
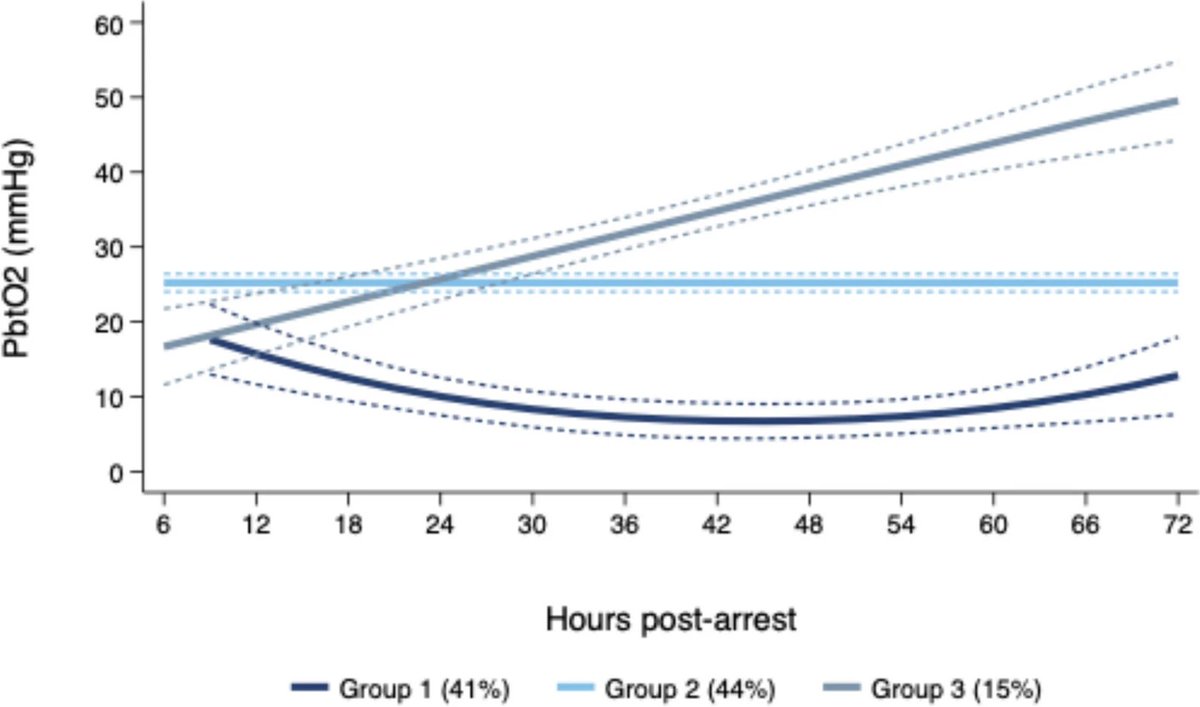
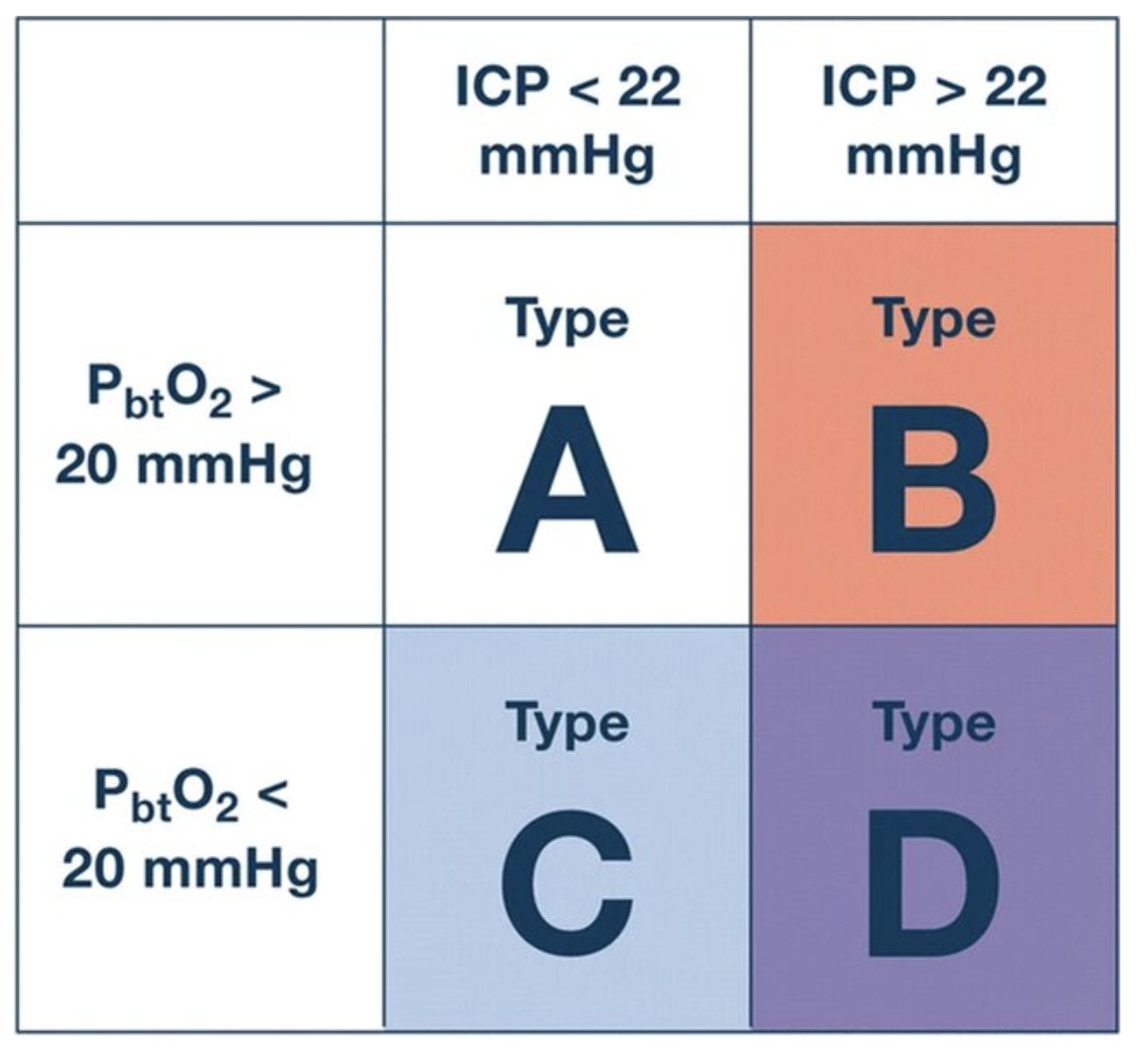
Distinct #ICP and #PbtO2 trajectories may exist after #CardiacArrest. Can we distinguish subtypes of pathology that could respond to targeted treatments? @NeurocritCareJ rdcu.be/fmkrv

1
4
9
758

Fascinating paper. It exposes how deeply we cling to pressure‑based dogma in TBI. Rigid CPP targets won’t move the field forward — evolving toward flow, oxygenation and metabolic monitoring will. Treat the brain, not the number.
#NeurocriticalCare #NeuroTrauma #CBF #PbtO2 #NeuroICU
@NCSIofficial @ISNACCINDIA @isccmnational @deepak_neuro @hhdashneuro @shobanarajan51 @girijarath @neurocritical
May 22

Pressure does not cause blood flow.
Circulation is still often taught as if pressure is the driver and flow simply follows. It doesn’t.
Pressure gradients are part of the description of a flowing system, not independent causes of flow. They emerge with flow from energy input, resistance, compliance, and dissipation.
In this review, we explain how:
• the heart supplies energy
• pressure reflects system state
• flow depends on delivery, acceptance, and dissipation
doi.org/10.1111/anae.70238
1
8
842

Apr 20
Daily Rounds | Day 15 of 120
- BOOST-II (2017): PbtO2-guided care in severe TBI
- PRODEX (2012): Dex vs propofol for prolonged sedation
- ECASS III (2008): Alteplase 3 to 4.5 h after stroke
A lot of time of time spent working on the site this past week and weekend. I think some real noticeable improvements.
Full breakdowns: neurobedside.com

2
144

Apr 16
this is the first thing i made with opus 4.7
check out this prompt
single file index.html w javascript, CORTEX OS — brain-computer interface command platform, threejs renderer w webgl2, 3D BRAIN VISUALIZER full anatomical brain model w hemisphere split toggle, cortical surface mesh w 68-region desikan-killiany atlas parcellation color-coded by function (motor/sensory/visual/auditory/prefrontal/temporal/parietal/occipital/limbic), transparent skull overlay toggle w opacity slider, exploded view mode (separate lobes float apart w labeled connectors showing white matter tracts), subcortical structure isolation viewer (hippocampus/amygdala/thalamus/hypothalamus/basal-ganglia/cerebellum/brainstem individually selectable w info panel showing function/connectivity/associated-pathologies), brodmann area overlay w numbered regions and click-to-highlight, white matter tractography streamlines rendered as fiber bundle tubes (arcuate-fasciculus/corpus-callosum/corticospinal-tract/cingulum/uncinate/superior-longitudinal) w directional color encoding (rgb=xyz), vascular overlay showing circle-of-willis and major cerebral arteries w blood flow velocity animation, ventricular system translucent blue fluid-filled cavities, spinal cord extension w cervical/thoracic/lumbar segment labels and nerve root branching, cranial nerve pathways (all 12) traced from brainstem to target organ, glymphatic system visualization w csf flow particle animation during sleep-state toggle, zoom from whole-brain → lobe → gyrus → cortical-column → individual-neuron-model w dendritic tree and axon terminal boutons and synaptic cleft detail — REAL-TIME EEG ENGINE 256-channel electrode array mapped to 10-20 extended montage positions displayed as interactive dots on 3d scalp surface, live waveform display w per-channel scrolling trace (configurable speed 10/25/50mm-per-sec, amplitude scale µV adjustable), montage selector (referential/bipolar-longitudinal/bipolar-transverse/average-reference/laplacian/custom-montage-builder), frequency band decomposition per channel displayed as stacked power bars (delta-0.5-4hz/theta-4-8hz/alpha-8-13hz/beta-13-30hz/gamma-30-100hz/high-gamma-100-200hz), real-time fft spectrogram w time-frequency heatmap per channel (color = power, x = time, y = frequency), topographic scalp maps (2d head projection w interpolated color gradient showing power distribution per band, animated at configurable refresh rate), coherence matrix heatmap showing phase synchronization between all channel pairs, source localization engine (eloreta/beamformer) projecting scalp signals onto cortical surface mesh in real-time w activation hotspot coloring, artifact detection system (eye-blink/muscle/electrode-pop/line-noise auto-flagged w red highlight and optional auto-rejection), independent component analysis (ica) decomposition viewer w component topomaps and time-courses for manual artifact removal, event-related potential (erp) averager w stimulus-locked epoch extraction and grand-average waveform overlay (p100/n170/p300/n400/p600 component markers), connectivity viewer (directed transfer function/granger causality/phase-locking-value) rendered as animated arrows between brain regions on 3d model w thickness=strength — NEURAL SIGNAL PROCESSING PIPELINE configurable filter chain: bandpass (butterworth/chebyshev/fir w order and cutoff sliders), notch filter (50/60hz w harmonics), adaptive filter for ecg artifact removal, common average reference, surface laplacian (current source density), hilbert transform for instantaneous amplitude/phase extraction, wavelet decomposition (morlet/haar/daubechies w scale selection), multitaper spectral estimation w confidence intervals, cross-frequency coupling detector (phase-amplitude coupling comodulogram w modulation index), spike detection threshold editor w refractory period setting and waveform template matching, spike sorting interface (pca feature space scatter plot w cluster boundaries, template waveform overlay, isi histogram, auto-merge/split clusters), continuous wavelet transform scalogram w ridge extraction, real-time signal quality impedance monitor per electrode w color-coded pass/warn/fail thresholds (green<5kΩ/yellow<10kΩ/red>10kΩ) — INTRACRANIAL RECORDING MODULE ecog/seeg electrode localization on patient-specific mri-reconstructed cortical mesh, electrode contact visualization as spheres on brain surface (ecog grids/strips) or depth probes (seeg shafts penetrating to target structures), stimulation mapping overlay (motor/language/sensory responses logged per contact w color-coded function), high-frequency oscillation detector (ripples-80-250hz/fast-ripples-250-500hz) w automated marking and rate-per-minute calculator for epileptogenic zone identification, seizure onset zone heatmap from ictal recordings, electrocortical stimulation controller (bipolar/monopolar, current-amplitude/pulse-width/frequency/train-duration/polarity configurable, safety-limits enforced w charge-density-calculator and afterdischarge-detector), cortico-cortical evoked potential (ccep) analyzer w n1/n2 peak measurement and effective connectivity mapping rendered as directed graph on brain model — BCI DECODER SYSTEM motor imagery classifier (left-hand/right-hand/feet/tongue) w real-time csp lda pipeline and confusion matrix display, p300 speller matrix (6x6 character grid w row-column flash highlighting, bayesian classifier w dynamic stopping, words-per-minute counter), ssvep frequency detector (multiple flickering stimuli at different frequencies, cca-based classification, information-transfer-rate calculator), neural cursor control (2d screen cursor driven by decoded motor cortex signals w kalman filter smoothing, click via threshold crossing or dwell time), speech decoder (attempted-speech neural patterns → phoneme classifier → word assembly w language model correction via anthropic, real-time text output w confidence bars per phoneme), emotion state classifier (valence/arousal from frontal-alpha-asymmetry and gamma power, displayed as position on 2d emotion circumplex wheel), attention level monitor (theta/beta ratio w focus score 0-100 and distraction alert), meditation depth tracker (alpha/theta crossover detection w depth staging), sleep stage classifier (wake/n1/n2/n3/rem w hypnogram timeline and automatic epoch scoring matching aasm criteria), fatigue detector (theta burst alpha dropout slow eye movement pattern → drowsiness alert w progressive warning levels), imagined movement trajectory decoder for robotic arm endpoint control (3d position grip force decoded from motor cortex ensemble w recurrent neural network), handwriting decoder (imagined pen strokes → character recognition from motor cortex patterns w sequence-to-sequence model) — NEUROSTIMULATION CONTROLLER transcranial direct current stimulation (tdcs) montage designer (anode/cathode placement on scalp w current flow simulation rendered as vector field on cortical surface using finite element model of head tissues — scalp/skull/csf/gray-matter/white-matter conductivity layers), transcranial magnetic stimulation (tms) coil positioning guide (figure-8/circular coil 3d model w induced electric field hotspot projected onto cortex, motor threshold calibration protocol w mep amplitude tracker), deep brain stimulation (dbs) lead visualization (electrode contacts within subthalamic-nucleus/globus-pallidus/vim-thalamus w volume-of-tissue-activated sphere rendering, impedance monitor, stimulation parameter optimizer w symptom-diary correlation), closed-loop stimulation engine (detect biomarker → trigger stimulation w configurable latency/threshold/refractory, event log w pre/post-stim signal comparison), responsive neurostimulation (rns) seizure detection algorithm tuner (bandpass-energy/line-length/area detector threshold adjustment w sensitivity/specificity tradeoff curve), vagus nerve stimulation (vns) parameter dashboard w duty cycle visualization and heart-rate-variability responder tracking, transcranial focused ultrasound (tfus) targeting interface (acoustic simulation through skull w focus point adjustment on 3d brain w pressure field contour overlay and thermal safety calculator), optogenetics control panel (light wavelength/intensity/pulse-pattern w opsin-expression-region overlay for preclinical research) — NEUROIMAGING FUSION import and overlay: mri t1/t2/flair volumes w slice viewer (axial/sagittal/coronal oblique reformat) and 3d surface reconstruction, fmri bold activation maps thresholded by t-statistic overlaid on anatomical w paradigm timeline, dti fractional-anisotropy/mean-diffusivity scalar maps w tractography seeding from roi, pet/spect tracer uptake maps (fdg-metabolic/amyloid/tau/dopamine-transporter) w suv ratio calculator and asymmetry index, meg sensor-level butterfly plot and source-localized activation on cortex, fnirs channel layout on scalp w oxyhemoglobin/deoxyhemoglobin time-courses and cortical projection, ct for electrode localization co-registered to mri w automated contact detection algorithm, ultrasound b-mode/doppler for transcranial window assessment, all modalities alignable via rigid/affine/nonlinear co-registration w landmark and surface matching — PATIENT MONITORING DASHBOARD vital signs strip (ecg w qt-interval/heart-rate-variability, spo2 pleth waveform, etco2 capnography, arterial-blood-pressure w systolic/diastolic/map, temperature core/peripheral, respiratory rate from impedance), consciousness monitors (bispectral-index/entropy/patient-state-index trend lines), intracranial pressure waveform w mean-icp and cerebral-perfusion-pressure calculation (cpp=map-icp) w lundberg-wave classifier (a-waves/b-waves/c-waves), brain tissue oxygenation (pbto2) trend w ischemic threshold alerts, cerebral blood flow monitor (thermal-diffusion/laser-doppler), microdialysis metabolite trends (glucose/lactate/pyruvate/glutamate/glycerol) w lactate-pyruvate-ratio alarm, multimodal trending panel (all parameters time-aligned on shared timeline w event markers for medications/interventions/clinical-notes), alarm management system w configurable thresholds per parameter and escalation tiers (advisory→warning→critical w distinct audio tones) — COGNITIVE ASSESSMENT SUITE automated neuropsych test battery: reaction time (simple/choice/go-no-go), n-back working memory (1-back through 4-back w adaptive difficulty), trail making test (a b variants w path visualization and time/error tracking), digit span (forward/backward/sequencing), stroop test (congruent/incongruent w interference score), flanker task (congruent/incongruent w conflict adaptation), iowa gambling task w deck selection history and net score curve, tower of london planning task w move-count optimizer, continuous performance test w omission/commission error rates and d-prime sensitivity, wisconsin card sort w perseverative error ratio, verbal fluency timer w ai transcription scoring via anthropic, clock drawing test w ai analysis of spatial accuracy from canvas input, all tests generating standardized z-scores benchmarked against age/education normative databases, longitudinal tracking w session-over-session trend charts and decline-detection alerts, ai-generated comprehensive neuropsych report summarizing performance patterns and suggesting clinical correlates via anthropic — RESEARCH & EXPERIMENTAL DESIGN stimulus presentation engine (visual/auditory/tactile timing w sub-millisecond precision scheduling via requestanimationframe web audio scheduling), paradigm builder (block/event-related/mixed design w isi/iti/jitter configuration and condition randomization/counterbalancing), trigger/event-marker system synced to neural recording (ttl-pulse-equivalent timestamp logging), online experiment monitor (trial-by-trial performance, running accuracy/rt, abort-if-criteria-not-met), data export (edf /bdf/gdf/mne-python-compatible/bids-formatted w metadata json sidecars), analysis script generator (ai produces python/matlab analysis pipeline code from natural language experiment description via anthropic), statistical module (parametric/nonparametric tests, cluster-based permutation testing for eeg topographic effects, mixed-effects models for repeated measures, bayesian estimation w credible intervals, multiple comparison correction fdr/bonferroni), publication figure generator (journal-quality svg erp waveforms/topomaps/spectrograms/bar-charts w apa-formatted labels and export at 300dpi) — NEUROPROSTHETICS INTERFACE robotic arm control panel (6-dof endpoint position gripper calibration w decoded-vs-intended trajectory overlay), exoskeleton gait controller (hip/knee/ankle joint angle decoded from motor cortex w gait phase state machine: stance/swing/heel-strike/toe-off and balance perturbation compensator), cochlear implant mapping interface (electrode-to-frequency assignment, threshold/comfort-level per channel, virtual-channel current steering visualization), retinal prosthesis phosphene map editor (electrode grid → perceived phosphene location/size/brightness mapping w camera-to-stimulation image processing pipeline preview), speech synthesizer output (decoded phonemes → articulatory synthesis w prosody control for pitch/rate/volume, voice identity selector), smart wheelchair navigation (decoded direction intent → obstacle avoidance path planning w lidar overlay on room map), bladder/bowel neuroprosthesis controller (sacral nerve stimulation timing w intravesical pressure feedback), functional electrical stimulation (fes) sequencer for paralyzed limb movement restoration (muscle group activation pattern timeline editor w fatigue-compensating intensity ramp) — AI NEURAL COPILOT always-on ai assistant via anthropic streaming: "explain this eeg pattern" → annotates waveform w differential diagnosis, "what's causing this artifact" → highlights source and suggests filter, "is this a seizure" → runs automated seizure detection and compares to learned patient baseline, "optimize my bci accuracy" → analyzes confusion matrix and suggests feature/channel modifications, "summarize today's session" → generates clinical note w key findings/metrics/recommendations, "predict seizure risk" → runs pretrained forecasting model on recent interictal features and outputs probability timeline, "compare this to last week" → overlays longitudinal metric trends, natural language query interface for database ("show all sessions where gamma power in left temporal exceeded threshold during speech task"), conversational onboarding that adapts interface complexity to user role (neurosurgeon/neurologist/researcher/technician/patient/caregiver) — UI FRAMEWORK primary layout: left panel = 3d brain (rotatable/zoomable), center = signal traces (scrollable/scalable), right = controls/parameters/analysis, bottom = timeline scrubber w event markers, all panels draggable/dockable/resizable/detachable-to-second-monitor, theme presets (surgical-theater-dark-w-green-accent/research-lab-light-w-blue-accent/patient-friendly-warm-w-large-fonts/high-contrast-accessibility), waveform color schemes (classic-black-bg-w-colored-traces/publication-white-bg-w-black-traces/colorblind-safe-palette), annotation system (click any timepoint on any signal to add timestamped note w category tag: seizure/artifact/stimulus/medication/clinical-event), session recording w full-state replay (rewind to any moment and see exact brain visualization signals cursor position), undo/redo w 200-step history, keyboard shortcut system (space=pause/play, scroll=gain, arrows=navigate-time, number-keys=montage-presets), touch-optimized mode for intraoperative tablet use w large buttons and swipe gestures, print-ready report generator compiling session summary/screenshots/metrics/ai-notes into formatted pdf, data encrypted at rest (aes-256) and in transit (tls 1.3), role-based access control (admin/clinician/researcher/readonly), hipaa-compliant audit logging w access trail per patient record, session autosave every 30 seconds to sqlite w point-in-time recovery, 100% csrf/xss/sqli hardened
3
12
1,837

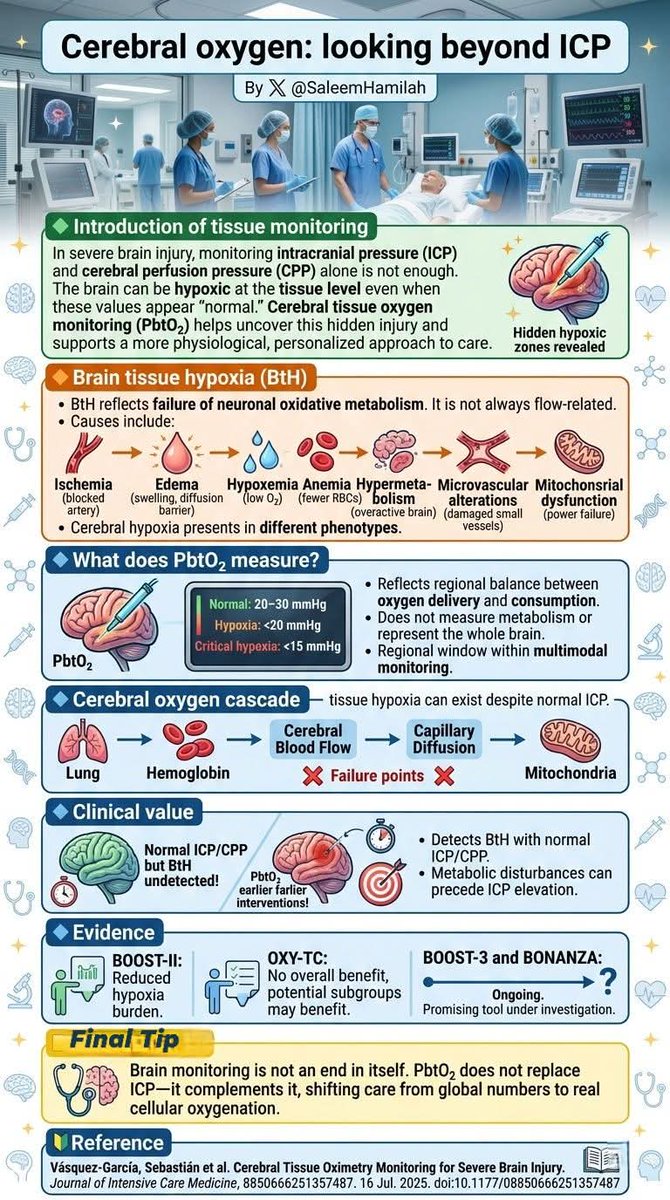
🟩Cerebral oxygen: looking beyond ICP
🟨TIP
Brain monitoring is not an end in itself. PbtO₂ does not replace ICP—it complements it, shifting care from global numbers to real cellular oxygenation.
⸻
🔰 Saleem N. Hamilah 🫁
⸻
#NeurocriticalCare #BrainOxygenation #PbtO2
8
37
965

Feb 14
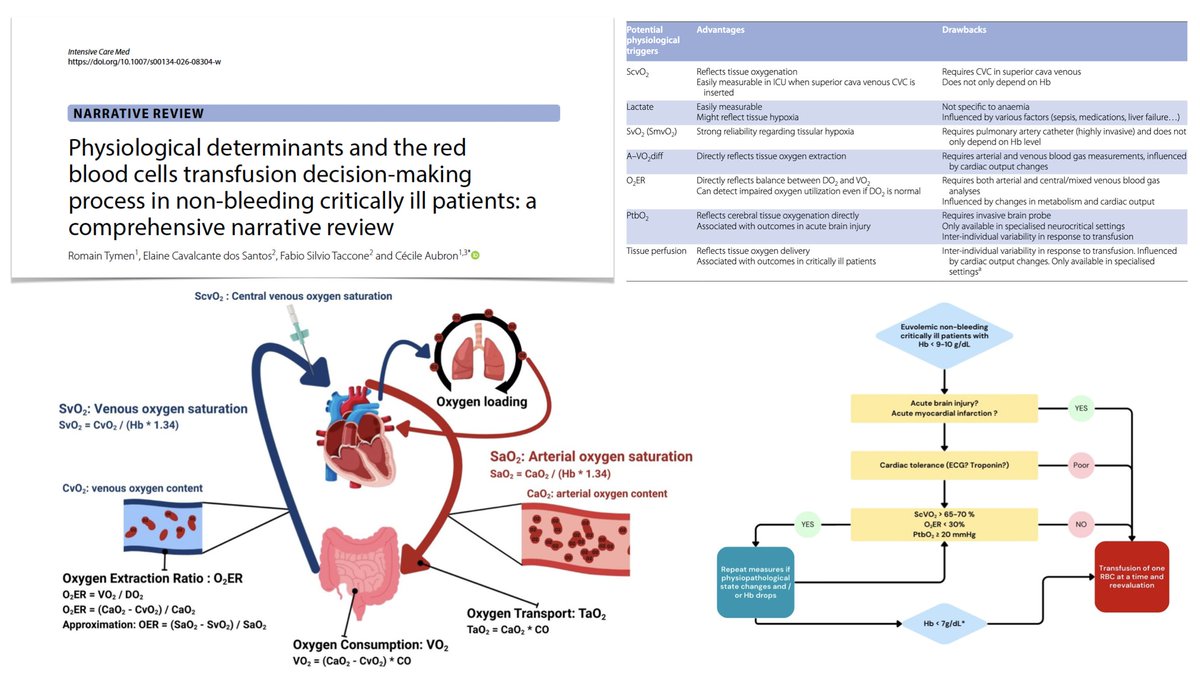
Physiological determinants and red blood cells transfusion decision making process in non bleeding critically ill patients, comprehensive narrative review
🩸 O2 transport/consumption, and adaptation mechanisms to a drop in Hb
🩸 why should RBC transfusion not be based only on Hb in critically ill patients?
🩺 clinical evidence supporting use of physiological triggers for RBC transfusion: ScvO2, artero–venous O2 difference, O2ER, arterial lactate, troponin, tissue perfusion, PbtO2
#FOAMcc
🔓 rdcu.be/e31QP
28
110
7,916

21 Nov 2025
A solid cohort study of 56 poor-grade #SAH patients undergoing brain MMM w/ 1-yr follow-up.
Lower PRx and lactate-pyruvate rations = better 1-yr outcomes.
Interestingly higher PbtO2 did not correlate w/ outcome.
Remember: 20% of DCI is clinically silent, and this occurs exclusively in poor grades. How else to know when to pump up CPP and CO?
svn.bmj.com/content/early/20…
4
7
1,192

7 Nov 2025
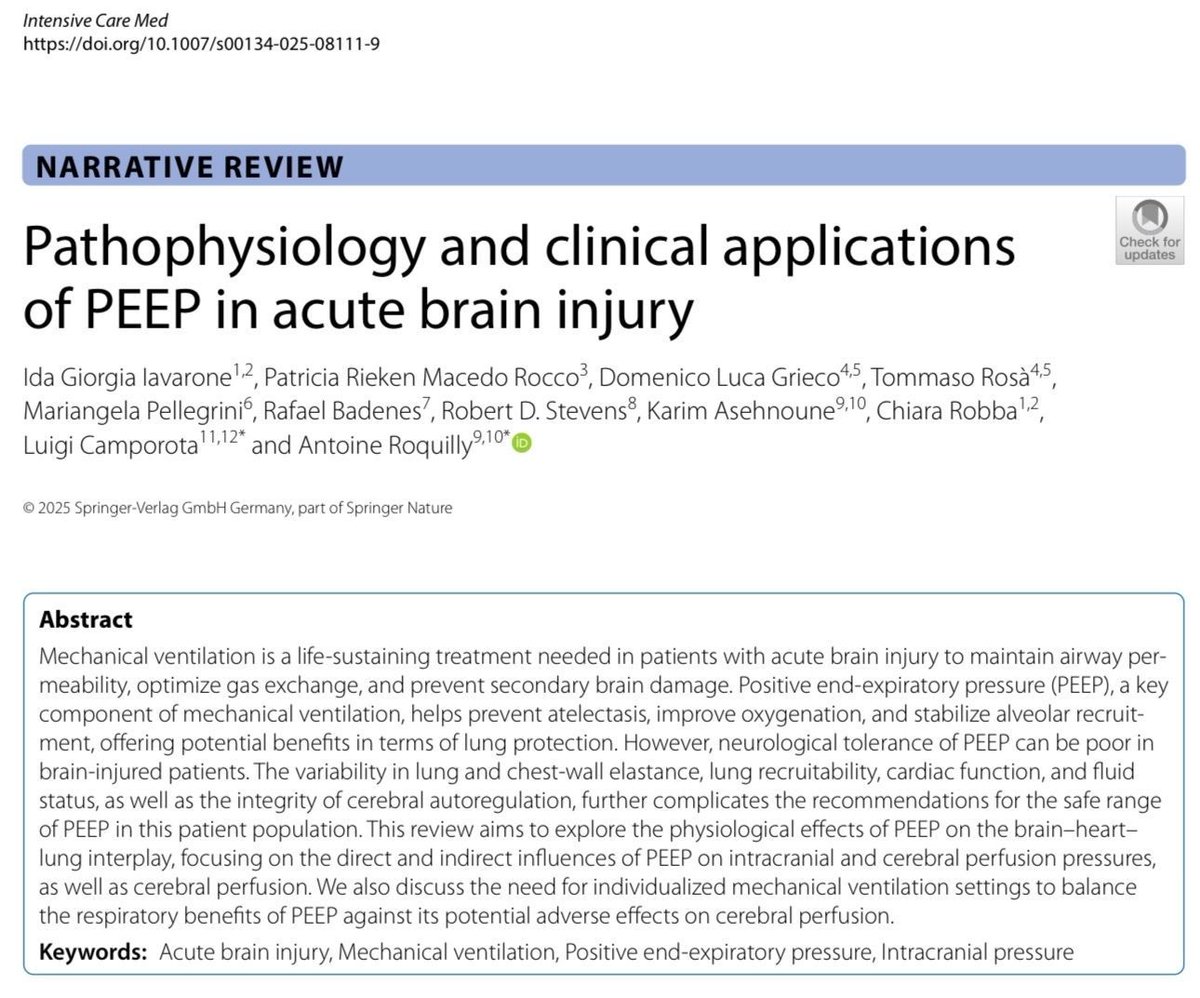
🧠💨 𝗣𝗘𝗘𝗣 𝗲𝗻 𝗹𝗲𝘀𝗶𝗼́𝗻 𝗰𝗲𝗿𝗲𝗯𝗿𝗮𝗹 𝗮𝗴𝘂𝗱𝗮 (𝗟𝗖𝗔)💥
@Springer_Med @ClinMedJournals @yourICM
👇🏼👇🏼👇🏼👇🏼
📑🔗🔑🔓
t.me/ClubCrit
⬇️⬇️⬇️⬇️
🧵👇
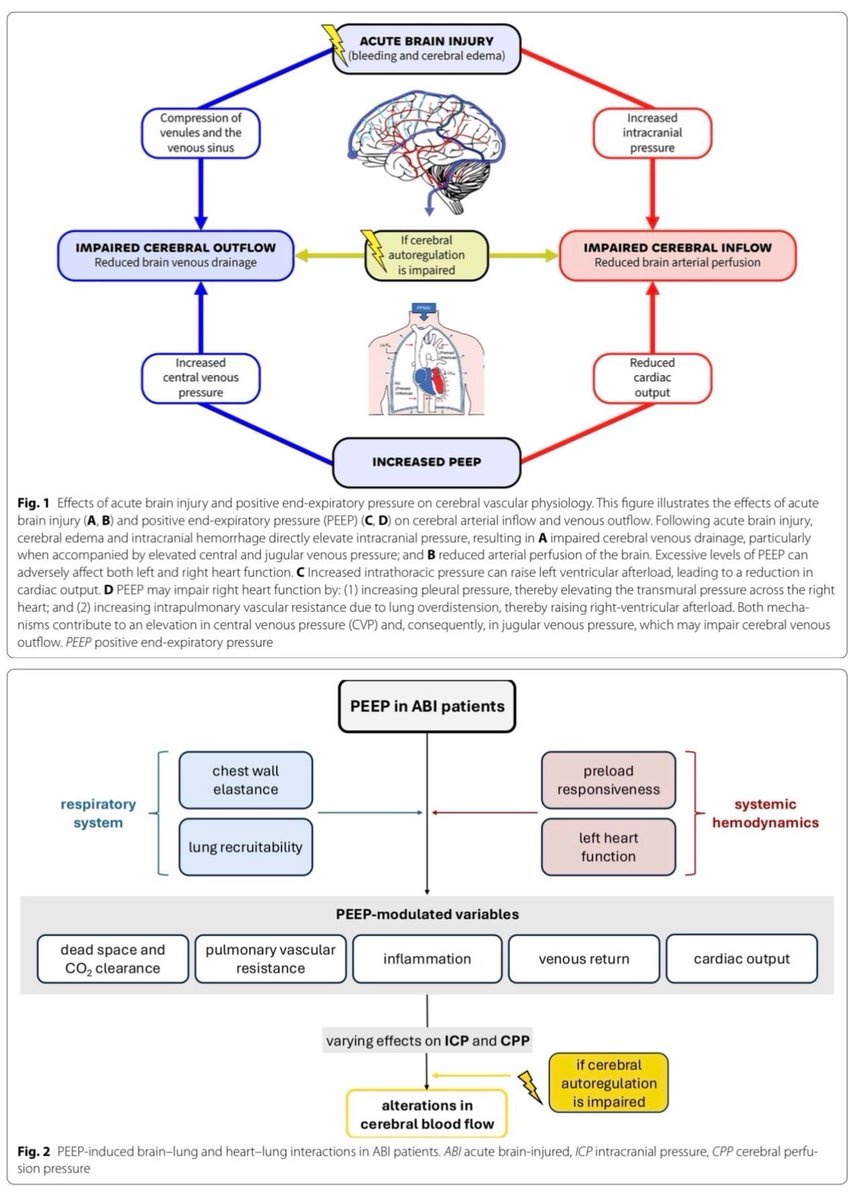
‼️Clave para oxigenar el pulmón, pero puede alterar 𝙋𝙄𝘾/𝙋𝙋𝘾. La respuesta es 𝙝𝙚𝙩𝙚𝙧𝙤𝙜𝙚́𝙣𝙚𝙖 → ¡individualizar!
⚙️ El efecto “neto” de la PEEP = 𝙗𝙚𝙣𝙚𝙛𝙞𝙘𝙞𝙤 𝙧𝙚𝙨𝙥𝙞𝙧𝙖𝙩𝙤𝙧𝙞𝙤 (reclutamiento, mejor V/Q) 𝙢𝙚𝙣𝙤𝙨 costo hemodinámico/venoso (↑PIC/↓PPC).
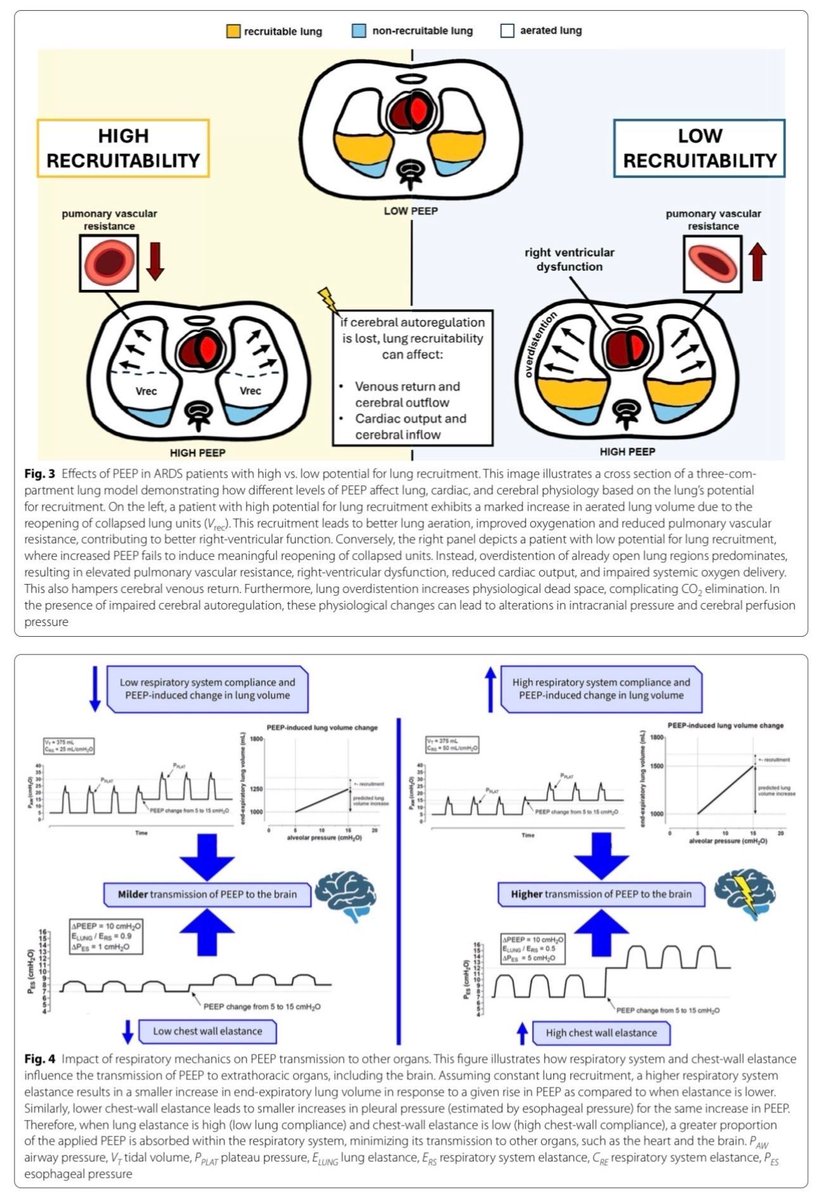
🧱 𝙀𝙡𝙖𝙨𝙩𝙖𝙣𝙘𝙞𝙖 𝙙𝙚 𝙥𝙖𝙧𝙚𝙙 𝙩𝙤𝙧𝙖́𝙘𝙞𝙘𝙖 y 𝙧𝙚𝙘𝙡𝙪𝙩𝙖𝙗𝙞𝙡𝙞𝙙𝙖𝙙 determinan cuánta presión llega al cráneo. Alta elastancia = ↑riesgo de ↑PIC con PEEP.
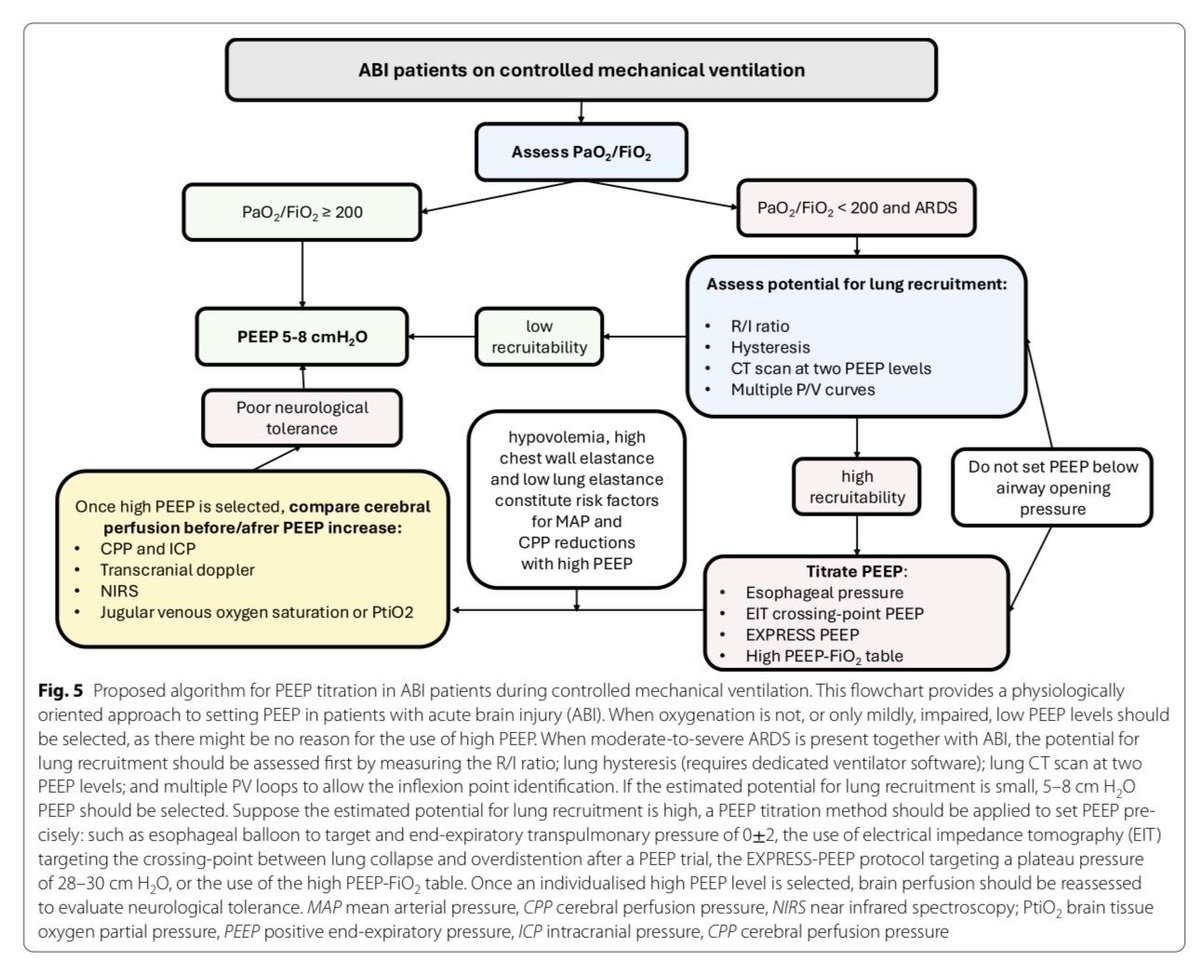
🫁 En 𝙇𝘾𝘼 𝙎𝘿𝙍𝘼 (~25%) puede requerirse PEEP alta, pero 𝙨𝙤́𝙡𝙤 si se preserva 𝙋𝙋𝘾 y mejora 𝙋𝙗𝙩𝙊₂.
🔬 Evidencia clínica: PEEP puede ↑PIC si compromete el drenaje venoso o ↓GC; pero 𝙧𝙚𝙘𝙡𝙪𝙩𝙖𝙢𝙞𝙚𝙣𝙩𝙤 𝙪́𝙩𝙞𝙡 puede ↑PbtO₂.
🛰️ 𝙇𝙐𝙎 ayuda a distinguir reclutamiento vs hiperinflación y se correlaciona con cambios de 𝙋𝙄𝘾 durante ajustes de PEEP.
🧪 𝙋𝙧𝙤𝙩𝙤𝙘𝙤𝙡𝙤 𝙥𝙧𝙖́𝙘𝙩𝙞𝙘𝙤: suba PEEP en 𝙥𝙖𝙨𝙤𝙨 𝙙𝙚 2–3; revalúe 𝙎𝙖𝙊₂/𝙋𝙖𝙊₂, 𝙇𝙐𝙎, 𝙋𝙄𝘾/𝙋𝙋𝘾, 𝙋𝙗𝙩𝙊₂ 𝙮 𝙏𝘼 𝙢𝙚𝙙𝙞𝙖/𝙂𝘾. Mantenga si gana pulmón y tolera el cráneo.
🧠 Si ↑𝙋𝙄𝘾 sostenida o ↓𝙋𝙋𝘾 sin ganancia respiratoria → 𝙗𝙖𝙟𝙚 𝙋𝙀𝙀𝙋 y optimice hemodinamia (pre/poscarga, VD).
🔁 En obesidad/HTIA/alta elastancia torácica: ajuste 𝙢𝙖́𝙨 𝙡𝙚𝙣𝙩𝙤 y monitorice estrechamente; son quienes más “transmiten” presión.
🧩 𝘾𝙤𝙣𝙘𝙡𝙪𝙨𝙞𝙤́𝙣: No hay PEEP universal. En LCA, la 𝙫𝙚𝙣𝙩𝙞𝙡𝙖𝙘𝙞𝙤́𝙣 𝙘𝙚𝙧𝙚𝙗𝙧𝙤-𝙥𝙧𝙤𝙩𝙚𝙘𝙩𝙞𝙫𝙖 requiere 𝙋𝙀𝙀𝙋 𝙥𝙚𝙧𝙨𝙤𝙣𝙖𝙡𝙞𝙯𝙖𝙙𝙖 con monitorización pulmonar, cerebral y sistémica integrada.
📚📖 Más en el blog #ClubCrit 👉 [buff.ly/uS9NzRw]
#ClubCrit #NeuroCritCare #BrainLungBalance #Perfusión #PIC #PPC #PbtO2 #NeuroUCI #Individualización #POCUS #VExUS #MedTwitter #CritCare #UCI #ICU #CriticalCare #Diagnóstico #icu #intensivecare #diagnosis #management #Riesgo #UCI #Tratamiento #sonologist #MedicinaBasadaEnEvidencia #Terapia #MedEd #Medicina #Emergencias #FOAMed #FOAMcc #CriticalCare #CuidadoCrítico #MedX #IntensiveCare #EducaciónMédica #MedIntensiva #MedXCommunity #MedicinaCrítica #MedED #CritCare #ICUmanagement #MustRead #LecturaRecomendada
26
89
3,933
23 Apr 2025
🧠💥𝗔𝗰𝘁𝘂𝗮𝗹𝗶𝘇𝗮𝗰𝗶𝗼́𝗻: 𝗧𝗿𝗮𝘂𝗺𝗮𝘁𝗶𝘀𝗺𝗼 𝗖𝗿𝗮𝗻𝗲𝗼𝗲𝗻𝗰𝗲𝗳𝗮́𝗹𝗶𝗰𝗼 𝗚𝗿𝗮𝘃𝗲 𝗲𝗻 𝗹𝗮 𝗨𝗖𝗜💥🧠
@CO_Anesthesiol
👇🏼👇🏼👇🏼👇🏼👇🏼
📑🔗🔑🔓
t.me/ClubCrit
Menos protocolo, más personalización.
Te resumo las claves clínicas y fisiopatológicas que todo intensivista debe saber.
⬇️⬇️⬇️
🧠🔢𝗚𝗹𝗮𝘀𝗴𝗼𝘄 𝗲𝘀 𝘀𝗼𝗹𝗼 𝗲𝗹 𝗰𝗼𝗺𝗶𝗲𝗻𝘇𝗼.
✔️ Modelos como CBI-M integran clínica, sangre e imagen
✔️ Pupilometría cuantitativa > examen pupilar clásico
➡️ 𝘼𝙣𝙩𝙞𝙘𝙞𝙥𝙖 𝙝𝙞𝙥𝙚𝙧𝙩𝙚𝙣𝙨𝙞𝙤́𝙣 𝙚𝙣𝙙𝙤𝙘𝙧𝙖𝙣𝙚𝙖𝙣𝙖
🧠🔺𝗣𝗜𝗖 𝘀𝗶𝗴𝘂𝗲 𝘀𝗶𝗲𝗻𝗱𝗼 𝗲𝗹 𝗲𝗷𝗲.
✔️ GCS ≤8 TC con lesión estructural = indicación formal
✔️ PbtO₂ suma información, pero su impacto es aún debatido
➡️ 𝘿𝙪𝙖𝙡 𝙢𝙤𝙣𝙞𝙩𝙤𝙧𝙞𝙣𝙜 𝙚𝙣 𝙘𝙖𝙨𝙤𝙨 𝙨𝙚𝙡𝙚𝙘𝙘𝙞𝙤𝙣𝙖𝙙𝙤𝙨
🧠🔁𝗖𝗣𝗣 𝗼́𝗽𝘁𝗶𝗺𝗮 𝗽𝗲𝗿𝘀𝗼𝗻𝗮𝗹𝗶𝘇𝗮𝗱𝗮.
CPP = PAM - PIC
✔️ Ideal: 60–70 mmHg
✔️ Autorregulación: PRx y CPPopt
➡️ 𝘾𝙊𝙂𝙄𝙏𝘼𝙏𝙀 𝙚𝙣 𝙘𝙪𝙧𝙨𝙤
🧠💉𝗕𝗶𝗼𝗺𝗮𝗿𝗰𝗮𝗱𝗼𝗿𝗲𝘀 𝘆𝗮 𝘀𝗼𝗻 𝗽𝗮𝗿𝘁𝗲 𝗱𝗲𝗹 𝗺𝗮𝗻𝗲𝗷𝗼.
🧬 GFAP, UCH-L1, NFL
➡️ Evaluación seriada
➡️ Ayuda pronóstica incluso con sedación profunda
🧠🩸𝗧𝗿𝗮𝗻𝘀𝗳𝘂𝘀𝗶𝗼́𝗻:
📌 Hb objetivo: >9 g/dL
✔️ Mejores desenlaces funcionales
✔️ Evidencia: HEMOTION, TRAIN
🧠💧𝗙𝗹𝘂𝗶𝗱𝗼𝘀:
✔️ Balance hídrico neutro
✔️ Monitorización avanzada en pacientes inestables
❗ 𝙃𝙞𝙥𝙤𝙫𝙤𝙡𝙚𝙢𝙞𝙖 𝙚 𝙝𝙞𝙥𝙚𝙧𝙫𝙤𝙡𝙚𝙢𝙞𝙖 𝙚𝙢𝙥𝙚𝙤𝙧𝙖𝙣 𝙚𝙙𝙚𝙢𝙖 𝙘𝙚𝙧𝙚𝙗𝙧𝙖𝙡
🧠🎛️𝗩𝗲𝗻𝘁𝗶𝗹𝗮𝗰𝗶𝗼́𝗻 𝗺𝗲𝗰𝗮́𝗻𝗶𝗰𝗮:
✅ Normocapnia (PaCO₂ 35–40 mmHg)
❌ PaCO₂ <32 o >45 → ↑ mortalidad
✔️ Ventilación protectora viable si no hay PIC elevada
🧠⚗️𝗦𝗼𝗹𝘂𝗰𝗶𝗼́𝗻 𝘀𝗮𝗹𝗶𝗻𝗮 𝗵𝗶𝗽𝗲𝗿𝘁𝗼́𝗻𝗶𝗰𝗮 (𝗛𝗧𝗦) 𝘃𝘀 𝗺𝗮𝗻𝗶𝘁𝗼𝗹:
✔️ Eficacia similar
✔️ Menor riesgo de AKI con HTS
➡️ 𝙃𝙏𝙎 𝙥𝙧𝙚𝙛𝙚𝙧𝙞𝙙𝙤 𝙚𝙣 𝙢𝙪𝙘𝙝𝙤𝙨 𝙘𝙚𝙣𝙩𝙧𝙤𝙨
🧠🌡️𝗧𝗲𝗺𝗽𝗲𝗿𝗮𝘁𝘂𝗿𝗮 𝘆 𝘀𝗲𝗱𝗮𝗰𝗶𝗼́𝗻:
✔️ T° ideal: 36–37.5 °C
✔️ Evitar fiebre: neurotóxica
✔️ Sedación dirigida
➡️ 𝘿𝙚𝙭𝙢𝙚𝙙𝙚𝙩𝙤𝙢𝙞𝙙𝙞𝙣𝙖 𝙢𝙪𝙚𝙨𝙩𝙧𝙖 𝙢𝙚𝙟𝙤𝙧𝙚𝙨 𝙙𝙚𝙨𝙚𝙣𝙡𝙖𝙘𝙚𝙨
🧠💊𝗕𝗮𝗿𝗯𝗶𝘁𝘂́𝗿𝗶𝗰𝗼𝘀:
Última línea para PIC refractaria
✔️ Solo si respuesta efectiva
❌ Altos efectos secundarios
🧠👨🏻💻𝗧𝗲𝗰𝗻𝗼𝗹𝗼𝗴𝗶́𝗮 𝗲𝗻 𝟮𝟬𝟮𝟱:
➡️ Dashboards predictivos
➡️ IA para anticipar PIC elevada
➡️ Neurocrítica basada en aprendizaje automático
✳️¿𝗤𝘂𝗲́ 𝗵𝗮𝗰𝗲𝗿 𝗵𝗼𝘆?
✔️ Monitorización individual
✔️ Biomarcadores imagen clínica
✔️ Ajustes dinámicos de CPP, fluidos y oxigenación
➡️ 𝙀𝙡 𝙥𝙖𝙘𝙞𝙚𝙣𝙩𝙚 𝙙𝙚𝙛𝙞𝙣𝙚 𝙚𝙡 𝙥𝙧𝙤𝙩𝙤𝙘𝙤𝙡𝙤
📖Resumen ampliado en el blog #ClubCrit
👉 [buff.ly/8b51wfX]
#neurocritcare #UCI #TraumaCraneal #TBI #ICU #Neurocriticalcare #PIC #CPP #PbtO2 #FOAMed #FOAMcc #MedEd #MedTwitter #EducaciónMédica #HemodinámicaCerebral #OxigenaciónCerebral #Osmoterapia #Neuroprotección #NeuroIA #MedicinaDelFuturo #neurology #neurocritical #neurosurgery #neurotwitter #NeuroX

1
50
122
5,967

10 Feb 2025
➡️Manejo de Neurotrauma🧠🩸 y Presión Intracraneal💥💥💥💥
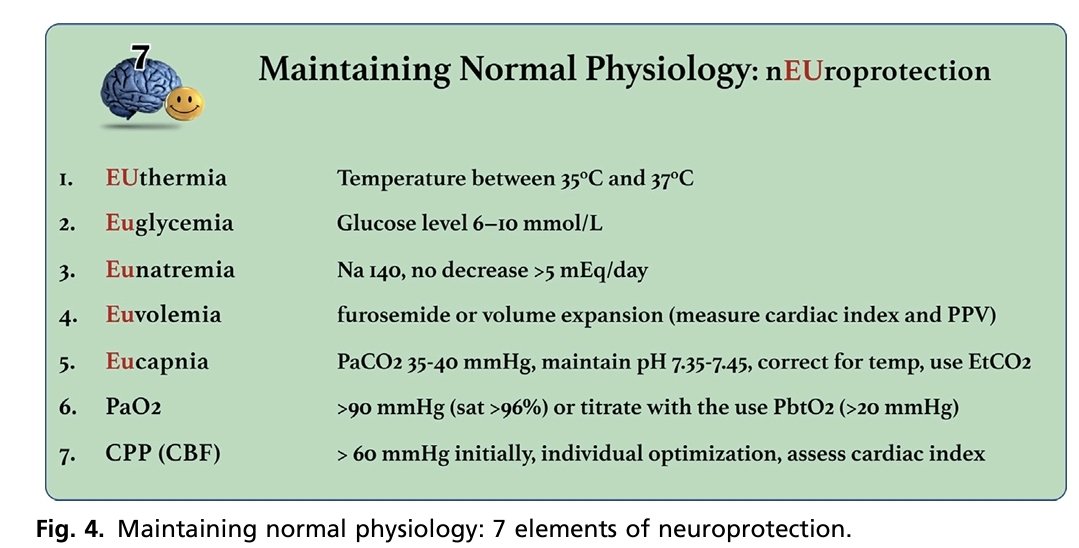
NEUROPROTECCIÓN: MANTENER EL CEREBRO FELIZ 😊
🟣El manejo de un cerebro lesionado 🩸🧠debe centrarse en mantener la homeostasis normal.
💥7 elementos del concepto de "cerebro feliz":
1️⃣EUtermia.35°C y 37°C
2️⃣EUglucemia. Nivel de glucosa 6-10 mmol/L
3️⃣EUnatremia Na 140, sin disminución >5 mEq/día
4️⃣ EUvolemia.Furosemida o expansión de volumen (medir el índice cardíaco y el VPP)
5️⃣EUcapnia.PaCO2 35-40 mmHg, mantener pH 7,35-7,45, corregir según temperatura, utilizar EtCO2.
6️⃣oxigenación normal PaO2: >90 mmHg (sat >96%) o titular con el uso de PbtO2 (>20 mmHg)
7️⃣ Presión de perfusión cerebral optimizado. PPC : > 60 mmHg inicialmente, optimización individual, evaluar índice cardíaco
La hiperglucemia puede afectar el resultado de la sin embargo, se debe evitar un control estricto de la glucemia en el TCE ya que la hipoglucemia cerebral también es perjudicial.
👇🏽👇🏽👇🏽👇🏽
pubmed.ncbi.nlm.nih.gov/3633…
🔏
acrobat.adobe.com/link/revie…

69
173
5,751

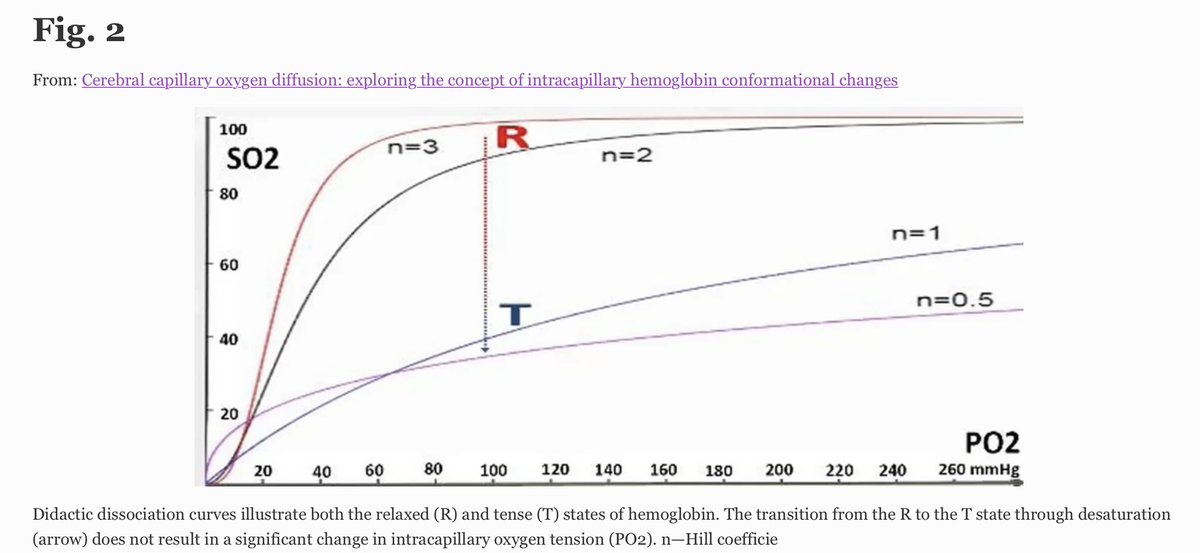
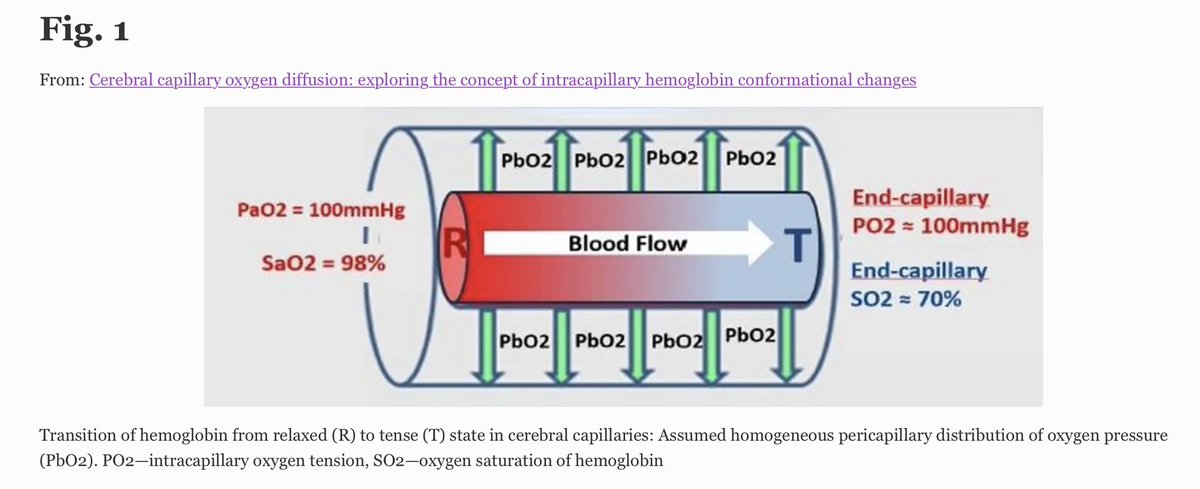
📃HyperO2-induced ⬆️ in 🧠 tissue pO2 (PbtO2) ✔️Circulating models 🔮 a ⬇️ PO2
✔️Hb transition relaxed (R) to tense (T) state, driven by deO2 ➡️ pO2 diff. across 🧠 capillaries.
✅ Hb R to T ➡️ for ⬆️ PbtO2 lvls in 🧠 tissue during hyperO2.
🔓 t.ly/NhIIb
#FOAMed
6
13
1,454



頭蓋内圧モニターを挿入するなら情報は最大限活用したい。波形・脳温・PRx...
できればPbtO2もほしいものです
medicalexpo.com/ja/prod/natu…
integralife.jp/icpmonitoring…
#神経集中治療 #脳神経モニタリング
4
594

14 Oct 2024
#Neurocritical care
✳️ My A to H neuroprotective approach:-
🔹 A B:
Normoxia, normocapnia
🔹C:
SBP > 100 mmHg (50 - 69y),
SBP > 110 mmHg (<50 or > 70y)
🔹D:
ICP < 22mmHg
CPP 60-70mmHg
SjVO2 > 55%
PbtO2 > 18mmHg
Seizure prophylaxis
Normothermia
🔹E:
Na 135 - 145mmol/L
🔹F:
Avoid albumin (SAFE trial)
Avoid BSS (BASICS trial)
🔹G:
BSL 6-10mmol/L
🔹H:
Hb > 80g/L
(HEMOTION trial vs TRAIN RCT)
Please do mention below about your approach..‼️
5
13
65
7,224

29 Aug 2024
Goal of treatment of severe brain injury:
- CPP > 60 mmHg
- ICP ~ 5-15 mmHg
- PbtO2 > 15 mmHg
- SpO2 > 95%
#atls
1
3
337

28 Aug 2024
Seeing the monitors at BNI today triggered memories of working with neurosurgery residents to insert PbtO2 monitors in our TBI patients during fellowship at @UTH_Neurocrit! Good times @HuimahnChoi @drltorres @abhaykjha @rjb1865

1
1
9
460
27 Aug 2024
Our very own Dr. Aditya Kumar has worked diligently to bring PbtO2 monitors to the neuro ICU with @BarrowNeuro neurosurgery residents! Treating TBI, one patient at a time! @BNI_NCC_RMJ @adityagarg42 @C_PatrickCrooks #neuroICU

1
3
15
1,603

5 Jun 2024
重症~中等度のTBIにおいて、PbtO2 ICPモニタリング併用はICPモニタリング単独と比べ、死亡率,機能回復,心血管イベント,敗血症などの転帰に変化を与えないことが示唆され、併用群では肺イベントのリスクが高いことがわかった、というRCTのMA。
PbtO2はless is moreとなるか
pubmed.ncbi.nlm.nih.gov/3881…
4
19
3,031
