
❤️ Venous Return vs Cardiac Function: Who Really Drives the Circulation?
For decades, intensivists have debated whether cardiac output (CO) is determined primarily by the heart or by venous return (VR). The answer is that both are inseparable components of the same system. At steady state, the heart can only pump the blood that returns to it.
Key physiological concepts:
🔹 Venous return is driven by the gradient between mean systemic filling pressure (Pmsf) and right atrial pressure (RAP).
🔹 Pmsf depends on stressed blood volume and venous tone.
🔹 Cardiac output equals venous return at equilibrium.
🔹 The operating point of the circulation is where the cardiac function curve intersects the venous return curve.
Clinical implications:
✅ In septic shock, vasodilation reduces effective circulating volume and venous return. Fluids increase stressed volume, while vasopressors recruit blood from the unstressed to the stressed compartment, restoring venous return and cardiac output.
✅ In cardiogenic shock, the failing heart becomes the major limitation. Increasing venous return often raises filling pressures more than cardiac output, worsening congestion and pulmonary edema.
✅ Venous congestion itself may impair organ perfusion even when cardiac output appears preserved.
The practical message is simple:
📌 Low cardiac output is not always a pump problem.
📌 Low venous return is not always a volume problem.
📌 Effective hemodynamic management requires identifying whether the primary limitation is venous return, cardiac performance, or both.
Understanding the interaction between Guyton physiology and Frank-Starling physiology remains essential for fluid therapy, vasopressor selection, and shock management in the ICU.
#CriticalCare #Hemodynamics #Shock #SepticShock #CardiogenicShock #ICU #POCUS #FluidResponsiveness #CardiacOutput #IntensiveCare
Reference 📚
Cecconi M, Ostermann M, Pinsky MR. Venous return versus cardiac function: who drives the circulation? Intensive Care Medicine. 2026. DOI: 10.1007/s00134-026-08499-y.
ALT
2
63
165
5,000

Anesthesiology,6月号(June), 2026
Keyword: セボフルラン(Sevoflurane), プロポフォール(Propofol), 麻酔報酬(AnesthesiaReimbursement), 麻酔後無呼吸(PostanesthesiaApnea), 人身売買(HumanTrafficking), ミトコンドリア(Mitochondria), 胃内容量(GastricVolume), フレッシュガス流量(FreshGasFlow), 周術期体験(PerioperativeExperience), うつ(Depression), 心拍出量(CardiacOutput), PANoptosis(PANoptosis), 術後せん妄(PostoperativeDelirium), ECMO(ExtracorporealMembraneOxygenation), デクスメデトミジン(Dexmedetomidine), 胸部大動脈瘤(ThoracicAorticAneurysm), 生成AI(ArtificialIntelligence), プライベートエクイティ(PrivateEquity), 麻酔後無呼吸(PostanesthesiaApnea), 麻酔後無呼吸(PostanesthesiaApnea), 産科麻酔(ObstetricAnesthesia), 手術室(OperatingRoom), 音楽(Music), 低栄養(Malnutrition), 研究資金(ResearchFunding), デクスメデトミジン(Dexmedetomidine), LGBTQIA (LGBTQIA), ミトコンドリア(Mitochondria), ストレス(Distress), ストレス(Distress), 肺リクルータビリティ(Recruitability), 肺リクルータビリティ(Recruitability), 肺リクルータビリティ(Recruitability), 神経興奮性(NerveExcitability), 神経興奮性(NerveExcitability), 腎障害(KidneyInjury), 腎障害(KidneyInjury), 腎障害(KidneyInjury), 小児麻酔(PediatricAnesthesia), 小児麻酔(PediatricAnesthesia), ケタミン(Ketamine), ケタミン(Ketamine), 慢性疼痛(ChronicPain), 慢性疼痛(ChronicPain), シナプス前タンパク質(PresynapticProtein), シナプス前タンパク質(PresynapticProtein), 外科史(HistoryOfSurgery), 妊娠糖尿病(DiabetesMellitus), 神経ブロック(NerveBlock), 訂正(Erratum), 腰神経叢ブロック(LumbarPlexusBlock), ポッドキャスト(Podcast), プロポフォール(Propofol)
1
2
404

May 29
Journal of Clinical Ultrasound
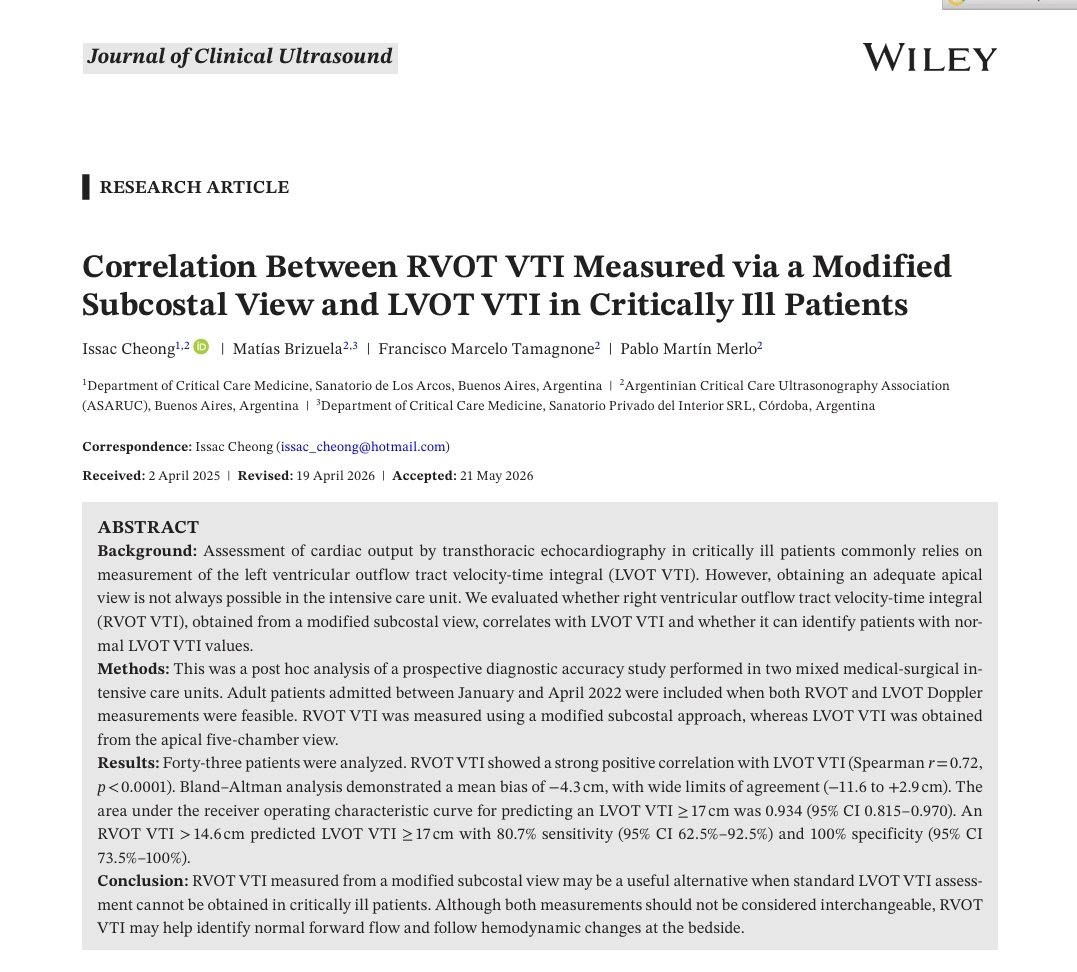
Correlation Between RVOT VTI Measured via a Modified Subcostal View and LVOT VTI in Critically Ill Patients
DOI: 10.1002/jcu.70280
Shareable-link: onlinelibrary.wiley.com/shar…
#POCUS #VTI #Strokevolume #cardiacoutput #Echo
5
18
955

facebook.com/share/r/1SpZbnv…
🩸💡 Your Heart Beats 100,000 Times Daily Here's Exactly Where Every Drop Goes ✅
This isn't circulation. This is masterful biological engineering.
🔬 Know your physiology. Master your cardiology.
#Cardiology #CardiacOutput #HeartFunction #Hemodynamics
13
66
3,064

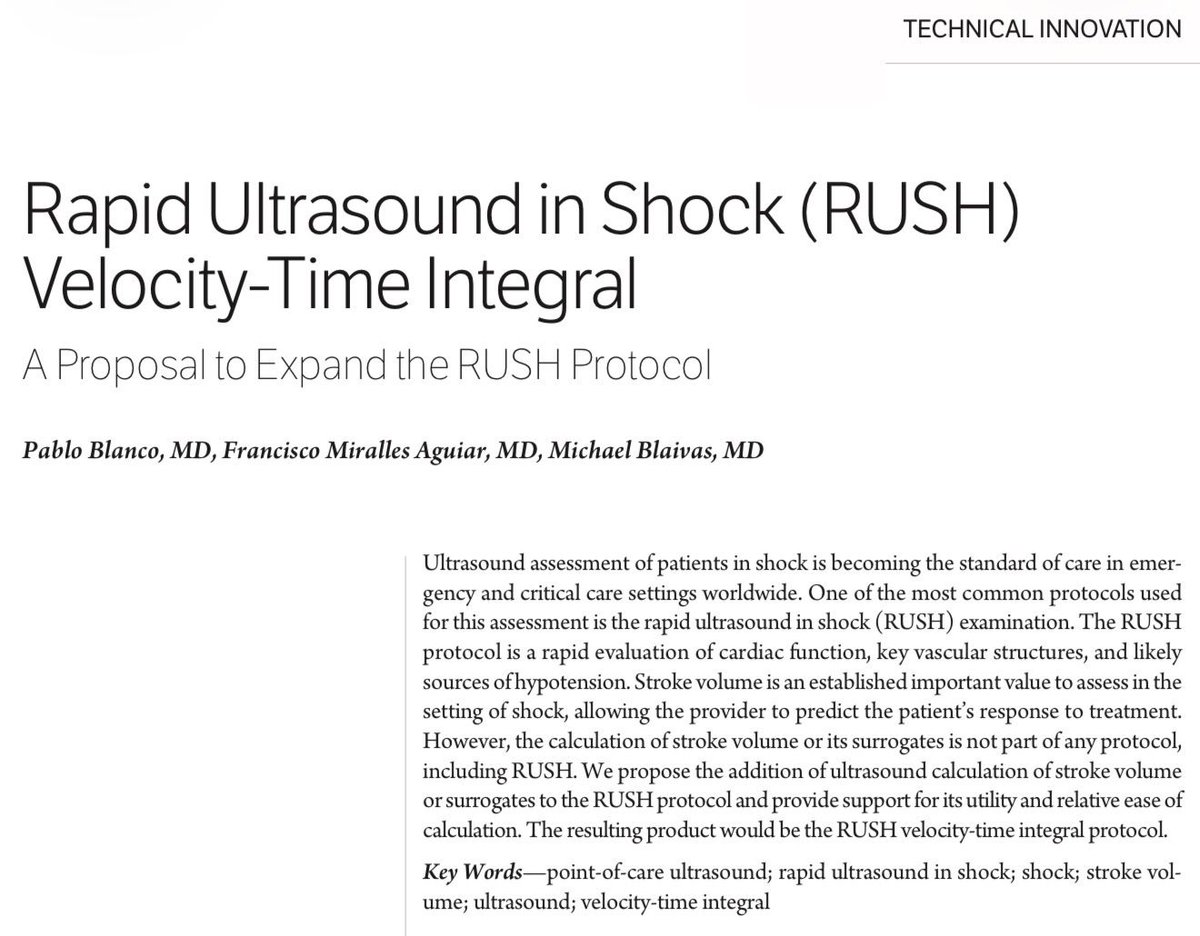
🫀🔊 𝗥𝗨𝗦𝗛-𝗩𝗧𝗜: 𝗲𝘃𝗮𝗹𝘂𝗮𝗰𝗶𝗼́𝗻 𝗲𝗻 𝘁𝗶𝗲𝗺𝗽𝗼 𝗿𝗲𝗮𝗹 🚨
@WileyGlobal @curromir
👇🏼👇🏼👇🏼👇🏼
📑🔗🔑🔓
t.me/ClubCrit
⬇️⬇️⬇️⬇️
🧵👇
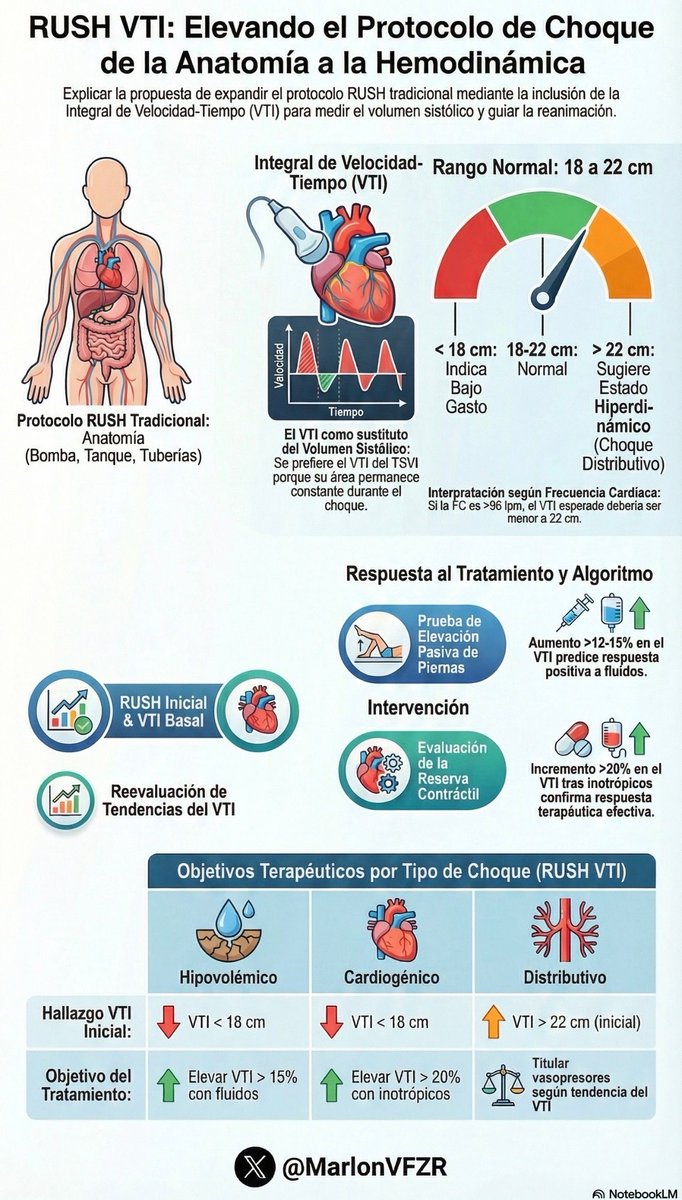
📌El artículo propone ampliar el protocolo 𝙍𝙐𝙎𝙃 agregando el 𝙑𝙏𝙄 para no quedarnos solo con la “causa” del shock, sino también con algo todavía más útil a pie de cama: 𝙘𝙤́𝙢𝙤 𝙚𝙨𝙩𝙖́ 𝙚𝙡 𝙫𝙤𝙡𝙪𝙢𝙚𝙣 𝙨𝙞𝙨𝙩𝙤́𝙡𝙞𝙘𝙤 𝙮 𝙘𝙤́𝙢𝙤 𝙘𝙖𝙢𝙗𝙞𝙖 𝙘𝙤𝙣 𝙚𝙡 𝙩𝙧𝙖𝙩𝙖𝙢𝙞𝙚𝙣𝙩𝙤 🎯.
🧠🔍 𝙍𝙚𝙘𝙤𝙧𝙙𝙖𝙩𝙤𝙧𝙞𝙤 𝙧𝙖́𝙥𝙞𝙙𝙤: 𝙍𝙐𝙎𝙃 = 𝙥𝙪𝙢𝙥, 𝙩𝙖𝙣𝙠, 𝙥𝙞𝙥𝙚𝙨
El RUSH clásico evalúa:
🫀 𝙥𝙪𝙢𝙥 = corazón/pulmón
🫗 𝙩𝙖𝙣𝙠 = volumen/IVC/abdomen
🩸 𝙥𝙞𝙥𝙚𝙨 = aorta/venas
👉 Muy útil para identificar el mecanismo del shock, pero 𝙣𝙤 𝙞𝙣𝙘𝙤𝙧𝙥𝙤𝙧𝙖 𝙜𝙖𝙨𝙩𝙤 𝙘𝙖𝙧𝙙𝙞𝙖𝙘𝙤 𝙣𝙞 𝙫𝙤𝙡𝙪𝙢𝙚𝙣 𝙨𝙞𝙨𝙩𝙤́𝙡𝙞𝙘𝙤 de forma directa 😮💨.
📏💓 𝙇𝙖 𝙥𝙧𝙤𝙥𝙪𝙚𝙨𝙩𝙖: 𝙨𝙪𝙢𝙖𝙧 𝙚𝙡 𝙑𝙏𝙄 𝙙𝙚𝙡 𝙩𝙧𝙖𝙘𝙩𝙤 𝙙𝙚 𝙨𝙖𝙡𝙞𝙙𝙖 𝙙𝙚𝙡 𝙑𝙄 (𝙇𝙑𝙊𝙏-𝙑𝙏𝙄) ✅
El volumen sistólico por eco se estima como:
🧮 𝙖́𝙧𝙚𝙖 𝙙𝙚𝙡 𝙇𝙑𝙊𝙏 × 𝙑𝙏𝙄 𝙙𝙚𝙡 𝙇𝙑𝙊𝙏
Pero como medir bien el diámetro del LVOT en urgencias puede ser engorroso 😵💫, el artículo propone usar el 𝙑𝙏𝙄 𝙘𝙤𝙢𝙤 𝙨𝙪𝙗𝙧𝙧𝙤𝙜𝙖𝙙𝙤 𝙥𝙧𝙖́𝙘𝙩𝙞𝙘𝙤 𝙙𝙚𝙡 𝙫𝙤𝙡𝙪𝙢𝙚𝙣 𝙨𝙞𝙨𝙩𝙤́𝙡𝙞𝙘𝙤.
👉 En otras palabras: si el área cambia poco, 𝙡𝙤𝙨 𝙘𝙖𝙢𝙗𝙞𝙤𝙨 𝙙𝙚𝙡 𝙑𝙏𝙄 𝙧𝙚𝙛𝙡𝙚𝙟𝙖𝙣 𝙡𝙤𝙨 𝙘𝙖𝙢𝙗𝙞𝙤𝙨 𝙙𝙚𝙡 𝙨𝙩𝙧𝙤𝙠𝙚 𝙫𝙤𝙡𝙪𝙢𝙚.
📊🫀 ¿𝙌𝙪𝙚́ 𝙫𝙖𝙡𝙤𝙧𝙚𝙨 𝙤𝙧𝙞𝙚𝙣𝙩𝙖𝙣?
En personas sanas, el 𝙇𝙑𝙊𝙏-𝙑𝙏𝙄 𝙣𝙤𝙧𝙢𝙖𝙡 suele estar alrededor de 𝟭𝟴–𝟮𝟮 𝙘𝙢 🧠
📉 VTI bajo → sugiere 𝙨𝙩𝙧𝙤𝙠𝙚 𝙫𝙤𝙡𝙪𝙢𝙚 𝙗𝙖𝙟𝙤
📈 VTI alto → puede sugerir 𝙖𝙡𝙩𝙤 𝙜𝙖𝙨𝙩𝙤 según contexto y FC
Pero lo más importante no es el número aislado… sino la 𝙩𝙚𝙣𝙙𝙚𝙣𝙘𝙞𝙖 🔄✨.
🔁💧 𝙇𝙤 𝙧𝙚𝙖𝙡𝙢𝙚𝙣𝙩𝙚 𝙥𝙤𝙩𝙚𝙣𝙩𝙚: 𝙫𝙚𝙧 𝙨𝙞 𝙧𝙚𝙨𝙥𝙤𝙣𝙙𝙚 𝙖𝙡 𝙩𝙧𝙖𝙩𝙖𝙢𝙞𝙚𝙣𝙩𝙤
El paper conecta el VTI con la reanimación real:
💧 𝙛𝙡𝙪𝙞𝙙 𝙧𝙚𝙨𝙥𝙤𝙣𝙨𝙞𝙫𝙚𝙣𝙚𝙨𝙨 ≈ aumento del stroke volume >15%
Como el VTI sigue al volumen sistólico, una 𝙨𝙪𝙗𝙞𝙙𝙖 𝙙𝙚𝙡 𝙑𝙏𝙄 tras fluidos, inotrópicos o liberar una obstrucción indica respuesta útil ✅
👉 O sea, no solo preguntas “¿qué tipo de shock es?” sino también “¿𝙡𝙤 𝙦𝙪𝙚 𝙚𝙨𝙩𝙤𝙮 𝙝𝙖𝙘𝙞𝙚𝙣𝙙𝙤 𝙚𝙨𝙩𝙖́ 𝙛𝙪𝙣𝙘𝙞𝙤𝙣𝙖𝙣𝙙𝙤?” 🎯.
🦵⚡ 𝙋𝙖𝙨𝙨𝙞𝙫𝙚 𝙡𝙚𝙜 𝙧𝙖𝙞𝙨𝙚 𝙑𝙏𝙄 = 𝙘𝙤𝙢𝙗𝙤 𝙗𝙚𝙙𝙨𝙞𝙙𝙚 𝙢𝙪𝙮 𝙥𝙤𝙩𝙚𝙣𝙩𝙚
Para el artículo, la maniobra práctica estrella para predecir respuesta a fluidos es el 𝙥𝙖𝙨𝙨𝙞𝙫𝙚 𝙡𝙚𝙜 𝙧𝙖𝙞𝙨𝙚 🦵
Si el 𝙑𝙏𝙄 𝙖𝙪𝙢𝙚𝙣𝙩𝙖 >𝟭𝟮%, eso sugiere 𝙧𝙚𝙨𝙚𝙧𝙫𝙖 𝙙𝙚 𝙥𝙧𝙚𝙘𝙖𝙧𝙜𝙖 y probable respuesta a volumen 💧📈
✅ reversible
✅ rápida
✅ sin “inundar” al paciente innecesariamente
👉 Muy útil justo donde más miedo da sobrecargar: shock séptico con SDRA, disfunción VI, etc.
🛠️🫁 𝙈𝙚𝙣𝙨𝙖𝙟𝙚 𝙛𝙞𝙣𝙖𝙡: 𝙍𝙐𝙎𝙃 𝙑𝙏𝙄 𝙘𝙤𝙣𝙫𝙞𝙚𝙧𝙩𝙚 𝙪𝙣 𝙥𝙧𝙤𝙩𝙤𝙘𝙤𝙡𝙤 𝙙𝙞𝙖𝙜𝙣𝙤́𝙨𝙩𝙞𝙘𝙤 𝙚𝙣 𝙪𝙣𝙤 𝙢𝙖́𝙨 𝙩𝙚𝙧𝙖𝙥𝙚́𝙪𝙩𝙞𝙘𝙤 🔥
La idea central del paper es elegante:
✅ usa 𝙍𝙐𝙎𝙃 para reconocer la fisiopatología del shock
✅ añade 𝙑𝙏𝙄 𝙗𝙖𝙨𝙖𝙡
✅ repítelo tras intervenciones
✅ si el 𝙑𝙏𝙄 𝙨𝙪𝙗𝙚 𝟭𝟱–𝟮𝟬%, la respuesta va por buen camino.
Además, si el LVOT no se puede medir bien, el artículo sugiere alternativas como:
🫀 𝙍𝙑𝙊𝙏-𝙑𝙏𝙄
🌊 𝙖𝙤𝙧𝙩𝙖 𝙙𝙚𝙨𝙘𝙚𝙣𝙙𝙚𝙣𝙩𝙚
👉 En resumen: 𝙍𝙐𝙎𝙃-𝙑𝙏𝙄 no solo te ayuda a encontrar el shock… te ayuda a 𝙧𝙚𝙖𝙣𝙞𝙢𝙖𝙧𝙡𝙤 𝙘𝙤𝙣 𝙢𝙖́𝙨 𝙥𝙧𝙚𝙘𝙞𝙨𝙞𝙤́𝙣.
‼️Si te sirve: ❤️ Me gusta | 🔁 Repost | ➕ Follow para más #MedED en #ClubCrit 😄🧠🫶
📚📖 Más en el blog #ClubCrit 👉 [buff.ly/hs2k39f]
#ClubCrit #RUSH #VTI #Shock #Ultrasound #POCUS #Shock #Echo #Hemodynamics #CardiacOutput #FluidResponsiveness #Resuscitation #PLR #CritCareMed #POCUS #VExUS #ICU #CriticalCare #CuidadoCrítico #MedTwitter #CritCare #Diagnóstico #icu #intensivecare #diagnosis #management #UCI #Tratamiento #MedicinaBasadaEnEvidencia #MedEd #Medicina #FOAMed #FOAMcc #MedX #IntensiveCare #EducaciónMédica #MedIntensiva #MedXCommunity #MedicinaCrítica #MedED #CritCare #ICUmanagement #MustRead #LecturaRecomendada

3
49
133
5,311

13 Dec 2025
CardiacOutput(CO)も後負荷になりうる
23 Feb 2025

すいません、言葉遊びでした。
後負荷は「心筋が打ち勝たなければならない抵抗」です。ASの場合、麻酔で血管が拡張しようが後負荷を決めるのはA弁になるので、「後負荷は変わらない」です。
むしろ血管が拡張して前負荷だけ減って後負荷が変わらずという最悪の状態が出来上がります。
4
22
8,247

11 Nov 2025
@TrackYourHeart Answer: C. Skeletal muscles. During intense exercise, ~80-85% of cardiac output shifts here via sympathetic vasoconstriction in visceral organs and local vasodilation, meeting oxygen demand while brain flow stays constant. #ExercisePhysiology #CardiacOutput
3
1,063

11 Nov 2025
C. Skeletal muscles
🤹During intense exercise, blood flow is redistributed to meet the high oxygen and nutrient demands of active tissues.
🤹Cardiac Output Distribution:
•🌀Skeletal muscles: ~80–85% of total cardiac output
•🌀Skin: increases moderately (for heat dissipation)
•🌀Brain: remains relatively constant
•🌀Kidneys & digestive organs (liver, GI tract): markedly reduced
🤹Mechanism:
•🌀Sympathetic activation → vasoconstriction in visceral organs
•🌀Local metabolic vasodilation → increased flow to active muscles
🤹Summary:
During intense exercise, the majority of cardiac output is directed to skeletal muscles to support increased metabolic activity.
#ExercisePhysiology #CardiacOutput #KriMeeraPharma
1
1
16
2,238

27 Jun 2025
1/
Most people think the heart drives circulation.
But what if that’s backwards?
Anderson’s model flips the whole idea of cardiac output on its head — and it changes how you think about fluid, flow, and failure.
🧵👇
#physiology #FOAMed #MedTwitter #criticalCare #cardiacOutput
10
118
319
89,427

7 May 2025
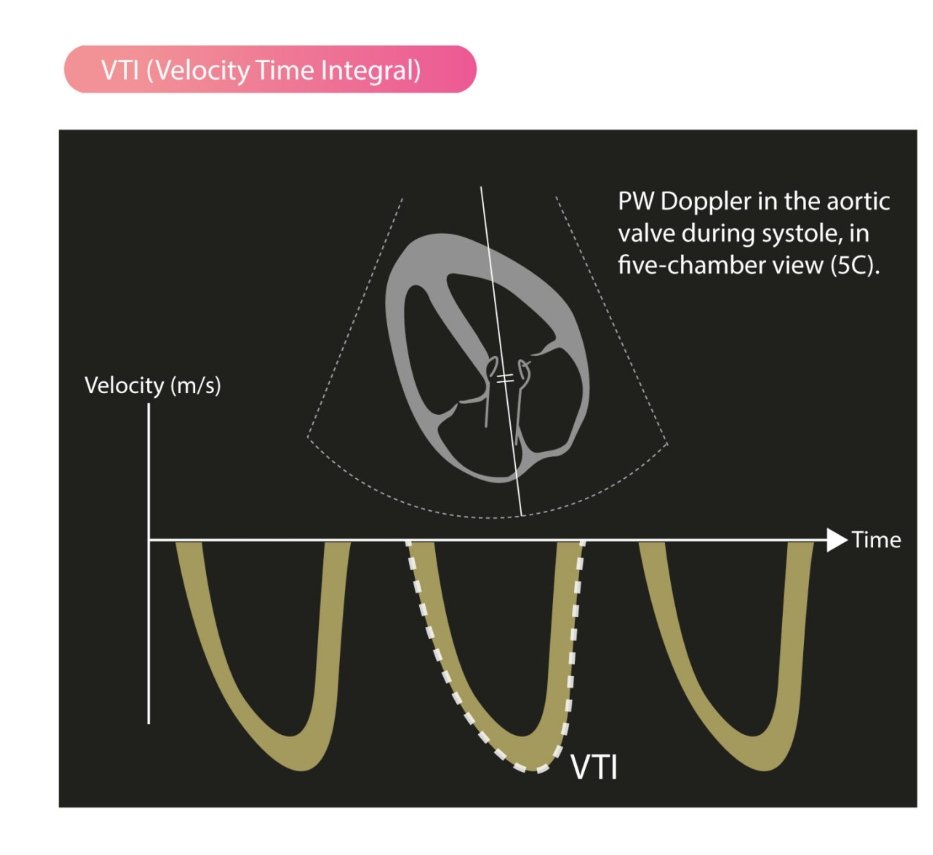
What is VTI (Velocity Time Integral) in echocardiography?
VTI measures the distance a column of blood travels during systole through the LVOT. It’s a vital parameter to estimate stroke volume and cardiac output noninvasively.
How is VTI measured?
1️⃣ Obtain an apical 5-chamber view (5C).
2️⃣ Place PW Doppler just below the aortic valve (at LVOT).
3️⃣ Measure the area under the velocity curve during systole➡️ that’s the VTI (in cm).
Calculation of Stroke Volume (SV):
SV = VTI × LVOT area
LVOT area = π × (LVOT diameter/2)²
Requires accurate LVOT diameter from parasternal long-axis view.
Then,
Cardiac Output (CO) = SV × HR
♦️Normal LVOT VTI: ~18–22 cm (adults)
▶️A low VTI often means reduced stroke volume, requiring further hemodynamic assessment.
#Echo #Cardiology #VTI #StrokeVolume #CardiacOutput #POCUS
2
68
221
11,074

6 May 2025
Today’s Daily Dose ☕️: Critical Care 🥼🩺
Continuous Cardiac Output or Serial Echocardiography in Septic Shock?
Let’s rethink the monitor-vs-ultrasound debate for the resuscitating intensivist.
Septic shock is a complex beast—characterized by dynamic interactions between vascular tone, myocardial function, and tissue oxygenation. When managing these patients, how we monitor cardiac output (CO) matters—immensely.
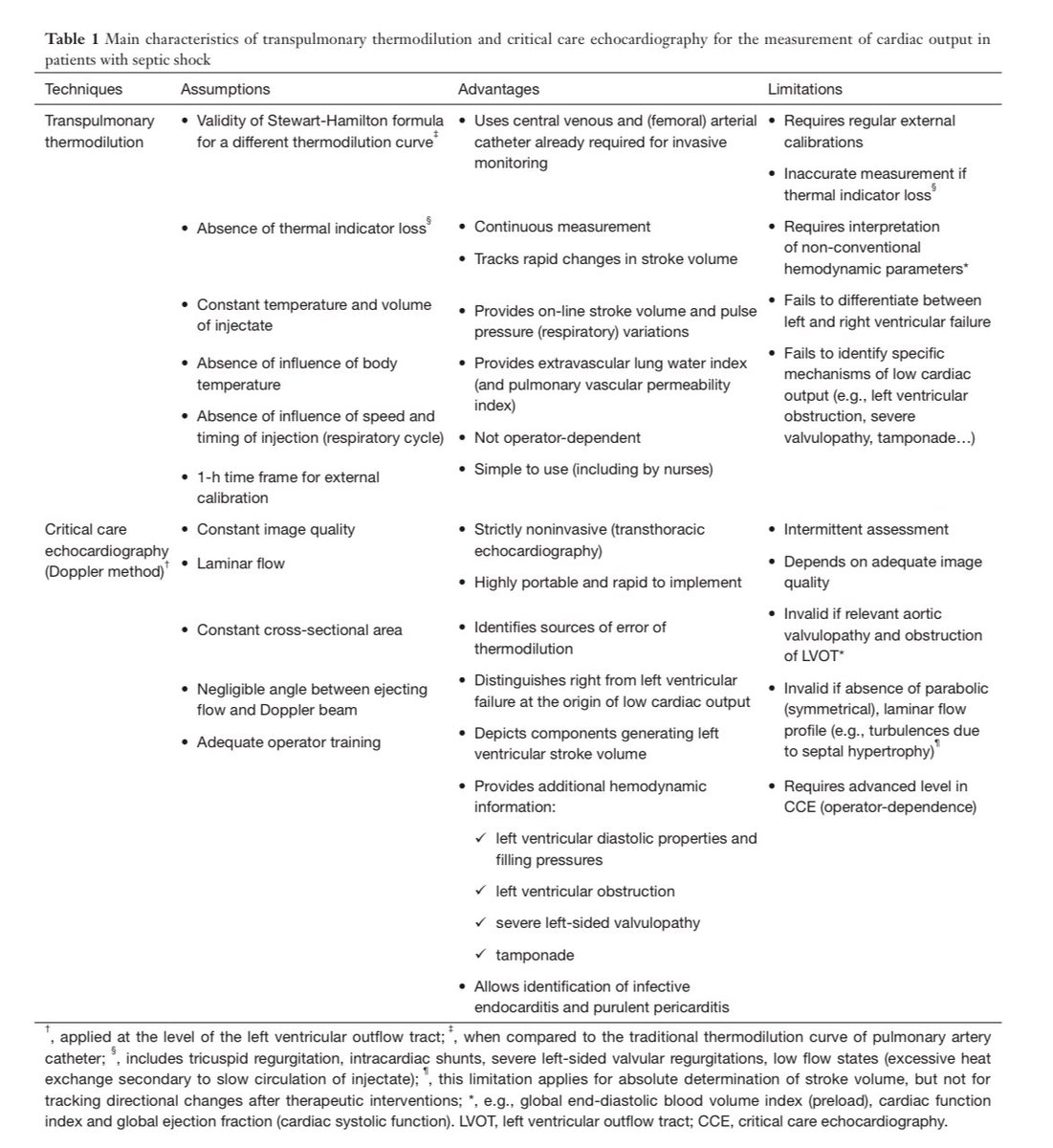
This recent review by Philippe Vignon in Annals of Translational Medicine lays out a detailed comparison of two key techniques:
⸻
1. Transpulmonary Thermodilution (TPT) 🖥️🧪
✅ Offers continuous, real-time CO monitoring
✅ Valuable during dynamic maneuvers (passive leg raise, end-expiratory occlusion)
✅ Useful for early detection of unexpected hemodynamic deterioration
⚠️ But: Accuracy falters in the presence of RV failure, severe TR, low flow states, or thermal indicator loss
⚠️ Requires external calibration every hour to remain trustworthy
⚠️ Does not reveal mechanisms behind low output—just trends
⸻
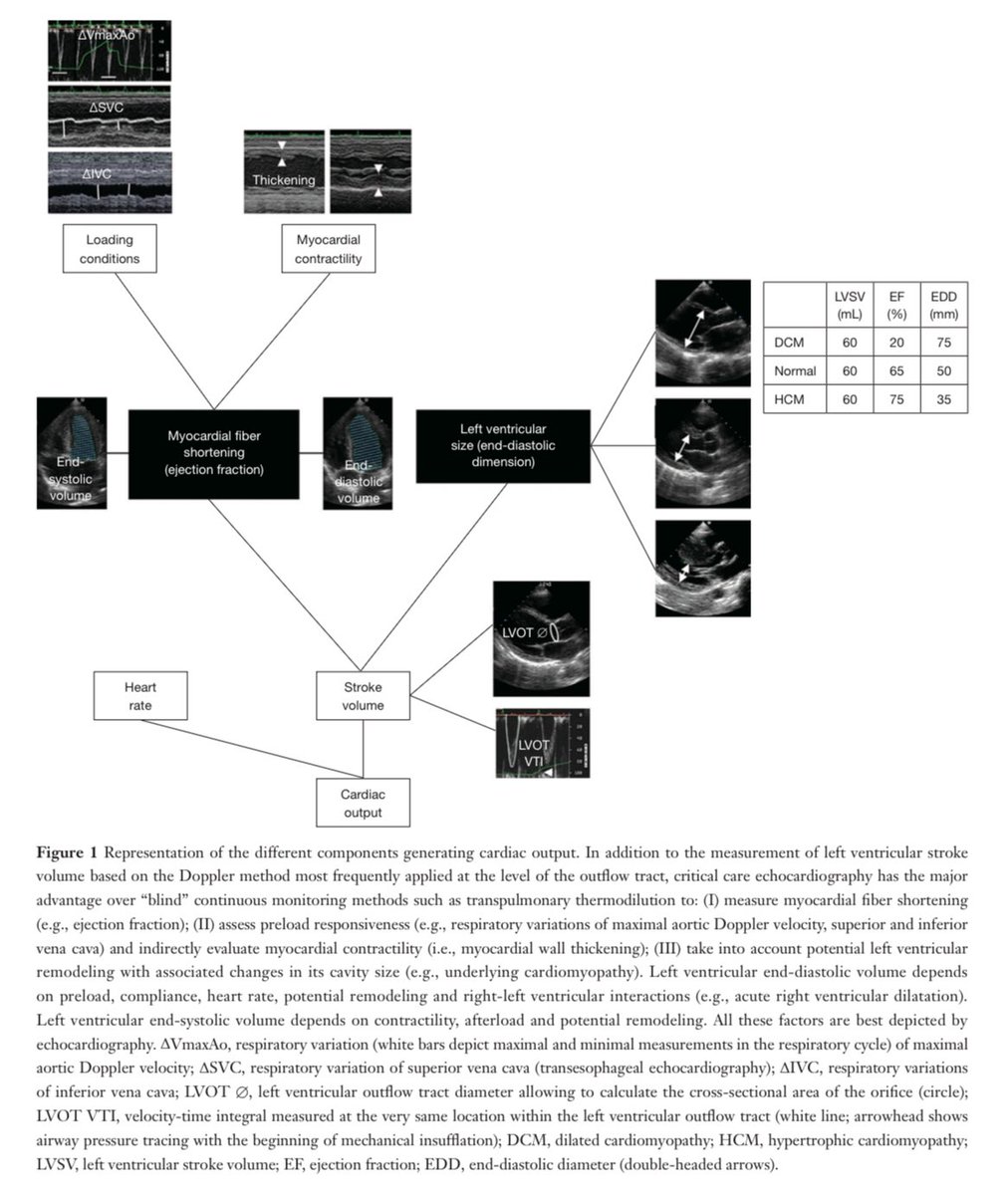
2. Critical Care Echocardiography (CCE) 📸🫀
✅ First-line for evaluating the type of shock, especially early in resuscitation
✅ Depicts stroke volume mechanics, ventricular function, filling pressures, and pulmonary pressures
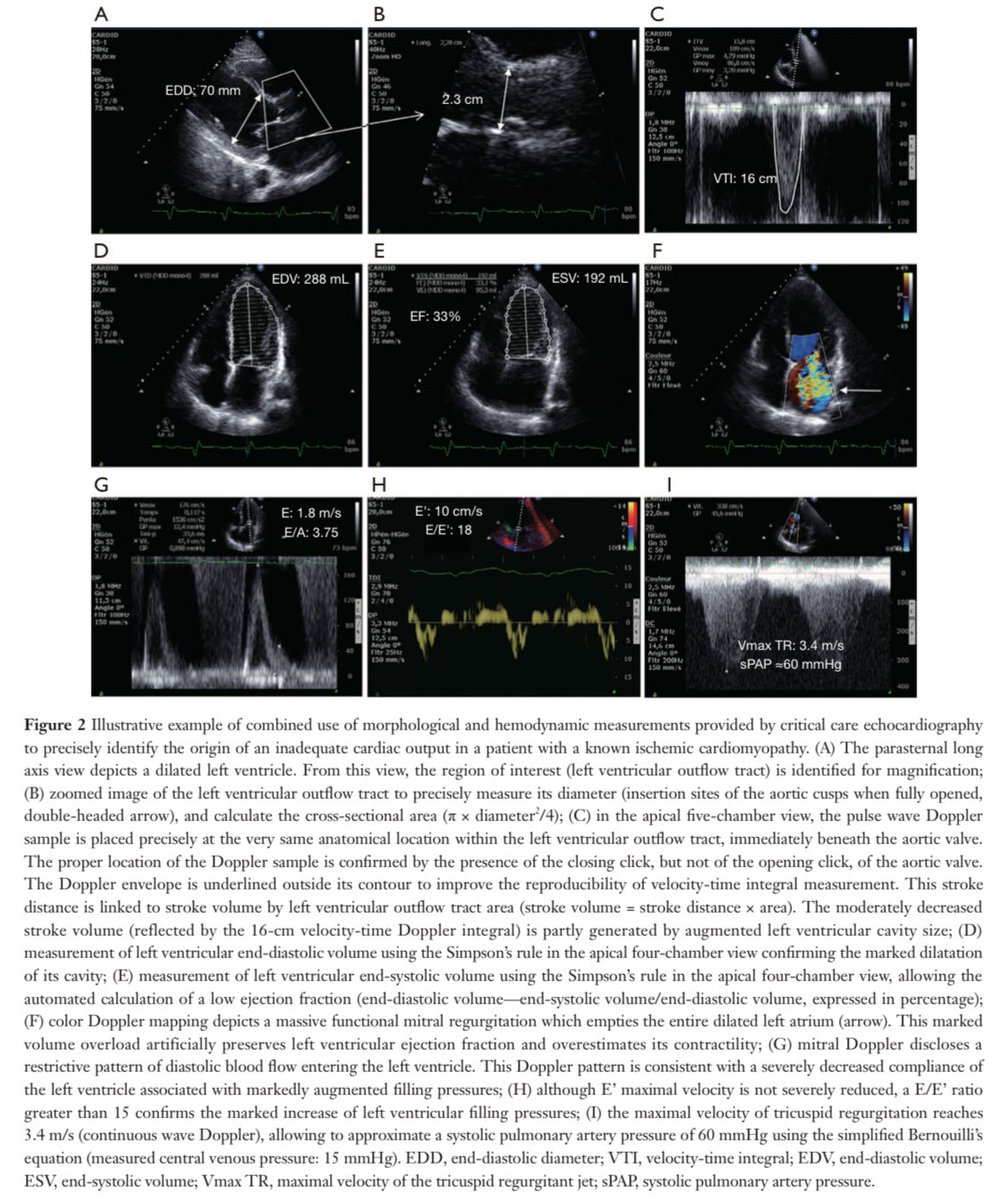
✅ Identifies causes of low CO missed by TPT: LVOT obstruction, mitral/aortic regurg, tamponade, cor pulmonale
✅ Allows therapy matching: fluids vs inotropes vs afterload control
⚠️ Limitation? Not continuous—but easily repeated, even daily
⸻
So, which one to use? The answer: BOTH.
These are complementary tools, not competitors.
Use CCE first to understand the phenotype.
Use TPT next to follow trends, provided it’s calibrated and interpreted wisely.
CCE helps avoid therapeutic mistakes:
❌ Starting dobutamine in dynamic LVOT obstruction
❌ Giving fluids in RV failure
❌ Over-relying on CO changes without context
⸻
Monitoring ≠ Management Unless Actionable
Just watching numbers doesn’t save lives—acting on the right information does. This means:
✔️ Avoid targeting supranormal DO2 or CO
✔️ Use inotropes only with evidence of pump failure tissue hypoperfusion
✔️ Reassess hemodynamics daily—phenotypes change!
⸻
What’s next? 🔭
The future includes miniaturized TEE probes, AI-guided ultrasound, and hopefully, real-time microcirculatory monitoring.
But even now, we can do better—by combining tools intelligently.
⸻
Bottom line?
👉 Use CCE to diagnose and guide
👉 Use TPT to trend and confirm
💡 Don’t just monitor—understand, personalize, and adapt.
References 📚
Vignon P. Continuous cardiac output assessment or serial echocardiography during septic shock resuscitation? Ann Transl Med. 2020;8(12):797. doi:10.21037/atm.2020.04.11
#CriticalCare #Echocardiography #Sepsis #ICU #Hemodynamics #TPT #CardiacOutput #Pocus #UltrasoundFirst #IntensiveCare #ShockManagement #Resuscitation #FluidResponsiveness
2
18
60
4,311

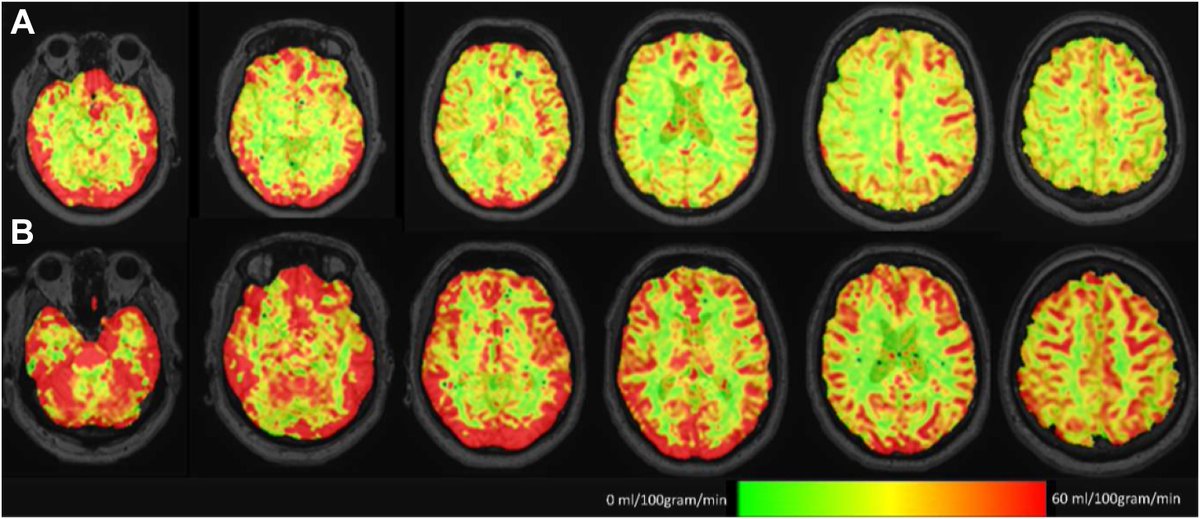
Cerebral blood flow and cognitive functioning in patients undergoing transcatheter aortic valve implantation
In patients with severe symptomatic aortic valve stenosis undergoing TAVI, #cardiacoutput, CBF, and #cognitivefunctioning improved after 3 months
thelancet.com/journals/eclin…
2
7
1,590



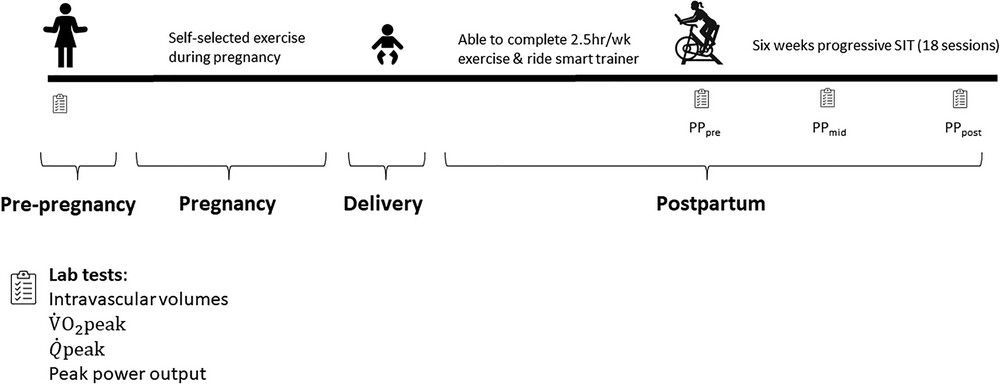
🎉 Exciting research alert! This #CaseReport explores how postpartum exercise could sustain the impressive #cardiacoutput seen during pregnancy. Congratulations to @Nrmnd_Rchrd, @mskoehle, and @exercise4heart for their important work! 🌟 Check it out! 📜 buff.ly/3UjWD9e
24 Oct 2024

In this #CaseReport article, @Nrmnd_Rchrd, @VClaydonLab, @mskoehle and @exercise4heart (@SFU) examine whether the enhanced #cardiacoutput of pregnancy could be maintained with strenuous #exercise training undertaken early #postpartum.
📜buff.ly/3UjWD9e
2
8
1,267

24 Oct 2024
In this #CaseReport article, @Nrmnd_Rchrd, @VClaydonLab, @mskoehle and @exercise4heart (@SFU) examine whether the enhanced #cardiacoutput of pregnancy could be maintained with strenuous #exercise training undertaken early #postpartum.
📜buff.ly/3UjWD9e
3
8
2,635
18 Sep 2024
Correlation between corrected carotid flow time and left ventricular outflow tract velocity‐time integral using a novel technique
Journal of Clinical Ultrasound
doi.org/10.1002/jcu.23838
Shareable link: onlinelibrary.wiley.com/shar…
#POCUS #cardiacoutput
2
12
38
4,236

11 Aug 2024
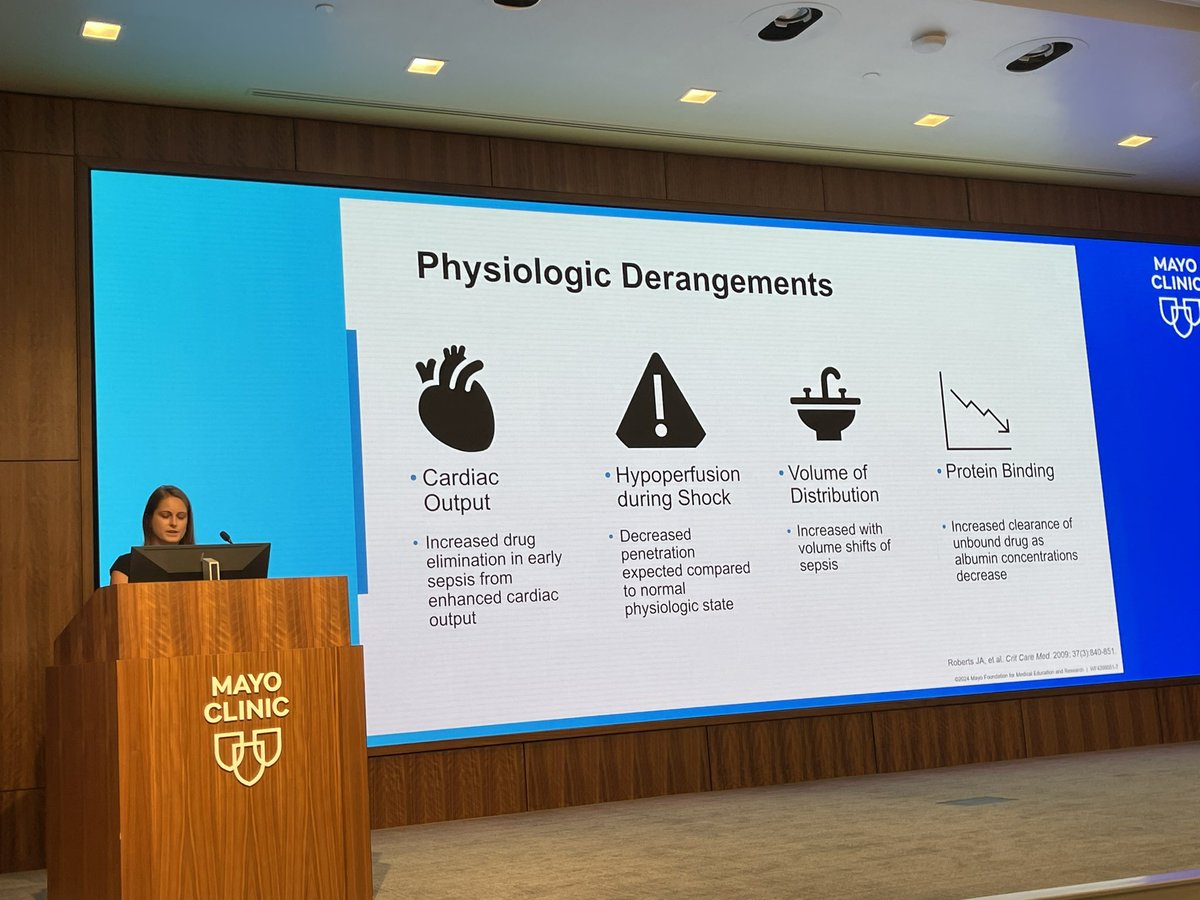
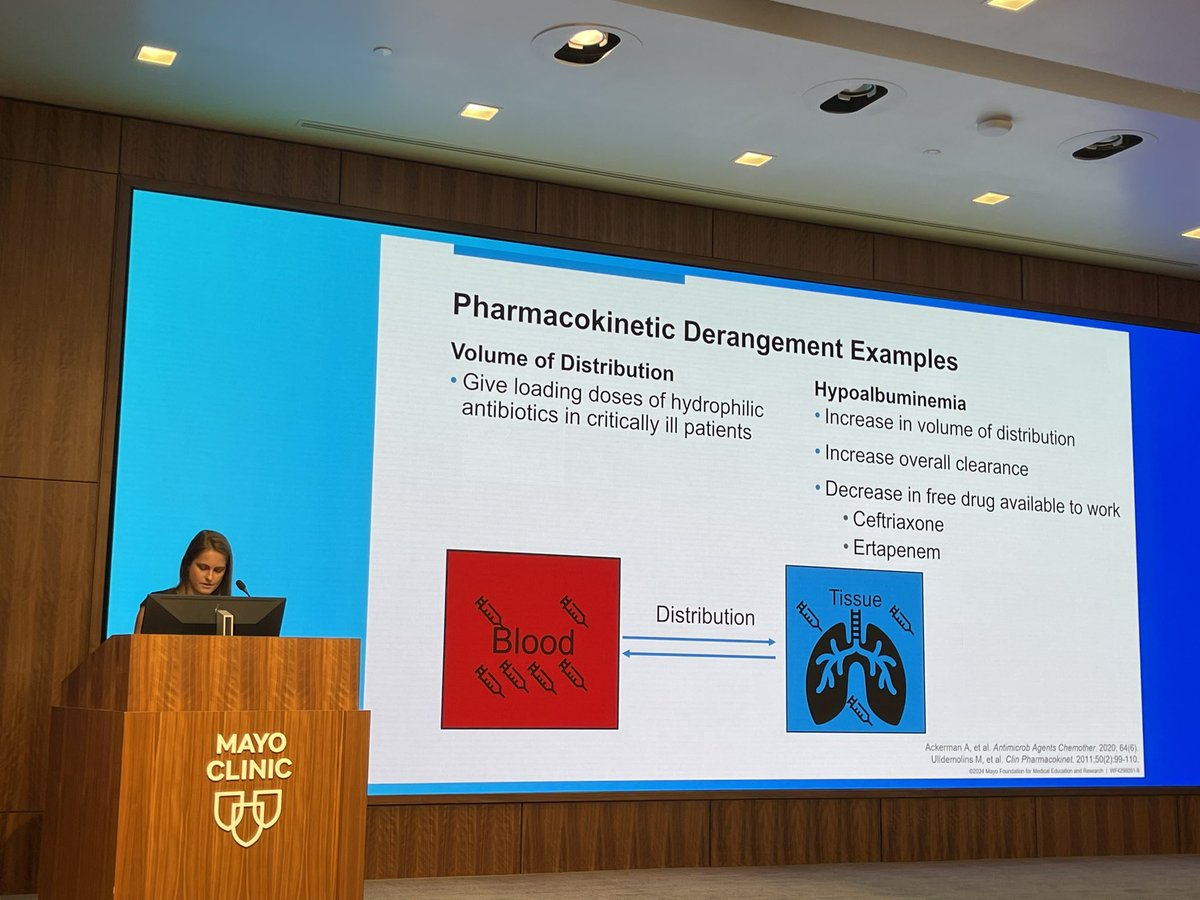
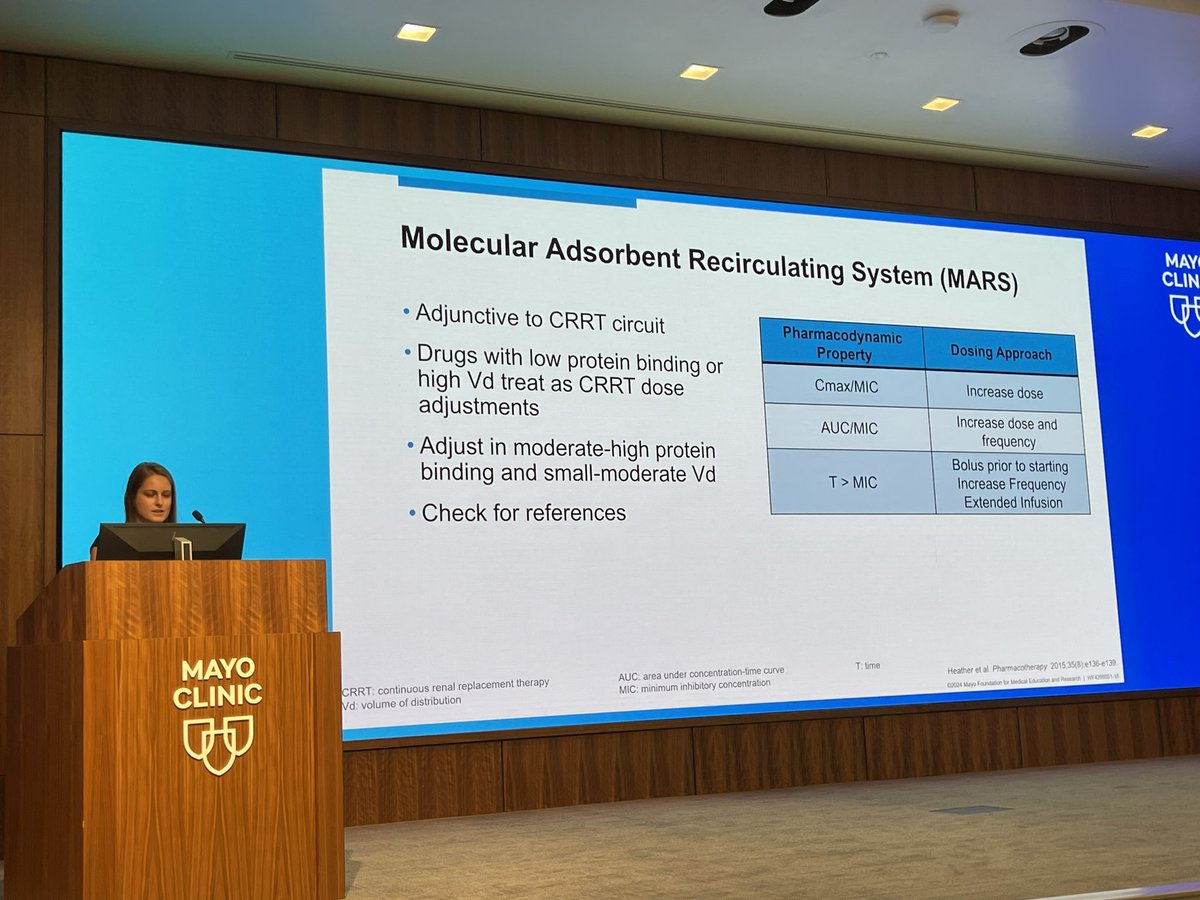
@hbrinkman23 Brinkman in depth assessment of pharmacist role in ICU and med management/dosing recs accounting for #cardiacoutput #VD and #Protein binding. SO MANY good insights for @pkguru10 @Dev_Sanghavi and our audience #MayoClinicInnovativeHorizons
2
121

5 Aug 2024
measurements of HR, BP, CBF, and CO. In 46 (9%) patients CO and CBF changes were in the normal range of HC, and in 488 (91%) an abnormal CO and CBF reduction was found. #MECFS #pwME #CBF #CardiacOutput
5
119
31 Jul 2024
Cardiac output monitoring in critical care : Technology and Choice
#cardiacoutput #hemodynamics
Accurate CO monitoring is essential for optimizing hemodynamics, ensuring adequate organ perfusion, and improving outcomes in critically ill and high-risk surgical patients.
🌟 Key Insights:
1.🔍 Importance of Cardiac Output Monitoring:
•Hemodynamic Optimization: Cardiac output is a vital indicator of cardiovascular function. Accurate monitoring helps guide fluid therapy and inotropic support, crucial for optimizing oxygen delivery to tissues and organs.
•Perioperative Management: In surgical settings, particularly for high-risk patients, CO monitoring is integral to goal-directed therapy (GDT), improving outcomes by optimizing hemodynamic parameters.
2.⚙️ Methods of Cardiac Output Monitoring:
•🩸 Pulmonary Artery Catheter (PAC) - Thermodilution:
•🌟 Advantages: Gold standard for CO measurement; provides direct and accurate readings.
•⚠️ Limitations: Highly invasive; associated with potential complications such as infection, arrhythmias, and pulmonary artery rupture.
•📌 Best for: Situations where precise hemodynamic data is critical, such as in complex cardiac surgeries or severely unstable patients.
•💧 Transpulmonary Thermodilution (PiCCO System):
•🌟 Advantages: Comprehensive hemodynamic profile, including extravascular lung water and global end-diastolic volume, with less invasiveness than PAC.
•⚠️ Limitations: Requires central venous and arterial access; prone to errors due to indicator recirculation.
•📌 Best for: Critically ill patients needing detailed hemodynamic monitoring but where reduced invasiveness is desired.
•📏 Fick Principle:
•🌟 Advantages: Highly accurate when applied correctly; based on fundamental physiological principles.
•⚠️ Limitations: Impractical for continuous monitoring; requires accurate measurement of oxygen consumption, which can be challenging.
•📌 Best for: Situations where non-continuous CO measurement is acceptable and high accuracy is needed, often used as a reference method in controlled settings.
•📊 Arterial Waveform Analysis (FloTrac/Vigileo System):
•🌟 Advantages: Continuous, real-time monitoring with minimal invasiveness; requires only an arterial line.
•⚠️ Limitations: Accuracy can be affected by changes in vascular tone and arrhythmias; less reliable in conditions of hemodynamic instability.
•📌 Best for: Patients needing continuous CO monitoring with minimal invasiveness, especially in stable hemodynamic conditions.
•🌈 Pulse Dye Densitometry and Lithium Dilution (LiDCO System):
•🌟 Advantages: Provides real-time CO measurements; minimal invasiveness with good correlation to PAC measurements.
•⚠️ Limitations: Specific limitations include potential cross-reactions with drugs (PDD) or contraindications in patients on lithium therapy (LiDCO).
•📌 Best for: Real-time CO monitoring in settings where reduced invasiveness is prioritized, but accuracy remains important.
•💡 Transthoracic Impedance and Bioreactance Analysis:
•🌟 Advantages: Non-invasive; suitable for continuous monitoring. Utilizes changes in thoracic electrical impedance to estimate CO.
•⚠️ Limitations: Accuracy can be influenced by patient movement, lung water content, and electrode placement.
•📌 Best for: Non-invasive, continuous CO monitoring, especially in settings where patient comfort and minimal risk are priorities.
•🛠️ The Doppler Principle:
•🌟 Advantages: Non-invasive or minimally invasive (depending on approach); provides continuous or intermittent measurements of blood flow velocity to estimate CO.
•⚠️ Limitations: Operator-dependent accuracy; requires precise probe positioning and may be less reliable in unstable or arrhythmic patients.
•📌 Best for: Patients requiring less invasive monitoring with a need for real-time data, particularly in perioperative or intensive care settings.
2
1
5
920