Emma Louise Webb. THT retweeted

#HERESHEIS edited this for Red Coat Racheal! #SHOULDADONE 😊
#TIMMYALEXISCARRINGTONWARD was diagnosed with #PROSTATECANCER last October 2025! #TELLINME 😜
We're doing “March for Men” on Saturday 13th June, please donate on the link below! #ISAIDIT 😘
justgiving.com/page/here-she…
2
3
123

Jun 10
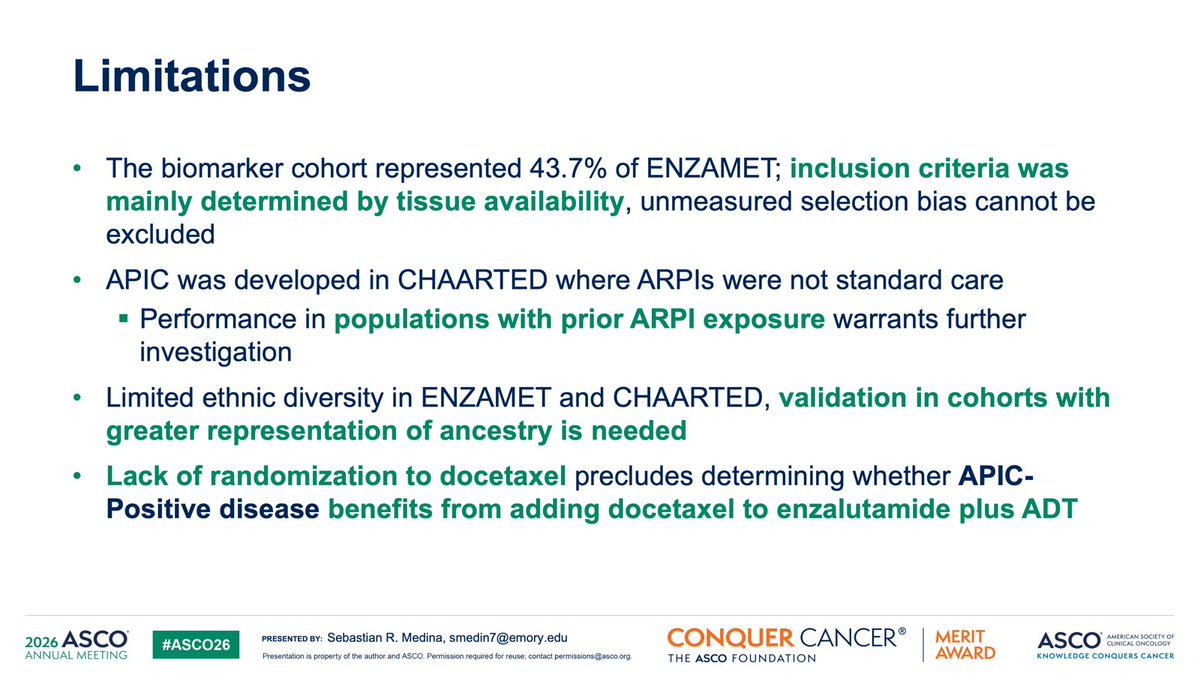
Clinical AI tool that reads a routine H&E slide from diagnosis to identify which mHSPC patients benefit from ARSI enzalutamide. APIC, presented at #ASCO26 from ENZAMET.
APIC was derived in CHAARTED and locked before ENZAMET analysis. Independent validation in 492 patients from the ENZAMET biomarker cohort.
Outcomes:
🎯 APIC-Negative (64%): 18.2% 5-yr OS from enzalutamide
🎯 APIC-Positive (36%): -3.2% 5-yr OS from enzalutamide
Significant treatment-biomarker interaction. Holds in multivariable analysis adjusting for volume, timing, PS, and Gleason. Not explained by docetaxel use.
No special assay or new test. Just a pathology slide you probably already have.
#mHSPC #ProstateCA #GUonc #ASCO26 #AIinMedicine #AIinOncology


2
6
11
835
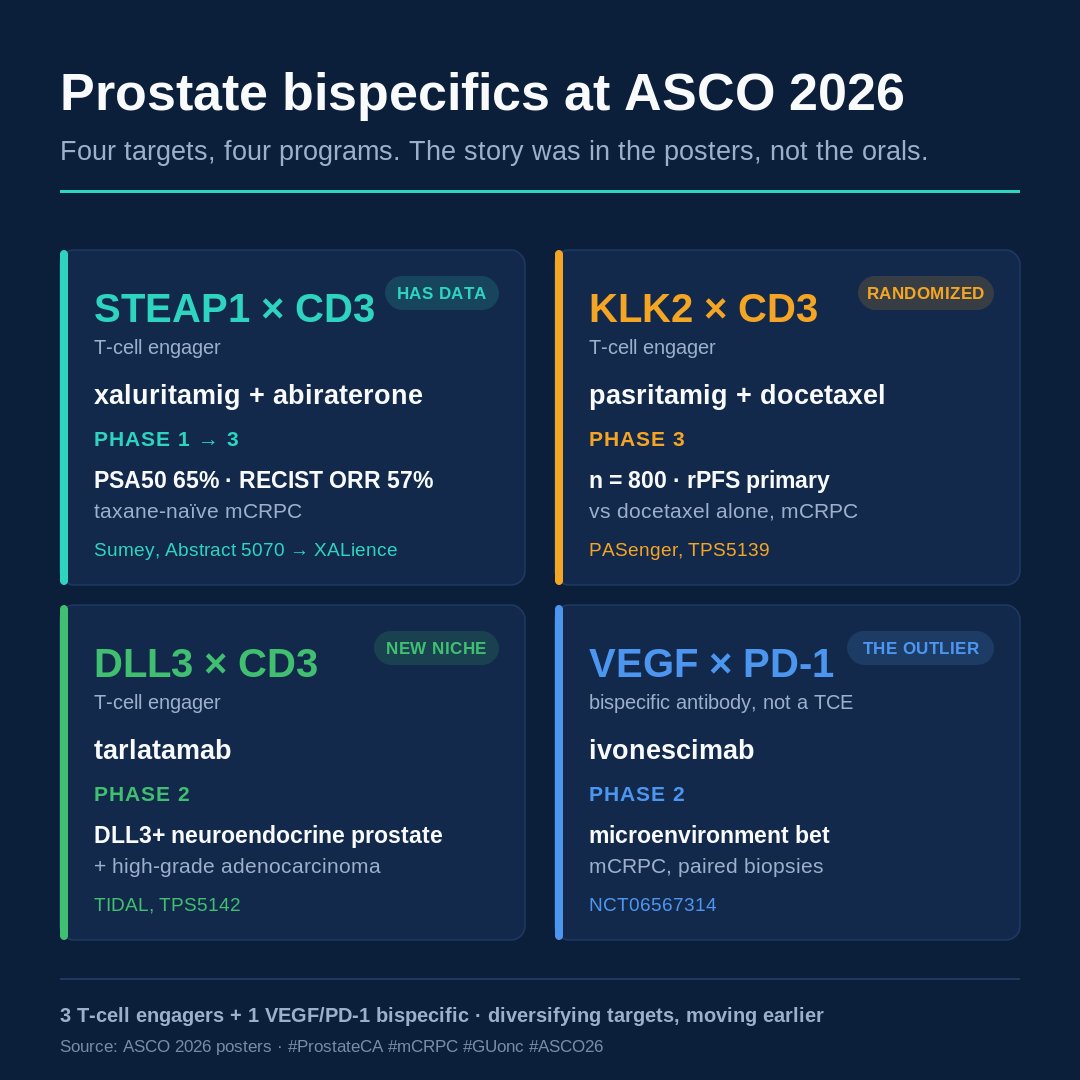
Not many prostate bispecifics in the oral sessions at ASCO this year. Most of the activity was in the posters.
Four programs, four targets:
🔬 STEAP1 × CD3, xaluritamig abiraterone (Sumey, 5070): the only one with efficacy data. PSA50 65%, RECIST ORR 57% in taxane-naïve mCRPC. Inphase 3 XALience.
🔬 KLK2 × CD3, pasritamig docetaxel (PASenger, TPS5139): already in randomized phase 3, n=800, rPFS primary.
🔬 DLL3 × CD3, tarlatamab (TIDAL, TPS5142): phase 2 in DLL3-positive neuroendocrine prostate, a setting with few options.
🔬 VEGF × PD-1, ivonescimab (NCT06567314): not a T-cell engager, testing the microenvironment in mCRPC.
The targets are diversifying (STEAP1, KLK2, and DLL3 each handle prostate specificity differently), and the trials are moving earlier rather than sitting late salvage.
Excited to follow this movement and the idea of an immune based therapy in this typically immune resistant tumor.
#ProstateCA #mCRPC #GUonc #ASCO26 @OncoAlert
1
15
30
2,367
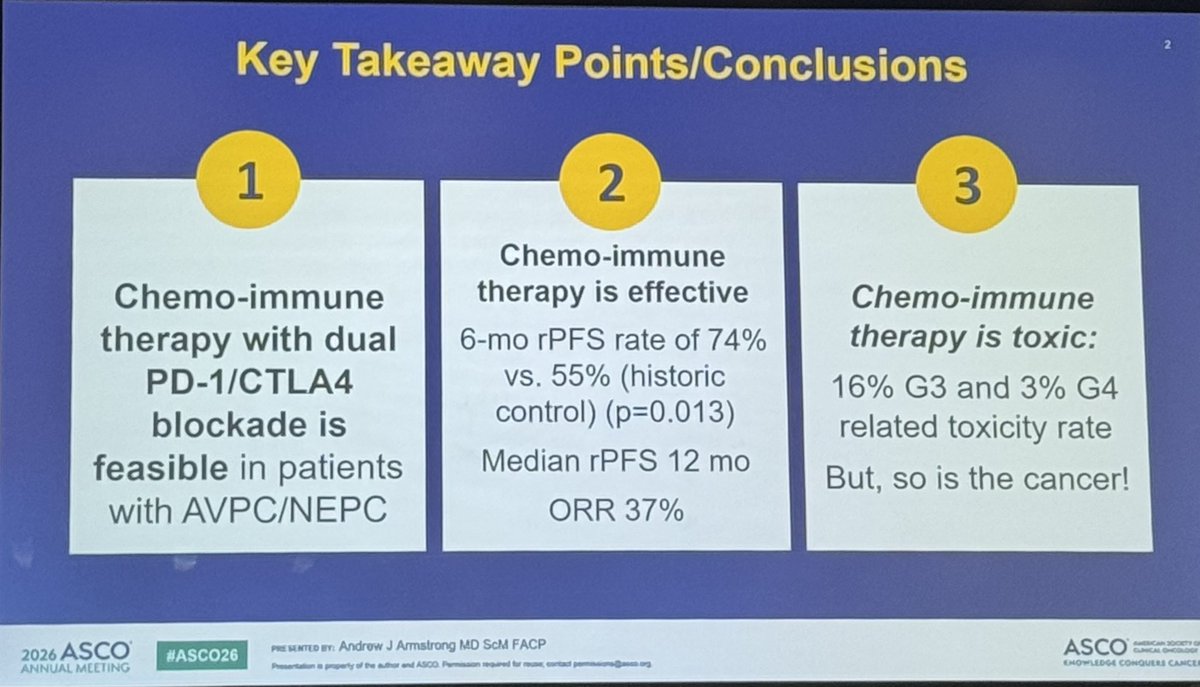
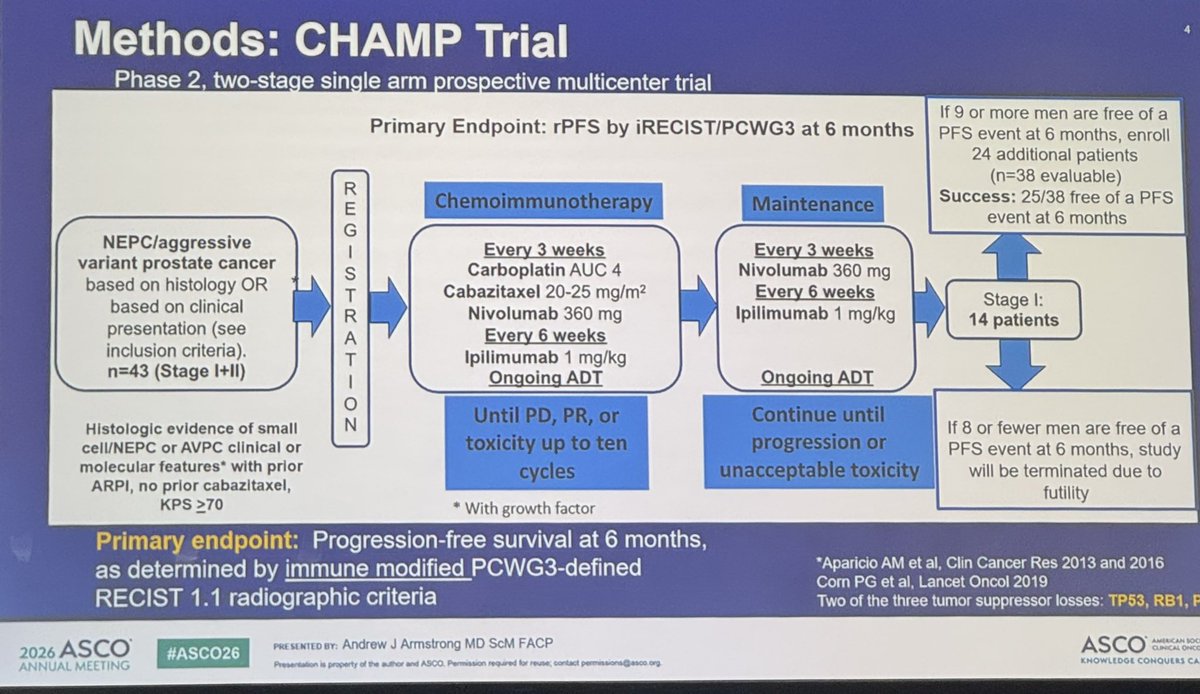
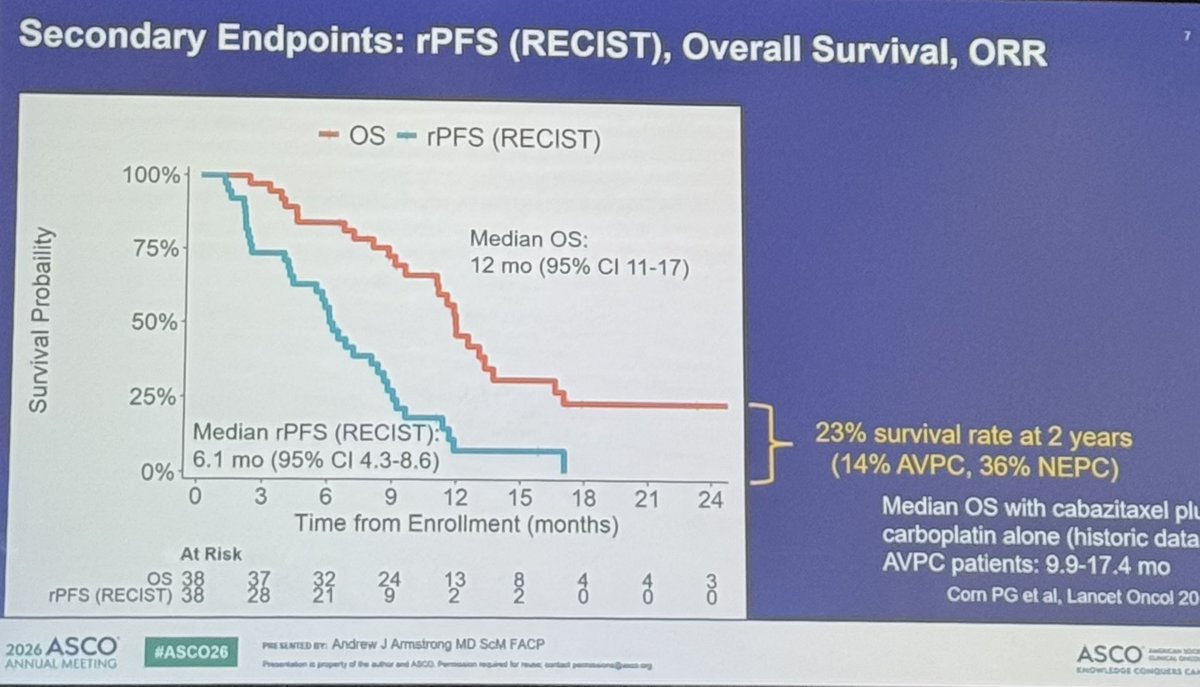
CHAMP met its primary endpoint: 6-month PFS 74% vs 55% historical control, with 23% 2-year survival in a population where platinum-taxane alone rarely gets patients past a year.
The randomization question is the right question. Single-arm with historical comparator is often the only feasible design when you’re enrolling NEPC/AVPC, but it makes regulatory translation hard. A randomized phase 2 would require network coordination and sustained sponsor commitment to a rare, rapidly progressing population. Worth pushing for.
This is the most actionable data we have in this space. Well done to the Duke team.
@AarmstrongDuke @DukeGUCancer
#ProstateCA #GUonc #ASCO26

#CHAMP is an important trial led and presented by @AarmstrongDuke from our @DukeGUCancer team evaluating chemoIO with cabazitaxel/carboplatin and ipilimumab/nivolumab in patients with aggressive variant or neuroendocrine metastatic #ProstateCancer. Maintenance IO continued after up to 10 chemo cycles.
Met primary endpoint of 6 mo PFS 74% vs 55% historic carbo/cabazi with expected but manageable toxicity. 23% survival at 2 years is much better than historical data. Two patients alive and off therapy at 30 months!
Aggressive treatment for aggressive disease, but shows chemoIO should be considered as SOC for these patients with historical poor outcomes.
#ASCO26 @DukeCancer @Daniel_J_George @hannahdzmd @MRHarrisonMD @MattLabsMD @OncoDailyGU @OncoAlert @urotoday @oncodaily
7
7
1,308
May 31
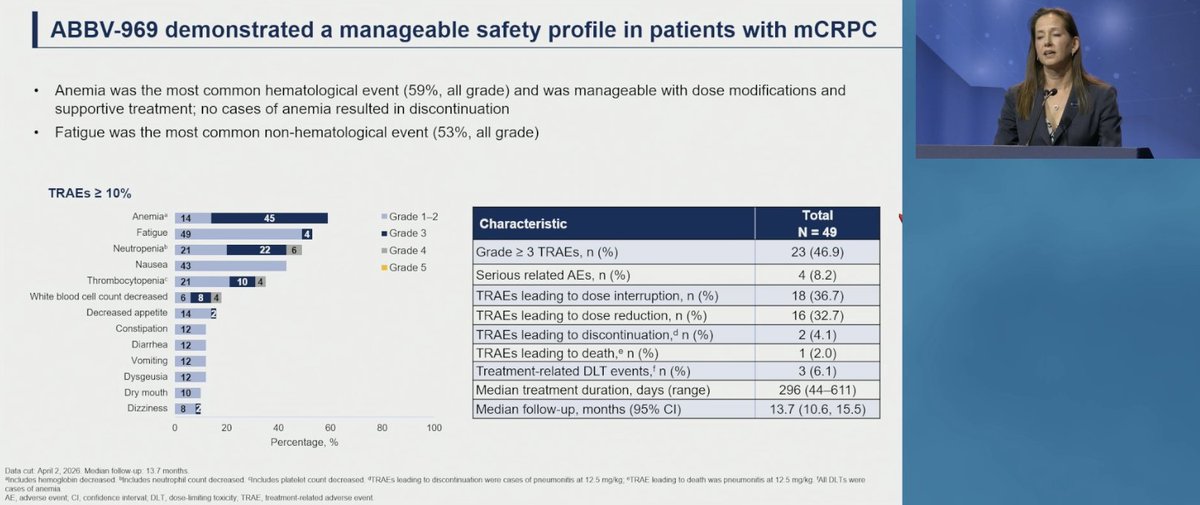
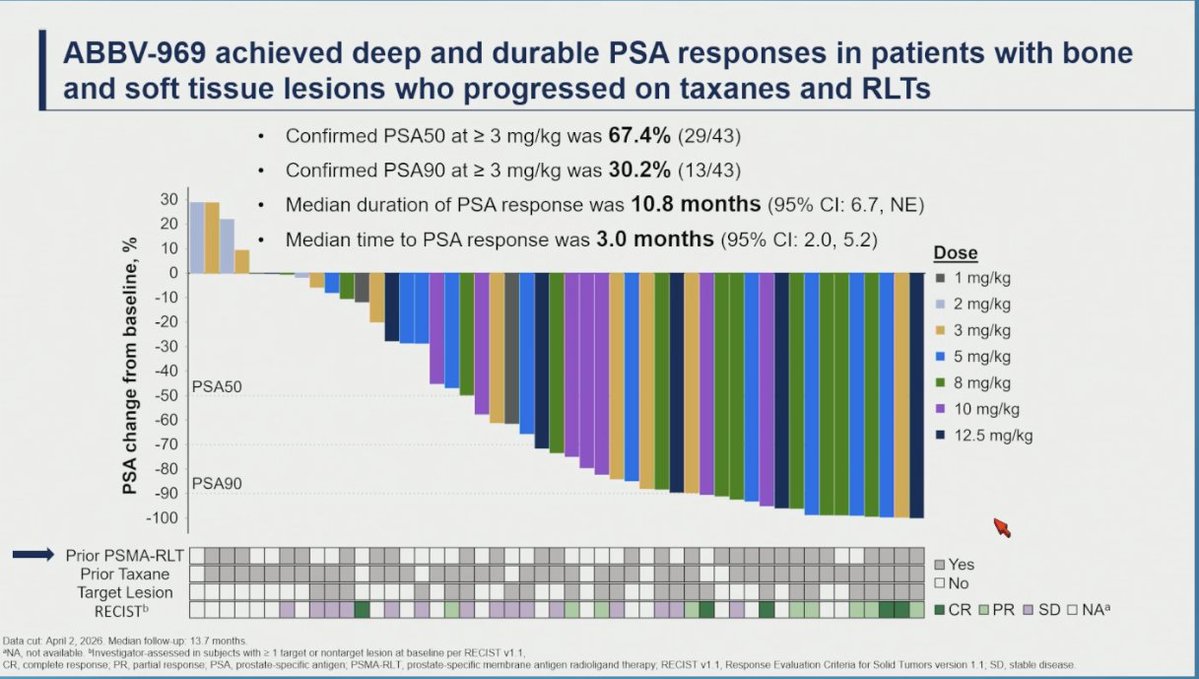
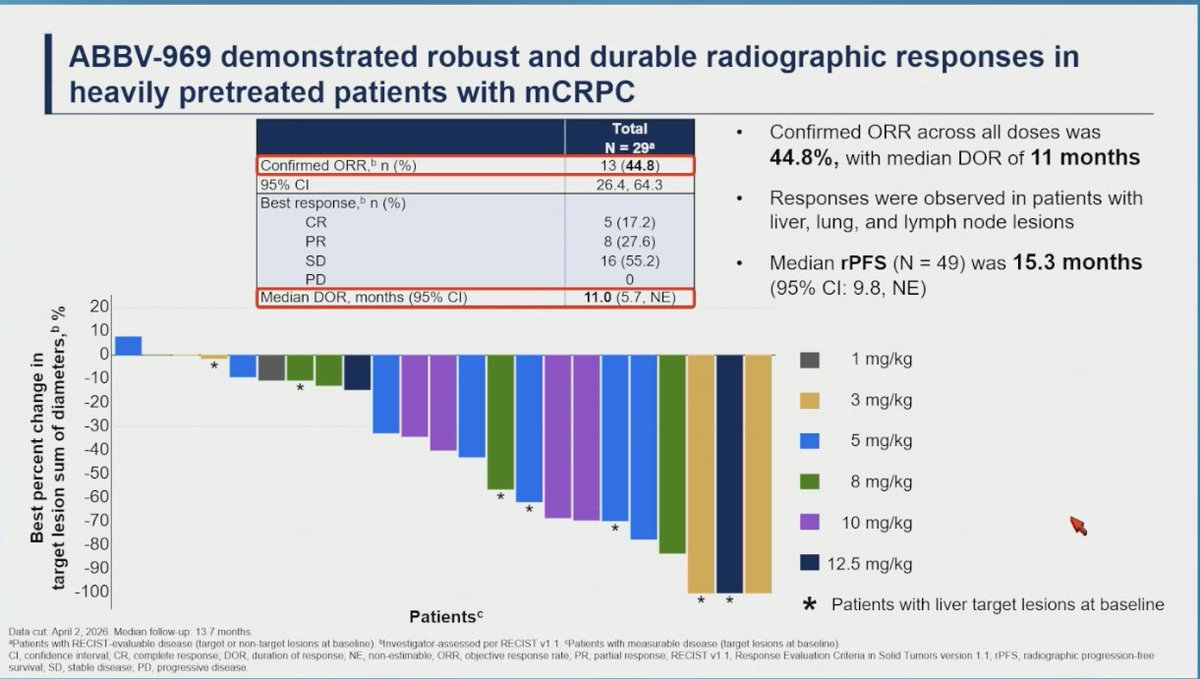
ABBV-969 delivered a median rPFS of 15.3 months (95% CI 9.8, NE) in heavily pretreated mCRPC, in patients who had already progressed on taxanes and/or PSMA radioligand therapy.
First-in-human dose escalation, biomarker-unselected. Median follow-up 13.7 mo.
🎯 Confirmed ORR 44.8%, including 17% CR, median DOR 11.0 mo
🎯 PSA50 67.4% and PSA90 30.2% at doses ≥3 mg/kg, median DoR 10.8 mo
📊 Responses across liver, lung, and nodal lesions
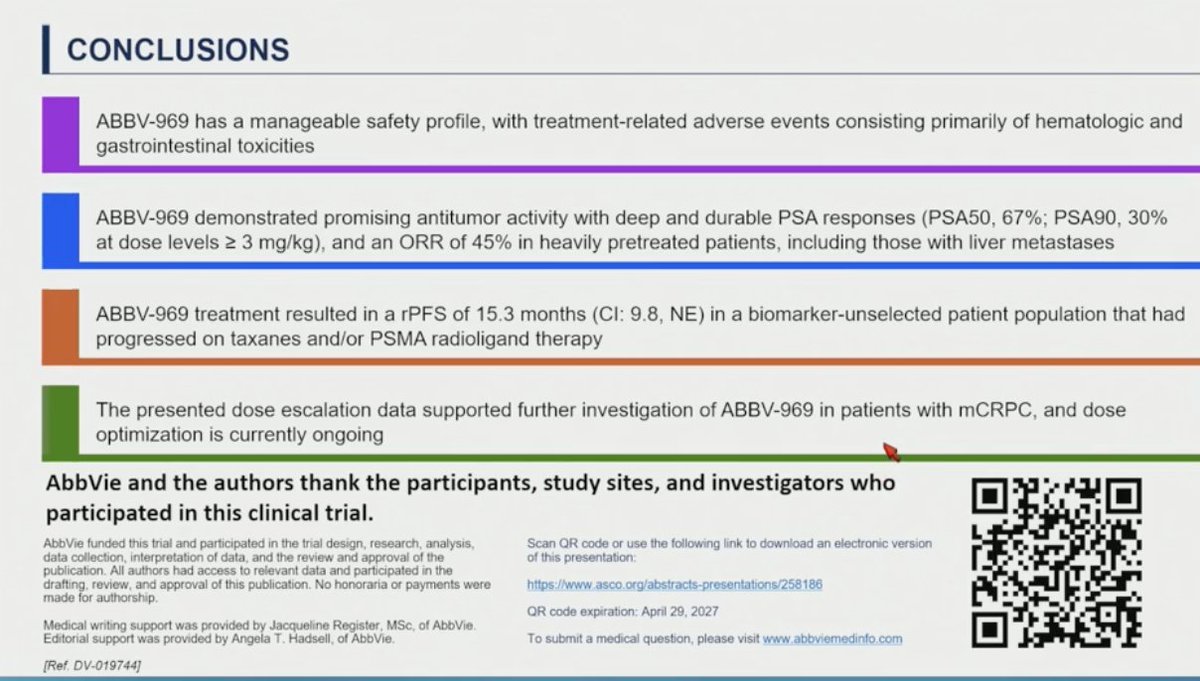
🔍 Manageable safety: anemia (59%) and fatigue (53%) most common, Grade ≥3 TRAEs 46.9%. ILD/pneumonitis only at the top dose, which has been dropped
Real activity in a post-taxane, post-RLT population that is running out of options. Dose optimization ongoing.
Congrats to the authors. @TDorffOnc
#ProstateCA #mCRPC #GUonc #ASCO26
9
14
902
May 31
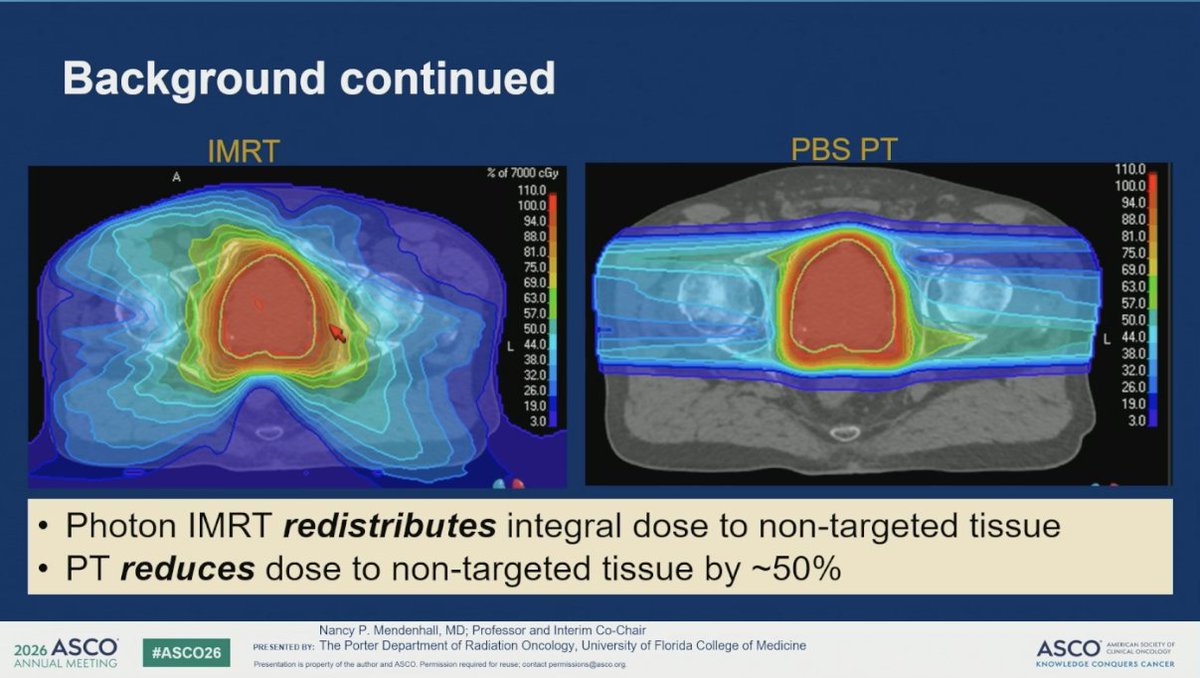
COMPPARE landed where its design pointed: proton and photon look equivalent for early toxicity and 3-year freedom from PSA progression, and both are reasonable standard of care. But the population may have been predicted to find no difference.
🔍 The case for protons is lower integral dose to non-target tissue. That matters most when you treat large volumes, like whole-pelvis nodal RT in high-risk or node-positive disease
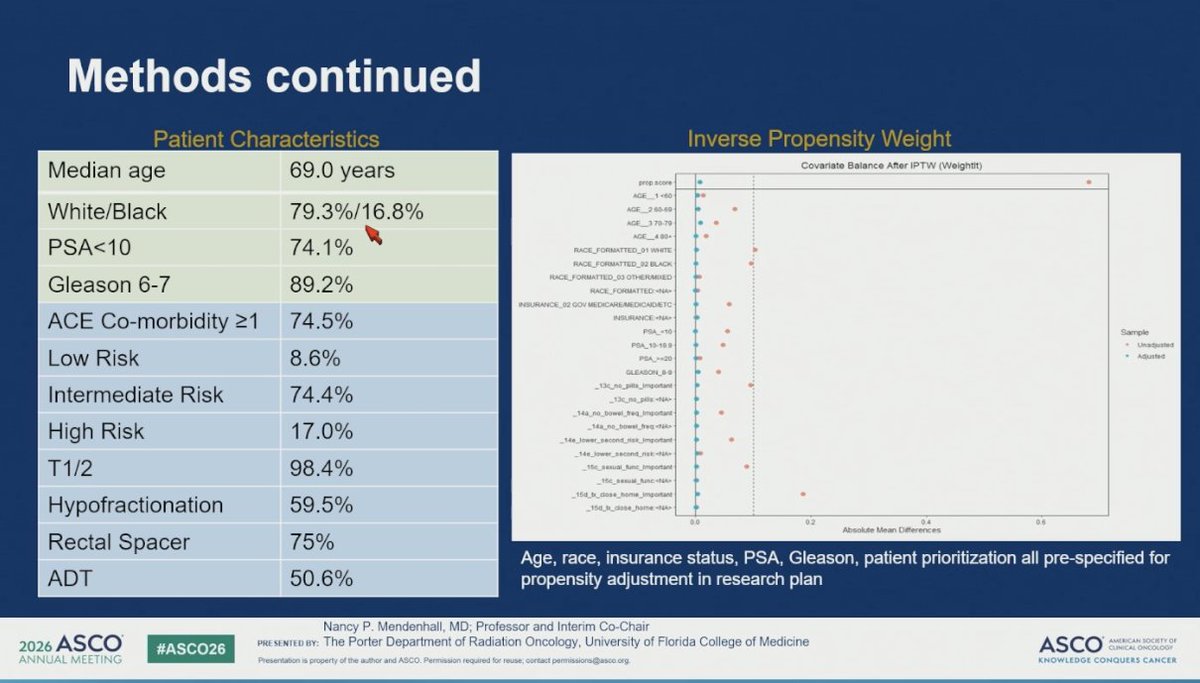
🔍 COMPPARE was 74% intermediate risk, 98% T1/2, mostly prostate-only fields, and excluded very high risk and metastatic. Small target, little room for protons to separate
🔍 75% got rectal spacers, which lowers rectal dose in both arms and narrows any modality gap
🔍 Bowel urgency was about 6% in both arms. At that event rate, equivalence is hard to interpret
The cleaner test is the patient you actually irradiate widely: high-risk, cN1, PSMA-PET node-positive, getting whole-pelvis treatment. That is where reduced integral dose could show up as less GI toxicity and, over time, fewer second malignancies.
The cleaner test is the patient you actually irradiate widely: high-risk, cN1, PSMA-PET node-positive, getting whole-pelvis treatment. That is where reduced integral dose could show up as less GI toxicity and, over time, fewer second malignancies. Hope we can see this study to come!
The patients most likely to benefit from protons were the ones this trial left out.
#ProstateCA #GUonc #ASCO26 @OncoAlert #RadOnc #ProtonTherapy

3
10
17
2,084
May 31
Perioperative apalutamide ADT improved event-free survival in high-risk localized or locally advanced prostate cancer. PROTEUS, now in NEJM.
Phase 3, double-blind, n=2,109. 6 cycles of ADT ± apalutamide before and after radical prostatectomy. Median follow-up 61.7 mo.
🎯 EFS: median 48.7 vs 39.9 mo, HR 0.71 (95% CI 0.63-0.80), p<0.001
🎯 pCR or minimal residual disease: 8.9% vs 1.0%, OR 10.17, p<0.001
🎯 5-yr MFS: 78.2% vs 73.5%, HR 0.80 (0.67-0.96), p=0.02
🔍 Grade 3/4 AEs 39.6% vs 31.0%, mostly rash
EFS separates early and holds. The MFS gain is more modest and OS is immature.
👉bit.ly/proteus-efs
#ProstateCA #GUonc #ASCO26

Presented at #ASCO26:
In high-risk localized prostate cancer, ADT plus apalutamide led to a pathological complete response or minimal residual disease and 5-year metastasis-free survival in a greater percentage of patients than ADT plus placebo. Full phase 3 PROTEUS trial results: nej.md/3RuNe00
Editorial: A Watershed Moment in the Perioperative Treatment of Prostate Cancer nej.md/4dLeiiW
@ASCO
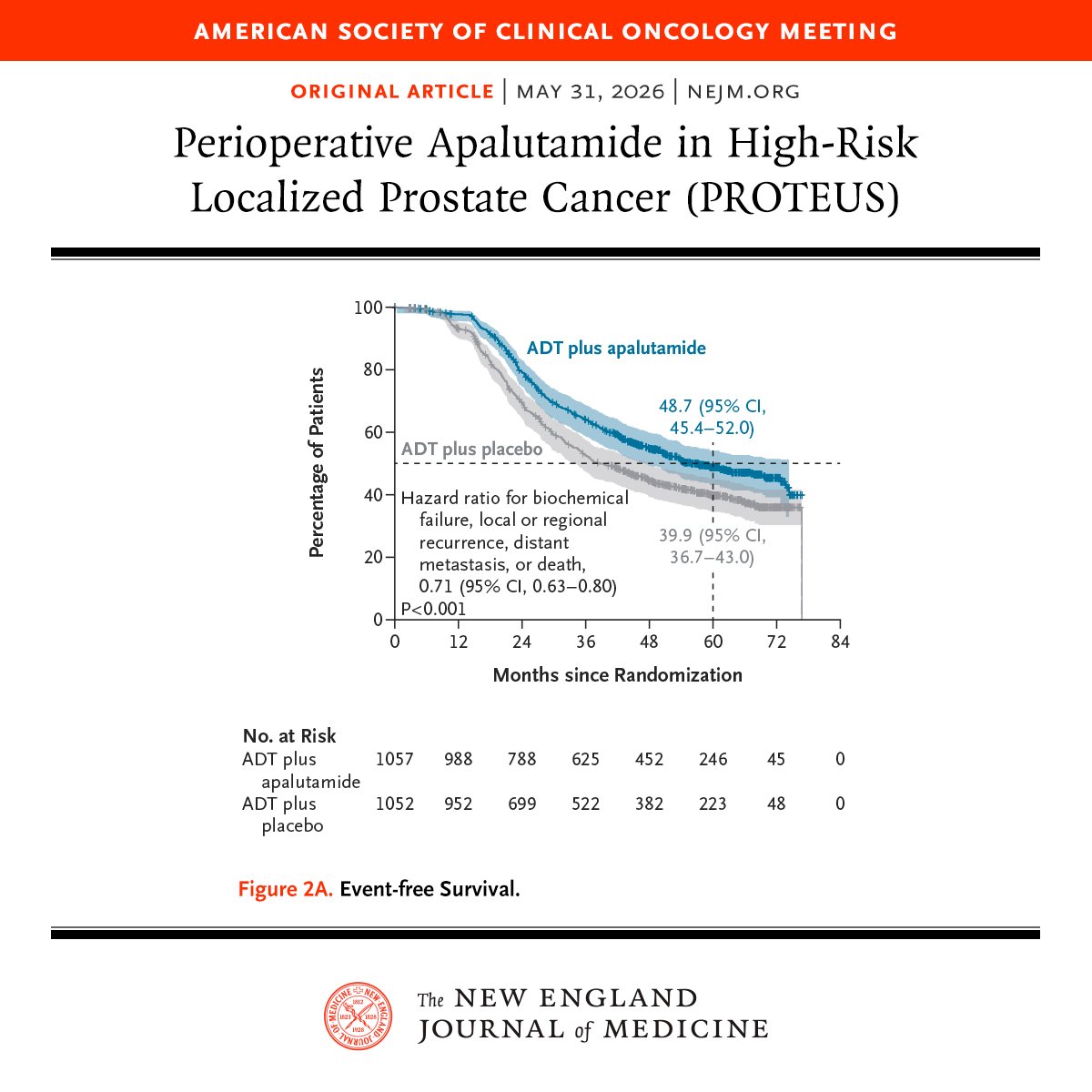
ALT A survival analysis graph from a study published in the New England Journal of Medicine shows the percentage of patients over time in months since randomization. The graph compares "ADT plus apalutamide" to "ADT plus placebo." Data includes hazard ratios and confidence intervals. The American Society of Clinical Oncology Meeting is mentioned at the top.
1
9
6
912
May 31
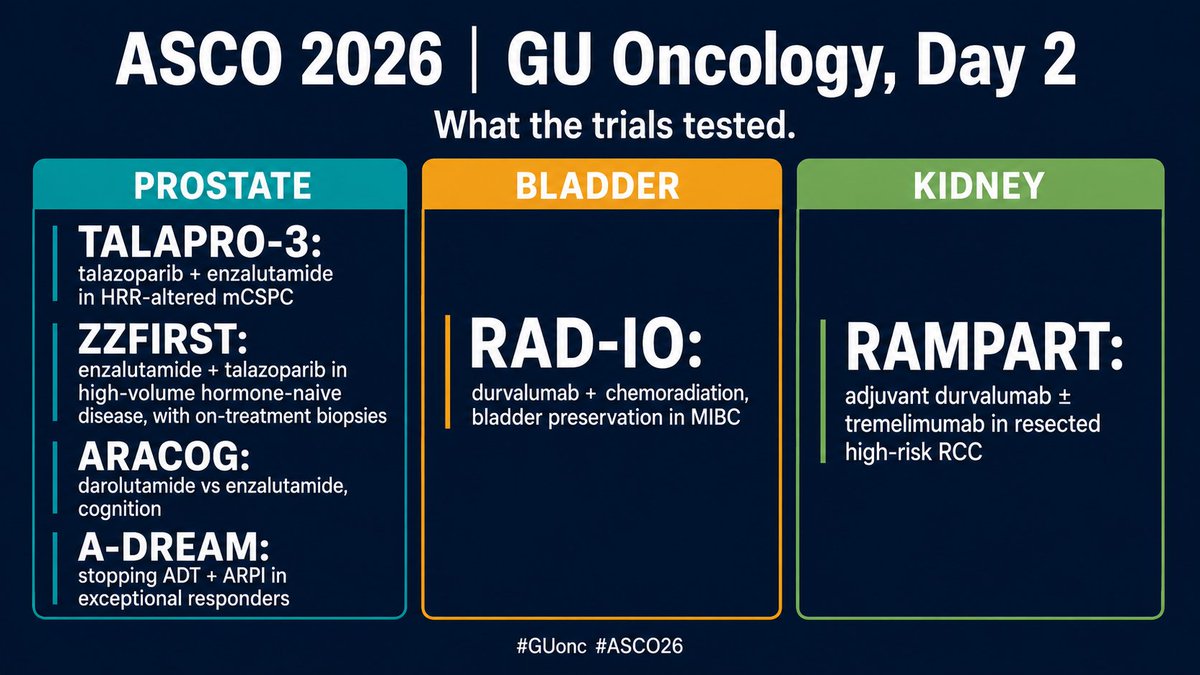
Day 2 of #ASCO26 in GU oncology covered all three diseases, and the through-line was personalization: who needs more, who needs less, and who needs testing first.
Prostate
🎯 TALAPRO-3: TALA ENZA cut progression risk 52% in HRR-altered mCSPC (rPFS HR 0.481), benefit beyond BRCA
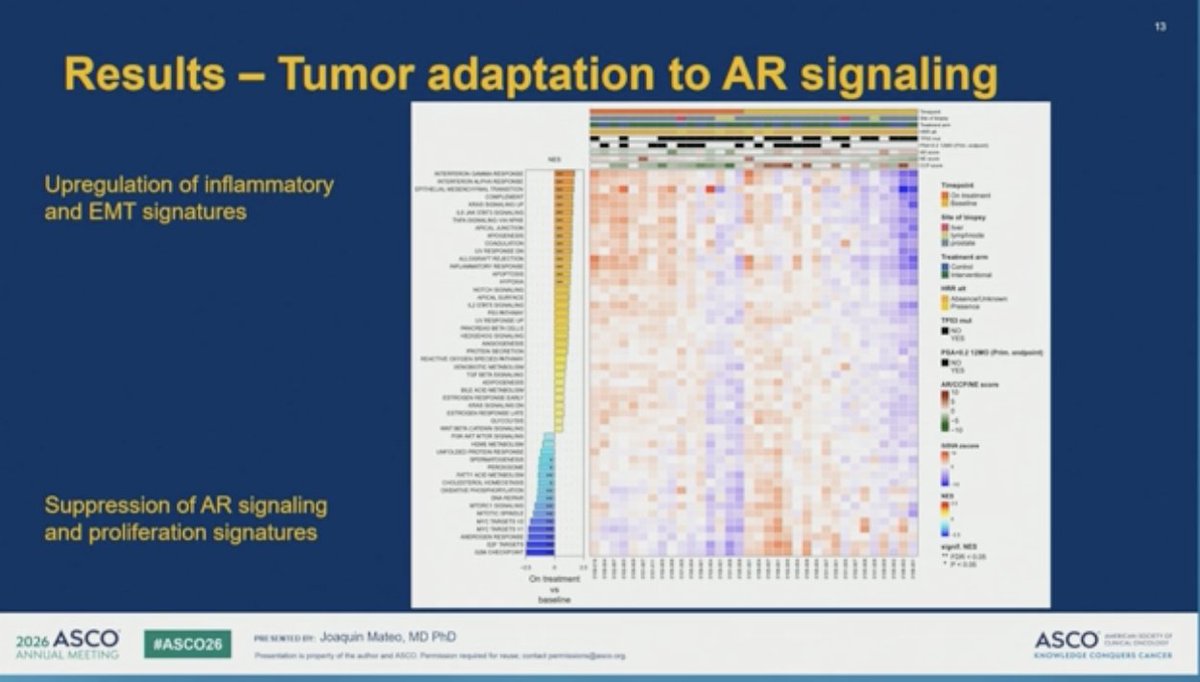
🎯 ZZFIRST: EZ TALA, 73% PSA <0.2 in high-volume mHSPC, with on-treatment biopsies showing the adaptive biology
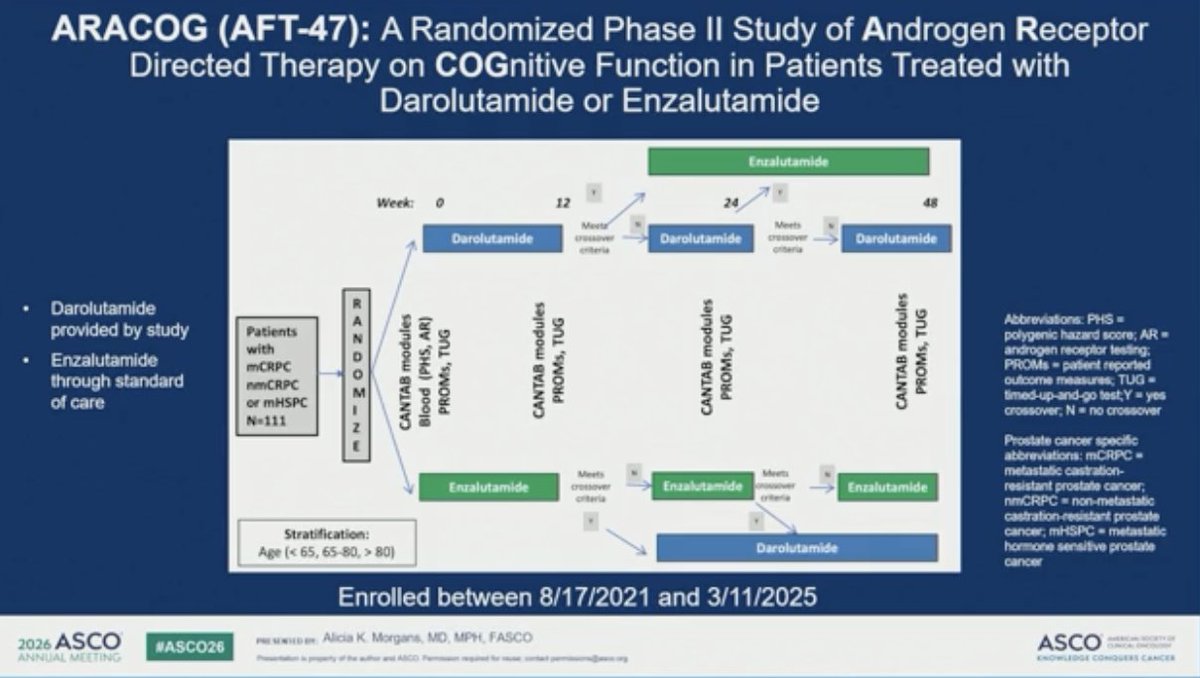
🎯 ARACOG: first US randomized head-to-head on cognition, enza declined more than daro at 24 wks
🎯 A-DREAM: 41% of exceptional responders stayed treatment-free 18 mo after stopping ADT ARPI
Bladder
🎯 RAD-IO: single arm feasibility, durvalumab chemoRT, bladder-preserving, with strong early DFS in MIBC
Kidney
🎯 RAMPART: adjuvant durvalumab ± tremelimumab in RCC, both IO arms moved the same direction, durva mono signal did not reach significance
More tomorrow.
#ProstateCA #BladderCancer #RCC #GUonc #ASCO26 @OncoAlert
1
11
18
1,132
May 30
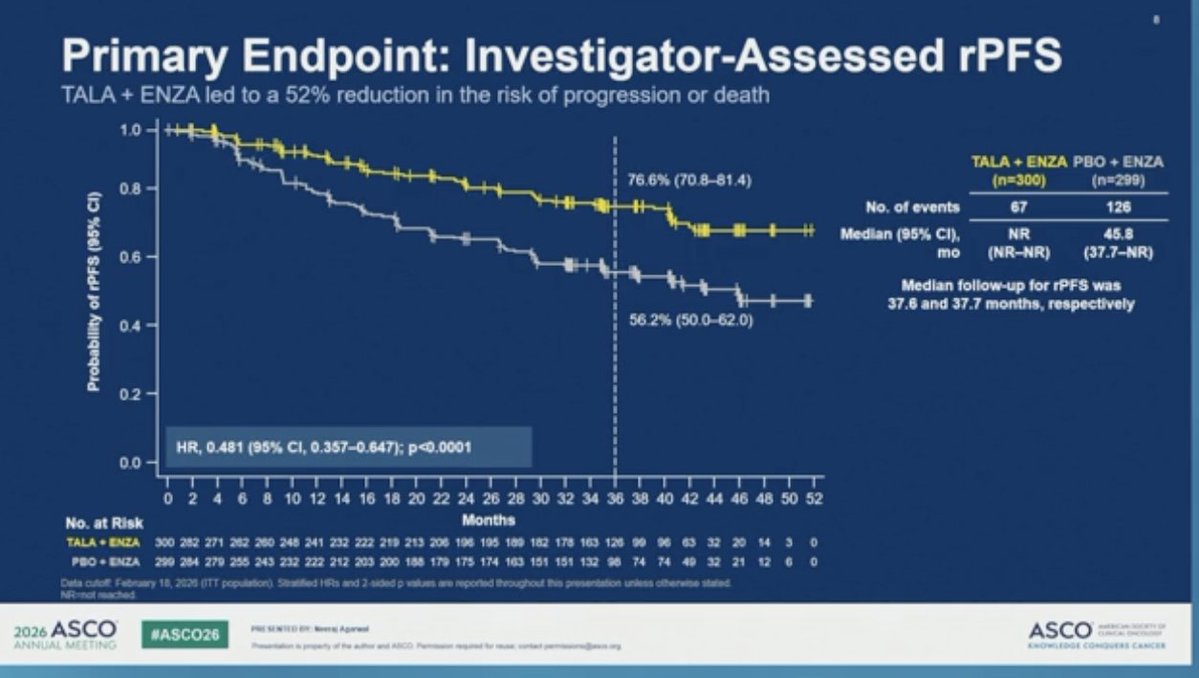
TALAPRO-3 met its primary endpoint: talazoparib enzalutamide cut the risk of progression or death by 52% vs enzalutamide alone in HRR gene-altered mCSPC (rPFS HR 0.481, 95% CI 0.357 to 0.647, p<0.0001).
Phase 3, 599 pts, first-line HRR-altered mCSPC, randomized 1:1 to TALA ENZA vs placebo ENZA. Median follow-up ~38 mo.
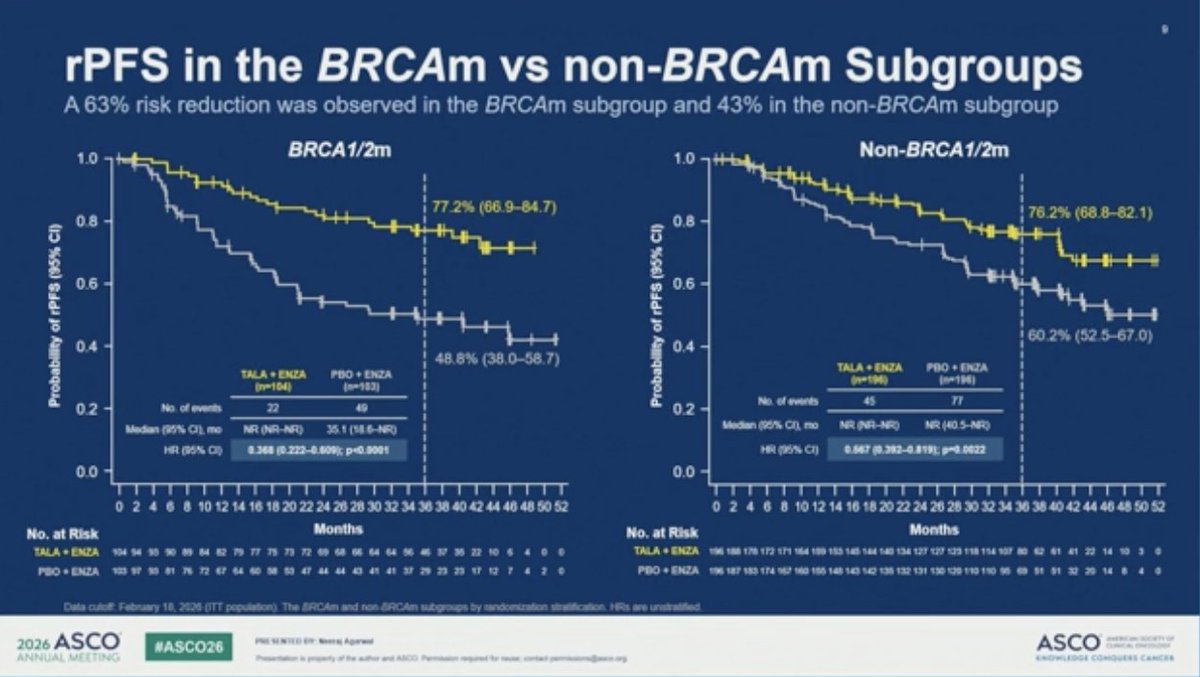
🎯 Median rPFS: NR vs 45.8 mo (HR 0.481, p<0.0001) 📊 BRCAm subgroup HR 0.37, non-BRCAm HR 0.57. The benefit was consistent, not BRCA-driven 📊 Interim OS trend favors the combination (HR 0.767, 95% CI 0.564 to 1.044, p=0.09), still immature 📊 No clinically meaningful PRO decline vs ENZA alone, despite the added drug
🔍 Toxicity is the trade. Anemia 71% (24% G≥3), 60% needed a TALA dose reduction, and AEs of special interest included 3 MDS and 2 AML in the combination arm.
The mCSPC space is getting crowded.
#⃣The number that should change practice today is upstream: you cannot offer this without HRR testing, and early molecular testing in prostate cancer is still the rate-limiting step.
Congrats to the team. @neerajaiims
NEJM 👉bit.ly/talapro3-rpfs
#ProstateCA #mCSPC #GUonc @OncoAlert

3
9
19
1,357
May 30
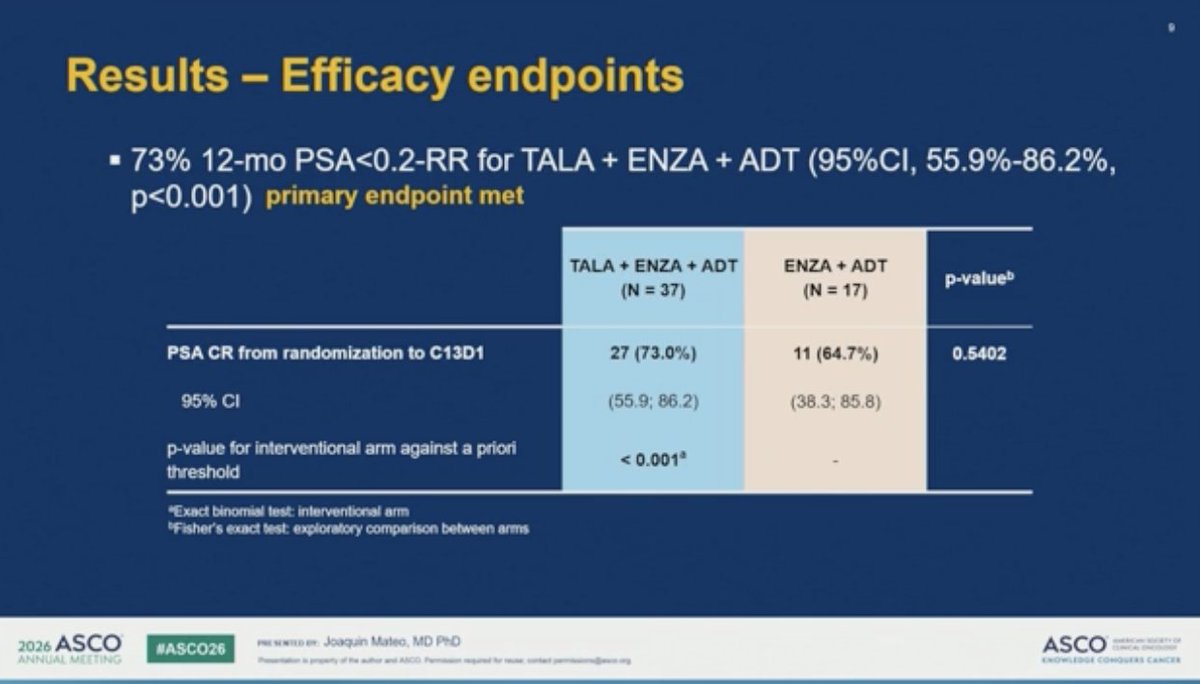
ZZFIRST met its primary endpoint: enzalutamide talazoparib hit a 73% confirmed PSA <0.2 response rate at 12 months in high-volume mHNPC
Randomized academic phase 2, 54 pts. ADT enza lead-in, then 2:1 to add talazoparib or continue enza. Only 13% HRR-altered.
🎯 12-mo PSA <0.2-RR: 73% EZ TALA vs 64.7% EZ
📊 Median rPFS 45.3 vs 31.1 mo (HR 0.62)
🔍 Small trial, exploratory between-arm comparisons, wide CIs. And real toxicity: anemia G≥3 40.5%, 2 AML cases with prolonged exposure.
🔬 The translational work is the story. Paired on-treatment biopsies showed AR and DDR signature downregulation with enza, the adaptive state that justifies adding PARP. Getting on-treatment tissue in prostate cancer, where tissue is so often the issue, is an amazing effort.
#ProstateCA #mHNPC #GUonc #ASCO26 @OncoAlert

6
10
915
May 30
ARACOG (AFT-47) met its primary endpoint: enzalutamide caused significantly greater cognitive decline than darolutamide at 24 weeks in advanced prostate cancer.
Randomized open-label phase 2, 111 pts (mHSPC, mCRPC, nmCRPC), DAR vs ENZ.
Cognition was measured with CANTAB, a validated computer-based battery testing memory, attention, working memory, and executive function at baseline, 12, 24, and 48 weeks. The primary endpoint was percent change in each patient's most-affected domain.
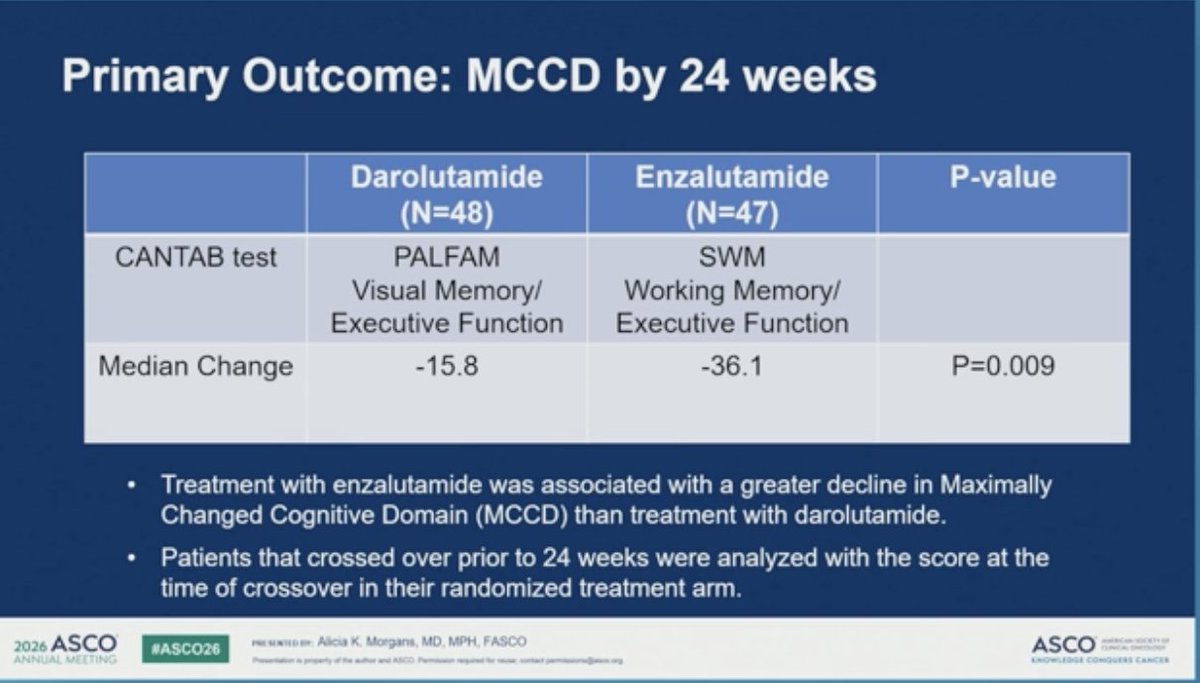
🎯 Median change in maximally changed cognitive domain at 24 wks: -15.8% DAR vs -36.1% ENZ (p=0.009)
📊 ENZ showed stable to declining learning effect
📊 Crossover allowed for cognitive or PRO decline. 23 pts crossed by 24 wks, and every one was randomized to ENZ, all switching to DAR
For the patient choosing therapy, this is the kind of data that actually informs the conversation.
Nicely done. @CaPsurvivorship
#ProstateCA #GUonc #mHSPC #ASCO26

6
9
702
May 30
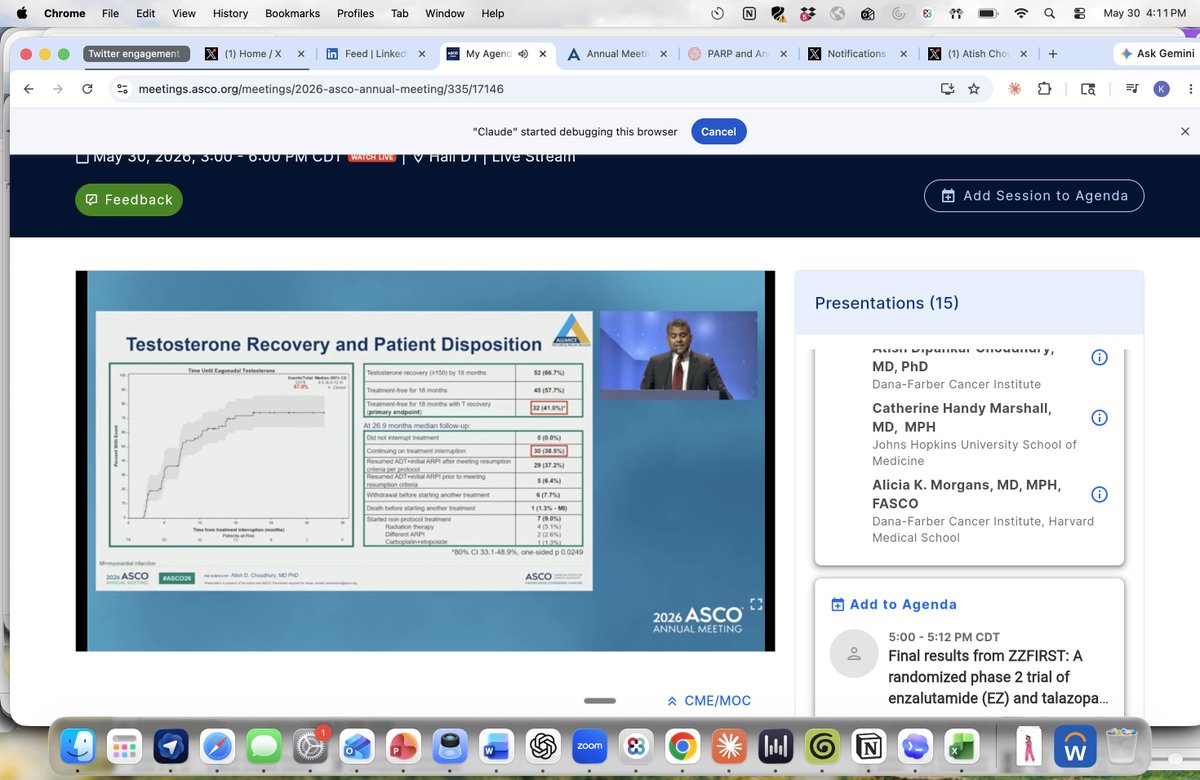
A-DREAM asked a question patients actually care about: can favorable responders to ADT ARPI safely take a break?
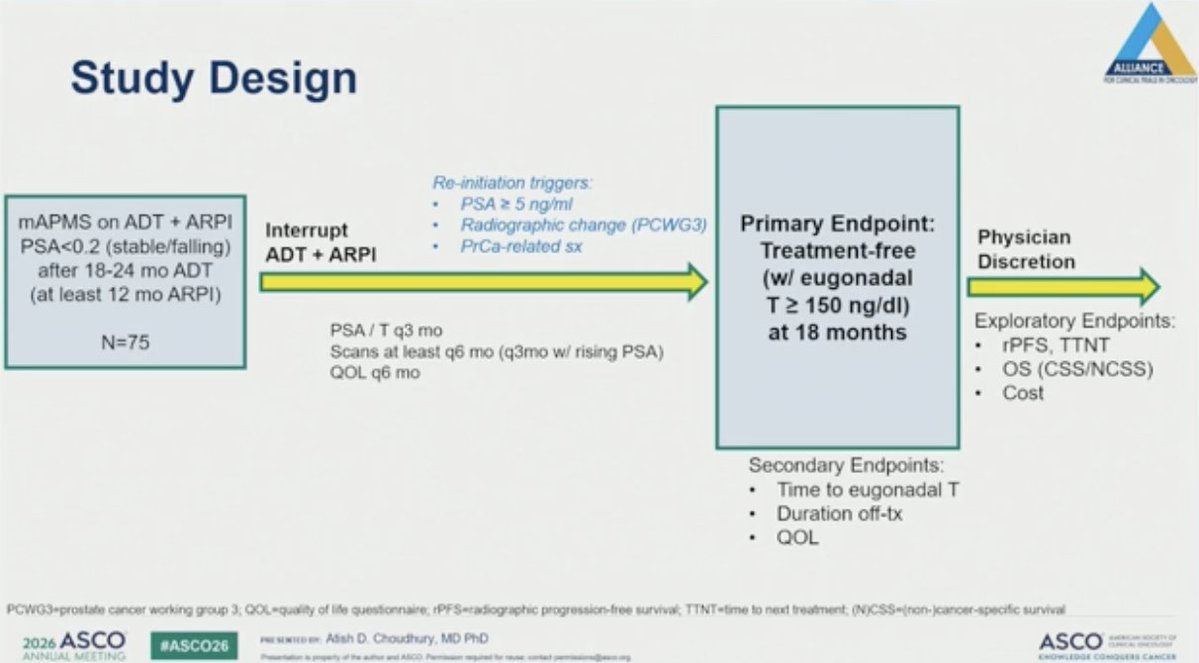
Single-arm phase 2 (Alliance A032101) in mHSPC. Eligible men had PSA <0.2 and suppressed testosterone after roughly 18 to 24 months on ADT ARPI, then interrupted treatment.
Primary endpoint met:
🎯 41% (32/78) treatment-free with testosterone recovery at 18 mo (80% CI 33.5 to 48.9%, one-sided p=0.0249)
📊 67% (52/78) recovered eugonadal testosterone
📊 58% (45/78) remained treatment-free at 18 mo
📊 Median 24.5 mo off treatment, and 38.5% still off at 26.9 mo median follow-up
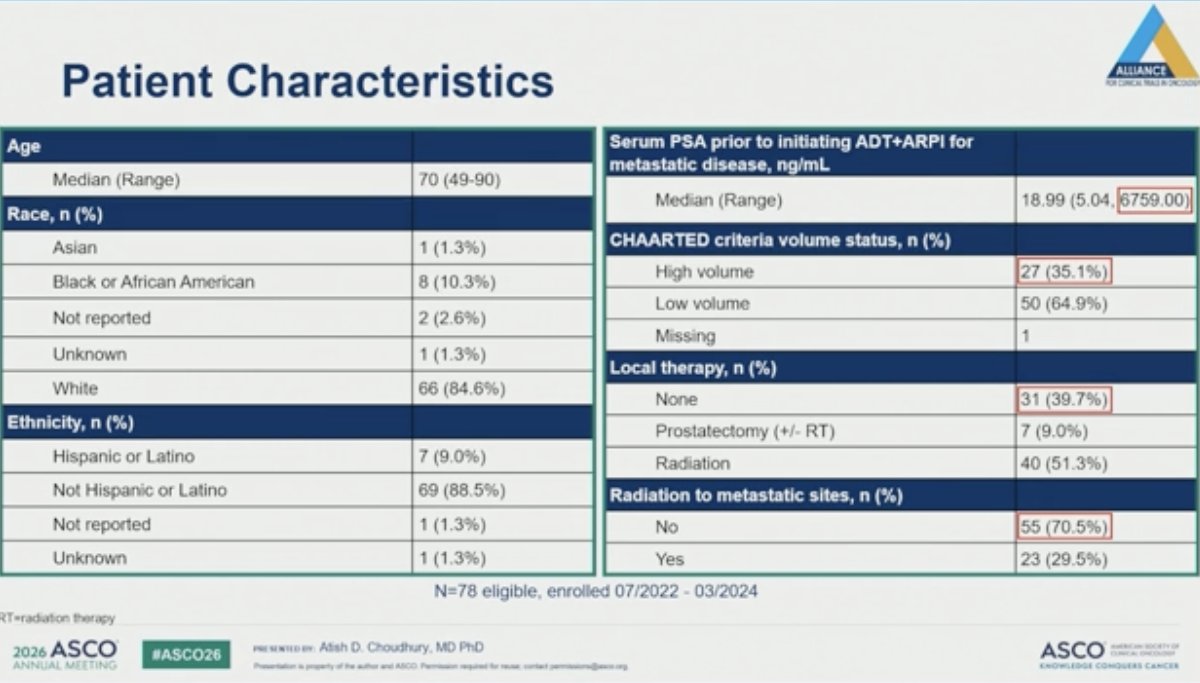
🔍 Low-volume disease and prior radiation to metastases predicted lower likelihood of needing to restart. Selection matters: these were patients and clinicians motivated to interrupt.
Defining the optimal intermittent strategy is the next question. Biomarker and PRO analyses pending.
Nicely done.
@AtishChoudhury #ProstateCA #mHSPC #GUonc #ASCO26
10
21
1,198
May 30
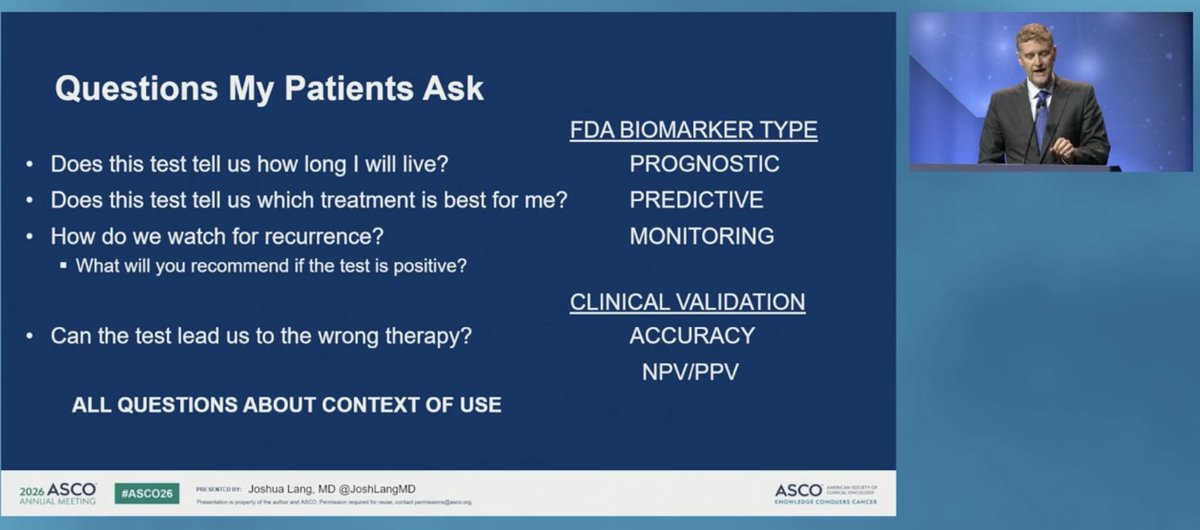
@JoshLangMD discussed approach to precision oncology:
🔍 Prognostic, predictive, monitoring are different claims. Most GU classifiers start as prognostic, then used as if predictive. Context of use is everything.
🔍 Models trained on cohorts that predate ADT ARPI or triplet may not hold in today's backbone.
🔍 Only randomized testing of the assay (NRG-GU009 PREDICT-RT) defines actionability.
Great discussion.
#ProstateCA #GUonc #AIinMedicine #ASCO26
2
157
May 30
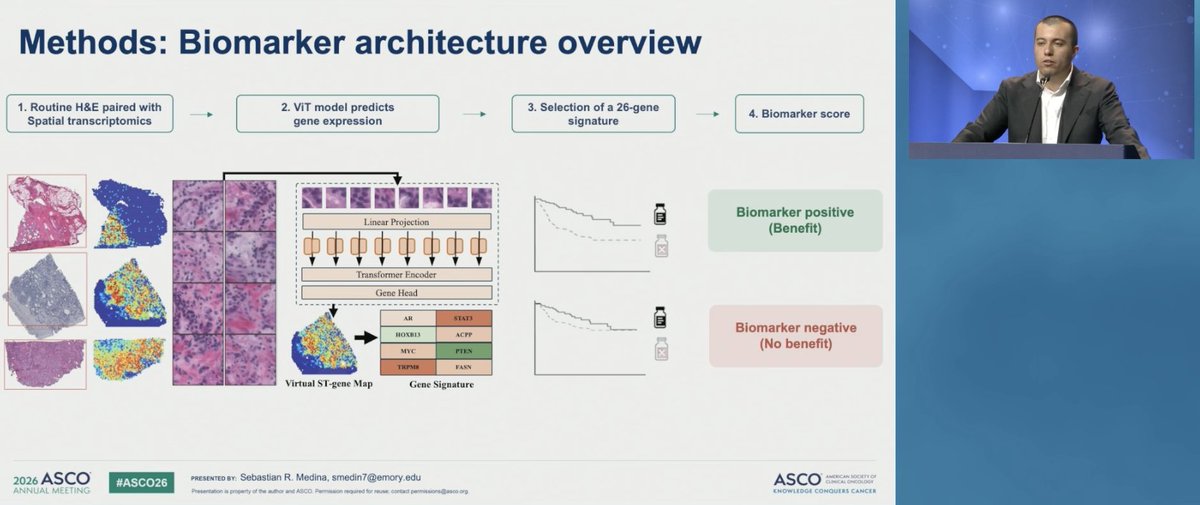
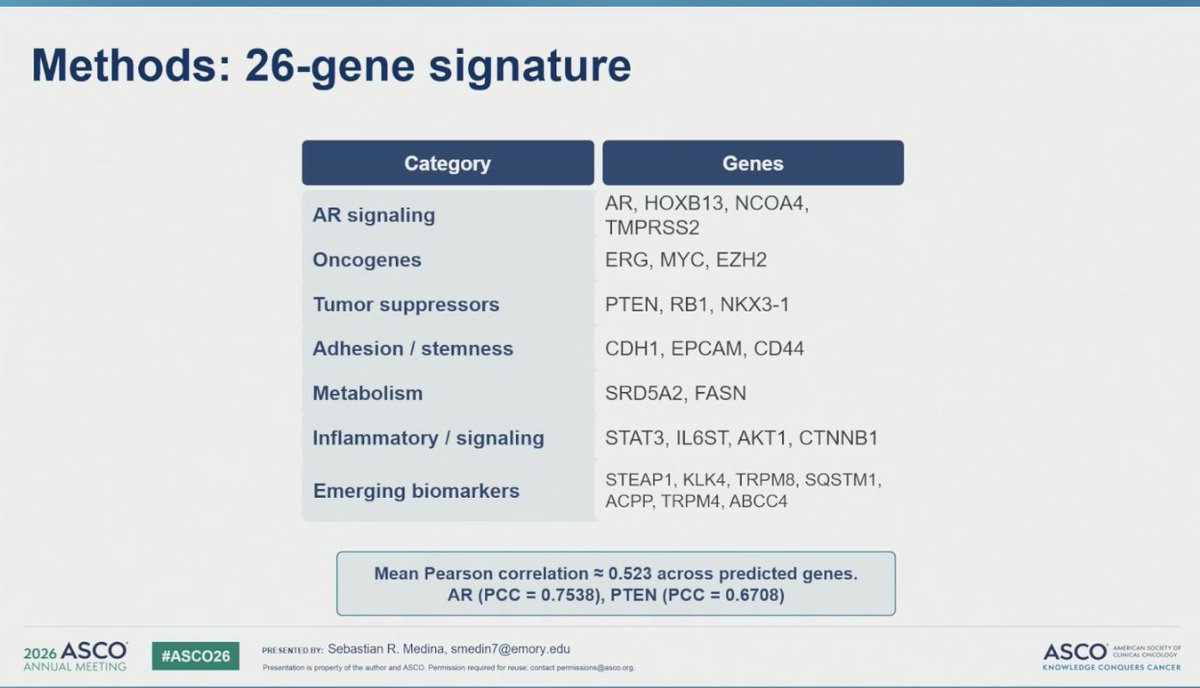
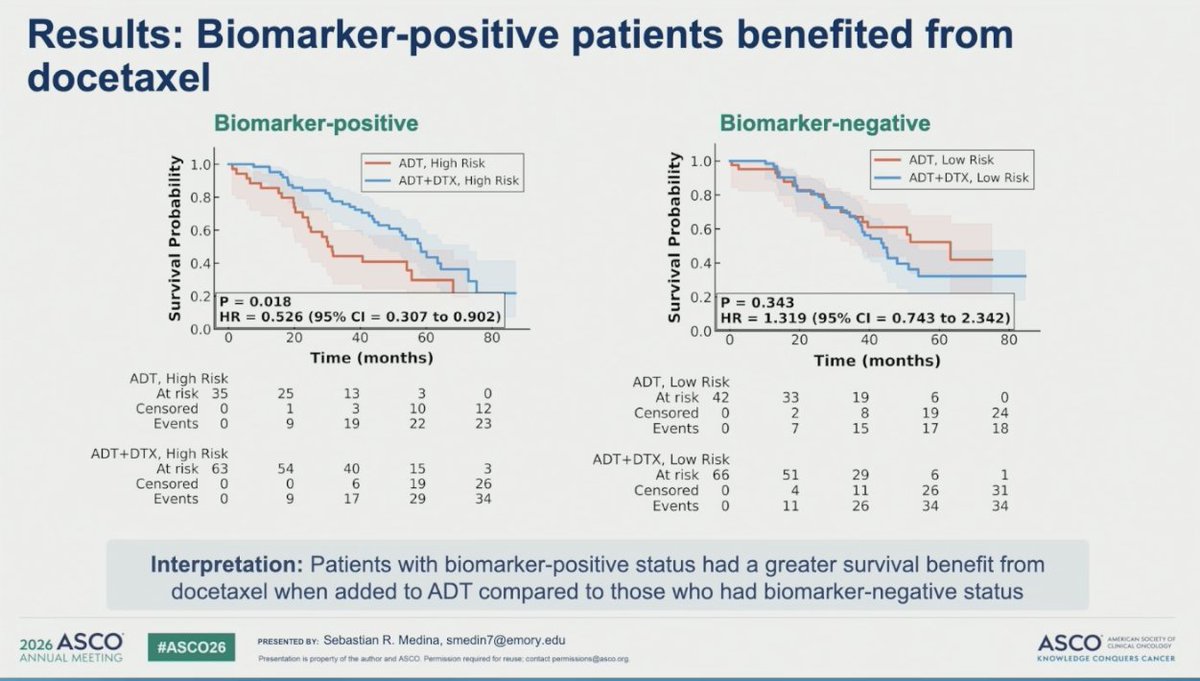
Predicting docetaxel benefit in mHSPC from a routine H&E slide. An AI biomarker that infers spatial gene expression from histology, then stratifies who actually gains from adding chemo to ADT.
Trained, locked, then applied to CHAARTED:
🔬 Biomarker-positive: docetaxel improved OS, HR 0.53 (0.31 to 0.90), p=0.018
🔬 Biomarker-negative: no benefit, HR 1.32 (0.74 to 2.34)
📊 Treatment-by-biomarker interaction held after adjustment (p=0.046)
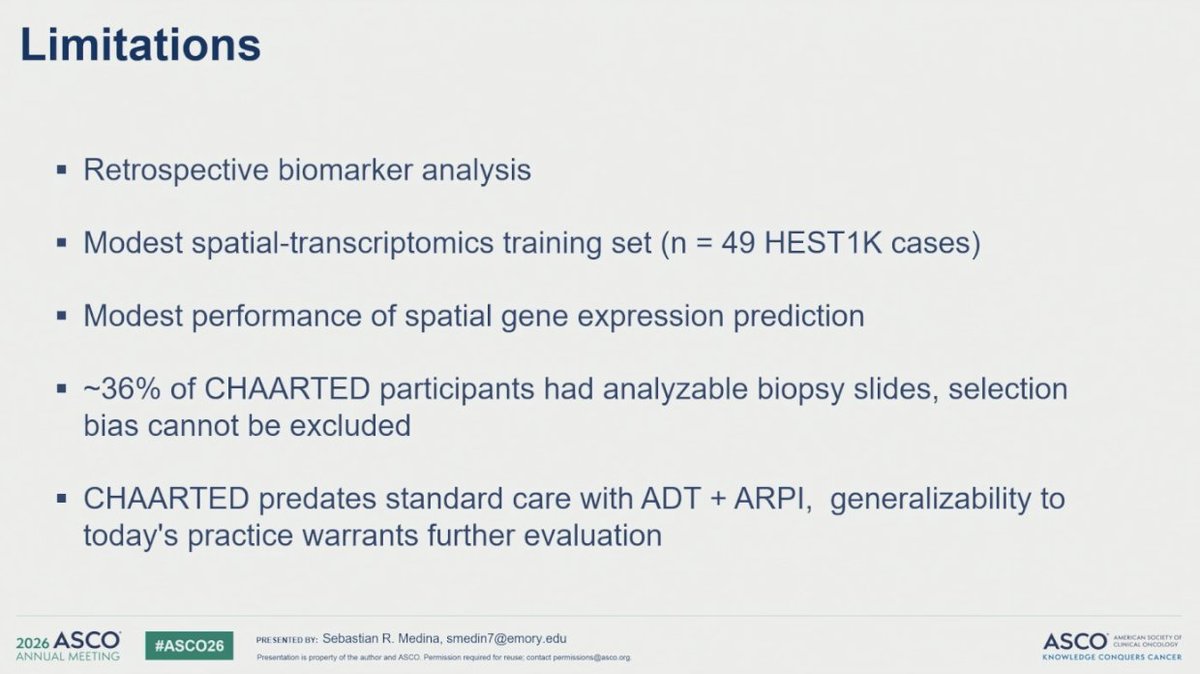
🔍 Retrospective, only ~36% of CHAARTED had analyzable biopsies, and CHAARTED predates ADT ARPI. Whether this holds in the triplet era is anotheranother question.
Promising proof of concept. Needs prospective validation in a modern treatment setting before it changes any chemo decision.
#SebastianMedina
#ProstateCA #mHSPC #GUonc #AIinMedicine #ASCO26 #CHAARTED
12
19
3,663
May 19
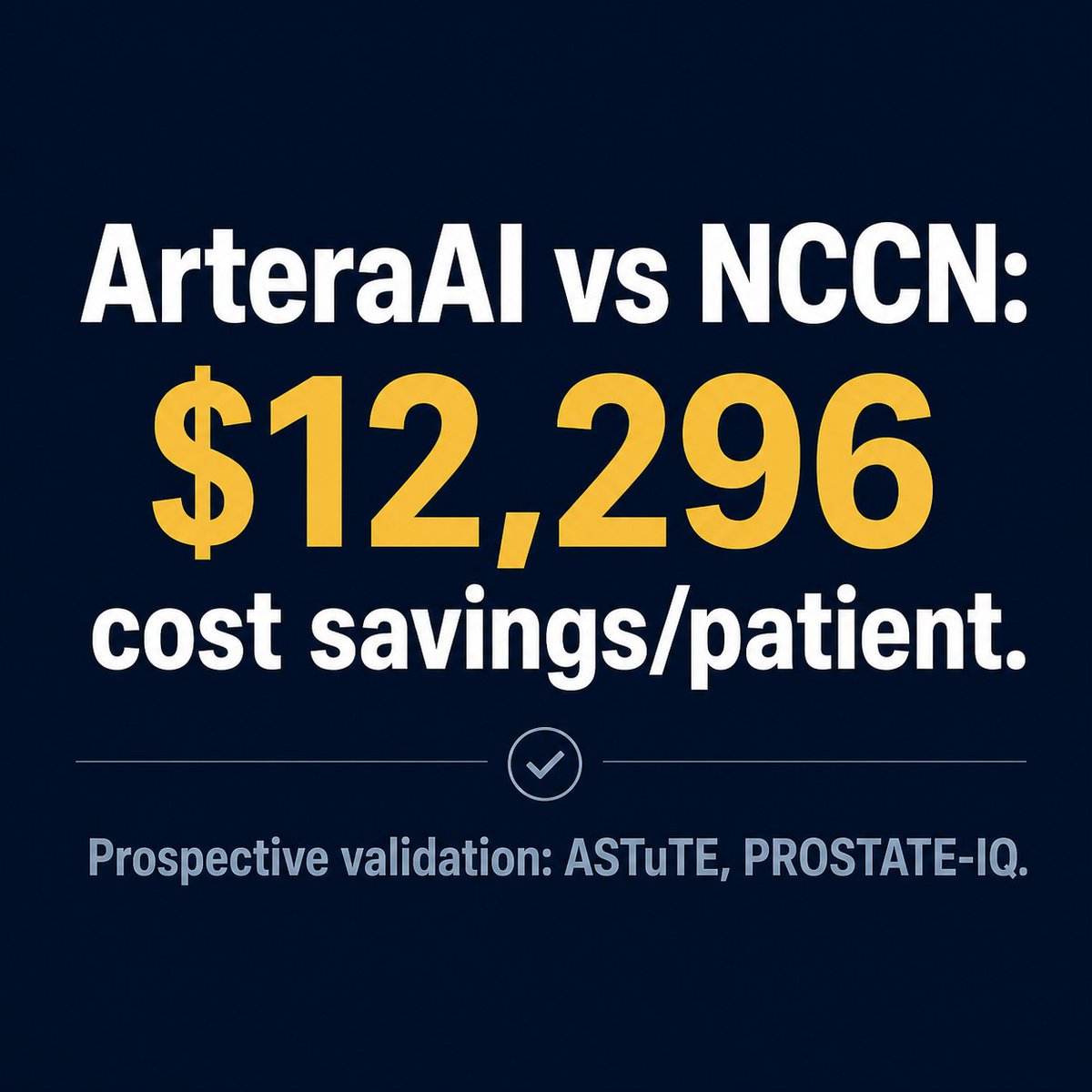
AI-guided ADT de-escalation in intermediate-risk prostate cancer: cost-effective on paper, prospective data still pending.
First cost-effectiveness analysis of the ArteraAI Prostate Test vs NCCN risk grouping (15-year Markov model, RTOG 9408 data):
📊 ArteraAI-guided strategy: dominant, lower costs AND marginally better QALYs vs NCCN
💰 $12,296 cost savings per patient
The prospective data are coming.
ASTuTE (n=800, Australia) is testing whether ArteraAI changes shared ADT decision-making in real-world IR prostate cancer with 5-year disease control endpoints.
PROSTATE-IQ is the randomized phase 3 trial using ArteraAI to personalize androgen axis therapy intensity after prostatectomy.
Those results will complete this story.
💡bit.ly/artera-adt-cea
Congrats on this work: @AnnRaldow_MD @amarukishan
#ProstateCA #GUonc #AI
2
6
10
1,115
May 15
Not a lecture. Not a debate. Just three GU oncologists saying what they actually think about the data.
Genuinely thrilled to sit down with @GUOncologyNow, @PGrivasMDPhD, and @CParkMD at #OncForum2026 in Chicago on May 31. People I genuinely respect and who will not hold back.
Register 👇
bit.ly/4sEtXG5
#GUOncology #OncForum2026 #bladderCa #RCC #prostateca
1
7
25
2,843
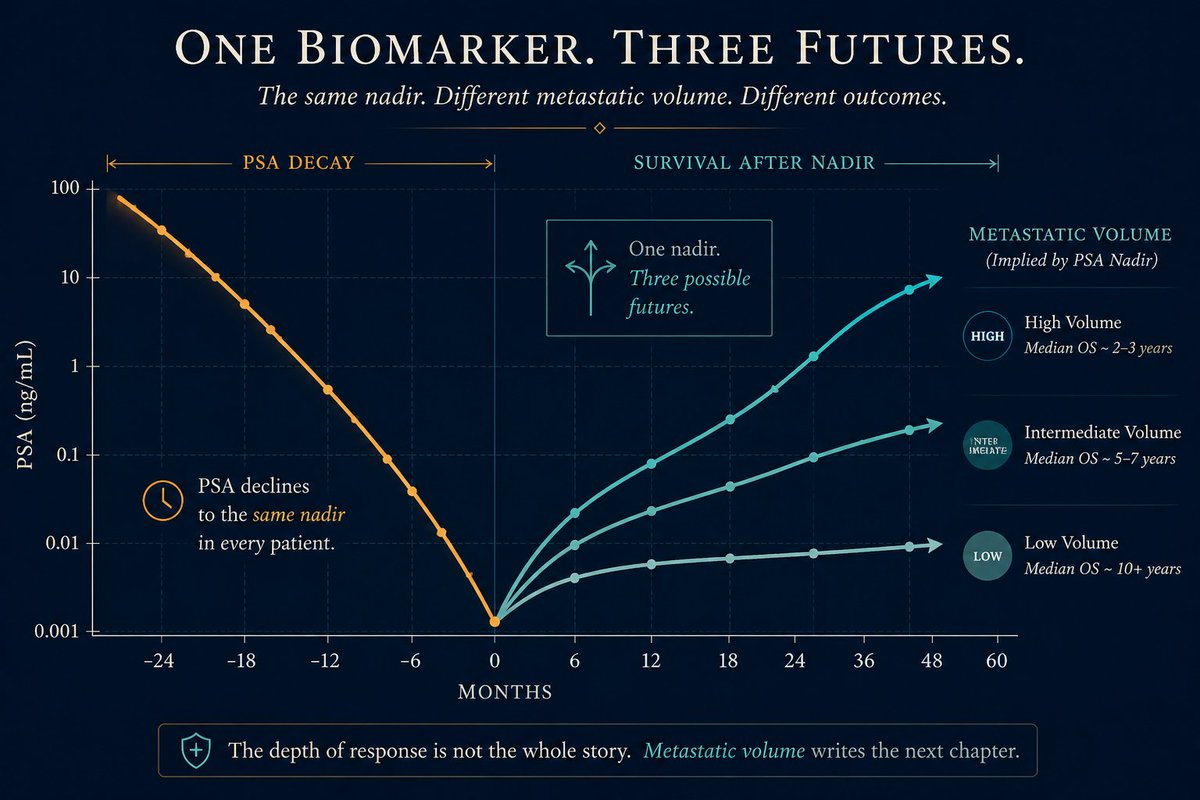
PSA nadir at 24 weeks remains one of the strongest prognostic signals mHSPC, but the meaning depends entirely on metastatic volume.
➡️ Pooled analysis of 5 STAMPEDE phase 3 trials (n=7,129)
➡️ With abi±enza PSA ≤0.2 ng/mL at 24 wks: 96-mo OS was 64% in low-volume mets vs 45% in high-volume
➡️ Non-metastatic, node-positive: 79% 96-mo OS
Could PSA nadir volumetric burden refine clinical-trial enrichment for treatment intensification? 🩺
bit.ly/3PgpID1
#ProstateCA #mHSPC #GUonc
1
31
65
4,333
Apr 30
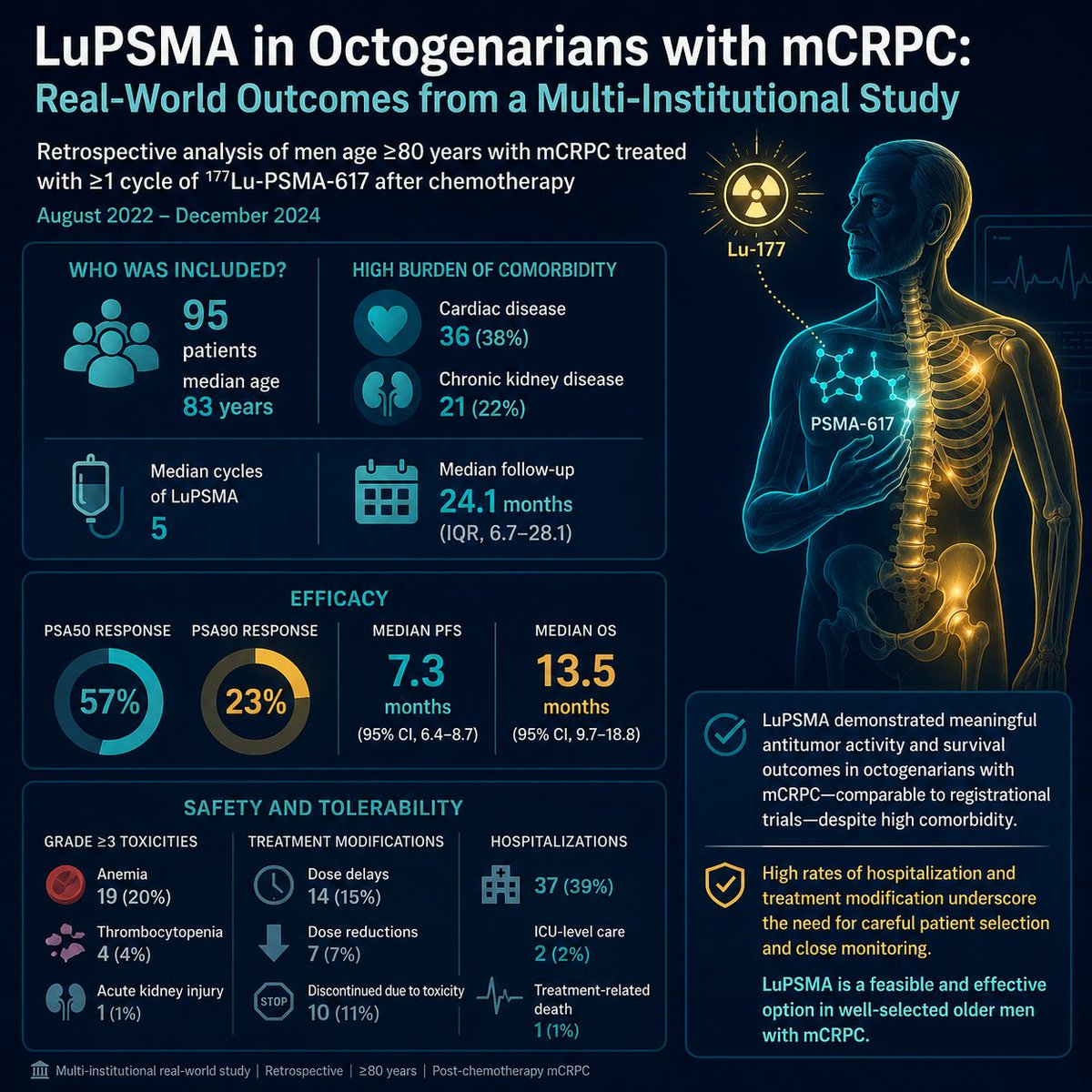
VISION enrolled mostly under 80. What about the 83-year-old in clinic today? Real-world data finally answer.
n=95 octogenarians on LuPSMA across DFCI, Mayo, Vanderbilt:
➡️ PSA50 57%, PSA90 23%
➡️ mPFS 7.3 mo, mOS 13.5 mo (matches VISION)
➡️ 39% hospitalized; G3 anemia 20%
Why this matters: 💡 LuPSMA works in octogenarians and close monitoring is necessary. Congrats @PrafulRavi1 as applicable to real-world populations in the community!
#mCRPC #ProstateCA #PSMA #GUonc
Apr 27

What are the outcomes of #LuPSMA in #octagenarians with advanced prostate cancer? Our collaborative experience with @DanaFarber_GU @MayoClinic @VUMChealth led by Daniel Sentana and Avina Rami, published in @JCOOP_ASCO: ascopubs.org/doi/10.1200/OP-…
10
17
2,428

Apr 30
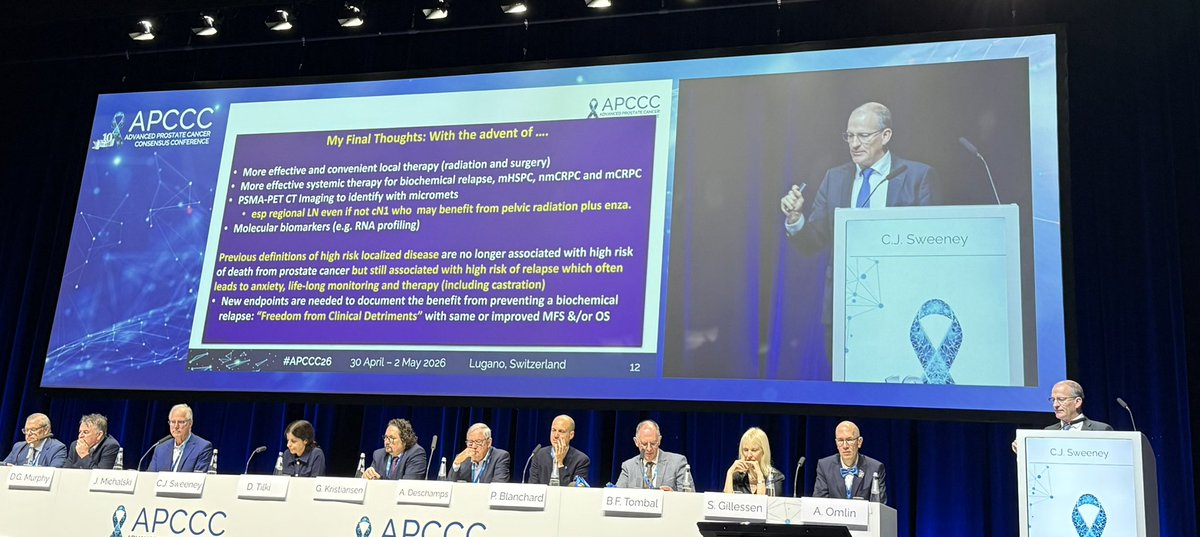
#APCCC26 Debate: Patients with high-risk localised #ProstateCa need the addition of an ARPI to RT plus long-term ADT?
For addition of ARPI to RT plus ADT - Tsunami of data coming! #RiskStratification essential @ChrisSweens1 @OncoAlert

10
15
525