
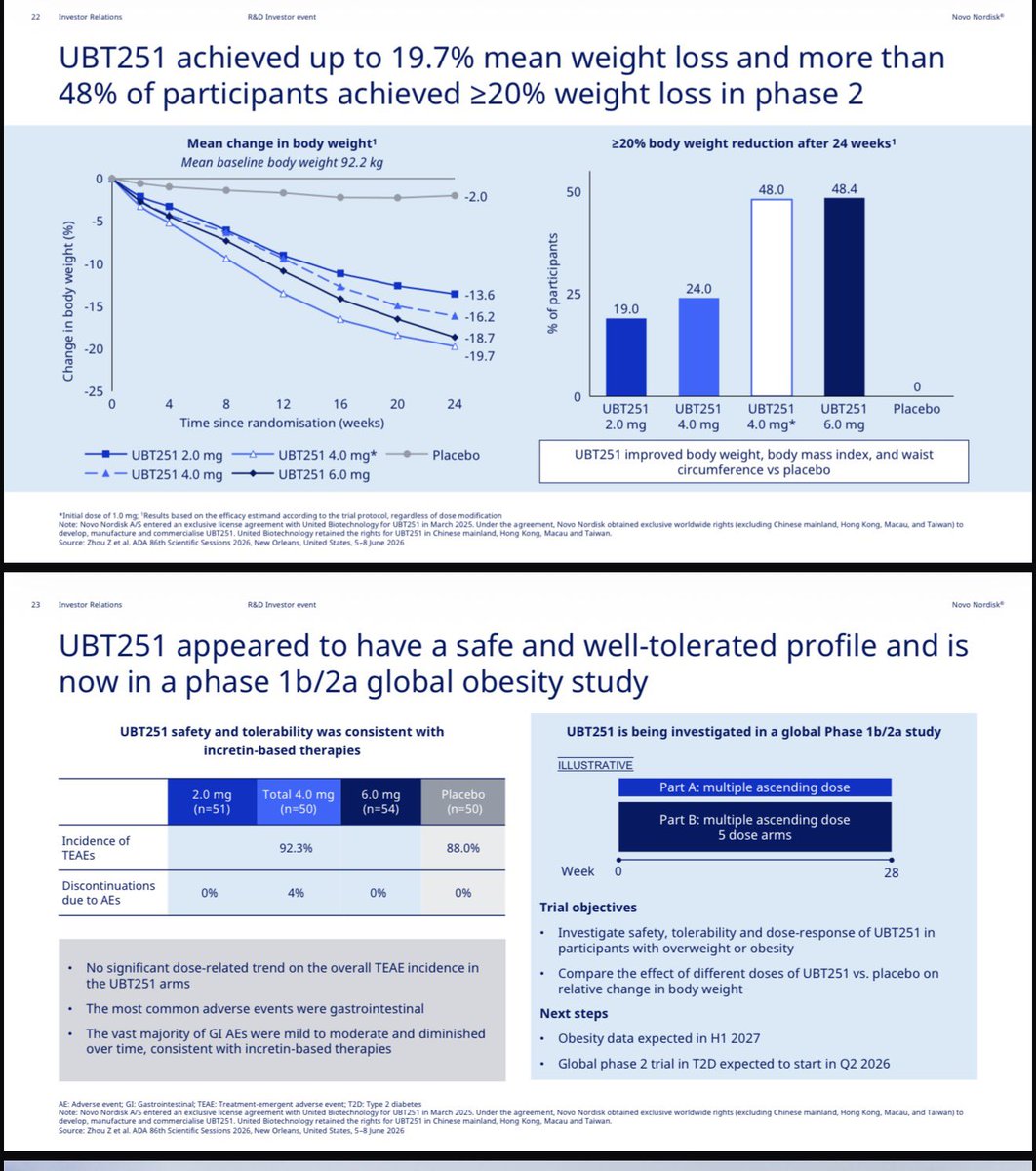
Another look at $NVO GGG UBT251 given novo crowd repeated posting on it
1- it was one step escalation trial in China so no wonder good wt loss and hiding of tolerability
2-novo is running global trial in which it is repeating MAD like dosing. It looks the optimal dosing -escalation is not determined yet. This is a very long term play
3- we don’t even know how many pts in each arm ?
4- low mg suggests a molecule based on Oxyntomodulin rather than GIP ( $LLY retatrutide is built on GIP backbone ) which may bias UBT more towards glucagon vs GIP ? This could harm efficacy / tolerability balance.
I think novo team is buying time here and fully aware this will not provide any help at least near term.


Don’t know what’s happening behind closed doors with $NVO but novo , $ABBV and others will not sit down and watch $LLy taking the whole obesity for next few years with tens of billions in revenues.. there are no other BD deals that even come close
What is clear is $PFE $AMGN and likely Roche will not take more than tiny part of market due to non competitive offerings.
Something has to give in this year. Laws of physics and entropy dictate that.
4
359

23m
@MaryanneDemasi Exactly right. A mere 0.8% absolute reduction in flu-like illness (2.8% → 2.0%) does not justify a 6-fold spike in severe reactions disrupting daily life.
The data superiority of protein-based vaccines like Novavax’s is obvious — yet captured regulators keep sidelining it. FDA previously refused to even review Moderna’s mRNA flu shot for using a substandard comparator instead of high-dose benchmarks for seniors. Now they appear ready to approve on essentially the same weak evidence? This flip-flop highlights the pattern.
Novavax did it properly. In the Phase 3 CIC trial (NCT06291857, adults ≥65):
• Standalone tNIV and COVID-Influenza Combination delivered robust responses (2.4-5.7-fold rises) comparable/superior to Fluzone High-Dose and standalone Nuvaxovid.
• True single-dose co-formulated potential.
• Excellent tolerability: >98% solicited AEs mild/moderate, reactogenicity matching authorized comparators, no new safety signals.
Contrast that with mRNA flu combos struggling on non-inferiority (e.g., Pfizer’s B-strain shortfalls) and higher reactogenicity from LNPs.
The only real mRNA advantage has been speed to market — not superior efficacy, safety, or durability. Is speed worth compromising safety, especially when protein platforms with Matrix-M have consistently shown stronger, cleaner results across trials?
This ongoing favoritism toward mRNA despite the evidence raises serious questions about regulatory capture over public health. Novavax’s protein technology deserves priority — the data has been clear.
#Novavax #FluVaccine #VaccineSafety @SecKennedy
1
14

🌟 Exciting news! Eli Lilly's retatrutide has shown up to 30.3% average weight loss in the Phase 3 TRIUMPH-1 trial! While efficacy shines, analysts are eyeing its tolerability. The future of obesity treatment is here! #Research #Peptides @ez_peptides
8

Not necessarily. More frequent dosing is better so monthly will be inferior to biweekly, as far as effectiveness and tolerability. But monthly will probably be similar to tirz biweekly which people are doing now just fine (to save money).
1
4
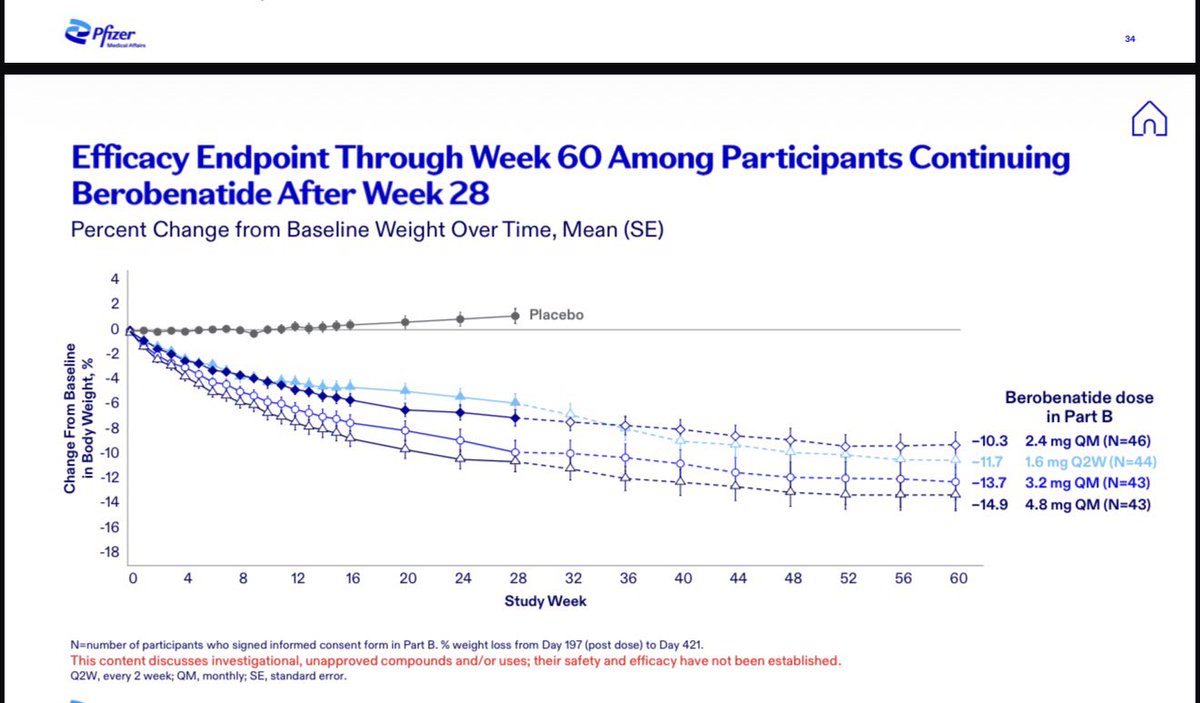
Got this slide from $PFE ADA presentation .. they show $NVO 7.2 mg sema with same efficacy or better than $LLY TZP. I discussed the unequal control 2.4 mg sema performance in previous posts that shows 7.2 mg is way inferior to TZP on efficacy and tolerability. How could Pfizer not put together a coherent basic literature comparison? They seem just wanting to trash TZP ?
And look at 60 wk Vesper 1 wt loss despite no escalation in dose ? How does Mr Bourla continue to equate this GLP1 with TZP performance ?

Jun 6
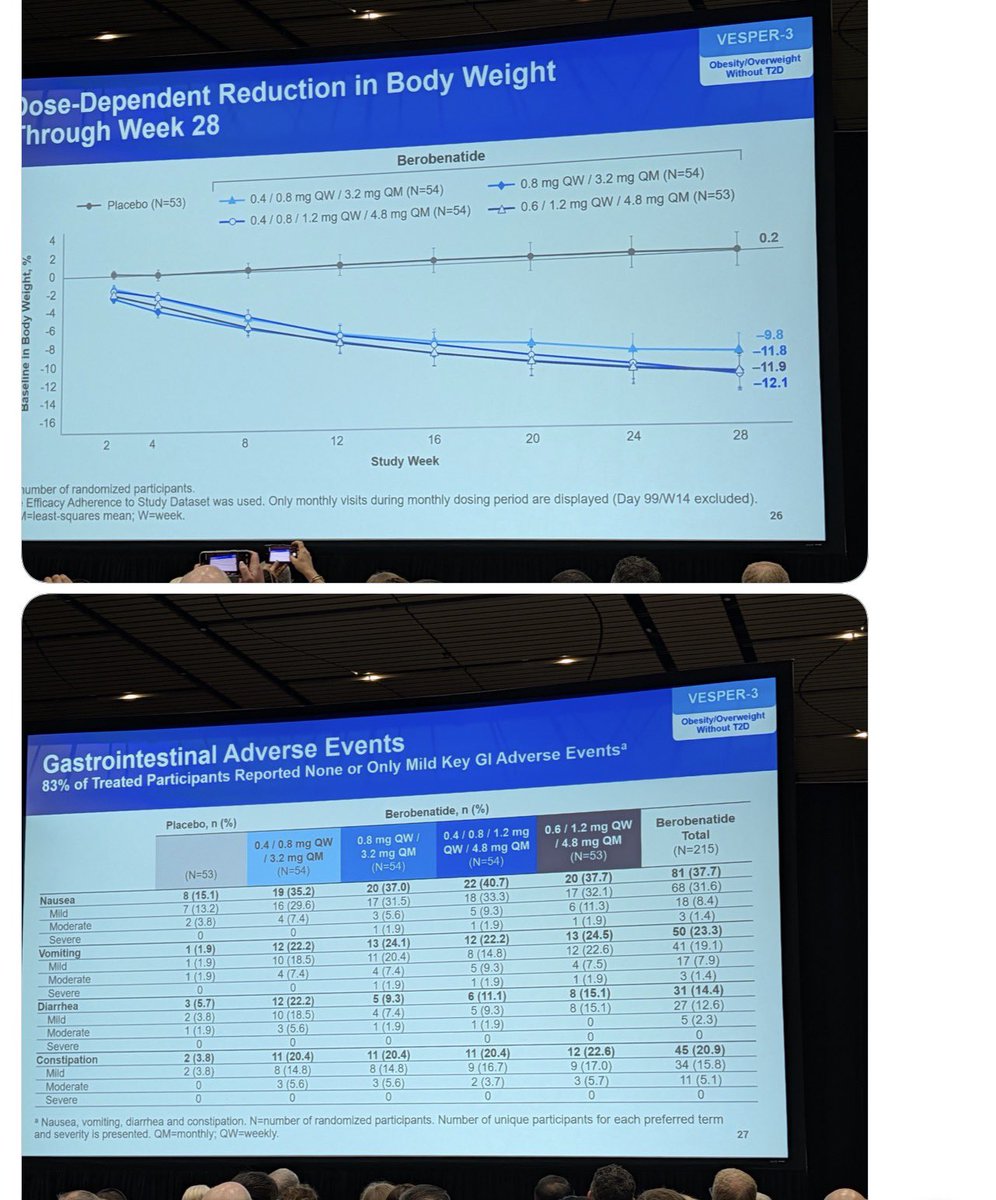
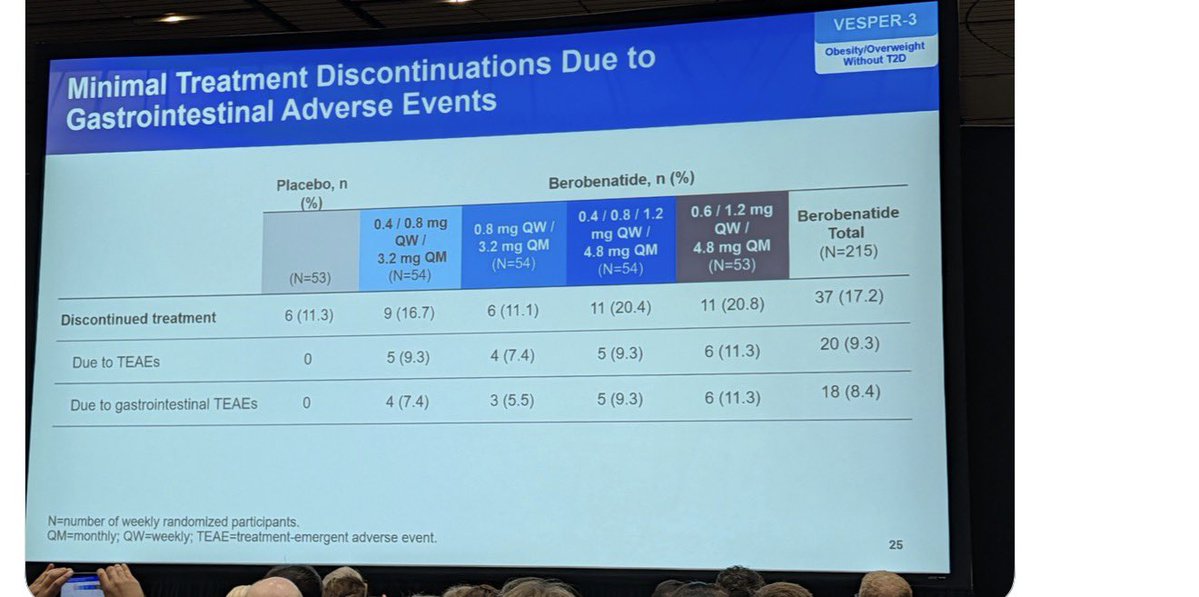
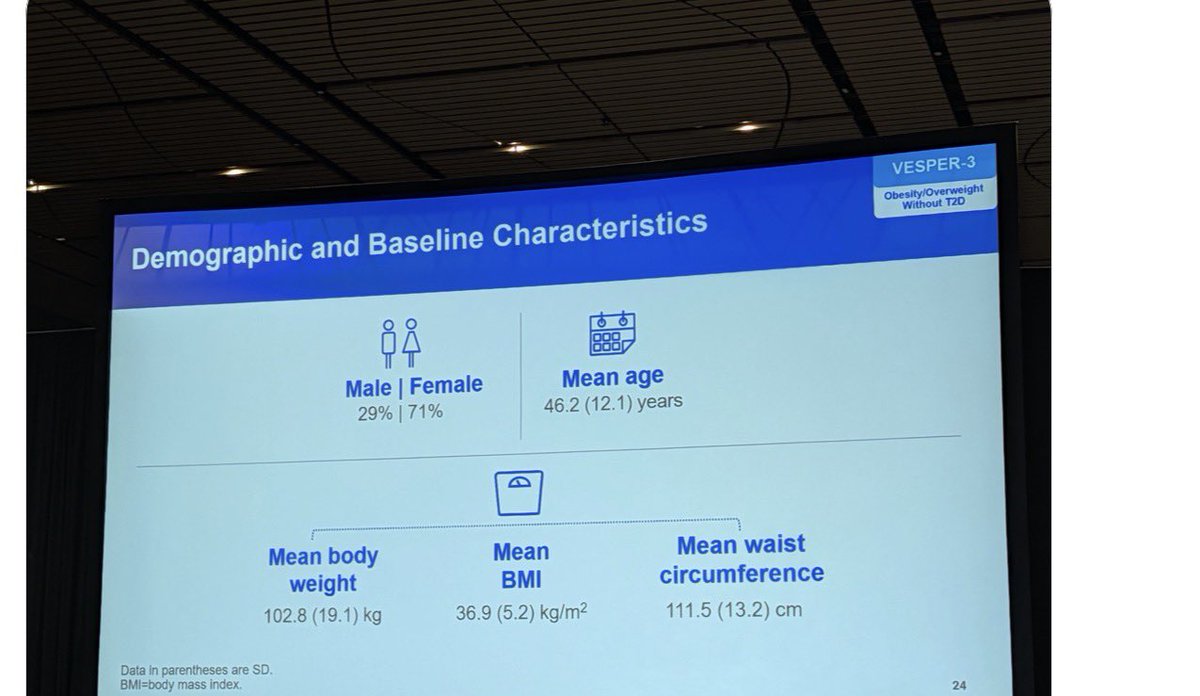
$PFE vesper 3 data in details.
Data seem to be at best in line with $NVO semaglutide. Efficacy may or may not reach 15% long term although higher female ratio than other trials. Higher DC rate vs semaglutide
5
1
8
1,477

Any longer than weekly injection (2Q or 4Q) will be more convenient on economic part only ,it means half or even 1/4 the cost with which you maintain your WL ,
longer 1/2 lives dual GLP GIPs will be cheaper even compared to monthly monos long term in absolute value, apart from better tolerability
1
11
The issue is the dose you'd need to administer for monthly. Tolerability will suffer. Every other week will do well given VK2735 half life of around 10 days. Should be similar to Tirz weekly as far as peak-to-trough.
1
1
16

Other than Bax and Loru, no ASI drug is close to commercialization in 3L/4L HTN..,
You keep reducing ASIs to “they lower BP,” while ignoring the biology and the tolerability angle versus current late-line options like spironolactone.
1
1
55
Q 2 wk obesity injection will likely be the dominant long term solution. It balances convenience with limited stress of chronic side effects etc. $VKTX 2735 as potentially BIC GLP1 GIP and with longer t1/2 vs $LLY tirzepatide could become best fit for that. I am expecting 7.5-10 mg q 2 wks to do the job with the least tolerability issues. Data in September
Feb 12

$VKTX BRiley nugget Fully enrolled Ph1 maintenance study incorporates newly added Q2W subcu arm. This addition occurred after trial initiation, driven by
investigator feedback and proprietary market research showing patients gravitating toward less frequent regimens, splitting the originally
planned 15mg monthly into two 7.5mg Q2W doses while retaining higher monthly options, thereby providing the most comprehensive
dosing frequency dataset in the class.
2
1
16
1,631

$CRVS I&I is likely the largest commercial opportunity for soquelitinib, but the oncology angle should not be ignored — especially in r/r PTCL, where the ongoing Phase 3 against physician’s-choice pralatrexate or belinostat is a real test. Soquelitinib will have to win on PFS.
The Phase 1 PTCL dataset was single-arm, so, accordingly, the cross-trial comparison should be treated carefully. That said, the soquelitinib data is interesting for reasons that go beyond a simple ORR comparison.
In the 200 mg BID, 1–3 prior-therapy subgroup, soquelitinib showed 37.5% ORR, 25% CR, 12.5% PR, 6.2-month median PFS, and 28.1-month median OS. The notable feature is not just the response rate. It is the response quality.
Three highly interesting PTCL features:
1. CR-dominant durability tail
Soquelitinib’s responders skewed toward CR: 6 CRs vs 3 PRs. That is the reverse of what we see with pralatrexate and belinostat, where responses are more PR-dominant.
That matters because the Phase 3 primary endpoint is PFS. If soquelitinib wins, the hazard ratio may possibly be driven less by headline ORR and more by a durability tail from deep, immune-mediated remissions. A reconstructed Phase 1 DoR appears to be in the ~18 to ~20-month range, though, for clarity, that is an estimate from the swimmer plot, not a company-reported median.
2. Immune-competence/earlier-line biology
Soquelitinib appears to work best in patients with a more intact immune system, especially earlier-line patients and those with ALC ≥900. The Phase 3 does not formally require ALC ≥900, which is a risk, but the 1–3 prior-line cap may capture much of that biology indirectly.
This is not just a patient-selection detail. If soquelitinib’s effect depends on functional T-cell biology, then preserving immune competence may be central to preserving the CR/durability profile.
3. Cleaner-looking tolerability versus SOC
The safety profile also matters. Pralatrexate and belinostat are active drugs, but their toxicity profiles can limit exposure, force dose interruptions, and potentially weaken patients before they ever get durable benefit.
Soquelitinib’s PTCL safety profile looks meaningfully cleaner cross-trial, especially on key Grade ≥3 cytopenias and mucositis-type toxicity. That could matter clinically and mechanistically: a drug that controls disease without burning down the immune system may have a better shot at generating durable responses.
Strikingly, there is also a provocative biomarker angle: soquelitinib has shown activity in GATA3-positive / GATA3-high PTCL, consistent with pharmacologically meaningful ITK/GATA3 pathway inhibition. This falls in the exploratory bucket for now, as GATA3 was not used for selection and the public biomarker dataset is still being investigated per management discussions.
Viewing down range: I&I may be the big commercial prize, but PTCL is the sharper proof-of-mechanism test. If soquelitinib can beat pralatrexate/belinostat on randomized PFS, that would say a lot about ITK as a drug target — and begin to establish soquelitinib as a potential “pipeline in a product.”
3
132

Phase 1 Maintenance Dosing trial for VK2735 in the third quarter of 2026. The market expects this data to establish VK2735 as a best-in-class obesity treatment—matching or exceeding the efficacy and tolerability of current market heavyweights. [1, 2, 3] $vktx
1
256


Concerns were understandable given the leadership and execution issues at the time. But focusing only on % weight loss misses what patients value: safety, tolerability, convenience, access and long-term adherence. Patients don’t always follow analysts’ models.
1
6

Suven Life Sciences Ltd announced the successful completion of Phase-1 first-in-human (FIH) clinical study of SUVN-I6107, a novel, potent, and highly selective muscarinic M1 positive allosteric modulator (M1-PAM).
The study demonstrated favorable safety, tolerability, pharmacokinetic and pharmacodynamic characteristics, supporting the advancement of SUVN-I6107 into Phase-2 clinical development.
This is the fifth internally discovered candidate (NCE) to enter clinical development.
#SuvenLifeSciences #SuvenLife #Suven
55

$ACOG
Alpha Cognition Announces First Patient Enrolled in RESOLVE Phase 4 Study Evaluating ZUNVEYL® in Patients with Mild to Moderate Alzheimer’s Disease
- RESOLVE is a multicenter, post-approval Phase 4 study designed to further evaluate the tolerability profile of ZUNVEYL in clinical practice, in patients with Alzheimer's disease.
- The study will collect safety and tolerability data and will also explore changes in Alzheimer's disease-related neuropsychiatric symptoms in an outpatient setting among patients receiving ZUNVEYL.
- RESOLVE is expected to enroll approximately 150 patients
stocktitan.net/news/ACOG/alp…
64

Ozempic was never designed to make you lean.
It was built for type 2 diabetes. GLP-1 is a signal your gut sends after you eat. It tells the pancreas to release insulin. It calms glucagon. And blood sugar improves.
Then researchers noticed something they weren’t looking for.
The patients were losing weight. They ate less. They got leaner. Not through willpower. Through improved satiety.
So it was studied for weight loss. And approved for it.
Then came the next layer. Tirzepatide. They added a second signal, GIP, to improve tolerability and insulin sensitivity. And in the trials, something fascinating showed up.
The improvements seemed to start before the weight came off. Markers of metabolic health moved early. Inflammation markers came down. The benefit didn’t appear to be just from weight loss alone.
Now researchers are asking the bigger question. Why does steady GLP-1 and GIP signaling seem to create broad band health benefits
7
3
51
8,249

$VSTM
Standard PoS would be at 45%.
Peak-Sales: 1.25B for NSCLC; 250M for mPDAC; 230M for CRC (each for mono and combi, for simplicity)
The key might be mPDAC, because the NSCLC market is so competitive.
Reporting data on VS-7375, Oral KRAS G12D (ON/OFF) Inhibitor data:
Tuesday, June 23 at 4:30 pm ET
Verastem’s management team will present preliminary data from the TARGET-D 101 dose-escalation and dose expansion cohorts across pancreatic, colorectal, and non-small lung cancers, including updated safety and tolerability, pharmacokinetic findings, as well as patient case studies evaluating VS-7375 both as a monotherapy and in combination across multiple tumor types.
A webcast of the call, along with accompanying slides, will be available under "Events & Presentations" in the Investor section of the Company's website.
If you want to read my article about the company, here it is:
open.substack.com/pub/plutoa…
1
125

Depression R&D looks crowded, but pull the pipeline apart and the data shows it's actually a barbell.
I used Sleuth to pull 649 depression assets in development across unipolar and bipolar indications, and classified each by mechanism, phase and sponsor. A few things stood out:
• The approved set is dominated by monoamine pharmacology: ~75% of drugs sit there, mostly classic monoaminergics and antipsychotic adjuncts.
• The modern exceptions, esketamine, Auvelity, zuranolone and brexanolone, offered a faster relief story versus the 4-8 week long SSRI / SNRI baseline
• But while faster onset is a differentiator, it needs to be paired with a workable care model - for example, brexanolone was pulled in 2025 because the 60-hour IV model restricted REMS left it unworkable next to the oral zuranolone
On the other side of the barbell, and somewhat unique within biopharma, pipelines are not converging around a single mechanism, but rather splintering across many.
The largest block is a 130 mechanism tail where no single MoA has more than a dozen assets, and most are preclinical. Another 115 assets have no disclosed mechanism at all.
For context, this undisclosed group is bigger than the entire psychedelic pipeline. And across the entire fragmented tail, Pharma shows up in 24% of programs versus just 2% of psychedelics.
So, while many sponsors are happy to take on target biology risk (which makes sense given the limitations of canonical approaches), the key strategic question for biopharma leaders is "where are we on the barbell?"
These two questions help sharpen your strategy:
• What indication offers the cleanest wedge?
As treatment dynamics vary significantly by disease - for example, most programs pursuing PPD are competing on convenience vs. the old IV model, while those pursuing treatment-resistant depression are scattered across dozens of novel mechanisms
• What burden can your program remove that incumbents cannot?
There are real positioning wins around route, tolerability, monitoring and keeping rapid relief without the dissociation.
If you're positioning an asset in this space for BD or portfolio review, get in touch for more tailored insights.
And comment below for a hi-res PDF of the deck with a few additional slides.

1
2
1,108

That said, the weaknesses: the older-adult clinical efficacy trial used a non-preferred comparator, the preferred-comparator evidence is immunogenicity-based, reactogenicity is meaningfully higher, and the most relevant 65 clinical question will be deferred to Phase 4. Is a faster, more flexible platform a public-health asset only if the product’s clinical performance and tolerability justify use?
1
2
243

More convenient, less stigma & similar efficacy when compared to injectables
greater accessibility & tolerability compared to Foundayo
Wegovy pill >>>
1
71