
Jun 11
Has anyone used DermaSensor, and if so, how has your experience been?
It sounds like it is a great adjunct for PCPs. @pgipe @AtlasMD @Steelmanmedical @docshanep
5
8
933

.@DermaSensor receives CE mark for skin cancer detection device bioworld.com/articles/731800 #medtech #skincancer
2
353

Jun 11
MedTech news with Smarteeva: 11 June
☑️ @JNJNews expands US availability of an intraocular lens. It designed the extended depth of focus (EDOF) lens to support visual clarity and quality for patients undergoing cataract surgery.
☑️ @KarlStorz gets FDA nod for exoscope for open surgery. It offers the ability to switch into NIR imaging using indocyanine green (ICG) to help reveal important information invisible to the naked eye.
☑️ @DermaSensor wins CE mark for skin cancer detection device. The technology uses hundreds of wavelengths of light in a manner similar to how sonar uses sound.
☑️ @Gore wins CE mark for Fortegra venous stent. It’s the latest addition to the Viabahn device family, engineered to treat patients with deep venous disease.
☑️ @AbbottNews launches next-gen CardioMEMS Hero pulmonary artery pressure reader in US. The CardioMEMS sensor’s design enables it to help people and their physicians proactively manage heart failure.
#InsightswithSmarteeva #Medtech #complaintmanagement #Pharma #Smarteeva #biotech #medtechtrends #medtechindustry #medicaltechnology #technology #health #medicaldevicediagnostics #ai #mdr #recalls #complaints #mir #fda #cvr
46

Jun 11
DermaSensor is expanding internationally with its skin-cancer detection device, receives $5M investment refreshmiami.com/news/dermas…
via @refreshmiami @ndahlberg @DermaSensor #MiamiTech #RefreshMiami #DermaSensor
48

Could @DermaSensor NHS study turn AI skin cancer tools into primary care infrastructure? pharmadevicenews.com/could-d… Find out how DermaSensor’s CE Mark and NHS study could reshape AI-assisted skin cancer assessment across European primary care. #DermaSensor #SkinCancer #MedicalDevices #AIDiagnostics #Dermatology #MedTech #DigitalHealth #PrimaryCare #HealthcareAI #CancerDetection
12
Javed retweeted

Jun 10
Latest Refresh Miami News: DermaSensor is expanding internationally with its skin-cancer detection device, receives $5M investment refreshmiami.com/news/dermas… #miamitech #miamistartups

2
5
389

Jun 10
Love seeing what DermaSensor has been able to do ever since they came through Miami Angels back in 2019.
Keep it up! 👏
Jun 10

A Miami medtech just unlocked Europe, and it did it with a certification most startups never reach.
DermaSensor’s handheld, AI-powered skin cancer assessment device earned a Class IIb CE Mark, and the company paired the milestone with a $5M investment.
The interesting part is what this changes about commercialization, partnerships, and how far a Miami-built clinical device can scale.
refreshmiami.com/news/dermas…
#RefreshMiami #MiamiTech @DermaSensor
ALT Miami’s DermaSensor Just Got Cleared For Europe, And $5M Behind It
10

Jun 10
A Miami medtech just unlocked Europe, and it did it with a certification most startups never reach.
DermaSensor’s handheld, AI-powered skin cancer assessment device earned a Class IIb CE Mark, and the company paired the milestone with a $5M investment.
The interesting part is what this changes about commercialization, partnerships, and how far a Miami-built clinical device can scale.
refreshmiami.com/news/dermas…
#RefreshMiami #MiamiTech @DermaSensor
ALT Miami’s DermaSensor Just Got Cleared For Europe, And $5M Behind It
85

Jun 10
NEW! @DermaSensor is expanding internationally with its skin-cancer detection device, receives $5M investment. "Rest of world, here we come" refreshmiami.com/news/dermas… @refreshmiami #MiamiTech
39

Hear directly from Dr. Joseph Gomes on how DermaSensor™ has enhanced his practice — from real-time clinical decision-making to streamlined patient care workflows.
Learn more at dermasensor.com.

16




May 6
Meet the Silicon Valley episode Founders! Follow the Meet the Drapers America tour and get to know these amazing founders and their companies
@DermaSensor Vivifi Medical @datakrypto Gene Lean 360
1
6
165

May 6
Innovation & Interactions | Glimpses from TiEcon 2026, USA 🇺🇸
STPI marked its presence at TiEcon 2026, one of the world’s premier tech gatherings, amidst a dynamic convergence of industry leaders, tech visionaries and AI pioneers. ⚙️✨
From insightful discussions to future-forward dialogues led by Nobel laureates, the conference dove into meaningful conversations on disruption, innovation and the evolving role of technology in shaping tomorrow.
#TiE #Tiecon #USA #Tech #TechConference #Technology #Startups #India #SiliconValley #AI #Innovation #DigitalIndia #STPI #STPIINDIA
@GoI_MeitY @AshwiniVaishnaw @JitinPrasada @SecretaryMEITY @arvindtw @_DigitalIndia @NeGD_GoI @startupindia @TiEDelhi @tiesv @DermaSensor @cloudeagleai @guptaa_sanjay @Shail2108 @easiofysolution @DeepCogLabs
74
83
641
May 6
BTS with Cody Simmons, CEO of @DermaSensor, where they are using AI driven technology, FDA approved device to detect skin cancer, a non invasive solution.

3
290
May 5
Snapshot of TiEcon 2026 | STPI at one of the world’s premier tech gatherings
From insightful discussions with eminent panelists to forward-looking dialogues led by Nobel laureates, TiEcon 2026, held in the USA, convened some of the most powerful perspectives on innovation and human potential.
During the event, Shri Shailendra Tyagi, Director, STPI Mohali, felicitated leading tech innovators at the prestigious TiE50 Awards Ceremony. He also interacted with distinguished participants, exploring avenues for collaboration and highlighting STPI’s core offerings and initiatives.
Further, Shri Vikas Garg, Joint Director, STPI HQ, also joined in the event and briefed industry leaders about various STPI services and its role in nurturing India's startup ecosystem.
Glimpses from the event:
#TiE #Tiecon #USA #Tech #TechConference #Technology #Startups #India #SiliconValley #AI #Innovation #DigitalIndia #STPI #STPIINDIA
@GoI_MeitY @AshwiniVaishnaw @JitinPrasada @SecretaryMEITY @arvindtw @_DigitalIndia @NeGD_GoI @startupindia @TiEDelhi @tiesv @DermaSensor @cloudeagleai @Shail2108




67
72
521

De nombreux médecins généralistes se sont déjà formés à la dermatoscopie en particulier numérique et au dépistage de carcinomes ou des mélanomes. L'intelligence artificielle devrait encore plus nous aider dans un avenir très proche. En particulier, je pense à des dispositifs médicaux comme le DermaSensor qui utilise une combinaison de spectroscopie optique de pointe et d'intelligence artificielle pour analyser rapidement les lésions cutanées suspectes et qui sont entraînés sur des milliers de lésions diagnostiquées.
aimatmelanoma.org/fr/Diagnos…
On a, hélas, une pénurie importante de ces spécialistes, donc gâcher du temps dermatologique déjà contraint pour du dépistage de mélanome avec un très faible rendement, est difficilement défendable.
@Dermatopoullos

2
3
24
4,238


𝑺𝒉𝒐𝒖𝒍𝒅 𝑨𝑰 𝒊𝒏𝒕𝒆𝒈𝒓𝒂𝒕𝒆 𝒘𝒊𝒕𝒉 𝑪𝒍𝒊𝒏𝒊𝒄𝒂𝒍 𝑾𝒐𝒓𝒌𝒇𝒍𝒐𝒘?
𝑰𝒏𝒄𝒓𝒆𝒂𝒔𝒊𝒏𝒈𝒍𝒚, 𝑵𝑶 ... 𝒂𝒏𝒅 𝒕𝒉𝒂𝒕'𝒔 𝒂 𝒈𝒐𝒐𝒅 𝒕𝒉𝒊𝒏𝒈!
This advice is becoming more questionable, if not obsolete.
Yes, AI scribes, apps like OpenEvidence, and use of AI in radiology, cardiovascular care, and serology have integrated into current workflows. They've compressed timeframes, improved diagnoses, and allowed HCPs to be more present with patients and reduced cognitive loads that have resulted in HCPs burnout.
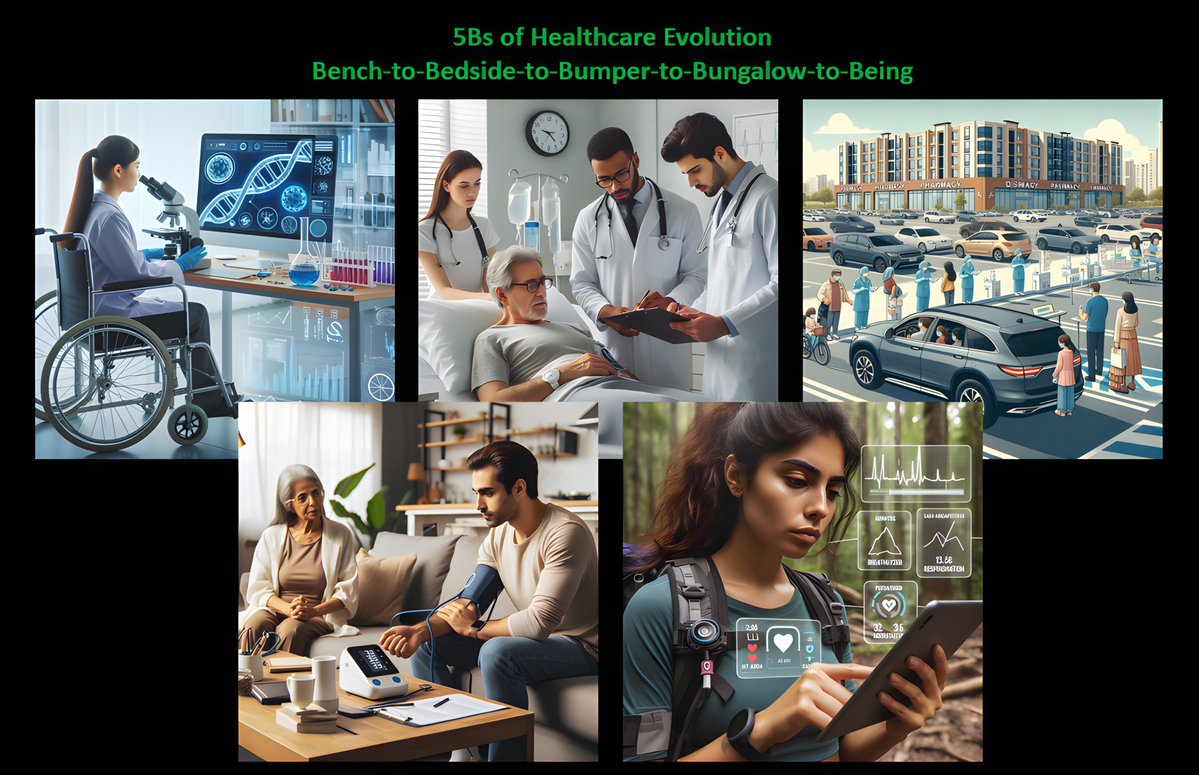
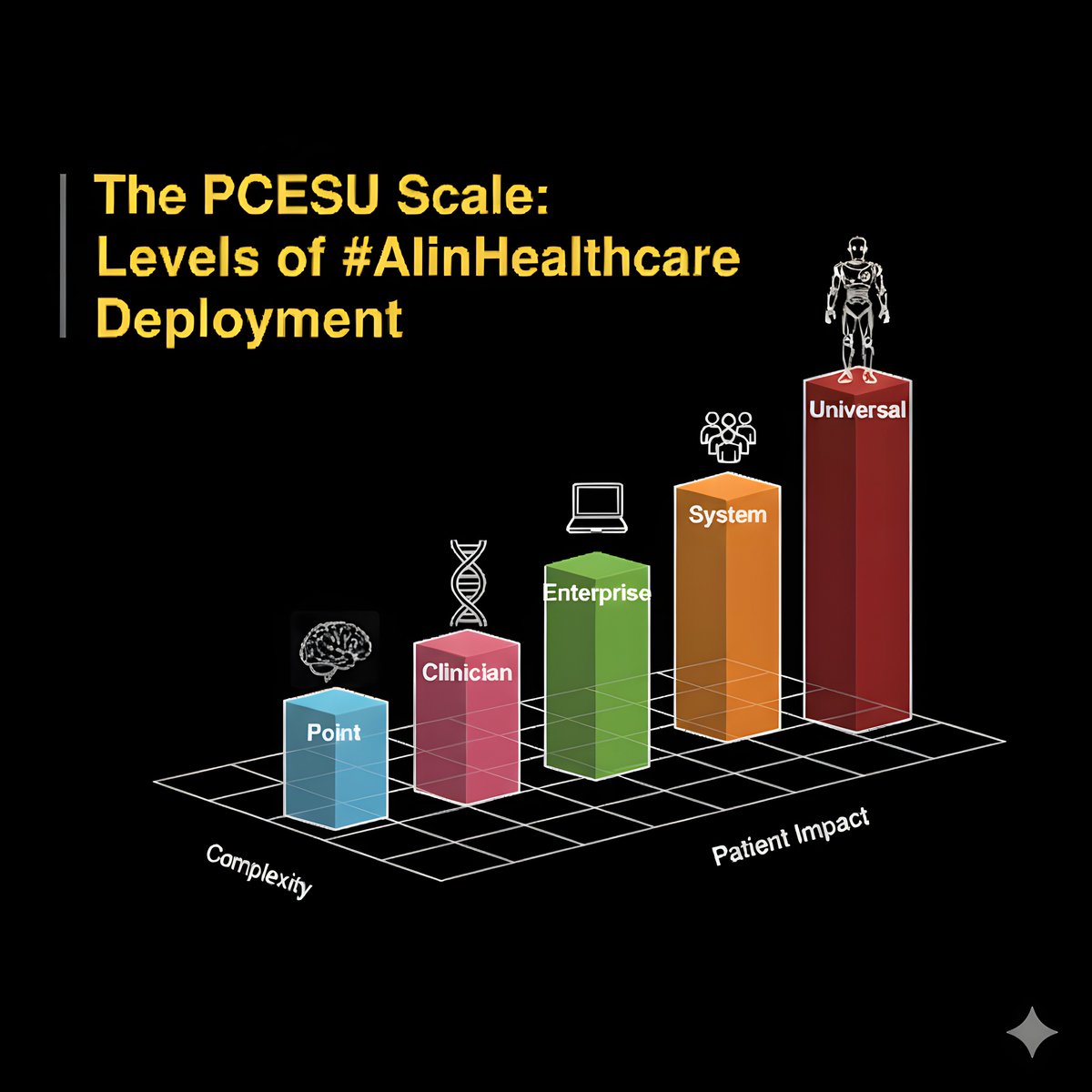
However, clinical workflows are often built around the pysical design of legacy facilities, outdated scopes of practice, and changing locations as portrayed in my 5Bs of Healthcare Evolution framework. In addition, AI in Healthcare deployment is rapidly moving along the five levels of the PCESU scale.
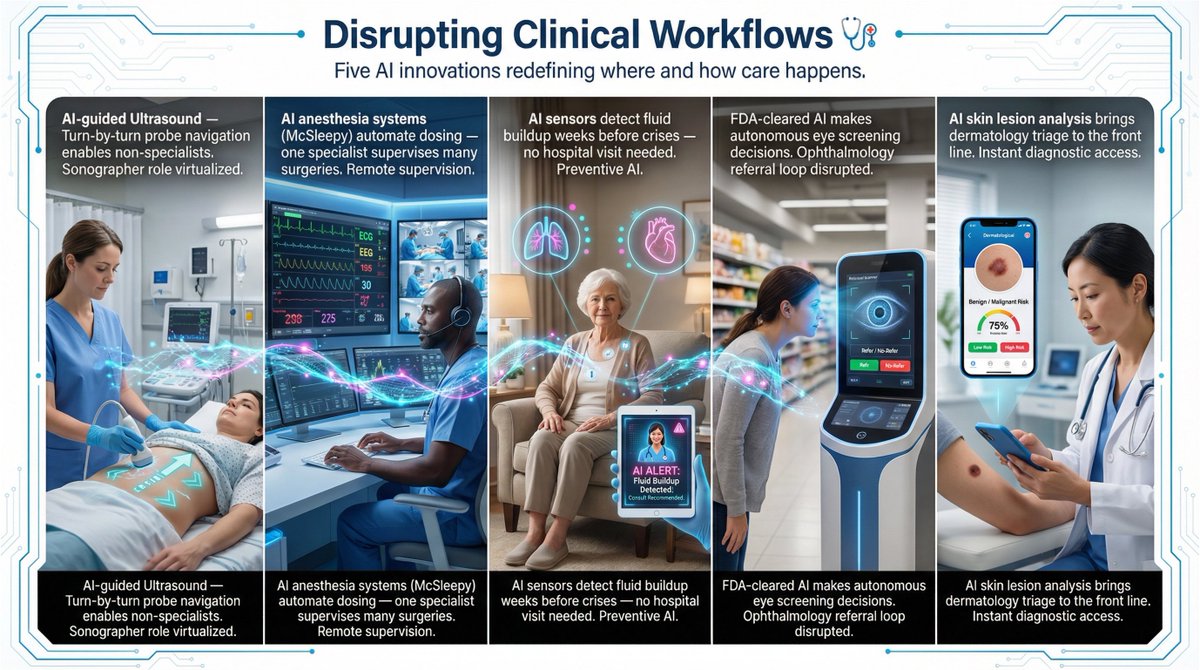
These AI innovations don't fit with clinical workflows; they change them.
1️⃣ Ultrasounds usually require a specialized sonographer with years of training in probe manipulation. Caption Health (a GE Healthcare company) provides real-time, turn-by-turn "GPS" guidance. It tells a medical assistant or nurse exactly how to tilt, slide, and rotate the probe to capture a diagnostic-quality image. This replaces the need for a sonographer for routine scans. And, the scan can occur at an ER bedside or a retail pharmacy by a tech.
2️⃣ Anesthesia has been a procedure where an anesthesiologist must stay in the room (by law or regulation) to manually administer anesthesia drugs. AI systems (like McSleepy), developed at McGill University, monitor brain waves (EEG) and vitals to deliver the exact dose of propofol or remifentanil every few seconds during surgery. Today, an anesthesiologist can "supervise" up to 10 operating rooms simultaneously from a central cockpit.
3️⃣ Heart Failure can require surgery (implanting sensors) or frequent hospital visits for fluid-level checks by cardiology nurses. Now, AI-powered sensors (RFID or Optical AI) can detect lung fluid buildup and heart rate variability in a patient's home. Clinic visits are removed for routine monitoring and surgery, and the AI can predict a "crash" weeks in advance, alerting a remote monitoring center.
4️⃣ Diabetic Retinopathy Screening usually requires a referral to an Ophthalmologist to look at the back of the eye. Now, LumineticsCore from Digital Diagnostics is FDA approved to make a "Refer/No-Refer" diagnostic decision without this specialized HCP. The referral loop disappears and a patient can get their eye checked by a machine at a local grocery store clinic or a GP's office.
5️⃣ Dermatology Triage for a skin lesion usually starts with a doctor's referral to a dermatologist (often, a wait of many months). DermaSensor, Inc. - AI-Powered Skin Cancer Detection Device allows doctor to get an instant, high-accuracy assessment of whether a mole is "benign" or "malignant." Screening is put into the hands of a primary care provider or even patients via smartphone apps.
And wait for my post this Saturday on PredictiveAI, it is obliterating workflows.
6
5
14
1,240