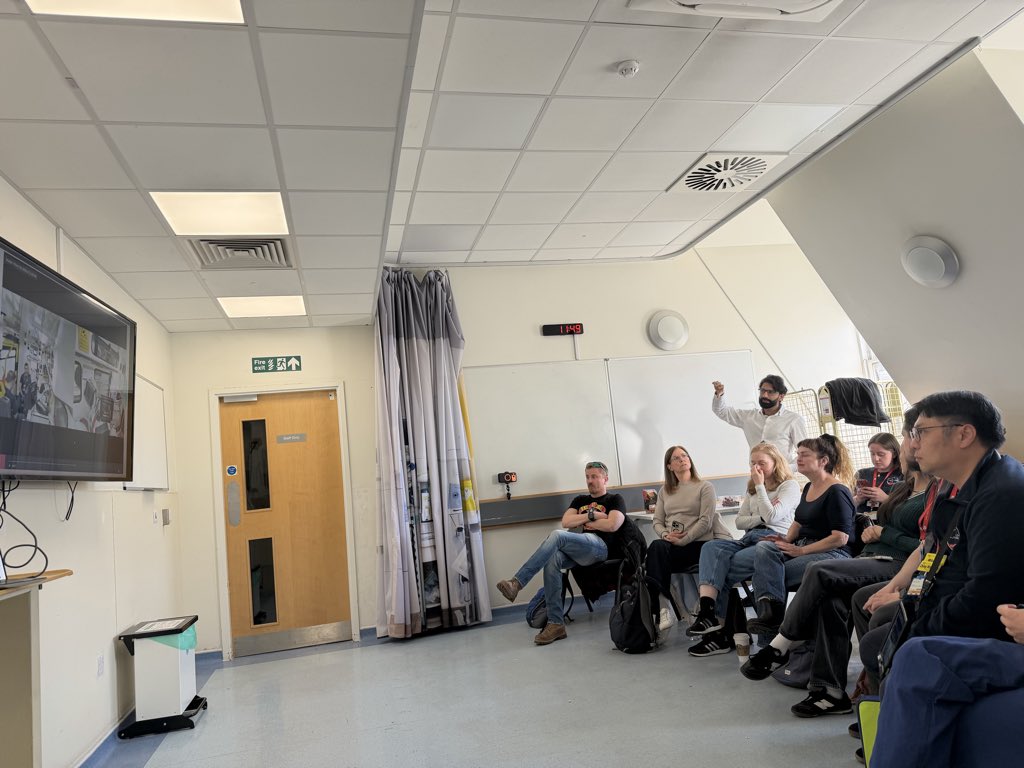
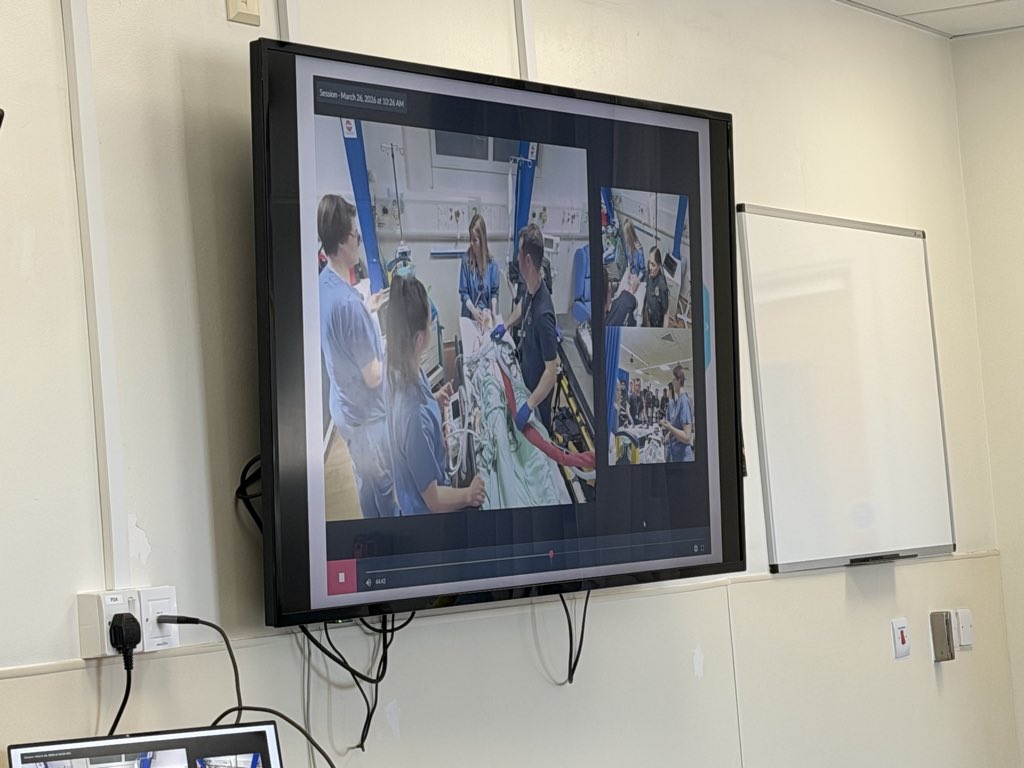
A macro-sim across entire system, over 60 staff participated incl. multpl sites of @NHSBartsHealth & high complexity transfer by @ACCESS_London1 Crit Care Retrieval Team in collaboration with @Ldn_Ambulance testing processes, individual and collective skills - This is readiness
Mar 26
🚨 ACCESS Mega Sim Day 🚨
High-fidelity, high-pressure, real-world simulation in action today with the ACCESS team. This isn’t routine ICU — it’s ICU in motion.
👏 Huge well done to everyone undertaking the sim today — pushing boundaries!

1
2
8
765
Feb 2
Practicing or budding Resuscitationists and Critical Care Physicians - do not miss this conference! Best wishes @ThinkingCC & Co
Feb 2

Totally amped to announce HR26 registration is open! Foundations Reimagined. Lets rake everyone’s game to another level!!! thinkingcriticalcare.com/202…
1
1
6
1,522
Jan 27
Congrats to our USA colleagues & #ECPR collaborators on the first Helicopter facilitated ECMO-CPR in the United States #Resuscitation #ECPR #ECMO
Jan 26

Today marked an important step forward in US resuscitation science!
The Center for Resuscitation Medicine’s MMRC completed the first Helicopter EMS–facilitated extracorporeal cardiopulmonary resuscitation (ECPR) in the United States!



9
513
Mamoun retweeted

25 Dec 2025
🎄✨ Merry Christmas from the ACCESS family ✨🎄
To our incredible team — the calm voices, sharp minds, fast wheels, and big hearts — thank you for showing up 24/7 for the sickest patients, no matter the day 💙🚑

1
4
11
711
23 Dec 2025
Leaving the best till last. @Ldn_Ambulance & @ACCESS_London1 touring #London in the best Christmas spirit sharing gifts round the capital and building bridges with partners & our community - A huge thank you to #TeamLAS who led this initiative - #OperationChristmasPresent
23 Dec 2025

Thank you to BloomsBury ambulance station NHS alone with @ACCESS_London1 for all your help this year with #OperationChristmasPresent @Ldn_Ambulance You have helped so many children smile this Christmas ❤️#ThankYou #Christmas #Ambulance #tuesdayvibe #AccessLondon @NHSBartsHealth

1
7
10
1,295
Mamoun retweeted

23 Dec 2025
Us @Ldn_Ambulance 🤝 looking after London 24/7 this festive period.


1
13
71
4,463
Mamoun retweeted

17 Dec 2025
On behalf of @LDNairambulance, Transform Trauma & @TheIoPHC, thank you to everyone who attended #Trauma2030. Huge thanks to our speakers, faculty, sponsors, partners & delegates, with special recognition to Dr Anne Weaver, Dr Mamoun Abu-Habsa & Dr Jess Payne for outstanding leadership. Grateful to our production team — Imen Rezgui, Beth Leonard & Rebecca Kennard — whose work made it all possible.
📍 RCS England | 15–16 Dec 2025




1
8
19
1,449
Mamoun retweeted

17 Nov 2025
Meet Dr Anne Weaver, London’s Chief Airborne Medic vogue.co.uk/article/dr-anne-…
1
10
32
12,693
Mamoun retweeted
13 Nov 2025
🔥 It’s Here. The Agenda Has Dropped.
🚨 ACCESS CDD: AORTA IN MOTION — 11 Dec 2025.
Free to attend | 5 CPD points
📍 Bearsted LT Theatre, RLH Education Academy
🔗 Register: form.jotform.com/accessdata/…
#AorticDissection #CriticalCare #ACCESSCDD #AortaInMotion #RCOA #NHS

1
10
16
2,223
Mamoun retweeted
7 Nov 2025
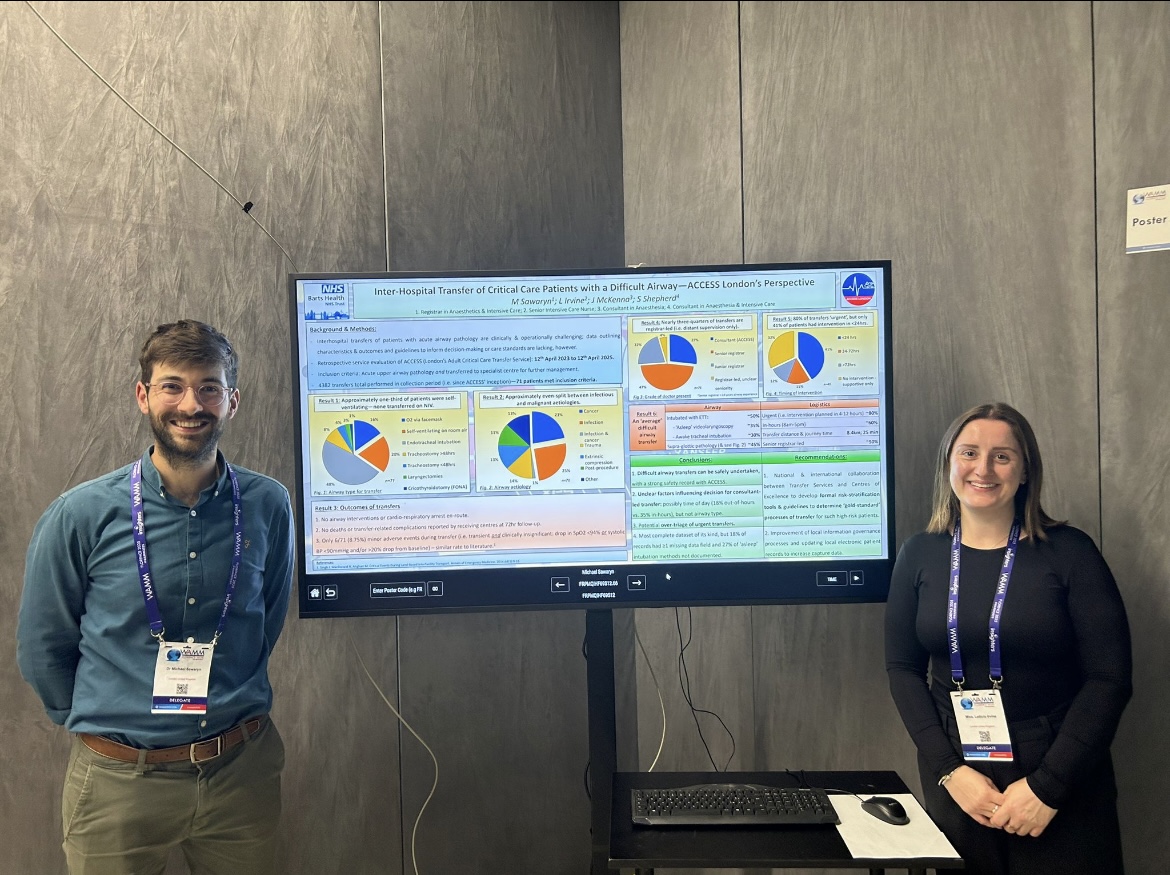
🇮🇹🚑 ACCESS goes to Italy!
Our Registrar Michael and Practitioner Letticia are representing ACCESS London at #WAMM2025 — presenting their work on “Inter-Hospital Transfer of Critical Care Patients with a Difficult Airway: The ACCESS Perspective.”
Proud to see our team showcasing innovation and collaboration on the global stage! 🌍💙👏👏
#CriticalCare #AirwayManagement #ACCESSLondon #NHS #WAMM2025
1
7
22
2,988
5 Nov 2025
Useful guide for fluid balance management during recovery phase in #CriticalCare
4 Nov 2025

(1/x) When you trying to decongest patients in the ICU, there are lots of drugs available... not just lasix
Here are some tips for diuresing patients🧵
Furosemide - backbone of diuresis. Start at a higher than you think and back off if diuresis achieved.
Metolazone (or other thiazides). Use when Na on the higher side as helps prevent distal Na resorption. You get more naturesis.
Acetazolamide. Use to prevent metabolic alkalosis. Aids in decongestion.
Spironolactone. Use to prevent K wasting and to achieve more natriuresis.
3% saline. Consider in diuretic resistant heart failure with hypochloremia.

5
572
24 Oct 2025
A story worth studying - well done to All involved @EMDocJB @DrPaulRees and others
23 Oct 2025

“Physiology-Guided CPR” 🚨🚨🚨
The inclusion of “physiology-guided CPR” in the ERC resuscitation guidelines marks a significant milestone in progress.
So here are my reflections on the journey we have undertaken and thoughts on the future directions
#SPEAR
🧵
1
6
17
2,823
Mamoun retweeted

23 Oct 2025
“Physiology-Guided CPR” 🚨🚨🚨
The inclusion of “physiology-guided CPR” in the ERC resuscitation guidelines marks a significant milestone in progress.
So here are my reflections on the journey we have undertaken and thoughts on the future directions
#SPEAR
🧵
3
36
147
30,178
Mamoun retweeted

21 Oct 2025
How do you save arrested bleeding trauma patients with pH <6.5? With systematic research and implementation across the Royal London Hospital Major Trauma Centre & London's Air Ambulance, supported by @Barts_Charity & @LDNairamb. This is what we've been up to (& where we're going)
19 Oct 2025

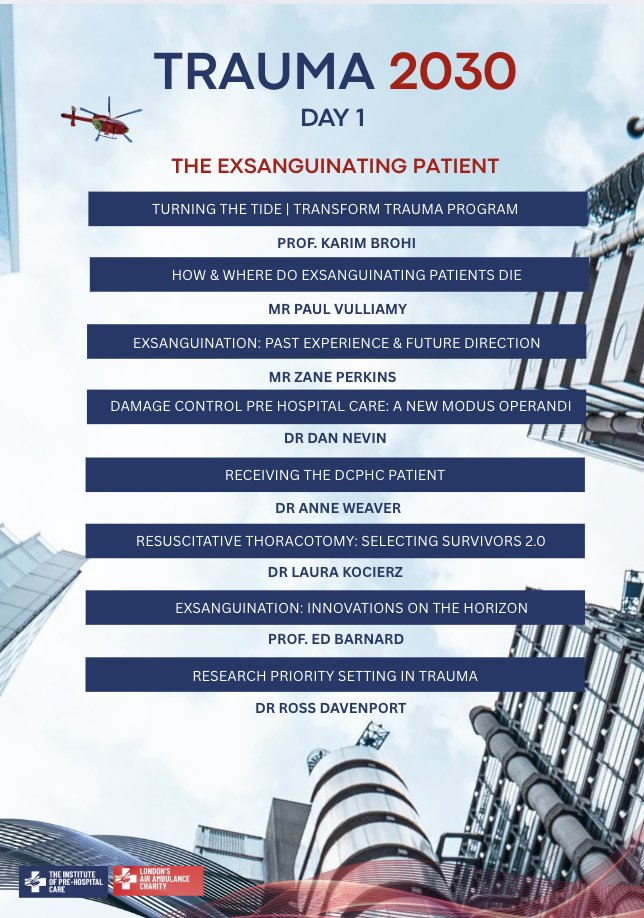
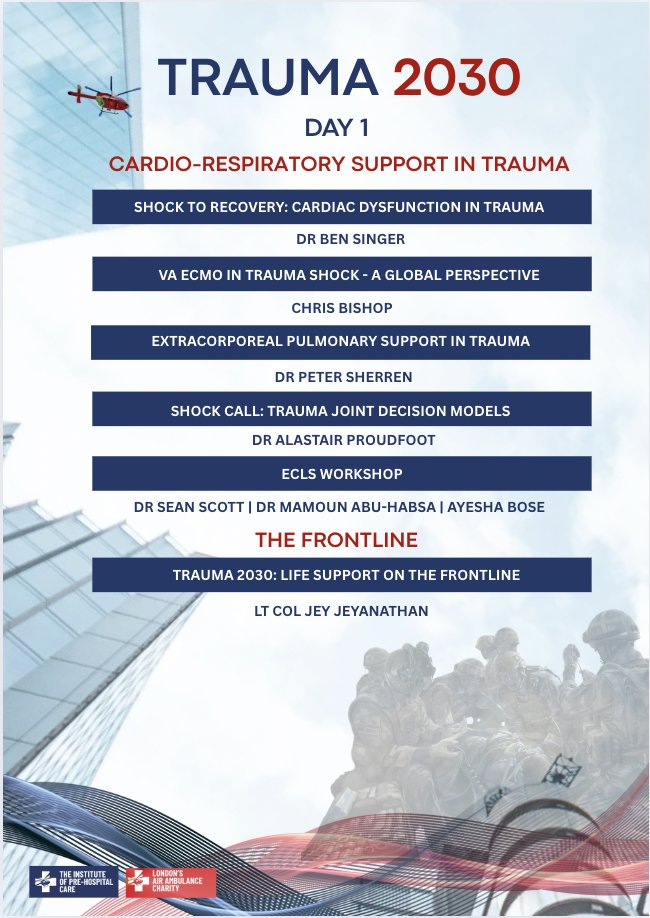
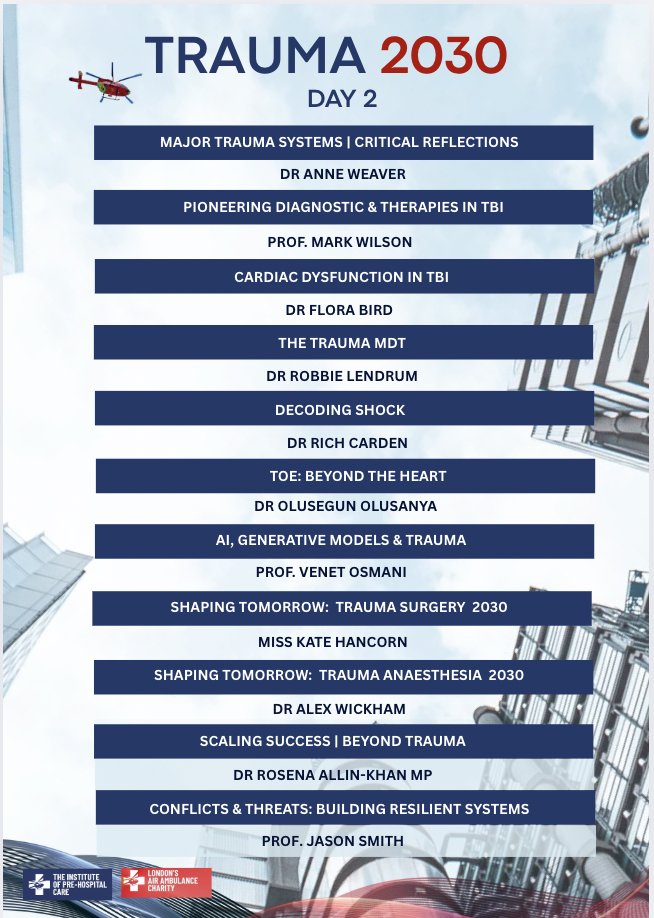
🚨 The #Trauma2030 Programme is LIVE
Two days. Global experts. One mission — to shape the next decade of trauma care. From damage control to digital innovation — discover what’s ahead.
1
8
35
7,982
Mamoun retweeted
20 Oct 2025
🚨 Abstract Submissions Open!
The #Trauma2030 Symposium invites clinicians, researchers, students & innovators to share groundbreaking work in trauma, surgery, critical care, AI — and more.
Submit your abstract and help rewrite the future of Trauma Care.
🧠💡 Deadline: 15 Nov 2025
📩 iophc@londonsairambulance.org.uk
14
30
4,711
Mamoun retweeted
19 Oct 2025
🚨 Introducing the Trauma 2030 Symposium 🚨
Transform Trauma & London’s Air Ambulance present a landmark two-day event shaping the future of Trauma Care.
🗓️ 15–16 December 2025
📍 Royal College of Surgeons, London
🎟️ Tickets now live → fundraising.londonsairambula…
#Trauma2030 #TransformTrauma #LAA #TraumaCare #InnovationInMedicine

2
13
56
7,763