
Jun 13
A new Circulation paper identifies RND3 as a mitochondrial metabolic switch that protects the heart from ischemia–reperfusion injury.
The key mechanism is elegant:
RND3 → ACAT1 inhibition → ↓ PDHA1 K321 acetylation → ↑ PDH activity → ↑ glucose oxidation → cardioprotection
Why this matters:
During ischemia–reperfusion, the heart faces an acute energy crisis. Glucose oxidation is more oxygen-efficient than fatty acid oxidation, so restoring pyruvate entry into the TCA cycle can be cardioprotective.
Xiong et al. show that cardiomyocyte-specific Rnd3 deletion causes:
• impaired cardiac glucose oxidation
• compensatory increase in fatty acid oxidation
• uncoupling of glycolysis from the TCA cycle
• reduced pyruvate/malate-driven complex I respiration
• decreased PDH activity
• reduced phosphocreatine/ATP energy reserve
• progressive cardiac dysfunction and lethality
Mechanistically, RND3 is not only cytosolic.
The authors identify RND3 as a mitochondrial matrix–resident small GTPase, imported through an internal amphipathic motif.
Inside mitochondria, RND3 directly binds ACAT1, disrupting the ACAT1–PDHA1 interaction.
Without RND3, ACAT1 binds PDHA1 more strongly and drives PDHA1 K321 acetylation, suppressing PDH activity and limiting glucose-derived carbon entry into the TCA cycle.
The disease relevance is strong:
RND3 expression falls in both human and mouse hearts after ischemia–reperfusion injury.
Loss of RND3 worsens I/R injury: larger infarct size, more apoptosis, lower LVEF/LVFS, higher LDH, lower ATP and phosphocreatine.
Conversely, cardiac-specific Rnd3 overexpression protects against I/R injury—but this protection is blunted when Pdha1 is knocked down.
So the protective effect depends on PDHA1.
This paper reframes RND3 as more than a Rho/ROCK cytoskeletal regulator.
It is a mitochondrial gatekeeper of cardiac substrate metabolism.
Therapeutic implication:
Restoring the RND3–ACAT1–PDHA1 axis may help shift the injured heart toward oxygen-efficient glucose oxidation and reduce reperfusion damage.
Reference:
Xiong et al. “RND3 Enhances Cardiac Glucose Metabolism Through Inhibiting ACAT1-Dependent PDHA1 Acetylation and Protects Against Ischemia-Reperfusion Injury.” Circulation 2026. DOI: 10.1161/CIRCULATIONAHA.125.075591.

1
77

The good news: research suggests women may get more cardioprotection per minute of movement than men, and we need both aerobic AND resistance training.
This was Dr. Gulati's own JACC 2024 study of 400,000 adults.
1
6
215

Jun 10
3/5
SS-31 (Elamipretide): Tetrapeptide investigated for cardiolipin binding and mitochondrial membrane stabilization—examined in cardioprotection and oxidative stress models for ATP efficiency and ROS reduction.

1
13

This week's #WNW features the first guideline that discusses cardioprotection management in CKM syndrome. Click below to check out the 2026 AHA/ACC/ADA/ASN Guideline for Cardiovascular-Kidney-Metabolic Syndrome!
bit.ly/4vvaJ7C
1
260

How do we better protect the hearts of cancer patients?
A new special focus in @ECRJournal, guest edited by Dr Massimiliano Camilli, covers anticoagulation, revascularisation, cardioprotection and emerging toxicities in cardio-oncology.
Explore the Collection | Submit to ECR Journal | radc.life/4LVtFym6
#CardioOncology #Cardiology #CardioEd #Oncology

2
152

Jun 9
Shared Strengths — Both Compounds Deliver
Both SLU-PP-332 and SLU-PP-915 are potent pan-ERR agonists with clean selectivity (no meaningful activity at classical estrogen receptors). They upregulate key metabolic genes (PGC-1α, PDK4, LDHA, DDIT4 and others) in muscle and heart tissue, shift metabolism toward oxidative/aerobic pathways, and produce clear “exercise-like” phenotypes in mouse models.
Exercise capacity & enduranceBoth enhance treadmill running distance and duration in exhaustion protocols. They strongly induce DDIT4 (a gene ramped up by real aerobic exercise) in skeletal muscle, often to levels that match or exceed what actual treadmill training produces. They support mitochondrial function and fatty acid oxidation programs that translate to better endurance and metabolic efficiency.
Cardioprotection in heart failure modelsIn the transaortic constriction (TAC) pressure-overload heart failure model, both compounds improve ejection fraction, reduce cardiac fibrosis, and support survival. They normalize perturbed cardiac metabolomes (fatty acids/lipids and TCA/OXPHOS metabolites) and improve mitochondrial ultrastructure and respiratory capacity without blunting adaptive hypertrophy. The net result: the heart gets the metabolic support it needs to handle increased workload. Effects are largely driven through ERRγ in cardiomyocytes, with strong autophagy induction as well.
Metabolic & muscle benefitsBoth boost energy expenditure and fat oxidation programs. They hold promise for metabolic health applications (obesity, insulin sensitivity, metabolic liver conditions) and muscle adaptation/sarcopenia contexts by mimicking the cellular benefits of training. In cell models they increase TFEB (autophagy/lysosomal regulator) and drive oxidative gene expression.
In short: both are legitimate high-performance research tools with overlapping, high-quality data packages across endurance, cardiac protection, and metabolic optimization.
1
3
253

Jun 9
This isn’t true
We have data cuts that show weight independent benefits
MACE reduction consistent across all baseline weight and waist circumference categories
weight loss at week 20 did not show a linear trend with subsequent MACE risk, while waist reduction explained only part of the benefit.
~33% of the observed MACE benefit was mediated through waist circumference reduction, and concluded the cardioprotection was independent of baseline adiposity and weight loss, implying mechanisms beyond adiposity reduction.
utsouthwestern.elsevierpure.…
also more studies show that hsCRP falls before weight loss is observed which means inflammation falls first (which is actually how you get heart and neuroprotective benefits)
Jun 9

Nearly all the medical miracles attributed to GLP-1s would likely be similar to simply just losing weight.
3
1,174

Jun 9
ADA 2026 Day 2 — 20 Best CME India Pearls
1️⃣ Obesity is now firmly positioned as a chronic disease, not merely a BMI number. ADA 2026 emphasizes screening, staging, complications, psychosocial context, social determinants, and long-term individualized therapy.
2️⃣ For Indian/Asian patients, BMI alone is not enough. Lower ethnicity-specific BMI cut-offs should be combined with waist circumference or waist-to-height ratio for better obesity-risk identification.
3️⃣ The 6A framework is practical for OPD obesity care: Ask permission, Assess risk, Advise, Agree on goals, Assist with plan, and Arrange follow-up.
4️⃣ GLP-1 RA and dual GIP/GLP-1 RA are now central obesity therapies in patients with cardiometabolic comorbidities because they address weight, glycemia, BP, lipids, and CV risk factors together.
5️⃣ Weight-loss targets should be complication-driven. A 5% weight loss is clinically meaningful, but 10–15% or more may be needed for T2D, MASH, HFpEF, OSA, and osteoarthritis improvement.
6️⃣ Dapagliflozin evidence in HFmrEF/HFpEF looks strong even in real-world emulation. In matched adults with HFmrEF/HFpEF and T2D, dapagliflozin showed a 24% lower rate of all-cause mortality or HF hospitalization versus sitagliptin.
7️⃣ Real-world data can complement RCTs when designed rigorously. The DELIVER trial emulation reproduced directionally consistent results, supporting fit-for-use observational data in HF–diabetes decision-making.
8️⃣ Beware of overdiagnosing prediabetes using conventional GMI. HbA1c–GMI discordance was common at lower glucose ranges; updated GMI aligned better with HbA1c and time above 140 mg/dL.
9️⃣ CGM-derived prediabetes labels need caution. In normoglycemia, only 19% had conventional GMI below 5.7%, whereas 63% had updated GMI below 5.7%, showing conventional GMI may inflate prediabetes classification.
🔟 Ramadan fasting: regimen simplicity matters. In insulin/SU-treated T2D, basal insulin alone or SU alone performed better than MDI or basal insulin plus SU for CGM targets during Ramadan.
1️⃣1️⃣ MDI during Ramadan carried the poorest CGM profile. Time in range was lowest and glycemia risk index highest in the MDI group, with more diabetes-related ER visits than simpler regimens.
1️⃣2️⃣ Metformin may have a cognition signal beyond glycemia. In DPPOS, long-term metformin exposure was associated with 59–62% lower odds of dementia versus placebo and about 60% lower odds versus intensive lifestyle intervention.
1️⃣3️⃣ Do not overstate the metformin–dementia finding yet. The signal is promising, but the study itself notes that longer follow-up and more dementia cases are needed for confirmation.
1️⃣4️⃣ Time in Range is becoming a CKM-risk marker. In older adults with T2D, lower TIR was independently and linearly associated with advanced cardiovascular–kidney–metabolic syndrome.
1️⃣5️⃣ For older T2D with CKM risk, TIR >70% may be a better target than 50%. Even TIR 50–70% carried elevated odds of advanced CKM syndrome compared with >70%.
1️⃣6️⃣ SGLT2 inhibitor persistence matters. Longer therapy duration was associated with progressively lower MACE and HF hospitalization risk over 5 years.
1️⃣7️⃣ The cardioprotection curve strengthens with time on SGLT2i. Compared with <1 year, ≥3 years of SGLT2i use showed lower MACE risk and lower HF hospitalization risk.
1️⃣8️⃣ Stopping SGLT2i unnecessarily may lose long-term CV–renal benefit. ADA Day 2 reinforces persistence, adherence, and affordability planning as part of evidence-based cardiometabolic care.
1️⃣9️⃣ AI prediction for T2D is moving toward real-world prevention. An EHR-based model in more than 3 million adults achieved excellent 1-year discrimination, with AUC around 0.88.
2️⃣0️⃣ The future OPD diabetes model is prevention plus precision. CGM metrics, CKM staging, AI prediction, SGLT2i persistence, incretin-based obesity care, and distress screening are converging into a more holistic diabetes clinic.
1
7
409


Jun 8
Cardioprotection of Atractylodes lancea against Hypoxia/ Reoxygenation-Injured H9c2 Cardiomyoblasts eurekamag.com/research/053/0…
5

5️⃣ Matthieu Josse – Biphasic cardioprotection by pre-dialysis exercise in HD patients
#ERA26 #Hemodialysis #CardioNephrology #Exercise
➡️ Key messages:
🔹 HD induces transient myocardial dysfunction (“myocardial stunning”), characterized by regional wall motion abnormalities (RWMA) and worsening global longitudinal strain (GLS).
🔹 Acute exercise performed immediately before dialysis may protect the myocardium against this dialysis-induced injury.
🔹 The proposed mechanism is ischemic preconditioning, whereby a brief exercise stimulus triggers protective pathways that persist beyond the exercise session itself.
📊 Study design:
🔹 Randomized crossover study
🔹 27 maintenance hemodialysis patients
🔹 Exercise performed 30 minutes before dialysis
🔹 Cardiac function assessed using:
▪️ Regional wall motion abnormalities (RWMA)
▪️ Global longitudinal strain (GLS)
🔹 Effects evaluated during:
▪️ First window of protection (FWOP)
▪️ Second window of protection (SWOP)
📊 Key findings:
Compared with control sessions, pre-dialysis exercise resulted in:
✅ Fewer regional wall motion abnormalities
🔹 FWOP: significant reduction (p<0.001)
🔹 SWOP: significant reduction (p=0.02)
✅ Better preservation of myocardial function
🔹 GLS improved by ~1.5% in both protection windows (p<0.001)
Importantly:
🔹 No significant differences in UF volume, UF rate or dialysis duration
🔹 No meaningful differences in blood pressure, cardiac output or blood volume changes
This suggests the cardioprotective effect was not explained by hemodynamic changes.
💡 Take-home messages:
🔹 A brief session of exercise before dialysis reduced dialysis-induced myocardial dysfunction, with benefits observed not only during the immediate dialysis session but also during the subsequent treatment.
🔹 These findings support the hypothesis that exercise-induced preconditioning may offer a simple, low-cost and non-pharmacological strategy to reduce cardiac injury in hemodialysis patients.
1
3
5
301
🧵 Free Communications 18: Bones, Hearts & Metabolism: Dialysis Complications Unpacked #ERA26
Chaired by Jovana Kusic Milicevic and Pieter Evenepoel.
Today’s session explores key complications in hemodialysis:
🩸 Bleeding risk and anticoagulation
🦴 Osteoporosis and fractures
❤️ Cardiovascular risk prediction
🏃 Exercise-based cardioprotection
Follow this thread for the key findings 👇
1
4
6
392

Jun 2
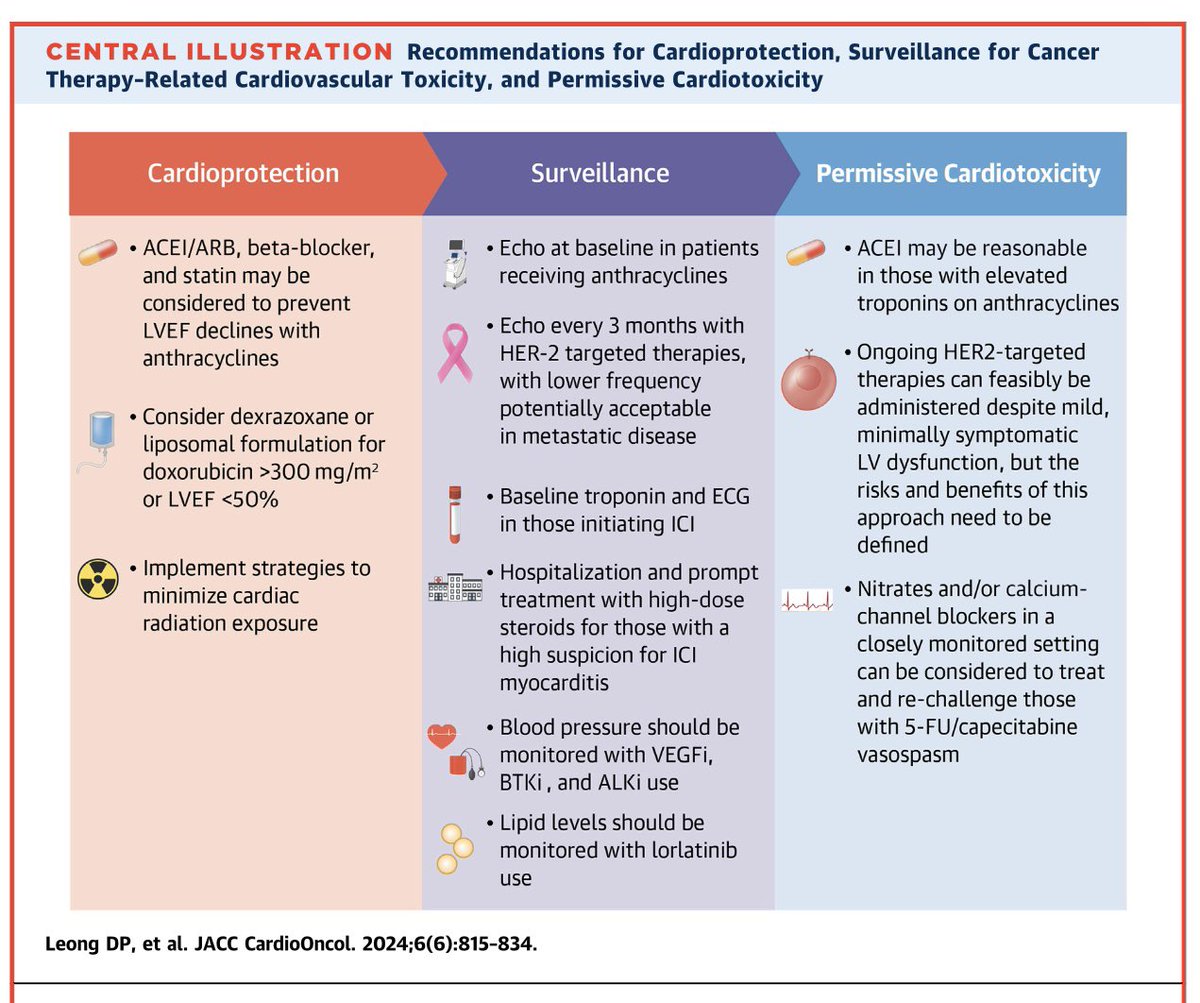
Cardiovascular considerations DURING cancer therapy🫀
The second of a 3 part #JACCCardioOnc Expert Panel series exploring cardiovascular care before, during, & after cancer therapy.
Recommendations for #CardioOncology care during cancer treatment:
Cardioprotection🛡️:
📍ACEI/ARB, beta-blockers, & statins may be considered to prevent ⬇️LVEF with anthracyclines
📍Consider dexrazoxane or liposomal doxorubicin for high cumulative anthracycline dose or LVEF <50%
📍Implement strategies to minimize cardiac radiation exposure
Surveillance🖥️:
📍Echo for anthracyclines & HER2-targeted therapies
📍Troponin & ECG for patients receiving ICIs
📍Prompt treatment & evaluation for high suspicion of ICI myocarditis
📍Blood pressure monitoring for VEGFi, BTKi, & ALKi therapies
📍Lipid monitoring for lorlatinib
Permissive cardiotoxicity⚖️:
📍Continue HER2-targeted therapy in selected patients with mild LV dysfunction, but need to evaluate risk & benefits
📍ACEi may be reasonable in patients with ⬆️ troponin during anthracycline therapy
📍Nitrates and/or calcium channel blockers can be considered to treat & rechallenge selected patients with 5-FU/capecitabine vasospasm, with close monitoring
Read more in @JACCJournals:
jacc.org/doi/10.1016/j.jacca…

43
90
4,399

Proven fish health benefits:
✅anti-oxidation
✅anti-inflammation
✅wound healing
✅neuroprotection
✅cardioprotection
✅hepatoprotection
✅immunoglobin defense agents against viral/bacterial infection
✅protein-calorie malnutrition prevention
sciencedirect.com/science/ar…
3
15

May 26
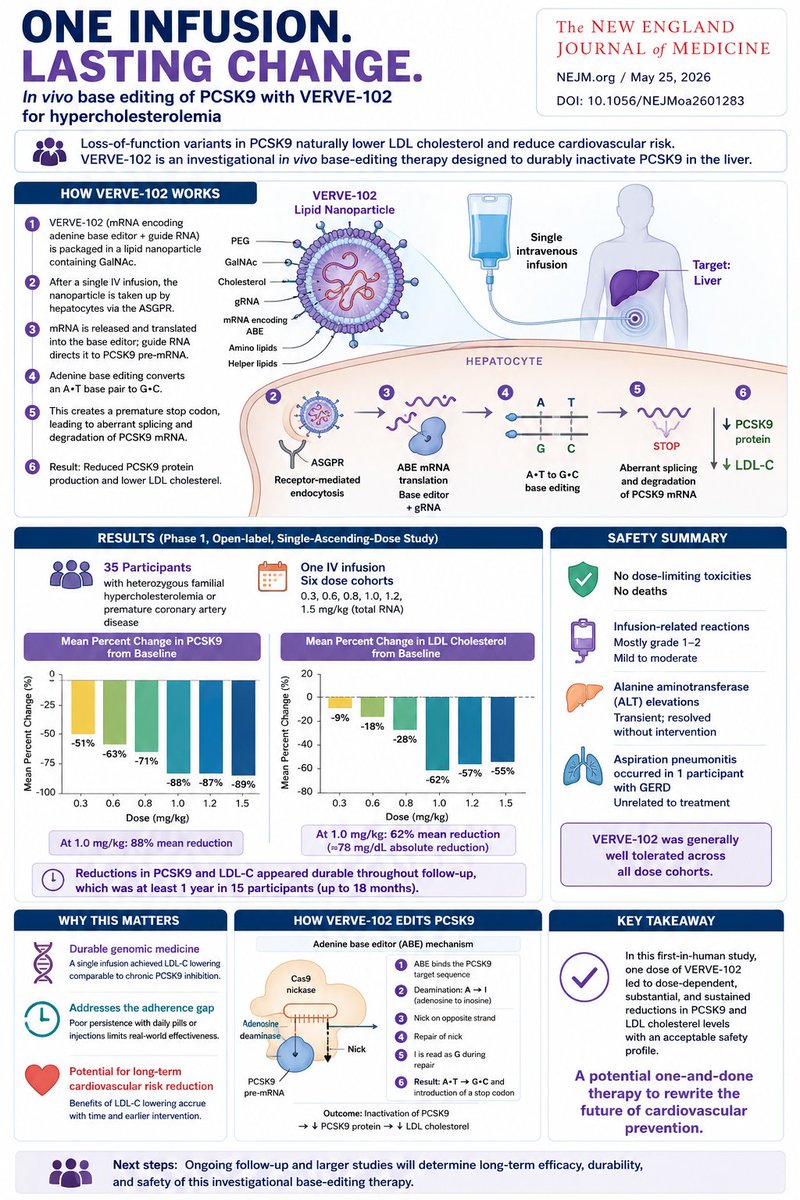
A single infusion to rewrite cardiovascular prevention.
A new phase 1 study in the New England Journal of Medicine reports that in vivo base editing of PCSK9 with VERVE-102 achieved durable LDL-cholesterol lowering after just one intravenous dose.
The concept is elegant: instead of repeatedly blocking PCSK9 with monoclonal antibodies or siRNA, VERVE-102 uses an adenine base editor delivered by a GalNAc-lipid nanoparticle to permanently disrupt PCSK9 splicing in hepatocytes. The edit converts an A•T base pair into G•C, introduces a premature stop codon, and suppresses hepatic PCSK9 production.
This is not conventional CRISPR cutting. The platform uses a Cas9 nickase plus adenine deaminase, avoiding double-strand DNA breaks — a key safety consideration for therapeutic genome engineering.
In 35 patients with heterozygous familial hypercholesterolemia or premature coronary artery disease, the highest dose (1.0 mg/kg) produced:
88% mean reduction in circulating PCSK9
62% mean reduction in LDL cholesterol
~78 mg/dL absolute LDL reduction
durability extending up to 12–18 months in ongoing follow-up
Importantly, the LDL reduction magnitude approaches what is typically achieved with chronic PCSK9 inhibition — but here after a single infusion.
Safety remains the critical question in all in vivo editing platforms. In this interim analysis:
no dose-limiting toxicities occurred
no deaths occurred
infusion reactions were mostly grade 1–2
transient ALT elevations resolved rapidly
one aspiration pneumonitis event was judged unrelated to therapy
The broader implication is substantial.
Cardiovascular prevention has historically depended on adherence: daily statins, periodic injections, pharmacy access, persistence over decades. Yet real-world discontinuation rates for lipid-lowering therapy often reach 30–50% within a year.
VERVE-102 represents a different model:
“one-and-done” genomic prevention medicine.
If long-term efficacy and safety hold, cardiovascular therapeutics may shift from chronic pharmacology toward durable genomic reprogramming of disease risk itself.
This study also signals something larger for the CRISPR field: base editing is moving beyond rare monogenic diseases into common cardiometabolic disorders with population-scale relevance.
Twenty years after natural PCSK9 loss-of-function variants revealed lifelong cardioprotection, medicine is now attempting to intentionally recreate that biology with programmable editing.
DOI: 10.1056/NEJMoa2601283
3
147

May 20
1️⃣3️⃣ Cardiac rehabilitation must be automatic after CABG
All eligible CABG patients should be referred to cardiac rehabilitation, ideally within 4 weeks of discharge. Best results occur when rehabilitation begins preoperatively, continues during hospitalization, and extends into outpatient or tele-rehabilitation care.
1️⃣4️⃣ Obesity management is now part of CABG secondary prevention
Obesity should be treated as a chronic disease, not just a BMI number. Lifestyle, behavioral therapy, structured exercise, and modern anti-obesity pharmacotherapy, especially GLP-1–based therapy when appropriate, may reduce cardiovascular risk after CABG.
1️⃣5️⃣ Vaccination is cardiovascular prevention
Influenza, COVID-19, and pneumococcal vaccination should be considered in post-CABG patients according to risk profile. Influenza vaccination has evidence for reducing cardiovascular events in ASCVD patients.
1️⃣6️⃣ Mental health is not optional after CABG
Depression, anxiety, frailty, and cognitive impairment are common before and after CABG and reduce adherence to secondary prevention. Screening and intervention should be part of routine CABG care.
CME INDIA Take-Home Message
After CABG, the prescription is not only aspirin and statin. The modern post-CABG survival package is: antiplatelet therapy, aggressive LDL lowering, BP control, diabetes cardioprotection with SGLT2i/GLP-1 RA, smoking cessation, cardiac rehabilitation, obesity care, vaccination, and mental health support. CABG fixes flow; secondary prevention protects the future.
2
187

May 20
More exercise, more cardioprotection — but the 3 labs that actually show that protection working in your body are almost never ordered by default.
Compiled the ones to ask for, with the diaspora context that changes the interpretation 👇
May 20

3 labs that predict heart attack risk better than total cholesterol — and most doctors skip all 3:
→ ApoB (particles, not volume)
→ Lp(a) (genetic, often missed, often fatal)
→ hs-CRP (inflammation; runs higher in Black adults)
Save this. Ask for them at your next visit.
2
507

May 19
Amazing editorial highlighting how EPA-derived pro-resolving mediators may help explain EPA-EE’s cardioprotection beyond triglyceride lowering, with potential roles in inflammation resolution and plaque stabilization!

Honored to share our editorial in the European Heart Journal, written alongside @LaylaAbushamat & the incredible @CBallantyneMD, discussing pre-clinical work by Alcover et al. doi.org/10.1093/eurheartj/eh… doi.org/10.1093/eurheartj/eh…
#REDUCEIT #EPA #Cvprev #Resolvins #CardioTwitter #EHJ
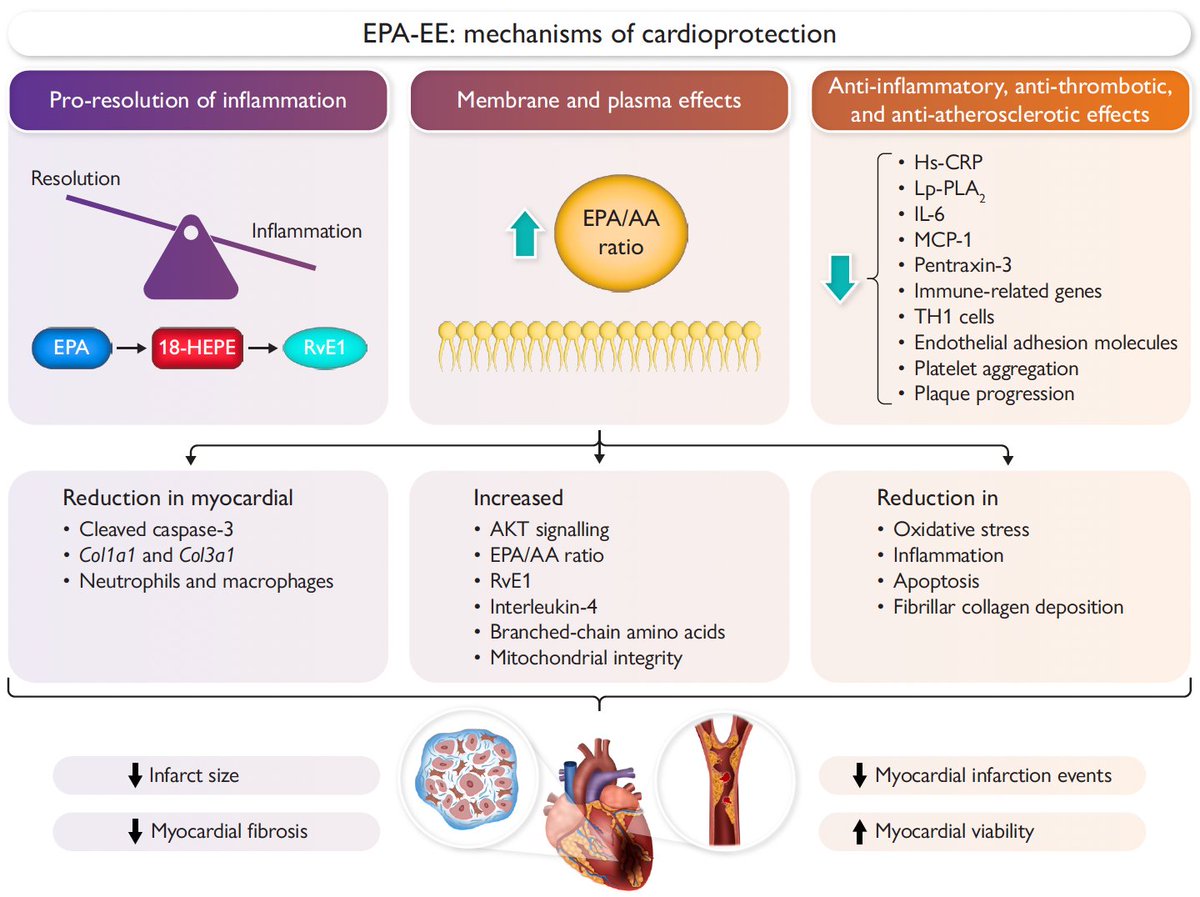
ALT Eicosapentaenoic acid ethyl ester (EPA-EE) reduced infarct size in a hypertriglyceridemia rat model. MI-related mortality nearly halved with EPA-EE (29% vs 56%), a strong trend despite p = 0.07. EPA-EE favored a pro-resolving response, boosting RvE1 levels and improving metabolomic & lipidomic profiles both systemically and in the infarcted heart. Cardioprotection via anti-inflammation, reduced apoptosis & fibrosis, and preserved mitochondrial integrity. EPA/AA ratio was the strongest predictor of infarct size (p < 0.001). The REDUCE-IT trial showed EPA-EE reduces MACE and MI rates. This preclinical work is hypothesis-generating for the mechanisms that may underlie those clinical benefits beyond TG lowering.
1
4
361