
Medical oncologist / theoncodoctor!/
Joined June 2009
- Tweets 214
- Following 269
- Followers 154
- Likes 260
15 Photos and videos










Dr Arun Chandran retweeted

May 16
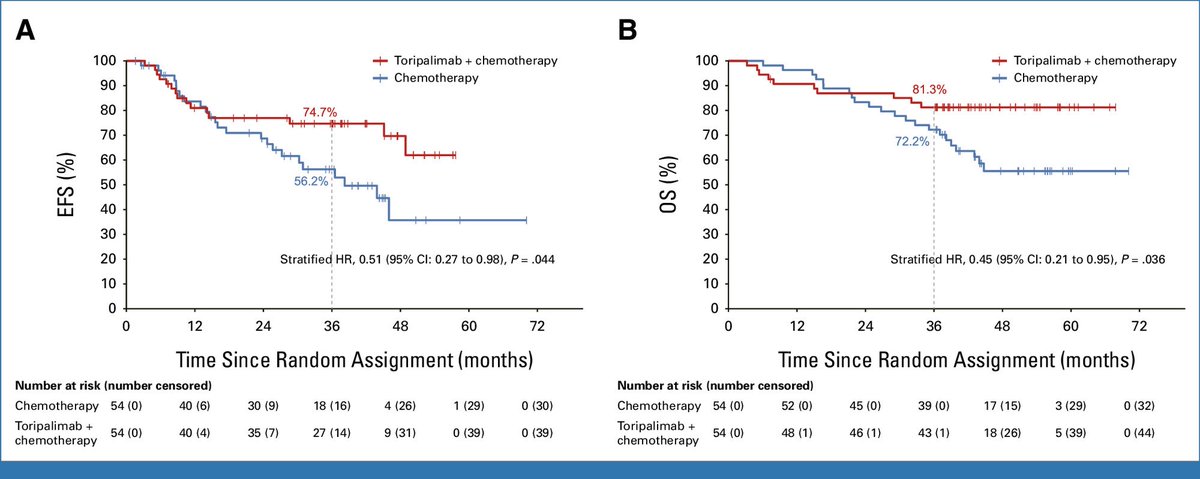
💥NEOSUMMIT-01 trial in LA gastric/GEJ cancer: perioperative toripalimab ChT vs ChT alone (3-year follow-up, n=108)
ascopubs.org/doi/full/10.120…
▪️ 3-year EFS: 74.7% vs 56.2% (HR 0.51)
▪️ 3-year OS: 81.3% vs 72.2% (HR 0.45)
▪️ Benefit maintained across most predefined subgroups
Perioperative IO TORI-pal the survival curves in GC 🍜
@OncoAlert @OncoReporte
@myESMO @_SEOM @GrupoTTD

10
22
1,628
Dr Arun Chandran retweeted
May 17
🚨 RESET-C trial: single-cycle neoadjuvant pembrolizumab in stage I–III dMMR colon cancer (n=85)
ascopubs.org/doi/full/10.120…
🎯 pCR 44% || MPR 57%
💥 DFS and OS rates: 96% and 98% at 18.4 months
▪️ Grade ≥3 AEs in 11%; only 1 recurrence reported
One shot and the tumor may already be hitting the RESET button 🔄
@OncoAlert @OncoReporte
@myESMO @_SEOM @GrupoTTD



9
29
1,494
Dr Arun Chandran retweeted

May 1
Medicine is all about a lot of learning & then a lot of de-learning also!
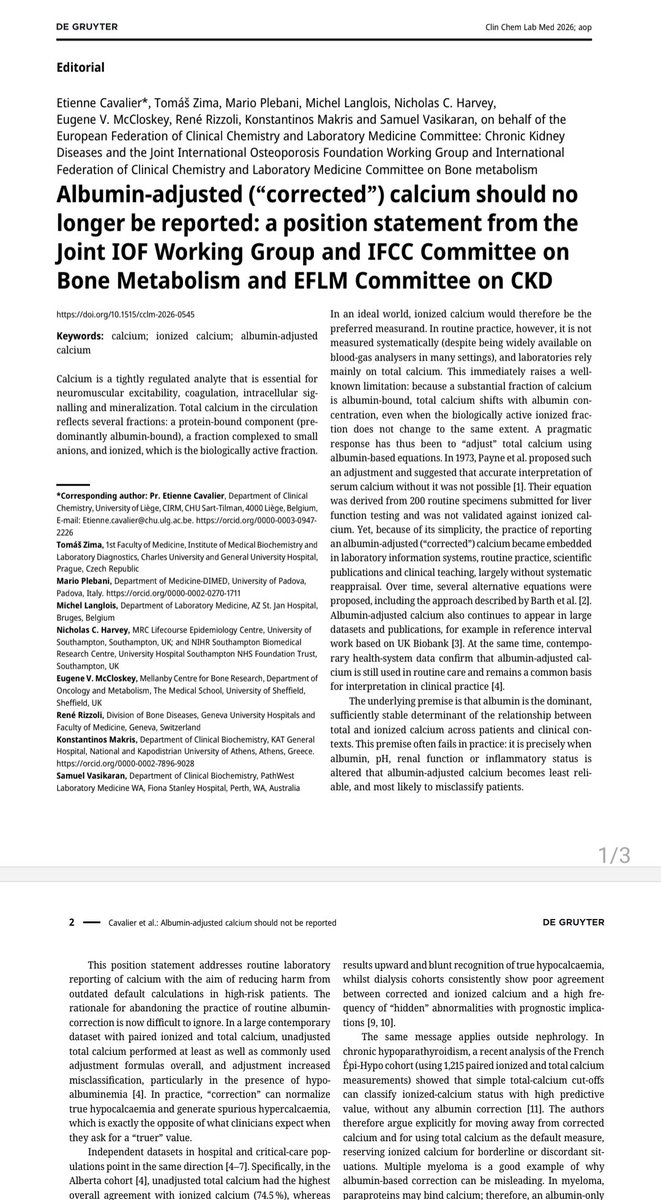
The very popular corrected serum calcium correction should no longer be used in the setting of abnormal albumin levels
Corrected serum calcium = measured serum calcium 0.8 (4-Albumin) formula should no longer be used
In the setting of low albumin levels, serum ionised calcium should be measured instead
@iofbonehealth @isbmrindia @ISBMRTweets @iofbonehealth @Osteoporosis_NL @osteoporosisNI @TeamSESH @RheumPearls @RheumJnl @RheumResearch @IndianRheum @nihardesai7 @j_metb @EndoSocAus @EndoSocJournals @TheEndoSociety @TheAACE @IndiaESI
10
120
392
33,405
Dr Arun Chandran retweeted

Jan 15
Premenopausal HR /HER2 eBC – Adjuvant ET
• RD after NAT → OFS AI
• pCR after NAT → risk-adapted
– Stage III → OFS AI
– Stage I–II → AI or TAM ± OFS
• Upfront surgery → baseline stage-driven ET
Principle:
RD = ER-dependent, chemo-resistant → needs ET intensification
Great editorial👇
thebreastonline.com/article/…
33
70
5,703
Dr Arun Chandran retweeted

Jan 13
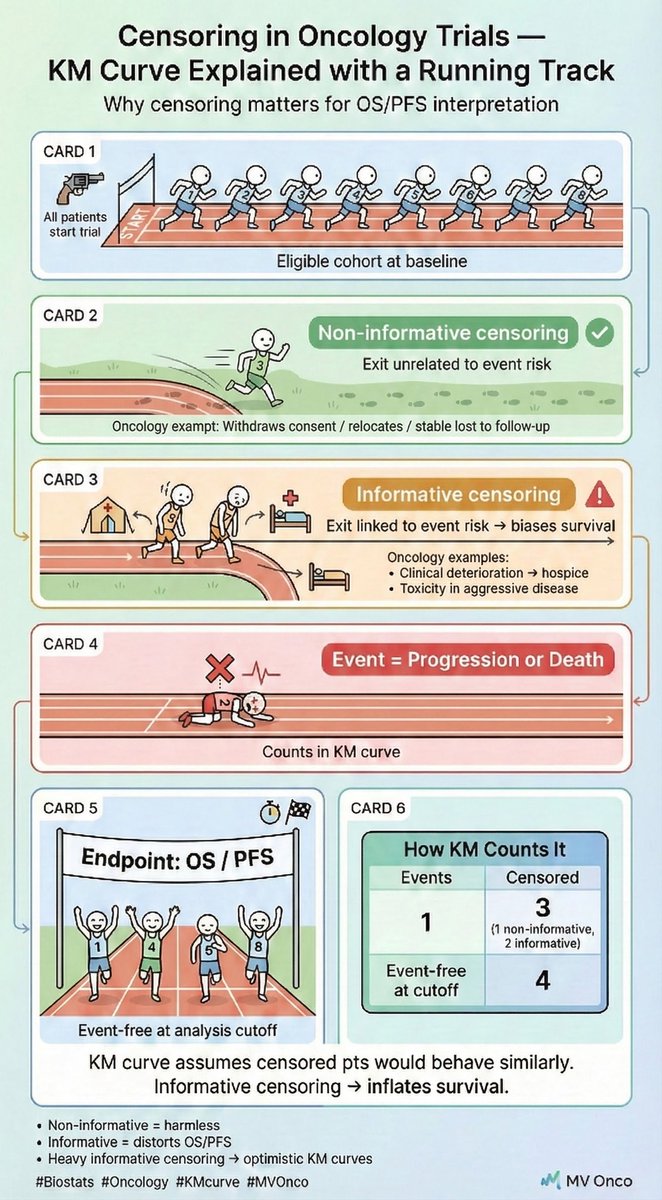
• Censoring = patient exits before event is observed
• Non-informative = exit unrelated to event risk
• Informative = exit linked to high event risk
• Informative censoring → inflates estimated OS/PFS
#Oncology #Biostats #KMcurve #SurvivalAnalysis #Trials #MVOnco
2
9
26
1,066
Dr Arun Chandran retweeted

22 Dec 2025
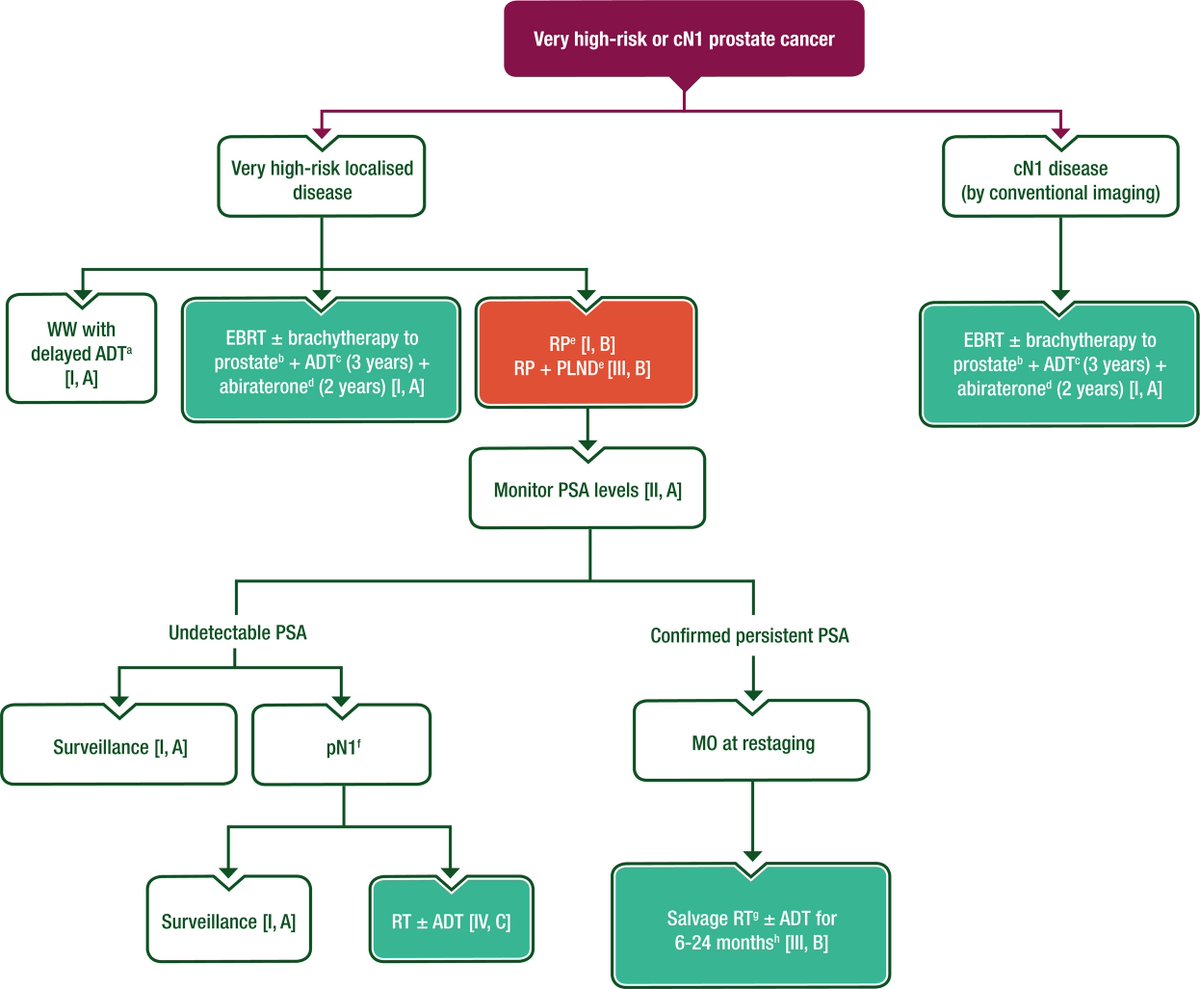
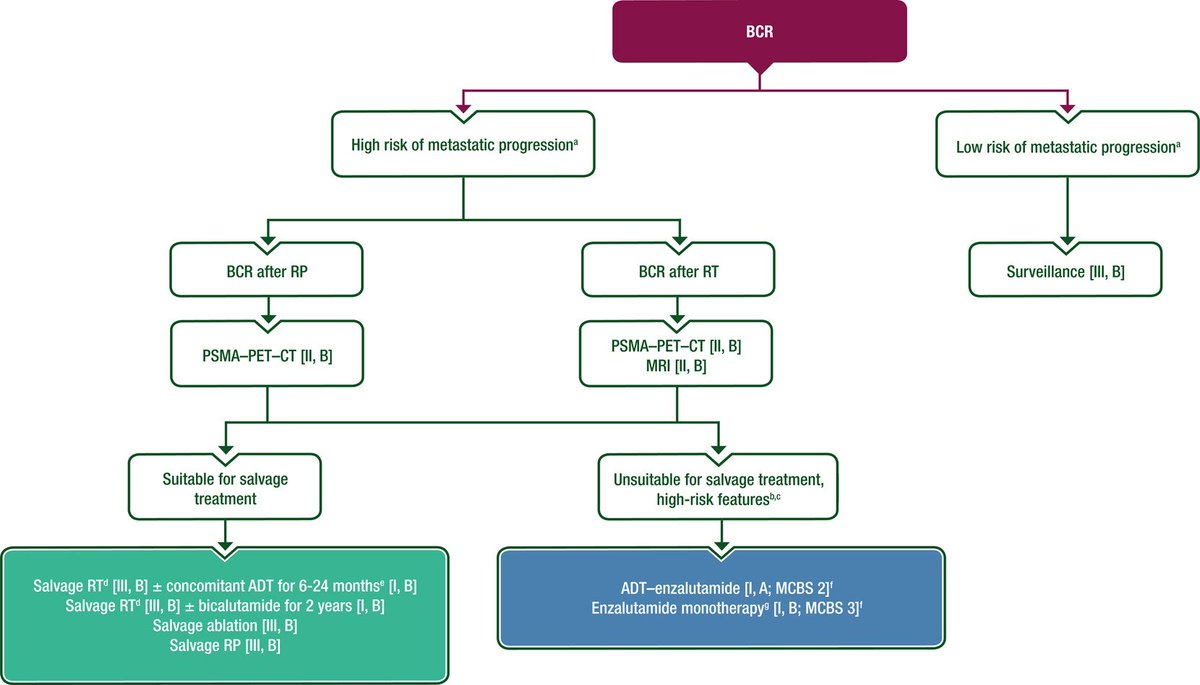
ESMO Clinical Practice Guideline: Local and locoregional prostate cancer!
@myESMO @APCCC_Lugano @AttardLab @Ecastromarcos @stefanofanti4 @Silke_Gillessen @Prof_Nick_James @piet_ost @MarkARubin1 @ChrisSweens1 @Tilki_De @ZilliThomas @alison_tree @OncoAlert
doi.org/10.1016/j.annonc.202…

5
46
144
8,742
Dr Arun Chandran retweeted
15 Dec 2025
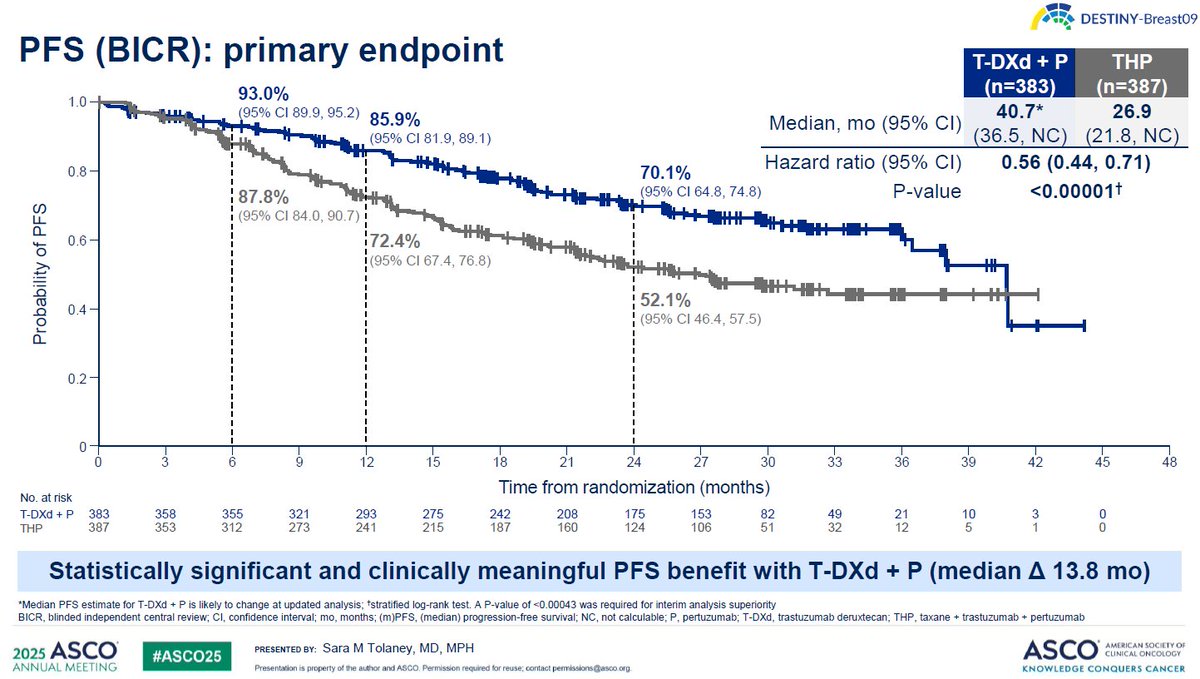
Why Induction Should Be Performed With T-DXd Pertuzumab (IMO)
The key distinction of DESTINY-Breast09 compared with HER2CLIMB-05 and PATINA is randomization at true treatment initiation. In both HER2CLIMB-05 and PATINA, only patients who did not progress during THP induction were randomized; early progressors were excluded by design.
DESTINY-Breast09 therefore captures the full early-risk population. At 6 months—approximately the end of induction—12.2% of patients in the THP control arm had already experienced a PFS event, compared with 7.0% in the T-DXd pertuzumab arm, corresponding to an absolute 5.2% reduction in early progression within the first 6 months. Importantly, this separation is not transient. By 12 months, the absolute PFS difference widens to 13.5%, indicating that T-DXd pertuzumab not only prevents early progression but continues to deepen benefit over time.
By contrast, PATINA and HER2CLIMB-05 never randomized the initial ~12% of patients who progressed during THP induction. Had induction been performed with T-DXd pertuzumab instead of THP, a substantial proportion of these early progressions—approximately 5% in absolute terms—might have been prevented. These patients would not have been lost upfront and could have proceeded to effective maintenance strategies rather than being excluded at the outset.
At present, because maintenance trials have uniformly used THP as induction, there are no prospective data evaluating palbociclib- or tucatinib-based maintenance following T-DXd pertuzumab induction. Nevertheless, indirect inferences from DESTINY-Breast09 suggest a pragmatic clinical strategy: in patients who develop tolerability issues, treatment may reasonably be initiated with T-DXd pertuzumab, followed by maintenance tailored to hormone receptor subtype once maximal disease control is achieved. This approach leverages early disease suppression while preserving the opportunity for durable, subtype-specific maintenance therapy.
Critically, in HR–positive disease, ET must remain an integral component of maintenance and should not be omitted.
15 Dec 2025

Great news💫
T-DXd plus pertuzumab has been approved by the FDA as a first-line treatment for HER2-positive mBC
5
29
86
14,522

20 Nov 2025
@NivaBupaSupport @Niva_Bupa @irdaindia Had a terrible experience with the agents from Niva Bupa. I was explaining that I was planning to change the policy rather than renew it, and they were issuing threats of terminating the policy.
Such crass, deplorable behavior.
2
50
20 Nov 2025
This person called Tanya was just shouting over the phone saying, all other agents are cheats and then just abused me and threatened termination of the policy. All this, beciased I dared to consider another policy. @Niva_Bupa
1
31
20 Nov 2025
@Niva_Bupa @NivaBupaSupport your people need to learn sales skills, not antagonize your customers with hate and threats. I was planning on renewal and have learnt my lesson. No way as a doctor will I ever recommend Niva Bupa to anyone. Hope the upper management knows this
1
42
Dr Arun Chandran retweeted

15 Nov 2025
🧬 PARP Maintenance After First-Line Chemo
Huge PFS benefit… but still no OS signal?
A 7-trial meta-analysis across 4013 pts.
🔍 Study Snapshot
🧪 7 RCTs
👩⚕️ Advanced-stage EOC (after response to platinum)
🧬 Subgroups: BRCA, HRD, BRCA-wt, HRP
🔪Surgery types: PCS vs NACT
💊 Agents: olaparib, niraparib, veliparib, senaparib, others
📈 Overall Results
🟢 PFS improved: HR 0.57
🔵 OS unchanged: HR 0.94
🔴 Grade 3 AEs ↑: RR 2.40
🧬 Molecular Breakdown
🔹 BRCA-mut
⭐ Strong PFS benefit (HR 0.40)
❌ No OS benefit
🔹 HRD
⭐ PFS HR 0.44
❌ No OS advantage
🔹 BRCA-wt
👍 Moderate PFS benefit (HR 0.62)
❌ No OS benefit
🔹 HRP
⚪ Minimal PFS activity (HR 0.74)
❌ OS neutral
🧵 Treatment Context
🏥 After NACT: HR 0.51
🏥 After PCS: HR 0.54
✔️ Works in both CR (HR 0.50) and PR (HR 0.57)
🔪 Across complete & incomplete cytoreduction
⚠️ Toxicity Landscape
🔥 Most toxicity: niraparib (RR 4.73)
🙂 Least toxicity: veliparib (RR 1.15)
🧩 Final Take
PARP maintenance = robust PFS benefit, strongest in BRCA/HRD.
But no OS benefit in any subgroup, and toxicity varies widely.
➡️ Use selectively, genotype-driven, toxicity-aware.
📖 Full paper in comment
#OncoTwitter #MedTwitter #GYNOnc #parp
@OncoAlert @myesmo @esmo_open @asco

2
21
56
4,368
Dr Arun Chandran retweeted
14 Oct 2025
💗 HER2CLIMB-05: TUKYSA takes the lead in HER2 MBC maintenance! 🚀
(PRESS RELEASE)
🧪 Phase 3 | n = 654 | 1st-line maintenance after chemo
Arms:
🔹 Tucatinib trastuzumab pertuzumab
🔹 Placebo trastuzumab pertuzumab
🎯 Primary endpoint met:
✨ Statistically & clinically meaningful PFS improvement by investigator assessment
💪 Safety:
Tolerable & consistent with known profiles of individual drugs
📊 Why it matters:
• HER2 ≈ 15–20 % of breast cancers
• 5-yr OS ~ 41–47 %
• SOC unchanged since 2012 → most progress < 2 yrs
➡️ HER2CLIMB-05 offers a potential chemo-free maintenance path 🌈
💡 Takeaway:
TUKYSA (tucatinib) may soon move from 3rd-line → 1st-line maintenance, shaping a new standard of care in HER2 MBC 💥
📖 Full release: businesswire.com/news/home/2…
#OncoTwitter #MedTwitter #BreastCancer #HER2 #Tucatinib #ESMO #ASCO
@OncoAlert @myesmo @esmo_open @Pfizer @JournalofOncology @ASCO @DFCI_BreastOnc
12
37
3,427
Dr Arun Chandran retweeted

20 Sep 2025
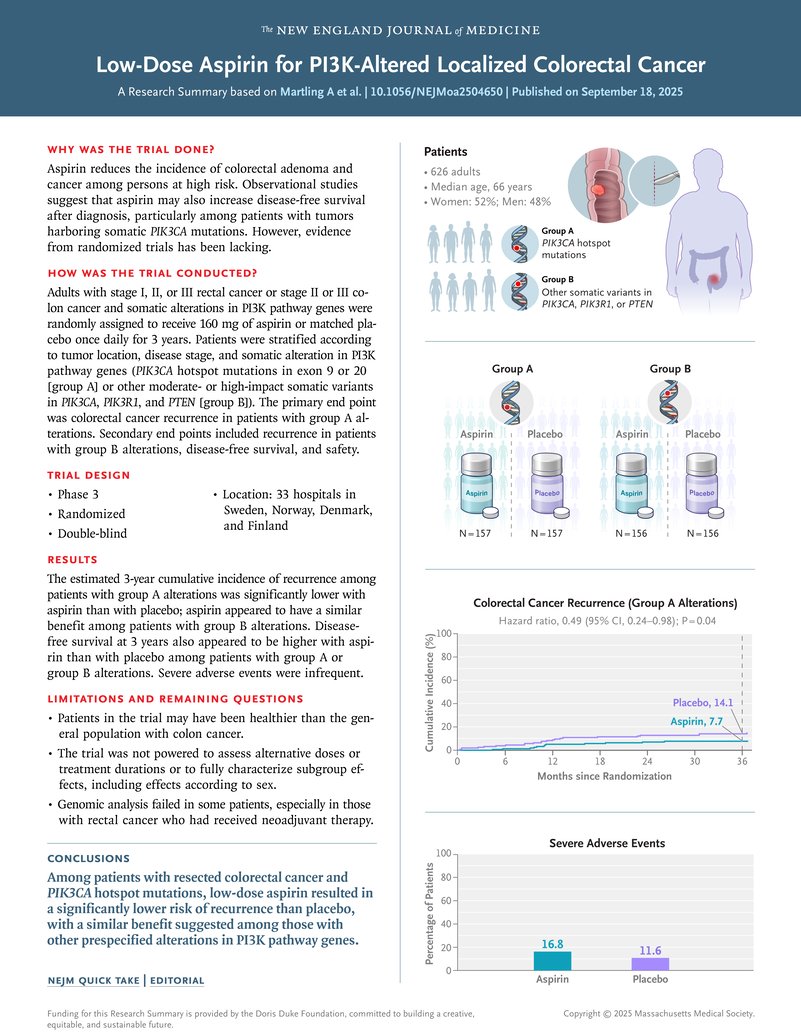
NEJM 2025 (ALASCCA): Low-dose aspirin (160 mg) in PI3K-altered stage I–III CRC ↓ 3-yr recurrence (7.7% vs 14.1%, HR 0.49).
🔎 6,397 pts screened → 2,980 sequenced → 1,103 (37%) had PI3K-pathway mutations
Hotspot exon 9/20: 17%
Other PI3K/PTEN: 20%
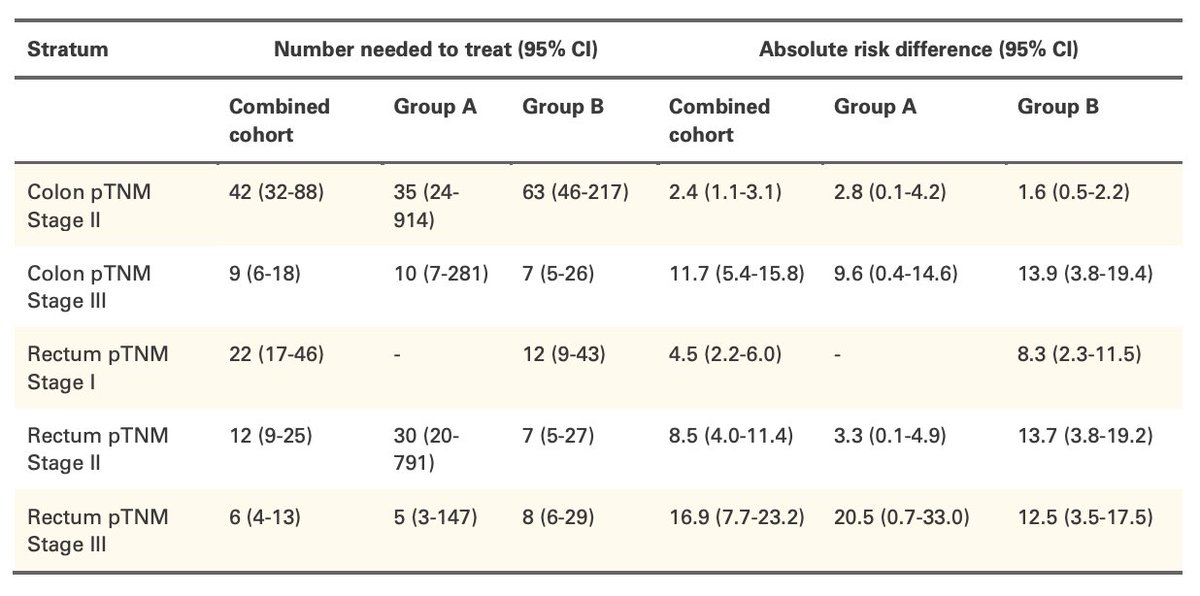
📊 NNT:
Colon II → weak (42)
Colon III → strong (9)
Rectum III → best (6)
⚠️ Borderline stats, no OS yet, ↑ severe AEs.( 16.8 vs 11.6 % )
👉 Signal clearest in stage III; stage II benefit marginal.
Promising, not yet blanket SOC. Wait for longer follow-up @dr_yakupergun
@GIMedOnc @NiuSanford @OncBrothers
3
28
88
7,766
Dr Arun Chandran retweeted
28 Jun 2025
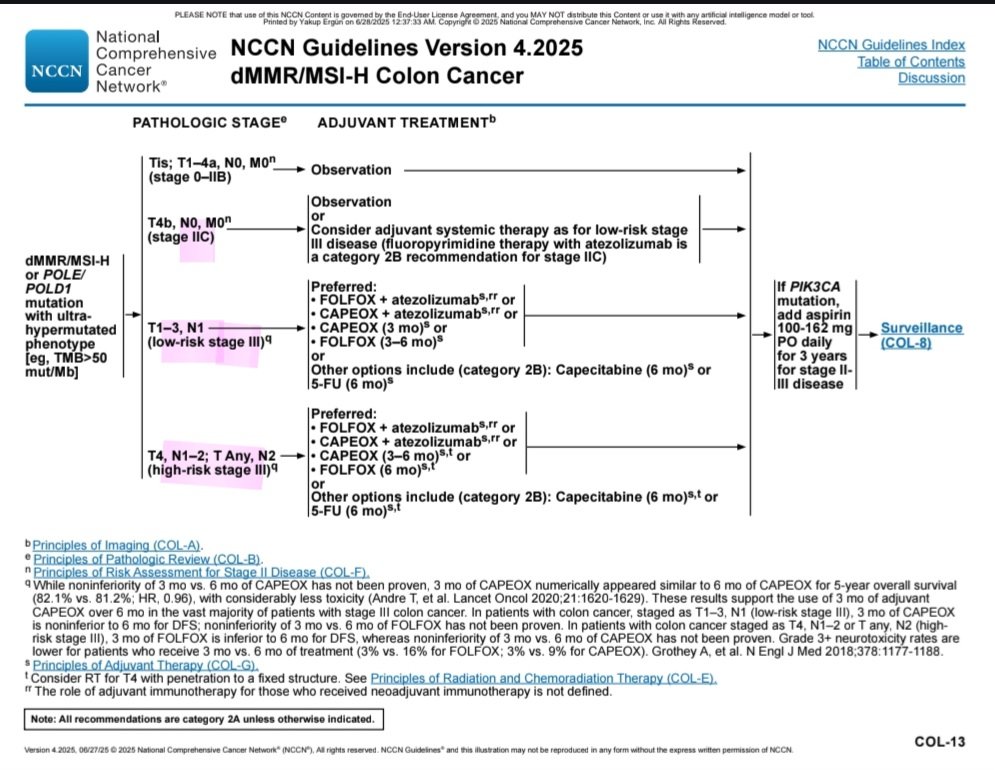
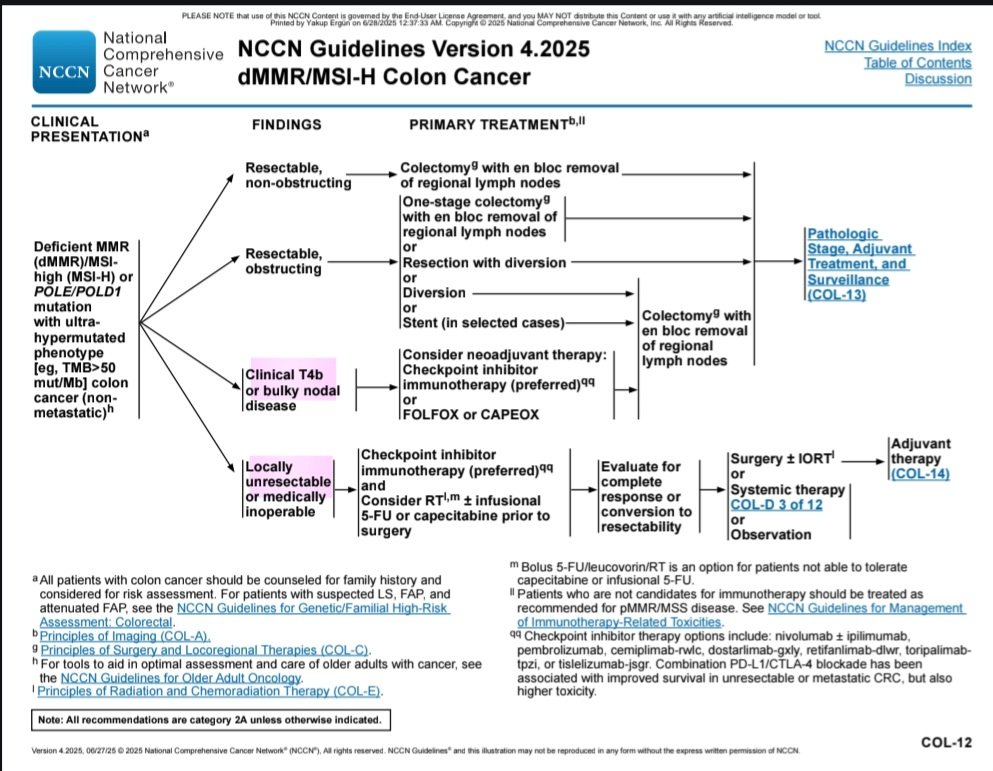
The NCCN has included adjuvant atezolizumab (for 1 year) in the treatment of stage pT2c–III dMMR colon cancer.
Given the positive trial results, its inclusion is certainly appropriate. However, the guideline adopts a somewhat conservative stance regarding neoadjuvant ICI use, limiting it only to cases with cT4b tumors or bulky positive lymph nodes.
In the NICHE-2 study, however, 57% of patients were staged as cT3–cT4a. Achieving a 3-year DFS of 100% with just 4 weeks of neoadjuvant ICI suggests that restricting this approach to such a narrow population may not be entirely reasonable.
We recognize the limitations of clinical staging, but these can be improved. In my view, neoadjuvant strategies that demonstrate a “less is more” effect deserve broader clinical adoption. Trials like NADINA, NICHE-2, and perhaps CheckMate-816( !?) point in this direction.
5
47
126
19,593
19 Jun 2025
🧪 NAPOLI-3 Trial: First-Line Treatment in Metastatic Pancreatic Cancer
Phase III, randomized, open-label trial
🧬 Study Arms
📌 NALIRIFOX (q2 weeks)
Liposomal Irinotecan (nal-IRI) 50 mg/m²
Oxaliplatin 60 mg/m²
Leucovorin 400 mg/m²
5-FU 2400 mg/m² (46 hr infusion)
🆚
📌 Gemcitabine Nab-Paclitaxel (standard regimen)
📊 Key Outcomes
NALIRIFOX VS Gem-NabPac
OS 11.1 months VS 9.2 months
PFS 7.4 months VS 5.6 months
ORR 41.8% VS 36.2%
Grade ≥3 AEs 70% VS 68%
🚨 Adverse Events
NALIRIFOX: More diarrhea, nausea
Gem-NabPac: More neuropathy
📌 Take-Home Message
✅ NALIRIFOX improves OS and PFS vs Gem-NabPac
✅ Suitable for fit patients (ECOG 0–1)
✅ Non-taxane option — helpful in neuropathy-prone patients
1
184
5 Jun 2025
🥈 Secured 2nd prize at the Interdepartmental Quiz @ Aster MIMS!
With 50 teams competing, it was a thrilling test of trivia covering health, business, and current affairs.
Proud of the teamwork and quick thinking! 💡🧠🔥
#QuizTime #AsterMIMS #TriviaChampions #MedicalQuiz #Teamwork #HealthcareAndBeyond


1
62
5 Jun 2025
🎓 Proud moment from #AsterMIMS!
Two of our studies by final-year residents were published online at #ASCO25:
🧬 NSCLC study led by Dr. Sreedhar Cherulli highlights disparity in access to targeted therapy despite widespread NGS testing.
🩸 HCC study led by Dr. Sireesh Kumar Ch shares real-world insights on atezolizumab bevacizumab from South India.
Kudos to both! 🙌
#GlobalOncology #LungCancer #LiverCancer #DNBResidents #MedicalOncology #CancerCare #RealWorldData #ASCO2025


1
113
Dr Arun Chandran retweeted

14 May 2025
1/n..Under the aegis of @CRSF_IN and guidance of @DrVijayPatil11, @VanitaNoronha, Dr. Kumar sir, our long-awaited study on Triple Metronomic therapy was published in @TheCancerLetter. Please read and comment. kwnsfk27.r.eu-west-1.awstrac…

4
5
25
2,248
3 May 2025
Kudos to Dr Sanudev Sadanandan for organizing ONCOSCOPE 2025, a groundbreaking conference that raises awareness about Oncology among undergraduates.🎉🙌🎉
Honored to have represented medical oncology, highlighting the progress of cancer treatment over the ages 💉💊⚕️⚕️

1
52

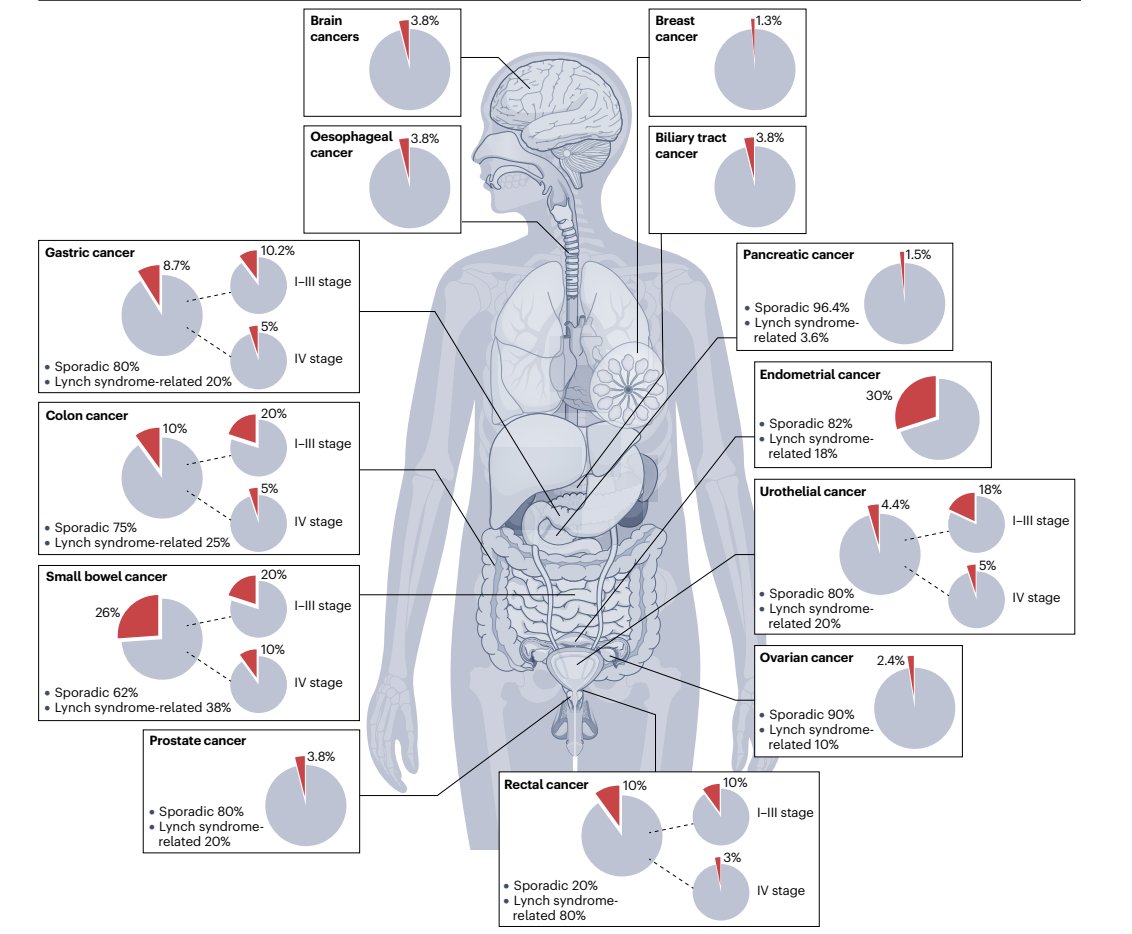
🧬 MSI-H = hallmark of mismatch repair (MMR) deficiency.
🧵 Prevalence: ~30% endometrial, ~10% CRC, ~8% gastric.
But not all MSI-H/dMMR tumors are alike:
1️⃣ MSH2/MSH6 loss → ↑ TMB, better ICI response
2️⃣ PTEN/AKT1 mutations → ICI resistance
Checkpoint blockade is now 1L in CRC & endometrial.
#MSI #Immunotherapy #Biomarkers
🔗 nature.com/articles/s41571-0…
4
135
356
29,368