
Jmml j’hesite entre arriver a la gare à 17h00 (mon train est à 14) sachant que je devrais traverser TT la gare pr y arriver ou alors j’y suis à 16h30…
1
21


May 25
Gran cierre de temporada y con la apuesta por la continuidad del mister, buscando seguir creciendo el próximo año.Aúpa Alba!!
3
39

Onda Deportiva Albacete. 25/05/2026.
🎙️Dirigido por @jmml en una tertulia con @georgebest84 y @ROVANIEMIAB
🏀🏐Play-off: Albacete Basket ganó 70 a 64 al Amics Castelló y el Albacete FS perdió 6-2 ante el filial del Palma Futsal
ondacero.es/podcast/emisoras… a través de @AlbaceteCero
2
6
7
346

Editors’ Pick by Cancer Research Catalyst
@AACR
RAS-driven plasticity and oncofetal reprogramming as a key mechanism and vulnerability in JMML.
The article is freely available for a limited time:
aacr.org/blog/2026/03/27/edi…
#hematology
#oncology
#epigenetics
#development
3
116

Apr 9
若年性骨髄単球性白血病(JMML)は、乳幼児に発症する治療が難しい希少疾患
高感度な新しい解析技術を用いて微細な遺伝子変異を網羅的に検出
診断時にごく一部の白血病細胞にしか存在しない遺伝子変異であっても、病気の進行や治療成績に大きく影響することが分かった
Apr 9

【注目プレスリリース】超高感度次世代シーケンスで若年性骨髄単球性白血病の「微小クローン」を可視化~見逃されてきた遺伝子変異が予後不良と強く関連~ / 名古屋大学 research-er.jp/articles/view…
4
15
1,788

Feb 25
For those of you who are fans of Micky Redmond, @DetroitRedWings, @NHL @usahockey or just hockey in general. This little kids family can use your help Fundraiser by Logan Wonfor : Support Teddy’s Fight Against JMML Leukemia gofundme.com/f/support-teddy…
3
1
1
96

🧬 KRAS Somatic Mutation vs Inherited RASopathy in AML — 50 Pearls (with emojis)
1.🧬 Somatic KRAS = acquired mutation in leukemic clone; not present in all body cells.
2.🧬 RASopathy = germline pathogenic variant in RAS/MAPK pathway (e.g., PTPN11, SOS1, KRAS, RAF1, BRAF, SHOC2, NRAS, CBL, NF1), present in every cell.
3.🎯 AML usually involves somatic mutations; germline RASopathy–linked myeloid disease is far rarer in adults (classically pediatric overlap).
4.🧩 Inherited RASopathies most strongly associate with JMML / myeloproliferation of infancy, not classic adult AML.
5.📌 Key clinical consequence: germline = family counseling surveillance donor selection implications; somatic = prognosis/therapy only.
🔬 Biology / Where the mutation “lives”
6.🧪 Somatic KRAS: detected in marrow/blood tumor DNA; may clear with remission.
7.🧬 Germline RASopathy: variant persists in non-hematologic tissues (skin fibroblasts best).
8.⚠️ Testing pitfall: using blood/saliva can be contaminated by clonal hematopoiesis/leukemia—false “germline” calls.
9.✅ Best confirmation of germline: cultured skin fibroblasts (or truly non-hematopoietic tissue).
10.📉 Somatic KRAS often shows variable VAF depending on blast % and subclonality; germline tends toward ~50% (heterozygous) but VAF alone is not definitive.
👤 Phenotype clues (when to suspect RASopathy)
11.👶 If AML is in a patient with lifelong syndromic features, think germline RASopathy.
12.❤️ Congenital heart disease (esp. pulmonary valve stenosis/hypertrophic cardiomyopathy in Noonan-spectrum) supports RASopathy.
13.📏 Short stature, characteristic facies, developmental history → raises pretest probability.
14.🧠 Neurocutaneous features (e.g., NF1 stigmata) can overlap with RAS/MAPK disorders.
15.👪 Family history of similar phenotype ± cancers supports germline.
16.🧾 Past childhood “myeloproliferation/JMML-like” episodes or cytopenias → big clue.
17.🩺 Multiple congenital anomalies cancer risk syndromes → consider germline evaluation.
📊 Cancer risk signal (RASopathy side)
18.📈 RASopathies carry elevated cancer risk, including strong signals for JMML.
19.⚠️ Germline KRAS-related RASopathy has been reported with very high standardized incidence ratios for JMML (rare but striking).
20.🧒 Practical translation: most “RASopathy myeloid malignancy” literature is pediatric-heavy; adult AML association is uncommon.
🧾 Frequency & prognostic signal (somatic KRAS in AML)
21.🧬 NRAS/KRAS are recurrent AML mutations; frequency varies by cohort/therapy context.
22.📉 Multiple datasets suggest KRAS (more than NRAS in some series) may correlate with inferior outcomes in certain contexts.
23.💉 In HMA-based regimens (incl. HMA ven), RAS-pathway mutations have been linked with relapse/resistance patterns in some analyses.
24.🧩 Co-mutation patterns matter (e.g., signaling epigenetic/spliceosome) more than KRAS alone.
25.🧠 Remember: ELN 2022 risk grouping is driven mainly by cytogenetics select gene entities; RAS mutations are not primary ELN-defining favorable/adverse markers.
🧭 When to pursue germline workup in “KRAS AML”
26.🚩 AML syndromic features (Noonan/CFC/Costello/NF1-like) → germline evaluation.
27.🚩 AML at unusually young age with suggestive phenotype/family history → evaluate.
28.🚩 Variant persists at ~50% VAF in morphologic remission (and/or across timepoints) → evaluate germline.
29.🚩 Multiple malignancies or strong family clustering → evaluate.
30.🚩 Planned related donor transplant: rule out inherited predisposition in patient/donor when suspicion exists.
🧫 Lab strategy (high-yield practicalities)
31.🧪 Do paired tumor–normal sequencing when possible (tumor = marrow; normal = skin fibroblasts).
32.🧬 If only saliva is available, interpret cautiously (can contain blood-derived DNA).
⸻
2
2
10
365

Grateful to @JianXuLab for this perspective highlighting how oncogenes, developmental ontogeny, and cellular plasticity intersect in pediatric leukemia, alongside the JMML study by @mp_hartmann and @dblipka1. @BCD_AACR @CD_AACR aacrjournals.org/bloodcancer…
1
6
18
2,948
JMML stem cells aren’t epigenetically “stuck” in a fetal state.
They mature postnatally—yet show striking transcriptional plasticity, with oncofetal reprogramming in high-risk disease, challenging the classic “maturation block” model.
doi.org/10.1158/2643-3230.BC…
#JMML #epigenetics
2
86
🧬📊 Post-Allo-HSCT Chimerism: 50 High-Yield Pearls
1️⃣ 🩸 Peripheral blood is the specimen of choice in most cases.
2️⃣ 🦴 Bone marrow chimerism is reserved for selected scenarios (e.g. discordant PB results).
3️⃣ 🧪 STR-based assays remain standard of care (LoD ~1–5%).
4️⃣ ⚠️ Always report assay LoD—interpretation depends on it.
5️⃣ ⏱️ Routine TAT <2 weeks; urgent results <5 working days.
6️⃣ 📈 Serial trends > single values—falling donor % matters.
7️⃣ 🧬 Chimerism MRD are complementary, never substitutes.
8️⃣ 🧫 Lineage-specific testing (CD3, CD15, CD19, CD34) adds precision.
9️⃣ 🔍 Subset purity must be reported to avoid false results.
🔟 ❌ FISH is rarely indicated for chimerism.
1️⃣1️⃣ 📆 Day 30 whole-blood STR is recommended for baseline risk.
1️⃣2️⃣ 🧠 Early mixed chimerism may reflect graft kinetics—not always relapse.
1️⃣3️⃣ 📉 >5% sequential donor drop is concerning in malignant disease.
1️⃣4️⃣ 🧑🔬 T-cell (CD3) chimerism guides immune manipulation best.
1️⃣5️⃣ 🚨 Mixed myeloid chimerism in malignancy → investigate promptly.
1️⃣6️⃣ 🔄 Confirm abnormal results before intervention.
1️⃣7️⃣ 💊 IS taper is first response to falling donor chimerism.
1️⃣8️⃣ 🧪 pre-DLI is evidence-based for mixed T-cell chimerism.
1️⃣9️⃣ ⚖️ Fractionated DLI reduces GVHD risk.
2️⃣0️⃣ 🛑 High GVHD risk → individualize chimerism-driven actions.
2️⃣1️⃣ 🧠 RIC T-depletion commonly yield mixed chimerism.
2️⃣2️⃣ 🧩 Alemtuzumab regimens → expect prolonged mixed T-cell chimerism.
2️⃣3️⃣ 🩺 AML: MDTC MRD positivity = highest relapse risk.
2️⃣4️⃣ 🧬 Molecular MRD (e.g. NPM1) may trump chimerism for DLI timing.
2️⃣5️⃣ 🧾 ALL adults (TBI-MAC): mixed chimerism is always concerning.
2️⃣6️⃣ 📅 Adults (malignant): CD3/CD15 at D 60, 100, then q3 months ×2y.
2️⃣7️⃣ 🛑 Stable full donor ×2 years → chimerism follow-up can stop.
2️⃣8️⃣ 🧠 Myelofibrosis: act on molecular relapse more than chimerism alone.
2️⃣9️⃣ 🧬 DLI more effective in molecular vs hematologic relapse.
3️⃣0️⃣ ⚠️ Context matters—conditioning, serotherapy, disease biology.
3️⃣1️⃣ 🧒 Children: thresholds less rigid; MRD correlation essential.
3️⃣2️⃣ 🧠 Paediatric ALL: DLI used cautiously due to CAR-T eligibility.
3️⃣3️⃣ 🧪 JMML: early IS withdrawal critical; chimerism monitored frequently.
3️⃣4️⃣ 🧬 Non-malignant diseases require lineage-specific targets.
3️⃣5️⃣ 🧫 CGD: ≥50% donor myeloid usually sufficient.
3️⃣6️⃣ 🧬 SCD: ≥20–25% donor myeloid can reverse phenotype.
3️⃣7️⃣ 🔁 SCD: unstable mixed chimerism risks late graft failure.
3️⃣8️⃣ 🧠 Aplastic anemia: persistent mixed T-cell chimerism is acceptable.
3️⃣9️⃣ ❌ Do NOT chase T-cell chimerism in AA—GVHD risk outweighs benefit.
4️⃣0️⃣ 🧩 IEI: full donor chimerism often unnecessary for cure.
4️⃣1️⃣ 📆 Non-malignant: monthly ×6 months → spaced surveillance to 5 years.
4️⃣2️⃣ 🧬 Functional assays (e.g. DHR, enzyme levels) complement chimerism.
4️⃣3️⃣ 🔬 NGS/dPCR/qPCR = promising but not standard yet.
4️⃣4️⃣ 💰 Cost & interpretability limit ultra-sensitive assays.
4️⃣5️⃣ 🧪 Microchimerism thresholds for action are undefined.
4️⃣6️⃣ 📊 EQA participation is mandatory for laboratories.
4️⃣7️⃣ 🧾 Reports must state “minimum % donor = full donor”.
4️⃣8️⃣ 🧠 Chimerism separates poor graft function vs rejection early.
4️⃣9️⃣ 🧑⚕️ Management decisions must be multidisciplinary.
5️⃣0️⃣ 🎯 Bottom line: chimerism is a dynamic clinical tool, not a number.
⸻
🔗 Reputable Sources (Guidelines & Reviews)
•British Journal of Haematology 2025 – UK recommendations for chimerism testing post-allo-HSCT
doi.org/10.1111/bjh.70061
•EBMT Practice Recommendations (2024 update) – DLI & post-HSCT monitoring
ebmt.org
•Blouin & Askar. Bone Marrow Transplant 2022 – Chimerism for clinicians
doi.org/10.1038/s41409-021-0…
1
15
647

Jan 24
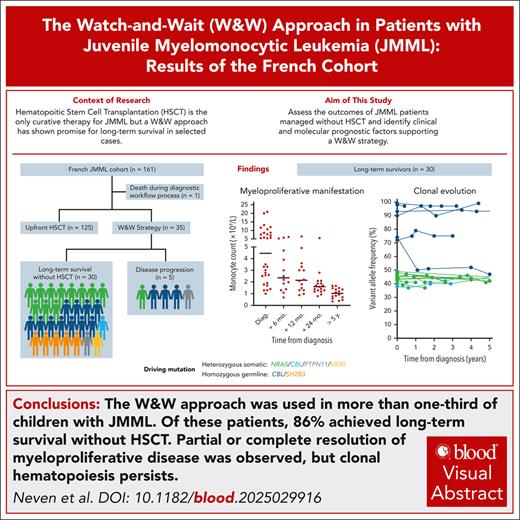
Results of a French cohort showed that the watch-and-wait (W&W) approach in children with Juvenile Myelomonocytic Leukemia (JMML) may be a promising alternative to hematopoietic stem cell transplantation (HSCT) in 86% of these children who showed long-term survival, with partial or complete resolution of the myeloproliferative neoplasm, potentially sparing them the HSCT-associated risks. However, with clonal hematopoiesis persistence and the high risk of extrahematological complications manifesting as failure to thrive, slowing of growth and development, organ dysfunction, and leukemic cell infiltration into bone marrow and other body organs, long-term monitoring remains essential. JMML is a rare aggressive pediatric MPN with onset at<4 years with peak at 2 years of age. It is caused by mutations in the RAS oncogenes: PTPN11, NRAS, KRAS, CBL, NF1 or homozygous germ line mutations like SH2B3, for which HSCT is currently the only established curative therapy.

The W&W approach was used in more than one-third of children with JMML; 86% of these patients achieved long-term survival without HSCT. Read the full article in Blood: ow.ly/fsfs50Y1jf6 #BloodJournal
3
248

The W&W approach was used in more than one-third of children with JMML; 86% of these patients achieved long-term survival without HSCT. Read the full article in Blood: ow.ly/fsfs50Y1jf6 #BloodJournal
2
2
11
1,578

Jan 13
This is pernio-like leukemia cutis secondary to juvenile myelomonocytic leukemia (JMML).
Jan 12

9yo/👦🏼 w/ NF-1 presented w/ 2 months of progressive fatigue, severe pain, edema, & violaceous lesions of the hands and feet. Symptoms began as intermittent foot pain, followed by systemic symptoms treated as viral illness & later pneumonia. Cutaneous lesions worsened w/ blistering & severe shooting pain, limiting ambulation & fine motor function.
O/E: dusky, eroded papules & plaques w/ hemorrhagic crust on the dorsal fingers & toes, w/ marked digital edema but no joint effusion.
Labs revealed severe anemia (Hgb 6.1 g/dL) w/ normal WBC & platelets. Peripheral flow cytometry showed monocytosis (>1 × 10⁹/L) w/ 4% blasts & low reticulocyte count. BMBX showed myeloid predominance w/ dysplasia of myeloid & erythroid lineages and an NF1 E524 mutation.
What’s the DDx❔


3
2
15
886
Jan 13
This is pernio-like leukemia cutis secondary to juvenile myelomonocytic leukemia (JMML).
The differential included infectious, rheumatologic, & neoplastic etiologies; malignancy was favored given acral violaceous lesions, anemia with thrombocytopenia, & underlying NF1. The patient was diagnosed with JMML and treated with mercaptopurine as a bridge to IV chemotherapy, followed by allogeneic stem cell transplantation, with improvement in cutaneous ulceration & edema.
Pernio-like leukemia cutis is rare, particularly in pediatric JMML. While pernio typically presents as cold-induced violaceous acral papules and plaques, persistent or atypical lesions may indicate systemic disease. In JMML, hyperviscosity & leukemic infiltration likely predispose to acral involvement. NF1 increases JMML risk, though leukemia cutis remains uncommon. JMML is aggressive and often chemoresistant; allogeneic stem cell transplantation is the mainstay of therapy.
ALT https://www.slideshare.net/slideshow/classification-of-all-and-amlpptx/258716985
6
596

🔴 Diagnosis: Juvenile myelomonocytic leukemia (JMML)
📍 NF1 patient, severe anemia, monocytosis, 4% blasts
📍 Skin: dusky, violaceous papules/plaques with edema & hemorrhagic crusts
🔷 BMBx: myeloid predominance, dysplasia of myeloid/erythroid lines, NF1 mutation
💡 Consider JMML and other myelodysplastic/myeloproliferative overlap syndromes in the differential
4
292

30 Dec 2025
Your gifts are fuel new research breakthroughs, turning discoveries into safer treatments and giving kids like Josie hope for a healthy future.🎗️
Josie was diagnosed with juvenile myelomonocytic leukemia (JMML) at 5 months old. Only 50% of kids with this rare cancer reach lasting remission.
For Josie, a brand-new clinical trial offered a potential cure without long-term side effects. That trial originated 2,500 miles away, but thanks to our Center of Excellence Grant, Josie could access the treatment at her home hospital in Cincinnati.
The treatment is working! Josie fills the hospital room with joy and sweetness as she coos, laughs, and shows incredible strength through treatment.
Your support of grant funding helped Dr. Elliot Stieglitz as he designed and activated the clinical trial. It will be available in 25 cities by the end of the year, bringing more cures closer to home for children with this cancer.
1
2
477
29 Dec 2025
This week's featured childhood cancer hero is Josie Selke!
Josie is the sweetest, happiest girl. Constantly smiling, laughing, having a good time – her smile lights up rooms and she just radiates joy! She is currently on a clinical trial to help fight her JMML diagnosis, one that Alex's is helping fund.
Her parents hope Josie can grow up and live a long, normal life. For Josie’s sake, they hope for no long-term complications but ultimately that she’s overall happy! She is their hero because she is absolutely the most resilient, strongest, and happiest girl they’ve ever known. Despite being sick her whole life, she always has a smile on her face and a good attitude. Read Josie's story> alexslemonade.org/hero/josie…

1
2
218
20 Dec 2025
🎗️Because of Dr. Elliott’s Stieglitz's research, made possible in part by funding from supporters like you, the future for children with JMML is changing. Through December 31, your gift will have 2X the impact. Arby’s Foundation will generously match online donations made to ALSF here*> alexslemonade.org/contribute…
Clinical trials offer life-changing treatments and new hope for kids like Josie, who is fighting a rare cancer called juvenile myelomonocytic leukemia.
With help from an ALSF grant, Dr. Elliot Stieglitz opened a clinical trial building off his research discoveries for kids with JMML. The trial was available in multiple cities, and Josie was able to enroll at a hospital near her home in Cincinnati.
Today, Josie has celebrated her first birthday and she has hope for a cure. Amazing things are possible for kids with cancer, all thanks to what you do 💛
*Up to $75,000. Only donations made to the form linked above will be matched.
2
4
257
14 Dec 2025
Josie just celebrated her first birthday.🎂 A celebration made possible by a cutting-edge clinical trial funded by supporters like you.
Josie was 5 months old when she was diagnosed with juvenile myelomonocytic leukemia (JMML), a rare pediatric leukemia. Of the kids diagnosed, only half reach long-term remission. There just haven’t been effective treatments for kids with JMML, until now. A brand-new clinical trial offered an upfront treatment: a potential cure without long-term side effects.
Thanks to an ALSF Center of Excellence Grant, Josie could access the treatment at her home hospital in Cincinnati. The treatment is working. And Josie continues to shine.
With your gift, you can fund critical research that can deliver more breakthroughs to help all kids fighting cancer. Through December 31, your gift will have 2X the impact. Arby’s Foundation will generously match online donations made to ALSF here> alexslemonade.org/contribute… *
*Up to $75,000. Only donations made to the form linked above will be matched.
1
1
316