
Dad and husband | @DukeGUCancer GU Oncologist, DCI Center for Prostate and Urologic Cancers | Former @UNC Hem/Onc Chief Fellow | @vtcsom grad | Phase 1 trials
Joined June 2023
- Tweets 346
- Following 343
- Followers 279
- Likes 188
152 Photos and videos




Pinned Tweet

10 Dec 2025
I recently spoke at the @KidneyCancer Association Duke/UNC patient event on #RCC treatment.
We covered:
• Adjuvant pembro for higher-risk pts
• IO/TKI and dual IO strategies
• How we personalize treatment
• Role of clinical trials
📽️ Full talk: youtu.be/fSeaxjagqz4?si=bMXk…
2
5
1,080
Dillon Cockrell, MD retweeted

Jun 2
We know Black men are at higher risk for #prostatecancer & that a variant T allele increases their risk 3.4 x. The news: if someone has 2 of these T alleles, risk appears 11.4 x. Listen as McManus & Shevach discuss. #ASCO26 @DukeGUCancer @DukeCancer @DukeHealth
2
6
16
2,112
Dillon Cockrell, MD retweeted
Jun 2
@DukeGUCancer late-night meeting to welcome Dr. Michael Superdock to the family. How can we not expect great things from someone named "superdock?"
@MSuperdock @DukeCancer

ALT Nine people sitting around a bar table with an explosed brick background
1
3
20
701
Dillon Cockrell, MD retweeted

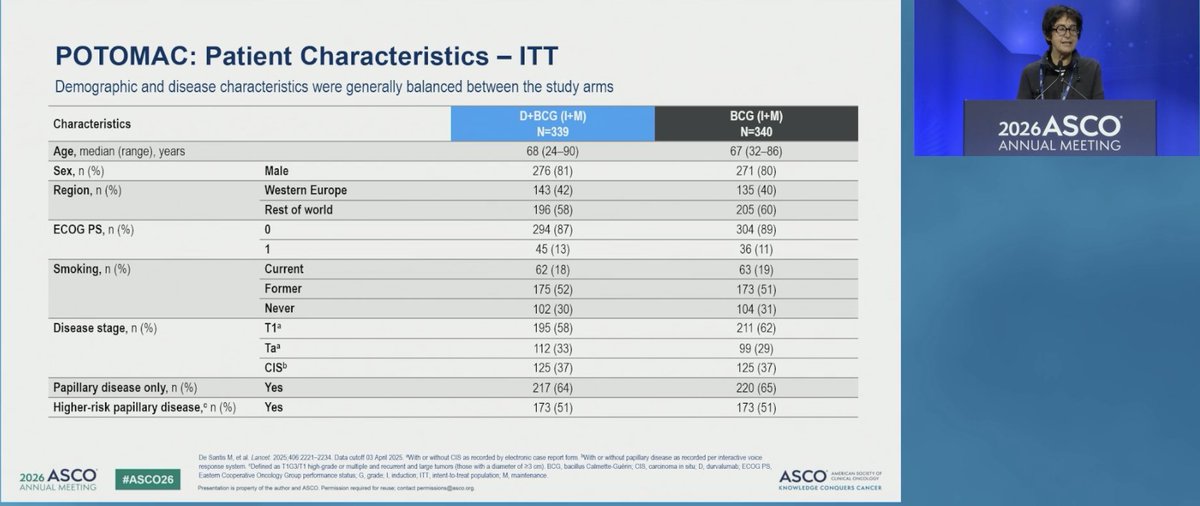
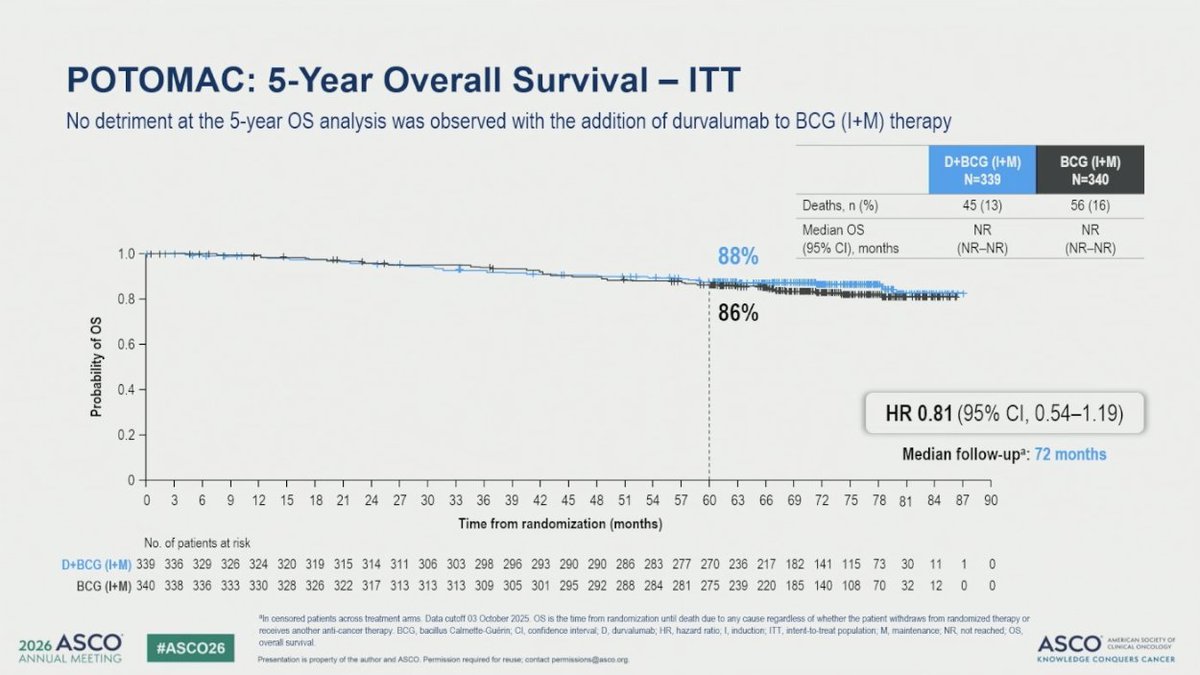
Radical cystectomy for recurrent high-risk NMIBC is not a benign salvage when considering radical cystectomy. POTOMAC's DFS benefit with D BCG matters more through that lens than a neutral OS curve suggests.
Phase 3, D BCG (I M) vs BCG (I M), n=679; median follow-up 72 months.
📊 5-year OS: 87.6% vs 86.3%; HR 0.81 (95% CI 0.54-1.19); median OS NR in either arm
🎯 DFS benefit established at primary analysis vs BCG alone
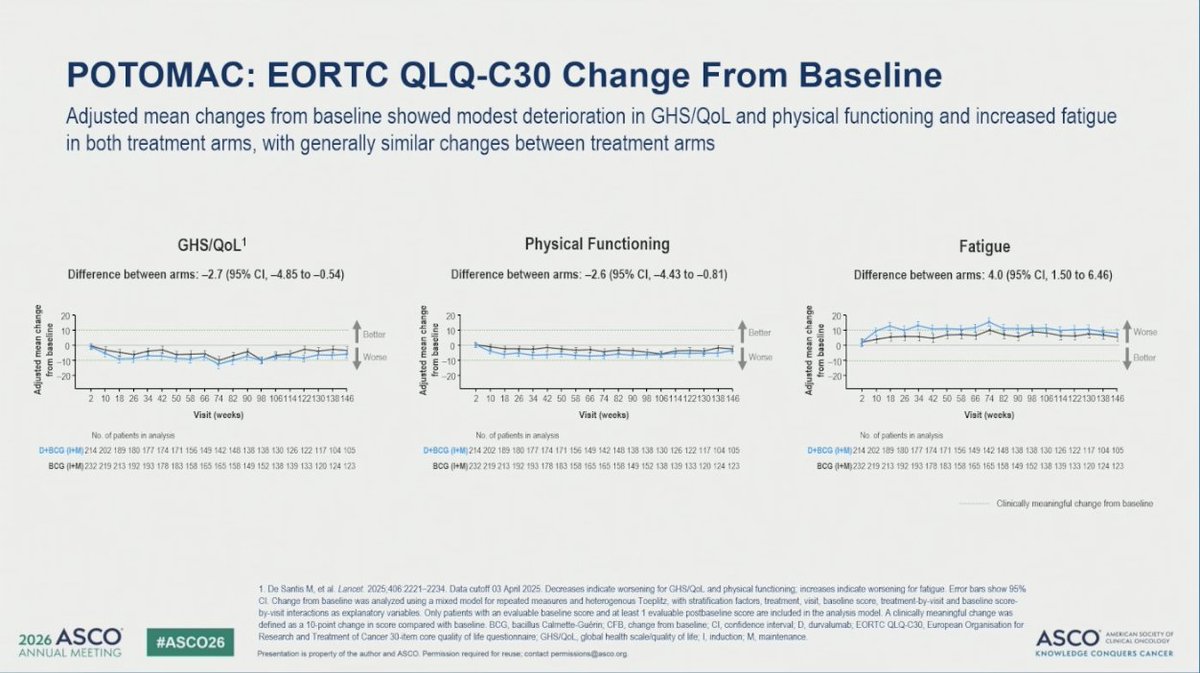
👥 PROs similar between arms; no meaningful QoL difference
Why this matters for your practice:
💡 OS may look equivalent because cystectomy is effective salvage but avoiding that surgery is the point. A regimen that delays or prevents recurrence without OS harm or QoL cost is worth the conversation.
#BladderCancer #NMIBC #GUOnc #ASCO26
2
5
11
1,457
Dillon Cockrell, MD retweeted
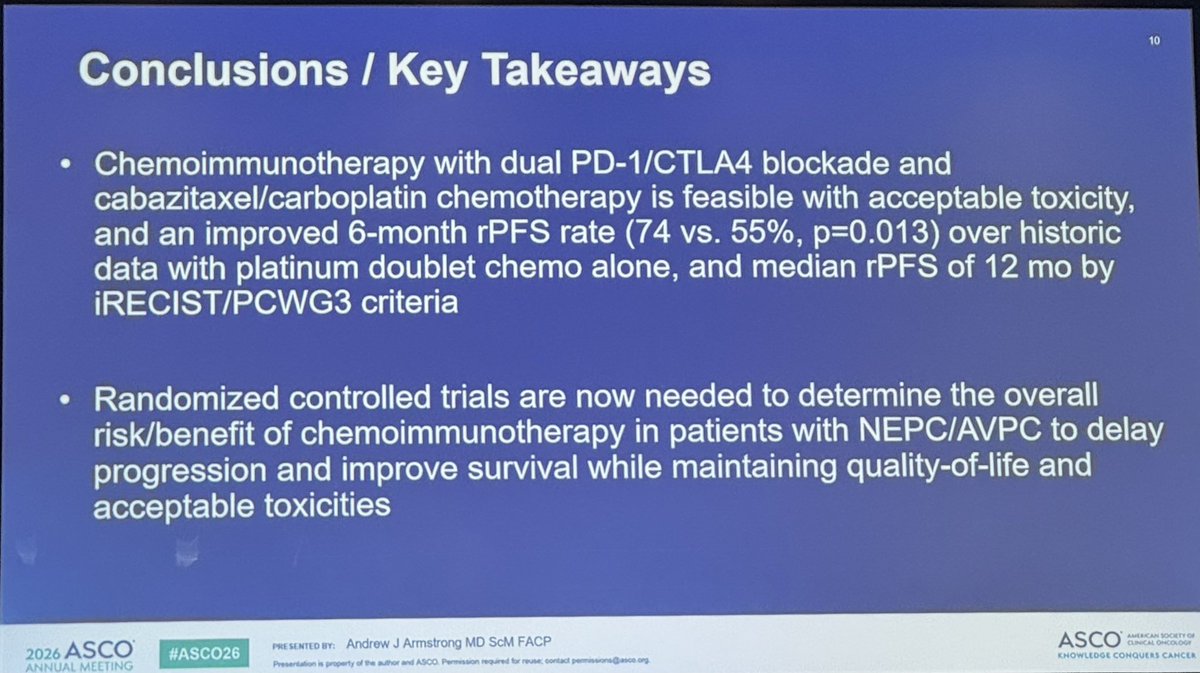
CHAMP met its primary endpoint: 6-month PFS 74% vs 55% historical control, with 23% 2-year survival in a population where platinum-taxane alone rarely gets patients past a year.
The randomization question is the right question. Single-arm with historical comparator is often the only feasible design when you’re enrolling NEPC/AVPC, but it makes regulatory translation hard. A randomized phase 2 would require network coordination and sustained sponsor commitment to a rare, rapidly progressing population. Worth pushing for.
This is the most actionable data we have in this space. Well done to the Duke team.
@AarmstrongDuke @DukeGUCancer
#ProstateCA #GUonc #ASCO26

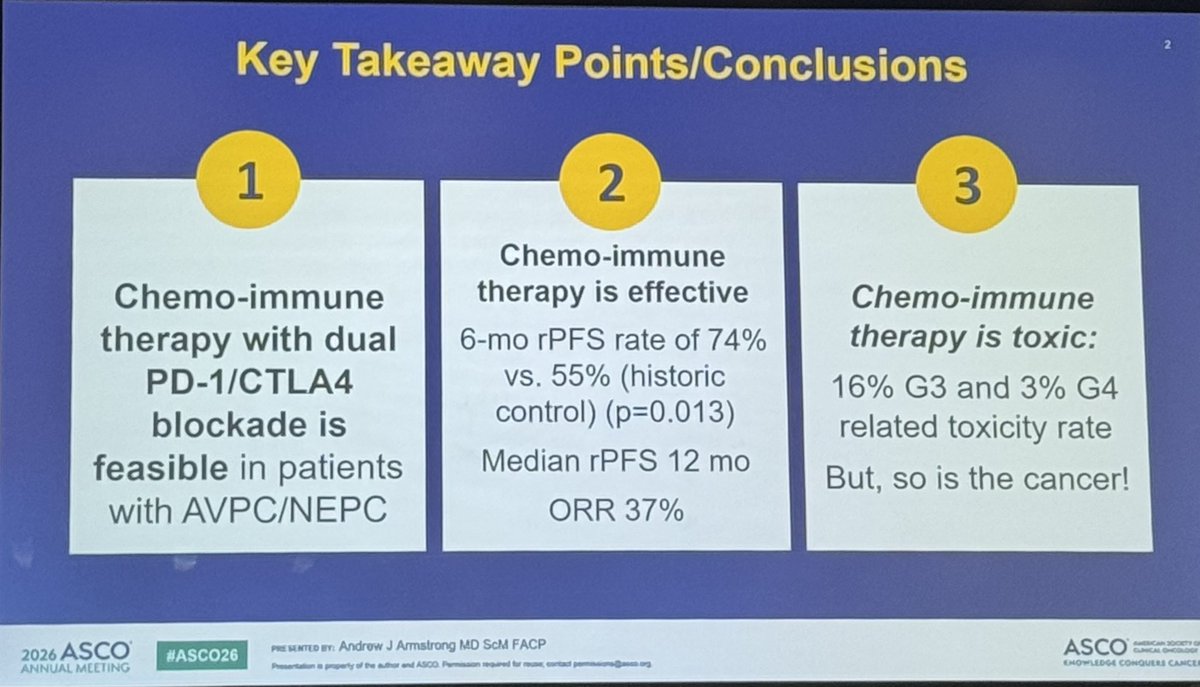
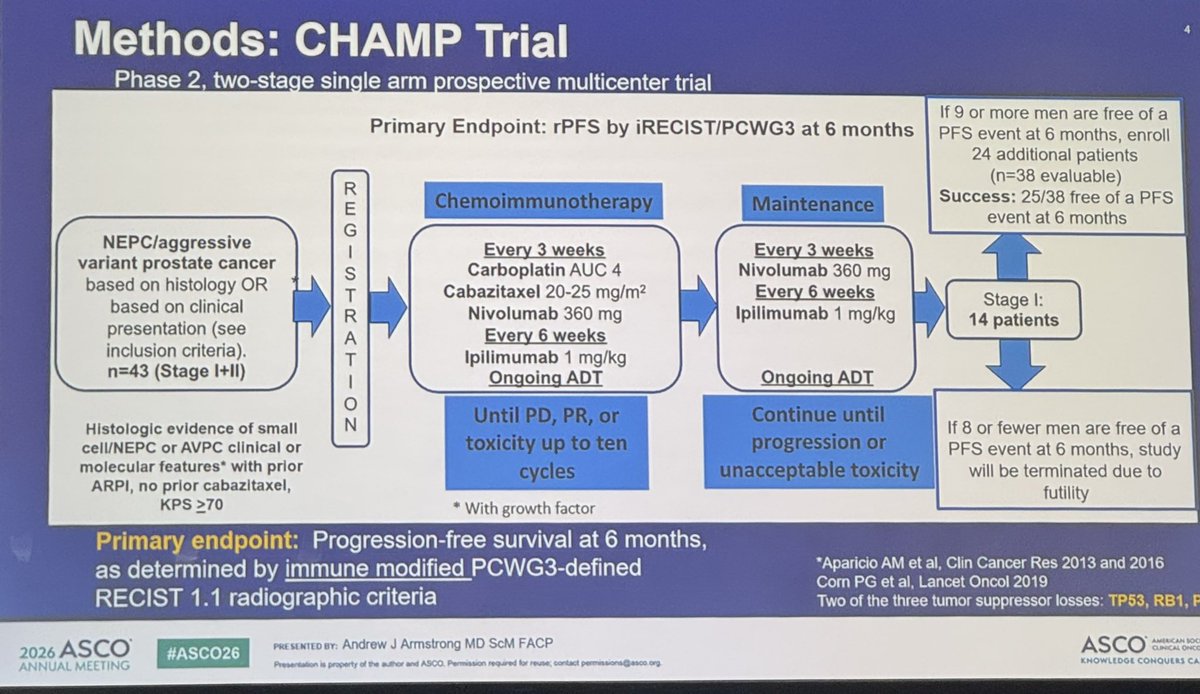
#CHAMP is an important trial led and presented by @AarmstrongDuke from our @DukeGUCancer team evaluating chemoIO with cabazitaxel/carboplatin and ipilimumab/nivolumab in patients with aggressive variant or neuroendocrine metastatic #ProstateCancer. Maintenance IO continued after up to 10 chemo cycles.
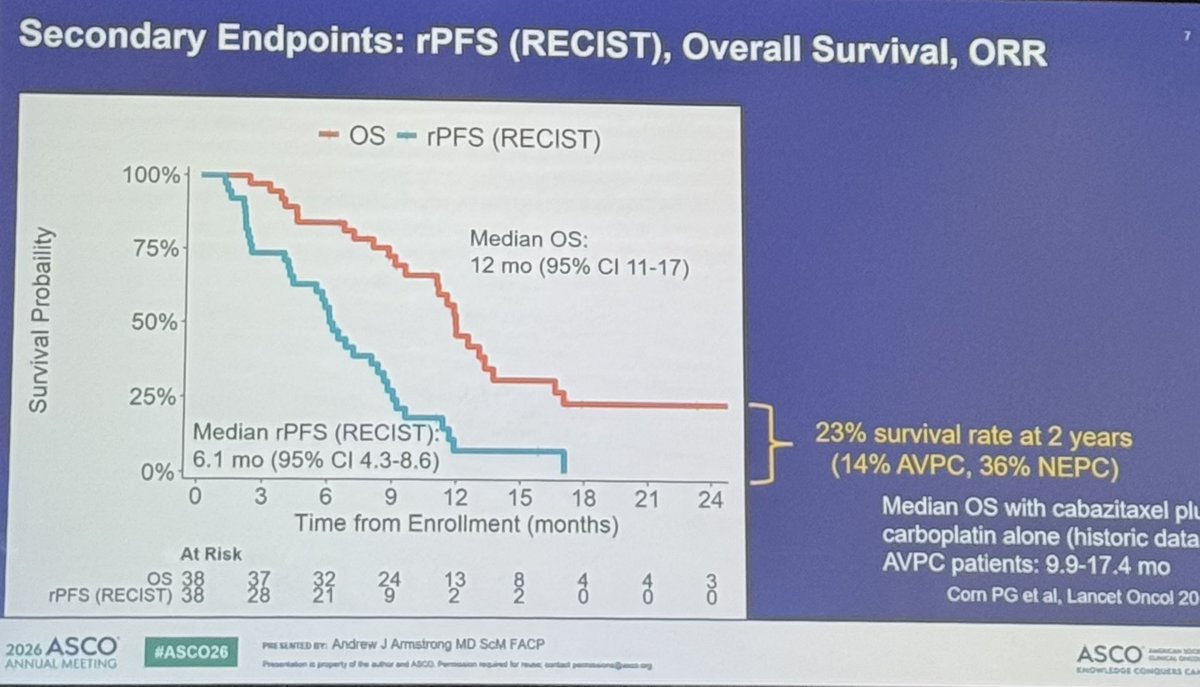
Met primary endpoint of 6 mo PFS 74% vs 55% historic carbo/cabazi with expected but manageable toxicity. 23% survival at 2 years is much better than historical data. Two patients alive and off therapy at 30 months!
Aggressive treatment for aggressive disease, but shows chemoIO should be considered as SOC for these patients with historical poor outcomes.
#ASCO26 @DukeCancer @Daniel_J_George @hannahdzmd @MRHarrisonMD @MattLabsMD @OncoDailyGU @OncoAlert @urotoday @oncodaily
7
7
1,305
Dillon Cockrell, MD retweeted

May 31
Dear Colleagues at #ASCO26
@OncoAlert 🚨Straight from the podium to your Feed, Proud to have @AarmstrongDuke 🇺🇸from Duke Cancer Institute discussing:
Phase 2 multicenter trial of chemoimmunotherapy for patients with neuroendocrine or aggressive variant metastatic prostate cancer (CHAMP). Just presented at #ASCO26
The phase II CHAMP trial demonstrated promising activity of cabazitaxel, carboplatin, ipilimumab, and nivolumab in metastatic neuroendocrine and aggressive-variant #ProstateCancer . The regimen achieved a 78% 6-month radiographic PFS rate and median rPFS of 12 months, outperforming historical platinum chemotherapy benchmarks, with manageable toxicity and durable responses in select patients.
@AarmstrongDuke @DrLaurenFHoward @DrChrisHoimes @LandonBrownMD @cnsternberg @aaparicioMD @BSiddiquiMD @Daniel_J_George
Ping OncoAlert Faculty
@montypal @crisbergerot @DrDanielHeng @apolo_andrea @DrChoueiri @PGrivasMDPhD @TiansterZhang @HHammersMD @ravikanesvaran @neerajaiims @amerseburger @sonpavde @drenriquegrande @scserendipity1 @Silke_Gillessen
@EfstathiouEleni @tompowles1 @BraunMDPhD @nataliagandur @cdanicas @brian_rini @AOmlin
@yekeduz_emre @DrYukselUrun @scocmem @AmandaNizamMD @weoncologists
1
9
17
3,541
#CHAMP is an important trial led and presented by @AarmstrongDuke from our @DukeGUCancer team evaluating chemoIO with cabazitaxel/carboplatin and ipilimumab/nivolumab in patients with aggressive variant or neuroendocrine metastatic #ProstateCancer. Maintenance IO continued after up to 10 chemo cycles.
Met primary endpoint of 6 mo PFS 74% vs 55% historic carbo/cabazi with expected but manageable toxicity. 23% survival at 2 years is much better than historical data. Two patients alive and off therapy at 30 months!
Aggressive treatment for aggressive disease, but shows chemoIO should be considered as SOC for these patients with historical poor outcomes.
#ASCO26 @DukeCancer @Daniel_J_George @hannahdzmd @MRHarrisonMD @MattLabsMD @OncoDailyGU @OncoAlert @urotoday @oncodaily
4
8
1,874
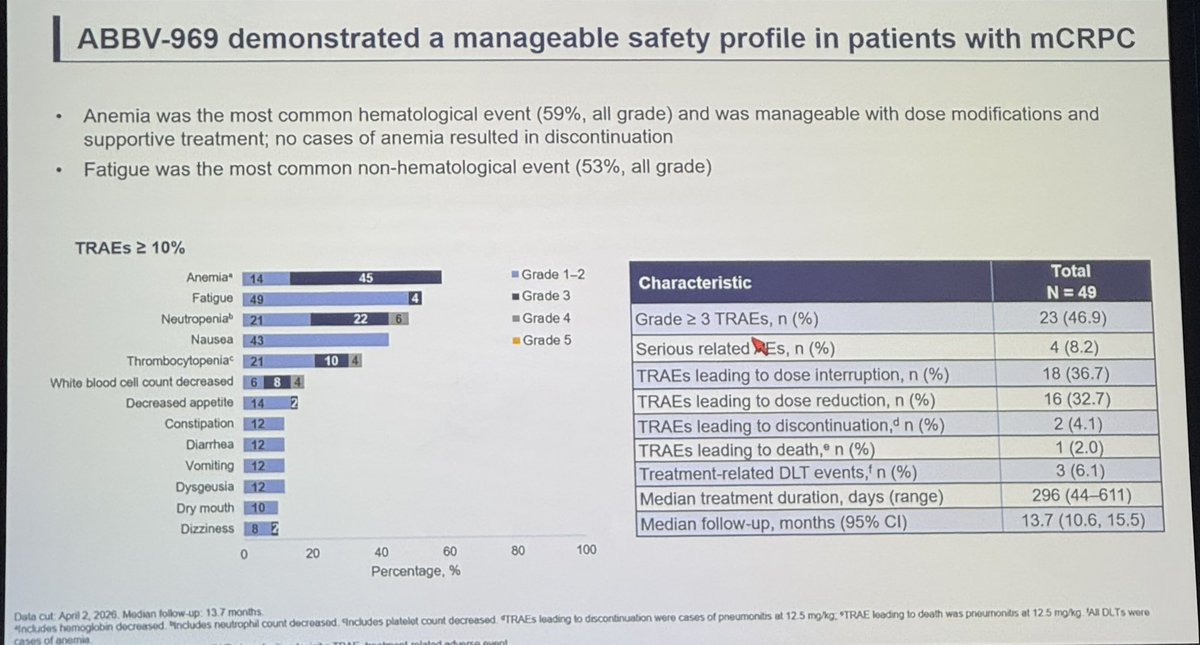
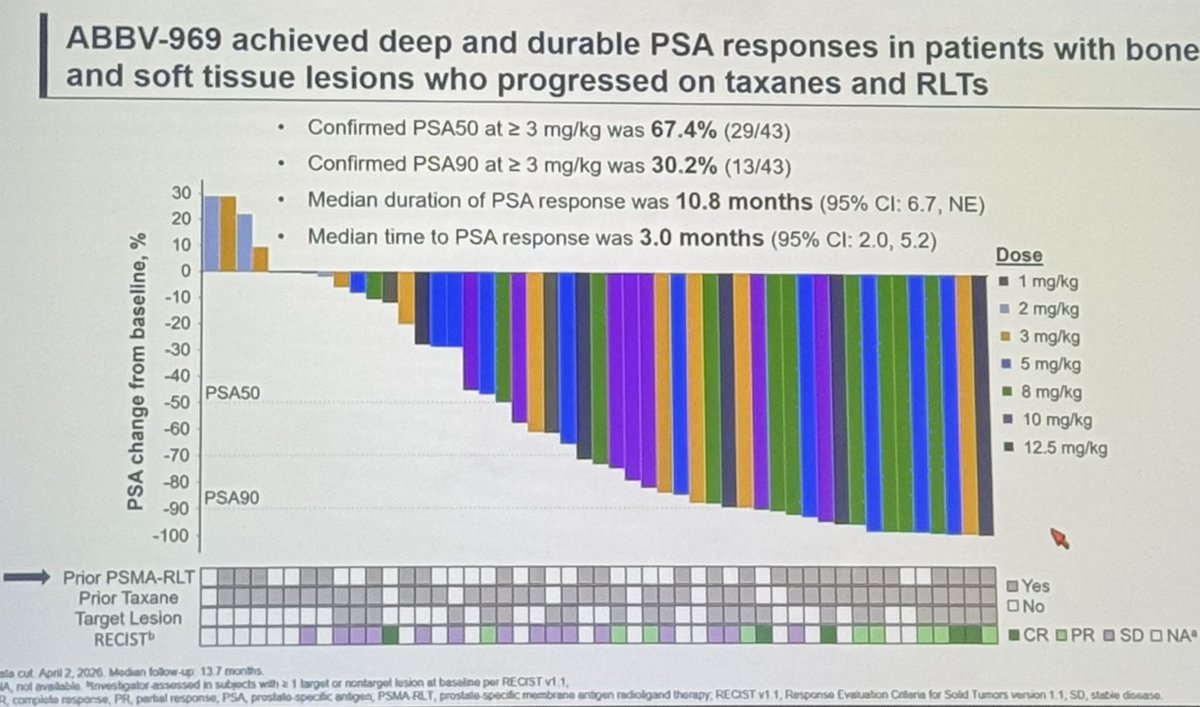
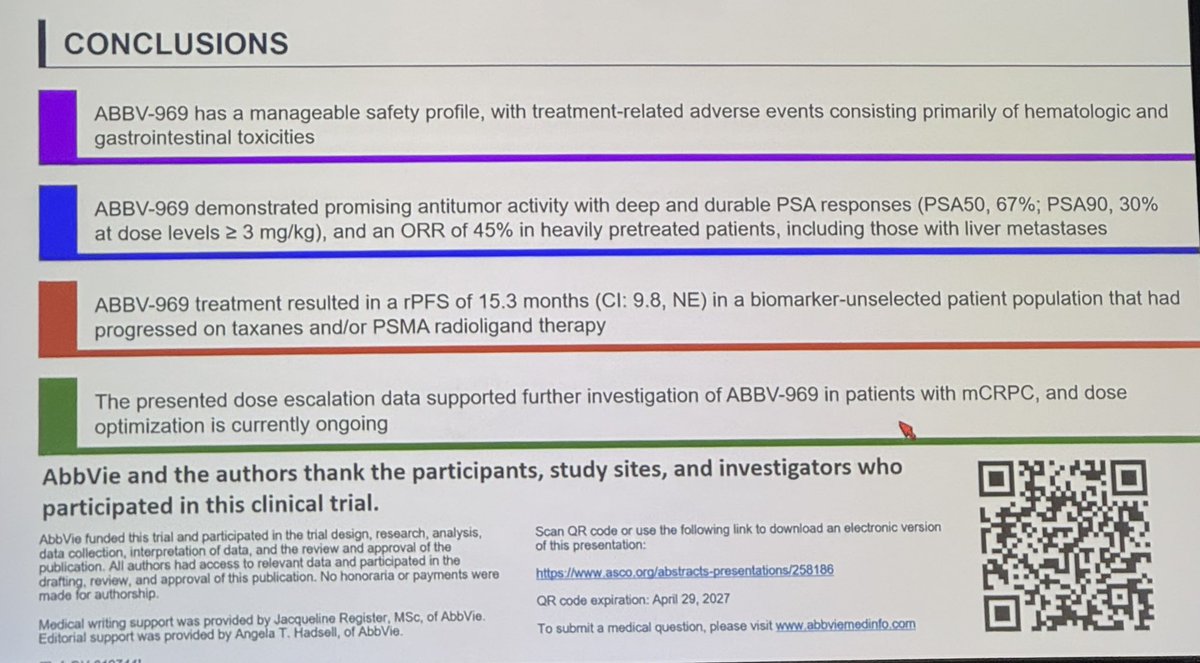
ABBV-969 is a PSMA-STEAP1 ADC with #ASCO26 phase 1 (n=49) data in mCRPC (prior taxane and ARPI required). Heavily pretreated cohort. Hematologic and GI toxicity most relevant at high doses.
Impressive PSA and radiographic responses. This looks like a viable future ADC treatment option for #ProstateCancer patients, albeit with expected toxicity. Great presentation by @TDorffOnc.
@OncoAlert @OncoDailyGU @urotoday @GUOncologyNow
1
12
31
4,066
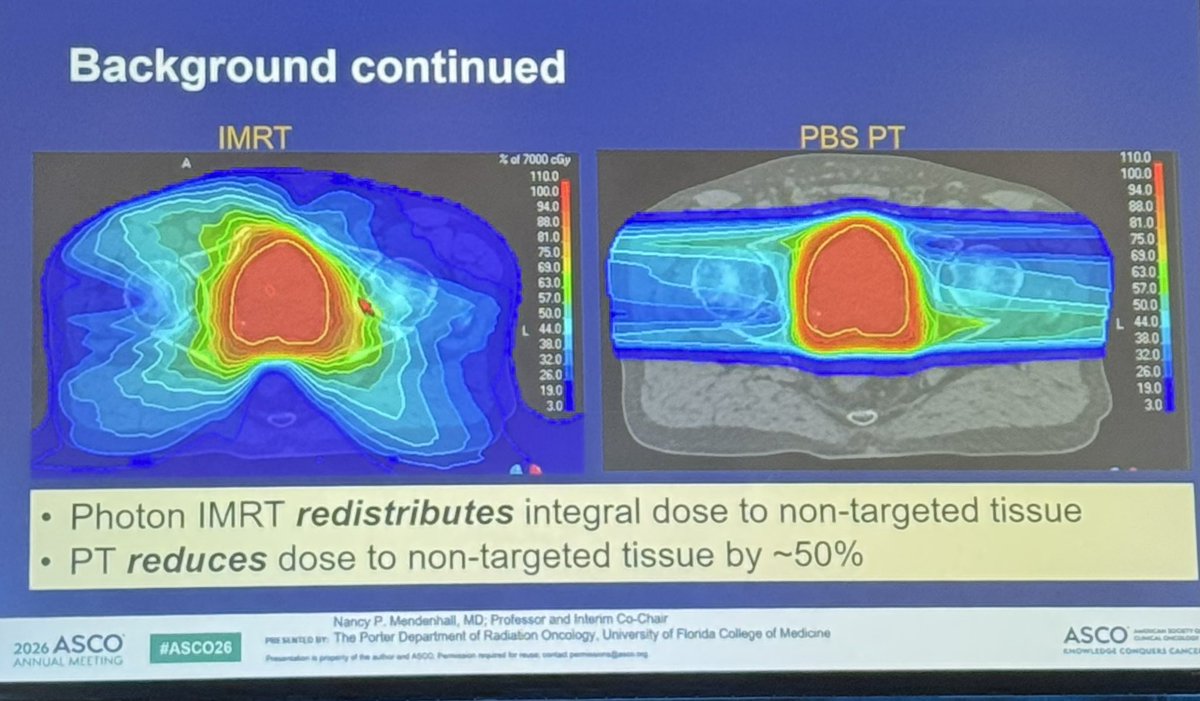
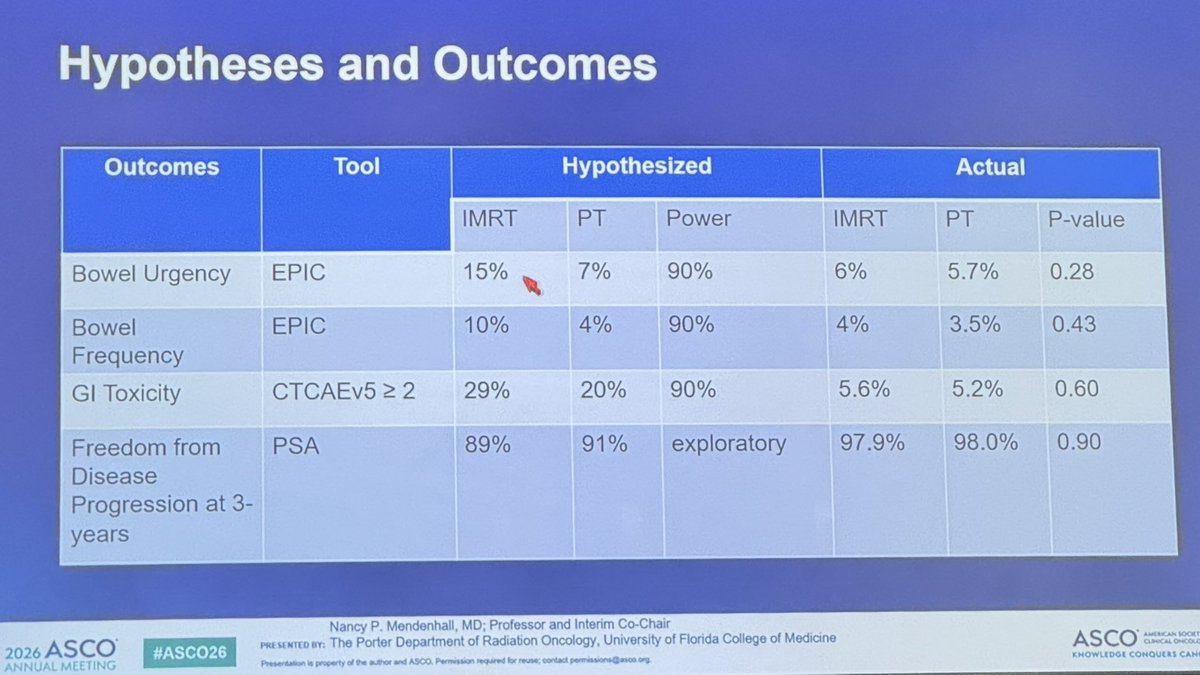
#COMPPARE is a large non-randomized study evaluating proton therapy vs IMRT for localized #ProstateCancer.
➡️ No significant difference in bowel toxicity or longterm outcomes.
👉 Rectal spacer use has led to minimal GI toxicity either way and should be incorporated. #ASCO26 @urotoday @OncoDailyGU @OncoAlert @GUOncologyNow
6
6
552
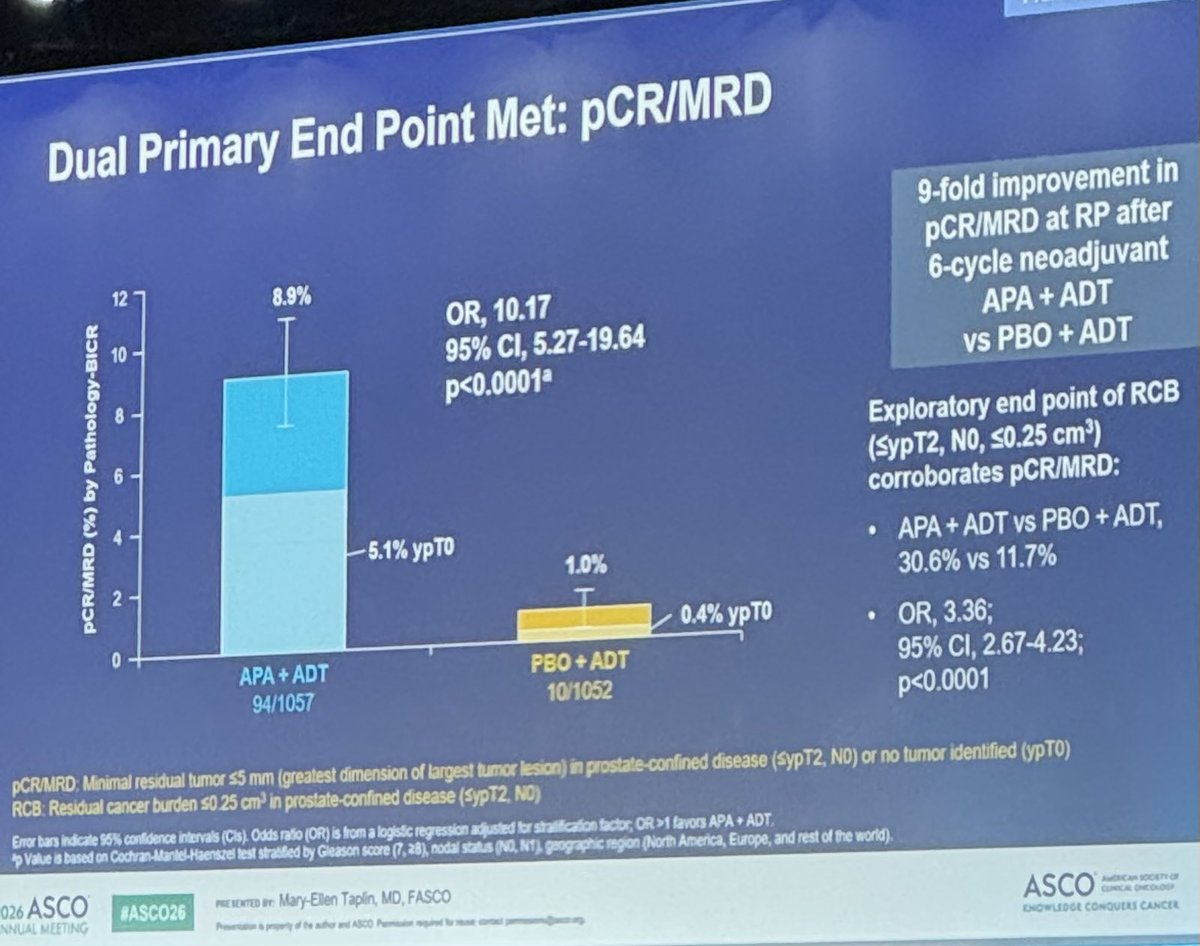
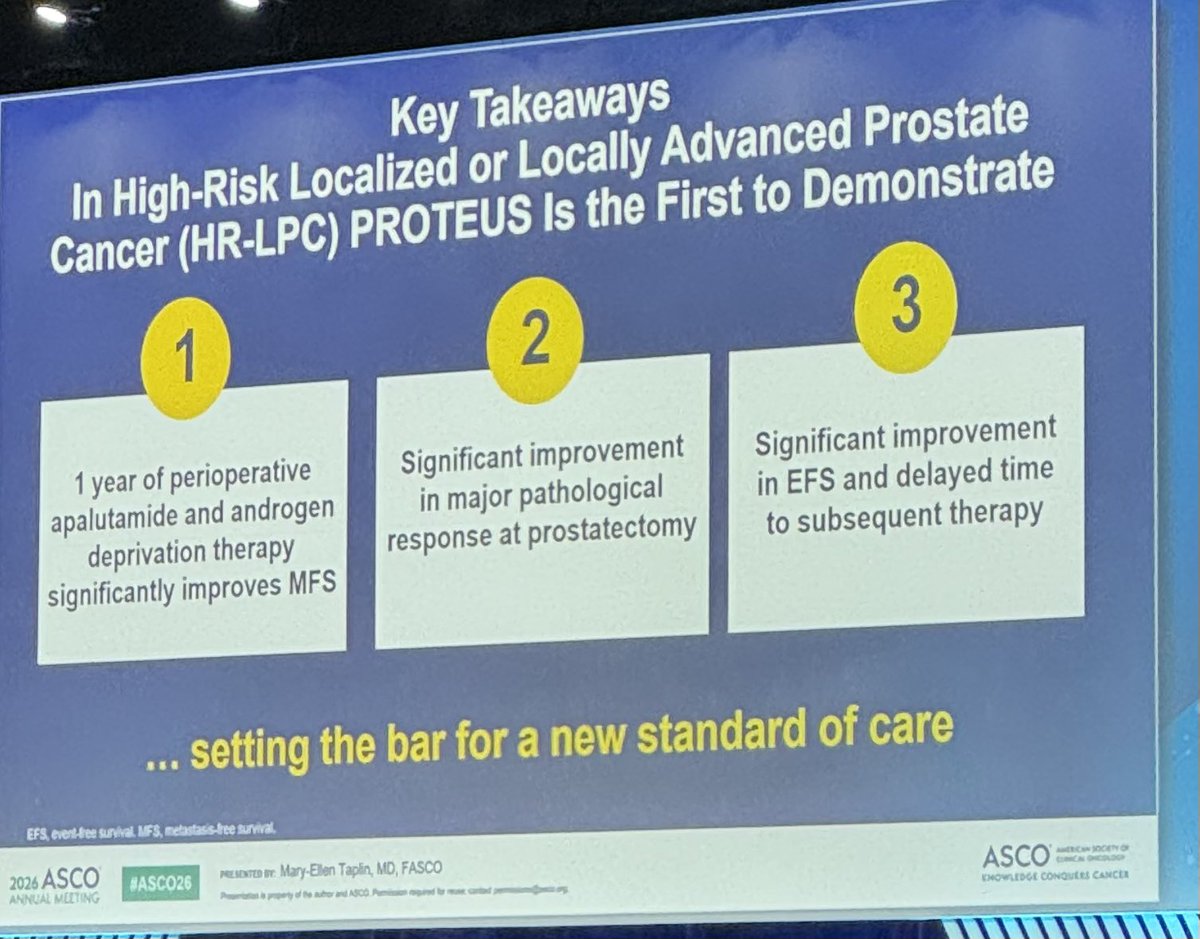
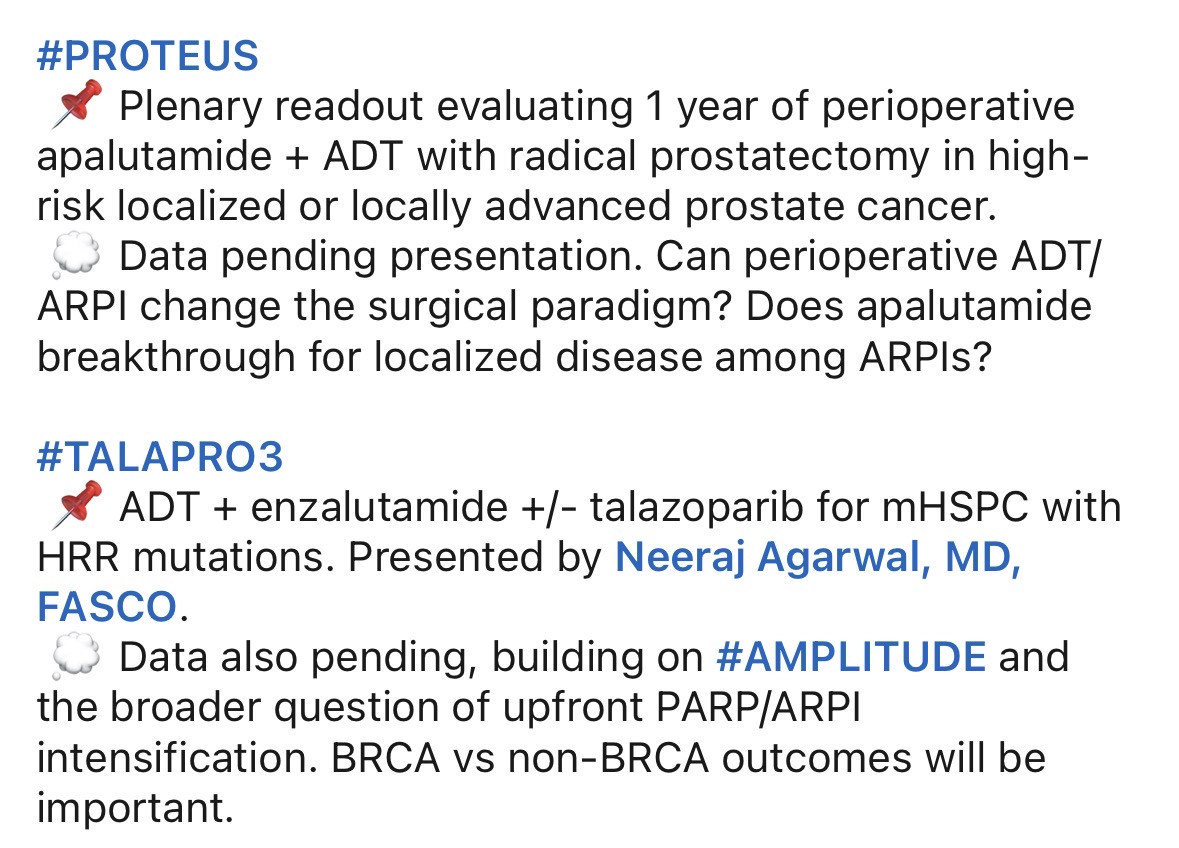
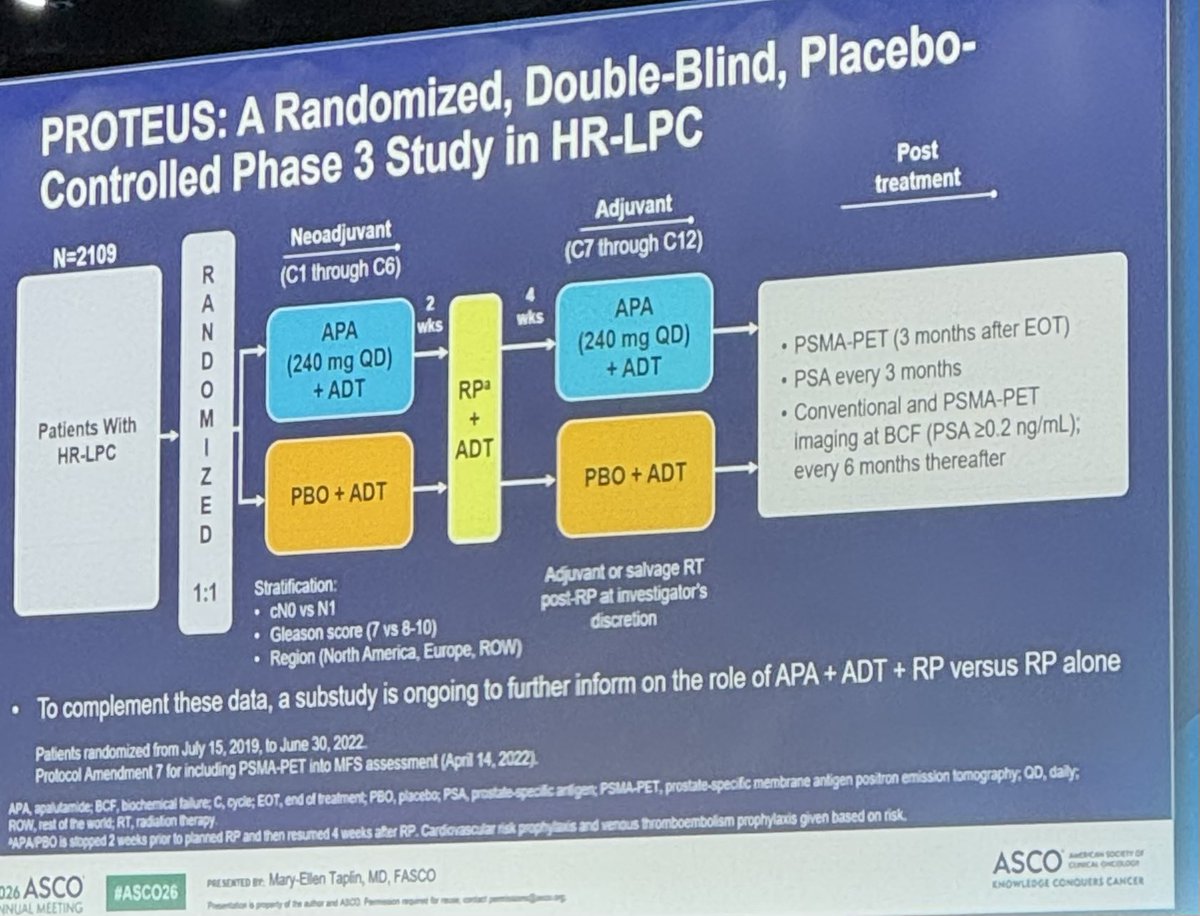
#PROTEUS is a plenary presentation at #ASCO26 and an important localized prostate cancer study.
Among 2,109 patients with high-risk localized/locally advanced disease undergoing radical prostatectomy, perioperative apalutamide ADT improved both co-primary endpoints, including MFS.
But the discussion coming out of this study will likely focus as much on the trial design as the positive results.
@OncoAlert @OncoDailyGU @urotoday @GUOncologyNow @oncodaily
1/4
1
4
13
2,039
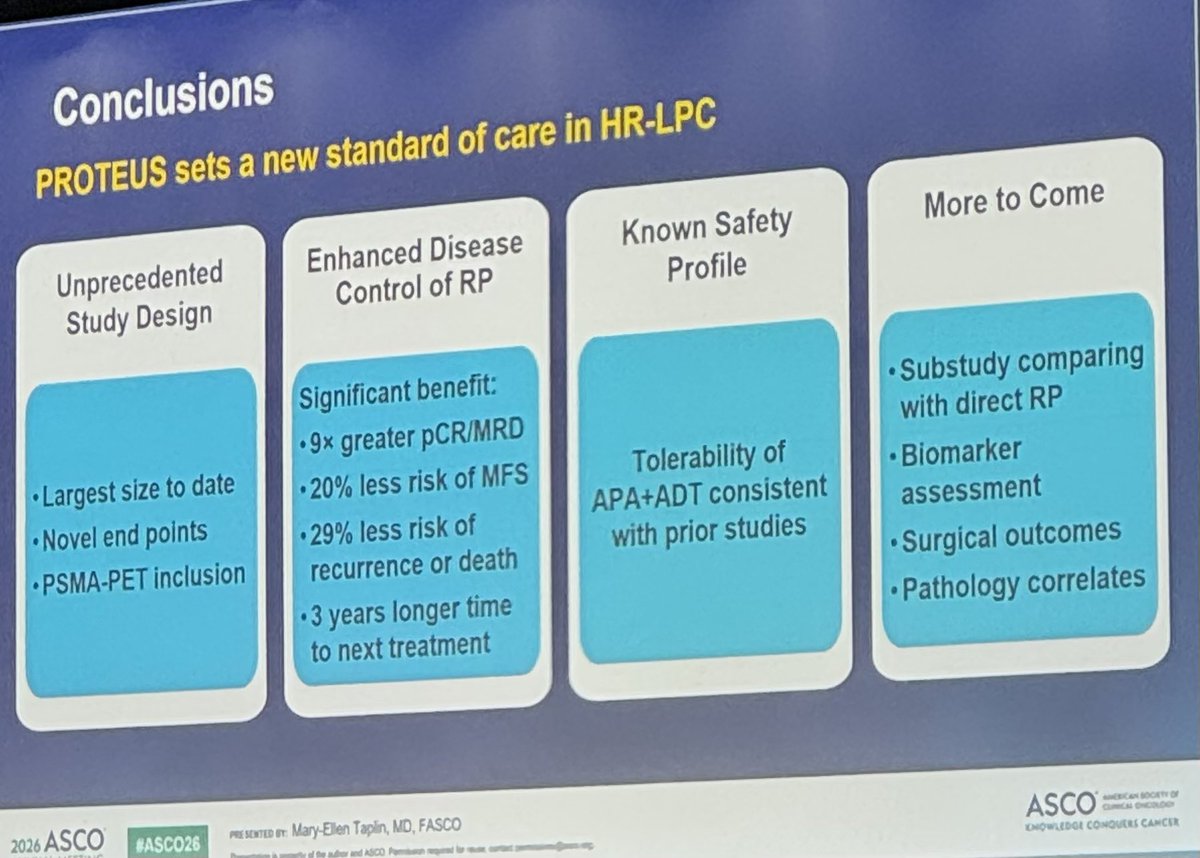
#PROTEUS data will likely influence practice in the future, particularly for patients with high-risk disease who strongly prefer surgery. A year of ADT/ARPI is less hormone therapy than the 2 years we use with radiation and likely results in better testosterone recovery.
We will need to see the ongoing substudy against RP alone as the better comparator. Eventually, a trial comparing this approach to radiation and long-term ADT with QOL metrics will be the most informative.
#ASCO26 @urotoday @OncoDailyGU @OncoAlert @GUOncologyNow @PCFnews
4/4
1
1
317
My (maybe) last take on #PROTEUS: an apalutamide alone arm would’ve been a better design.
For patients with high risk prostate cancer, many choose RT to avoid incontinence but the ones who choose surgery do so to hopefully avoid ADT. ARPI alone has activity and could have improved surgical outcomes while offering a chance to maintain testosterone with longterm cure.
#ASCO26 @urotoday @OncoDailyGU @Daniel_J_George @AarmstrongDuke @hannahdzmd @OncoAlert @GUOncologyNow
1
3
321
Dillon Cockrell, MD retweeted
May 31
The #ADREAM trial from #ASCO26 offers insight into time off therapy for patients with metastatic prostate cancer and great response to ADT/ARPI. Important data from @ALLIANCE_org. @hannahdzmd @DCockrellMD @DukeGUCancer @AarmstrongDuke @DukeCancer
4
17
2,455
Dillon Cockrell, MD retweeted

May 31
25 Posts Not To Miss From ASCO 2026 Day 2
@ASCO @ConquerCancerFd @SergeyBadalyan1 @shhovsepyan @fuatbcr @SPremji7866 @montypal @tompowles1 @TalhaBadarMD @drsarahsam @SuyogCancer @ErikaHamilton9 @ThinkingCancer @BartsECMC @BethN01 @DCockrellMD @theNCI @JasmineKambojMD @ArmandOrlandi @YJanjigianMD @JAMouabbi @weldeiry
oncodaily.com/not-to-miss/no…
#OncoDaily #ASCO26

1
7
8
607
#ADREAM: ADT/ARPI stopped after 18 months for mHSPC patients with PSA <0.2.
After being off treatment for 18 mo, 67% recovered T and 41% were still off ADT/ARPI with T recovery with median 24 mo off treatment. Meaningful data we can bring home from #ASCO26 to share with patients in clinic.
@Daniel_J_George @hannahdzmd @urotoday @OncoDailyGU @OncoAlert @AtishChoudhury @ALLIANCE_org @AarmstrongDuke @DukeGUCancer
May 31

The #ADREAM trial from #ASCO26 offers insight into time off therapy for patients with metastatic prostate cancer and great response to ADT/ARPI. Important data from @ALLIANCE_org. @hannahdzmd @DCockrellMD @DukeGUCancer @AarmstrongDuke @DukeCancer
6
9
984
Dillon Cockrell, MD retweeted

May 31
Talazoparib Treatment Delays Cancer Growth in Advanced Prostate Cancer - Dillon Cockrell
@DCockrellMD
oncodaily.com/voices/dillon-…

2
3
52
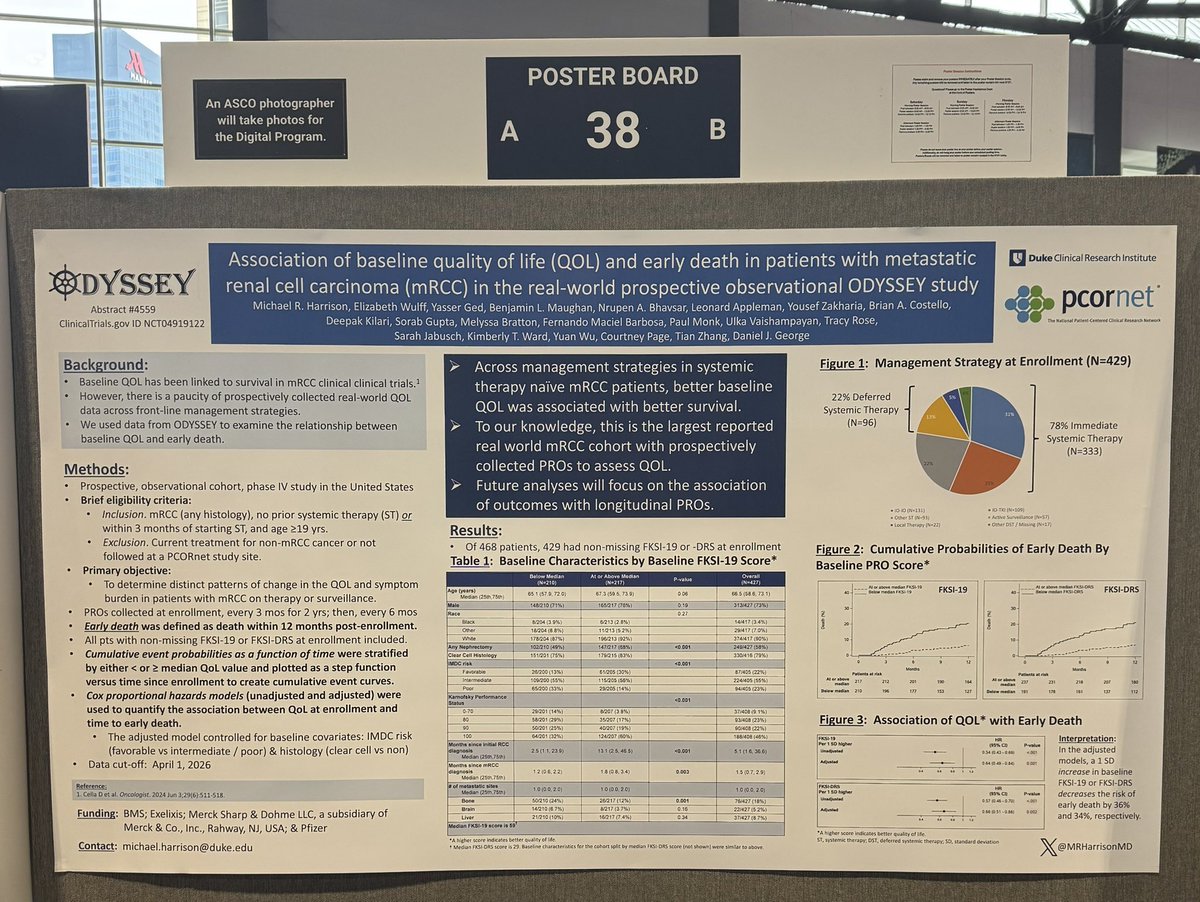
Here at #ASCO26, @MRHarrisonMD reports data from the prospective #ODYSSEY study showing that baseline patient-reported quality of life is strongly associated with early mortality in treatment-naïve mRCC.
For every 1 SD increase in baseline QOL:
➡️ FKSI-19: 36% lower risk of early death (adjusted HR 0.64, p=0.002)
➡️ FKSI-DRS: 34% lower risk of early death (adjusted HR 0.66, p=0.002)
Important reminder that PROs may provide meaningful prognostic information beyond traditional clinical factors.
@Daniel_J_George @DukeGUCancer @TiansterZhang @KidneyCancer @OncoDailyGU @OncoAlert @urotoday
4
7
651
Dillon Cockrell, MD retweeted
May 31
The #ASCO26 Day 2 RoundUp from
@OncoAlert 🚨For the FULL NEWSLETTER👉 buff.ly/25YHTzM
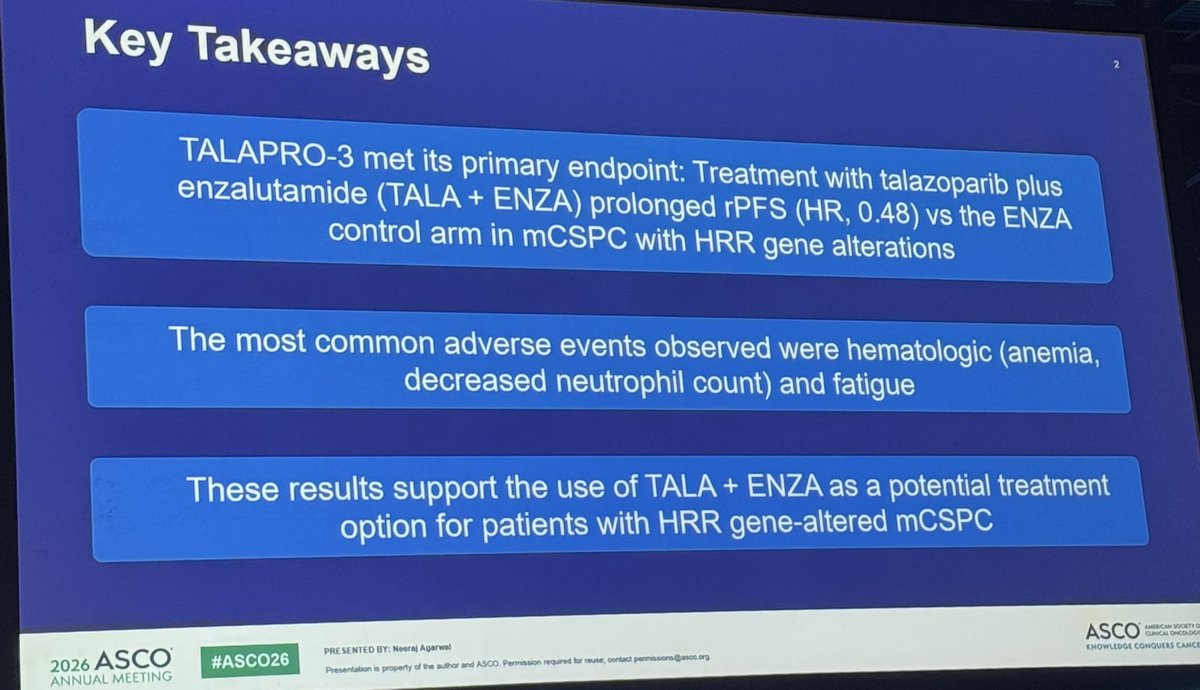
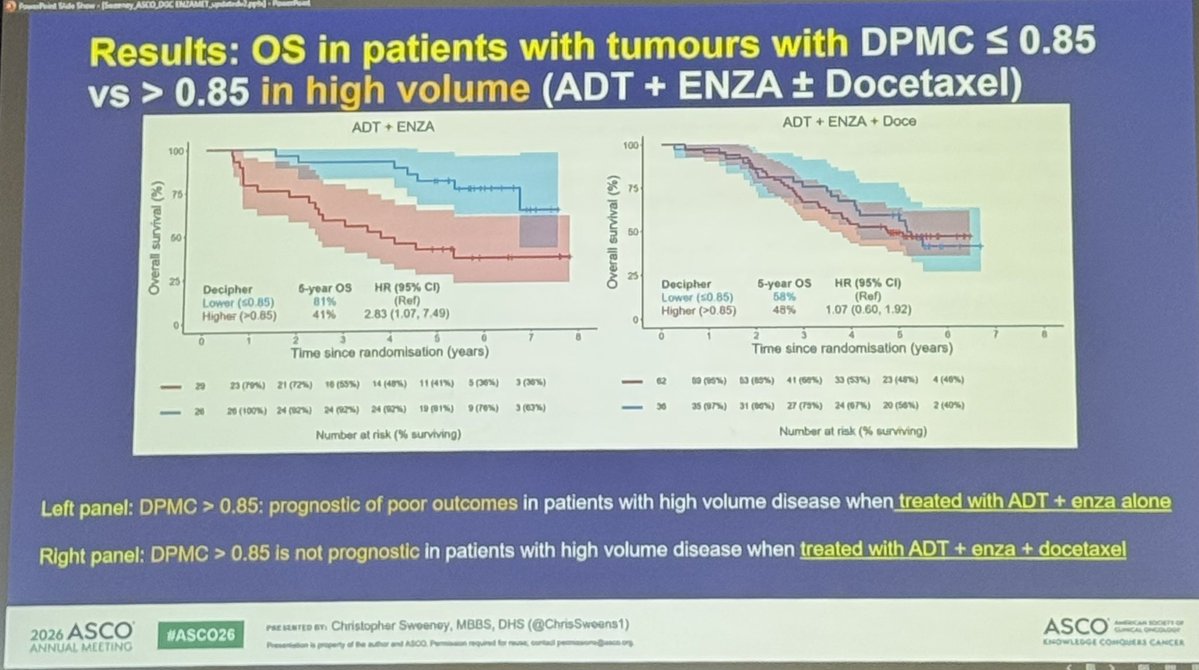
✅TALAPRO-3 (mHSPC, HRR ): talazoparib enzalutamide improved 3-yr PFS (77% vs 56%), 52% risk reduction; anemia increased
✅ RAMPART (RCC): durvalumab alone negative; durvalumab tremelimumab improved DFS → dual IO signal
✅ SENOMAC (breast): axillary dissection safely omitted in 1–2 sentinel node macrometastases; less morbidity, same survival
✅OPTIMA (breast): PAM50-guided approach supports chemo de-escalation, including selected node and premenopausal patients
✅ KEYNOTE-522 (TNBC): durable OS benefit with pembro chemo (85% vs 77% at ~8 years)
@DCockrellMD @zapatalaguadomd @jgong15 @montypal @TiansterZhang @tompowles1 @docjavip @katy_beckermann @RKSayyid @GlopesMd @Noah_Onc @DrChoueiri @hoperugo @DrJudyBoughey @OncBrothers @DrRishabhOnco @drsarahsam @teamoncology @ErikaHamilton9 @to_be_elizabeth @ElisaAgostinett @kazuki_nozawa @ArmandOrlandi @Dr_ElvinaA @OmarOnco @DrSGraff @YAbdouMD
1
12
25
6,339