
Jun 14
Breaking Access Barriers to Autologous Stem Cell Transplantation and Chimeric Antigen Receptor T Cell Therapy in Hematologic Malignancies @ASTCT @nmdp_org
astctjournal.org/article/S26…
#CARTCellTherapy #Celltherapy #patientaccess
1
4
49

At this upcoming ASTCT Cord Blood SIG webinar on July 1, researchers will discuss the role of cord blood as a graft source for patients with difficult-to-cure acute leukemia, exploring clinical outcomes and real-world applications through roundtable discussion.
Register now and join colleagues for a conversation on the latest developments in cord blood transplantation: ow.ly/ONCc50Z8BFc

1
4
237
In this ASTCT Board Member Spotlight, Sophie Paczesny, MD, PhD, reflects on her work advancing GVHD biomarker research and immunotherapy innovation, shares her priorities as an ASTCT board member and offers insights on the current opportunities and challenges in the field.
Read the full spotlight: ow.ly/vpkP50Z8BGz

1
241

🧬 EHA2026 DLBCL — Speaker: Guilherme Perini
Talk: Choose the Next Move: To Be or Not To Be Chemo-Free
⚖️ CAR-T eligibility ≠ ASCT eligibility
A key practical message: many patients considered “not transplant fit” may still be reasonable candidates for CAR-T, because eligibility thresholds and toxicity profiles differ.
⚡ CAR-T eligible — broader than many clinicians think
👴 Very advanced age alone should not automatically exclude CAR-T
🫀 Moderate comorbidities may be acceptable with careful MDT review
🧪 Creatinine clearance >30 mL/min may be sufficient in selected patients
🎯 Real-world CAR-T data support feasibility in older and less-fit patients, including transplant-ineligible populations.
🧫 Transplant eligible — usually stricter selection
💪 Needs adequate performance status
🫀 Significant cardiac dysfunction may limit HDT/ASCT
🧪 Organ reserve matters more because of high-dose chemotherapy
👴 In elderly patients, strict selection is essential to avoid excess toxicity
🔁 Treatment direction in R/R DLBCL
⏱️ Primary refractory / relapse ≤12 months → consider CAR-T if eligible
⏱️ Relapse >12 months → salvage therapy → ASCT if chemosensitive and fit
🚫 If not fit or not accessible → off-the-shelf options become crucial
ASTCT guidance supports CAR-T for primary refractory/early relapse and ASCT for late relapse responding to salvage therapy.
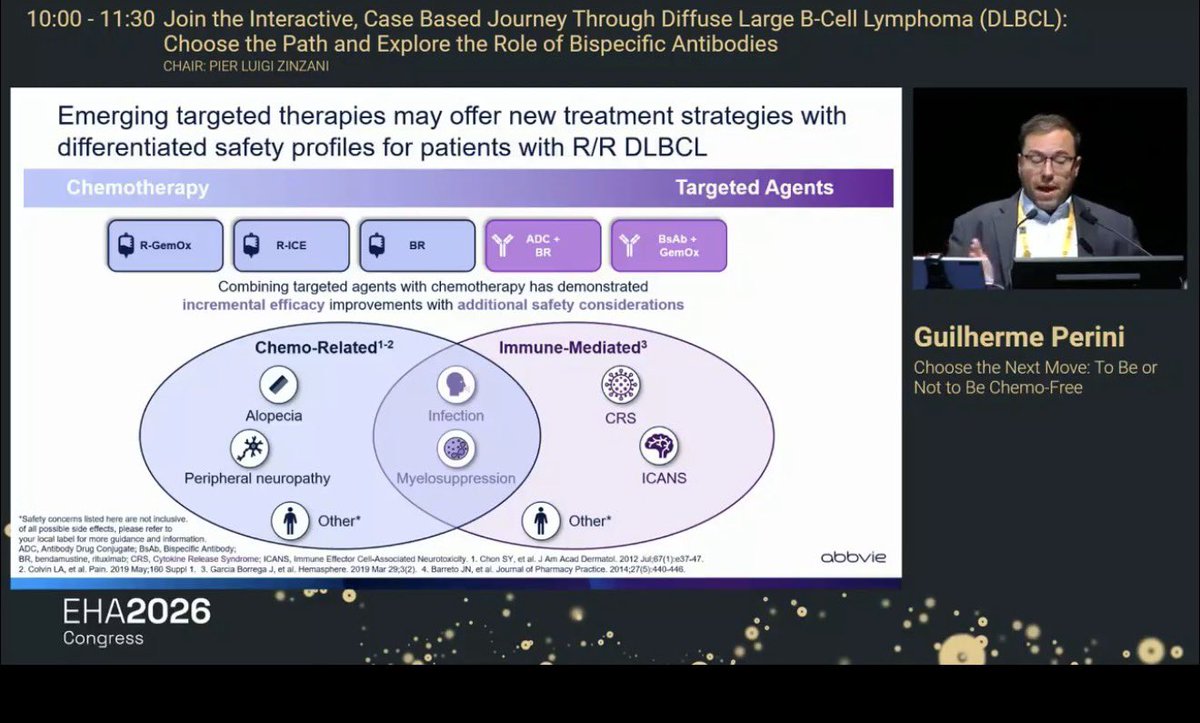
🧬 Emerging targeted strategies: efficacy vs toxicity balance
Classic chemo platforms:
💊 R-GemOx
💊 R-ICE
💊 BR
Targeted / immune platforms:
🎯 ADC BR
🧲 Bispecific antibody GemOx
⚠️ Toxicity patterns differ
Chemo-related: alopecia, peripheral neuropathy, myelosuppression
Shared: infection cytopenias
Immune-mediated: CRS and ICANS
This is why “chemo-free” is not automatically “toxicity-free”; it is a different toxicity language.
🎯 Practical takeaway
For R/R DLBCL, the real question is not only “CAR-T vs transplant,” but:
🧬 disease timing
💪 patient fitness
🧪 organ reserve
🌍 access
⚠️ toxicity tolerance
🚀 availability of off-the-shelf targeted options
✅ Perfect MCQ
A 76-year-old patient with R/R DLBCL relapsed 8 months after R-CHOP. ECOG 1, controlled comorbidities, CrCl 42 mL/min, not considered ASCT-fit. What is the most appropriate conceptual next step if available?
A. Exclude from CAR-T because he is not ASCT eligible
B. Consider CAR-T eligibility through MDT assessment
C. Observation only
D. R-CHOP rechallenge
✅ Answer: B — Consider CAR-T eligibility through MDT assessment
ASCT ineligibility does not automatically mean CAR-T ineligibility; CAR-T can be feasible in selected older or less-fit patients, while early relapse ≤12 months favors CAR-T when accessible.
#EHA2026 #DLBCL #RelapsedDLBCL #CART #ASCT #Bispecifics #Glofitamab #Epcoritamab #GemOx #Hematology #KFSHRC
2
1
297
🧬 EHA2026 DLBCL — Speaker: Guilherme Perini
Talk: Choose the Next Move: To Be or Not To Be Chemo-Free
🚨 First relapse DLBCL = decision depends on 2 major variables
⏱️ Timing of relapse after 1L therapy
💪 Fitness / eligibility for CAR-T or ASCT
⚡ Relapse ≤12 months = CAR-T territory if eligible
For early relapse or primary refractory LBCL, anti-CD19 CAR-T is the preferred curative-intent strategy for fit patients. Key options include axi-cel and liso-cel.
🧫 Relapse >12 months = consider ASCT if transplant-eligible
Late relapse remains a setting where salvage immunochemotherapy → HDT/ASCT can still be appropriate if the patient achieves CR/PR. ASTCT recommendations support ASCT consolidation for late-relapse DLBCL patients responding to second-line therapy.
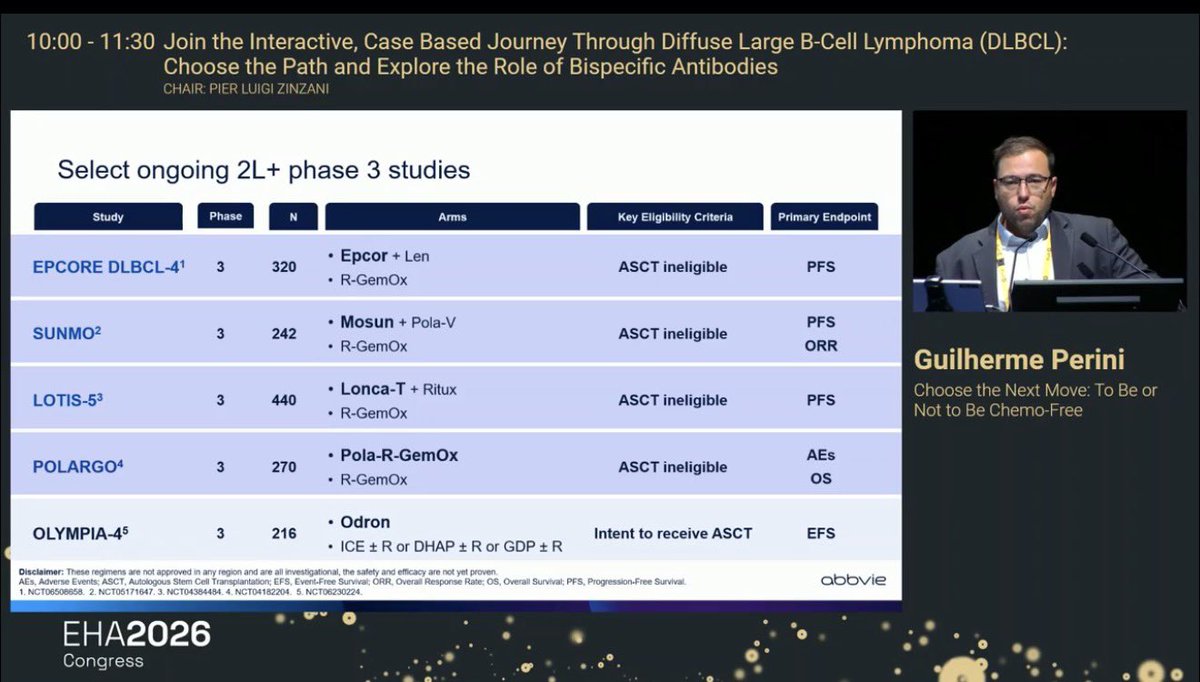
🧲 CAR-T ineligible / ASCT ineligible patients need accessible off-the-shelf options
The slide highlights practical regimens such as:
🧬 Glofitamab GemOx
🧬 Epcoritamab GemOx
🧬 R-GemOx
🧬 Tafasitamab-lenalidomide
🧬 Pola-BR
These are especially relevant when patients are not fit for cellular therapy or cannot access CAR-T/ASCT.
🌎 LATAM treatment gaps are clinically important
Prof. Perini emphasized that R/R DLBCL management is not only biology-driven; it is also access-driven:
🔬 21% of centers lack IHC
⏳ 56% wait ≥3 weeks for pathology report
🖥️ 41% have PET-CT access
🧬 only 15% have NGS
💊 restricted access remains high for polatuzumab, tafasitamab, glofitamab, and epcoritamab
⚡ CAR-T approval/access is largely concentrated in Brazil in the presented regional data
🎯 Key message from the LATAM slide
There is a real need for available, off-the-shelf, chemo-free or chemo-light therapies for patients unable or unwilling to receive CAR-T.
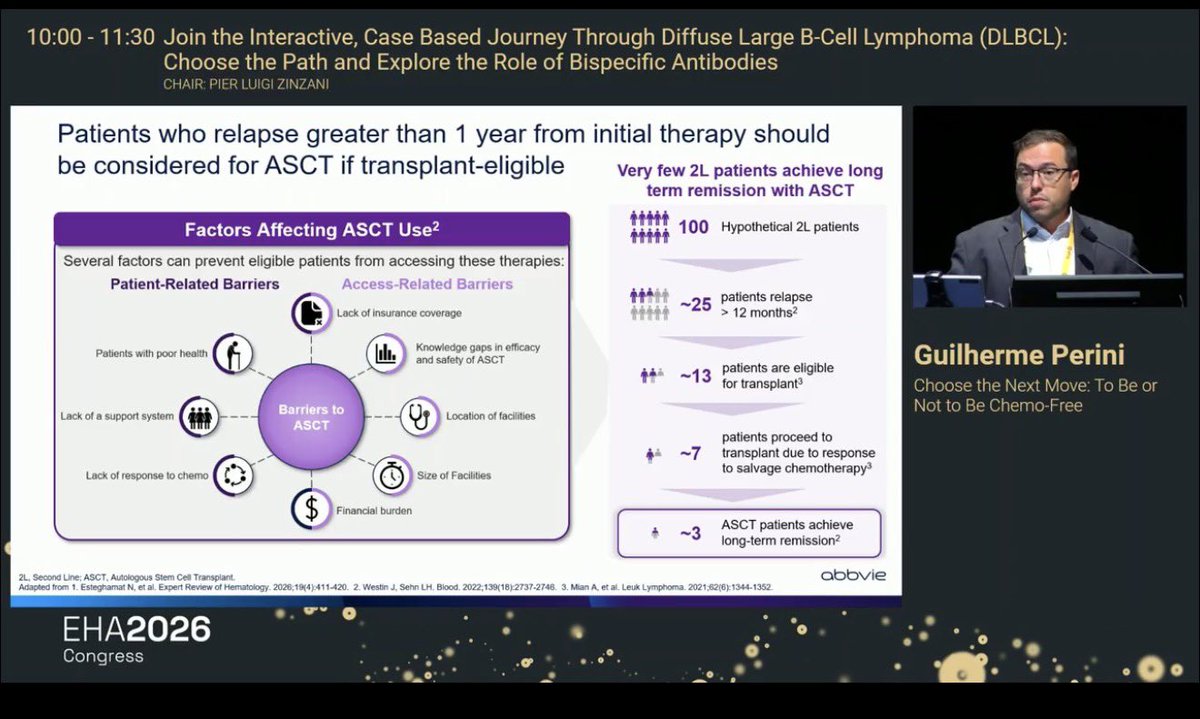
🧠 ASCT reality check
Even among patients relapsing >12 months, only a minority proceed to transplant and achieve durable remission. The slide’s funnel illustrates that from 100 hypothetical 2L patients, only ~3 may ultimately achieve long-term remission with ASCT. This makes patient selection and access to novel agents critical.
✅ Perfect MCQ
A 59-year-old fit patient with DLBCL relapses 7 months after completing R-CHOP. PET confirms active disease. Which strategy is most appropriate if available?
A. Salvage chemotherapy followed by ASCT regardless of response
B. Anti-CD19 CAR-T therapy
C. Observation
D. Rituximab monotherapy
✅ Answer: B — Anti-CD19 CAR-T therapy
Early relapse ≤12 months is now a CAR-T–preferred setting for eligible patients, with axi-cel and liso-cel supported by second-line randomized data and contemporary treatment algorithms.
#EHA2026 #DLBCL #Lymphoma #RelapsedDLBCL #CART #ASCT #Bispecifics #Glofitamab #Epcoritamab #PolaBR #Hematology #KFSHRC


1
10
20
1,089





This recognition is truly well-deserved. I had the opportunity to attend his presentation at the recent ASTCT meeting, and it was exceptionally insightful.

Huge congratulations, @NicoGagelmann, on the EHA Young Investigator Award! No one deserves it more. Your passion, creativity, and commitment to advancing our field make this recognition incredibly well earned.

4
501


Jun 10
We would like to inform you that your post has been published on OncoDaily. Thank you for sharing.
oncodaily.com/voices/al-ola-…
2
43
For 30 years, 'Transplantation and Cellular Therapy' has advanced the science and practice of HCT and cellular therapies. @ASTCT_Journal
ASTCT President Margy MacMillan reflects on the journal's impact and continued importance to the field.
ow.ly/5kSm50Z8jwa

1
4
364

Jun 9
Podcast: Unraveling Key Hematologic Oncology Developments at ASCO 2026
ASTCT Talks
June 9, 2026
#science #technology #engineering #medicine #health
@Spotify
ift.tt/qQ0hO7r
23

Excited to host and hear from:
Dr. Corey Cutler @DrCCutler @ASTCT
Dr. Nikhil Munshi @NikhilMunshiMD @Myeloma_Society

2/ This isn’t just another conference.
Faculty includes leaders of major societies, including:
▶️ASON
▶️American Society for Transplantation and Cellular Therapy (ASTCT)
▶️Int. Myeloma Society (IMS)
Along with division chiefs, directors, and internationally recognized experts.
1
223

2/ This isn’t just another conference.
Faculty includes leaders of major societies, including:
▶️ASON
▶️American Society for Transplantation and Cellular Therapy (ASTCT)
▶️Int. Myeloma Society (IMS)
Along with division chiefs, directors, and internationally recognized experts.
1
1
2
388
Explore two hot topics with the ASTCT Pharmacy SIG! Join the journal club to discuss:
✅Brexucabtagene autoleucel in BTKi naive relapsed/refractory mantle cell lymphoma
✅Carfilzomib, lenalidomide, and dexamethasone vs lenalidomide maintenance post transplant in multiple myeloma
Register today: ow.ly/yfPk50Z8joQ
2
341

Always proud of our superstar pharmacist leader @kczmj ! Her outstanding work, innovation, and dedication are helping shape the future of cellular therapy.
#mmsm #myeloma #MedEd #medtwitter #USMIRC @Larvol @ASTCT @US_HMC @USMIRCNEWS @MedwatchKate @oncodaily
astct.org/Nucleus/Article/me…
1
3
9
572