
Jun 14
THYROID & AKKERMANSIA, LPS & GAMMAPROTEOBACTERIA
'Gut microbiota in hypothyroidism: pathogenic mechanisms and opportunities for precision microbiome interventions'
(Review 30 September 2025)
frontiersin.org/.../fmicb.20…
"Results from a two-sample Mendelian randomization study demonstrate a causal relationship between Akkermansia and hypothyroidism, indicating that Akkermansia may inhibit the occurrence and progression of hypothyroidism"
'Cross-talk between the gut microbiota and hypothyroidism: a bidirectional two-sample Mendelian randomization study' (2024)
frontiersin.org/.../fnut.202…
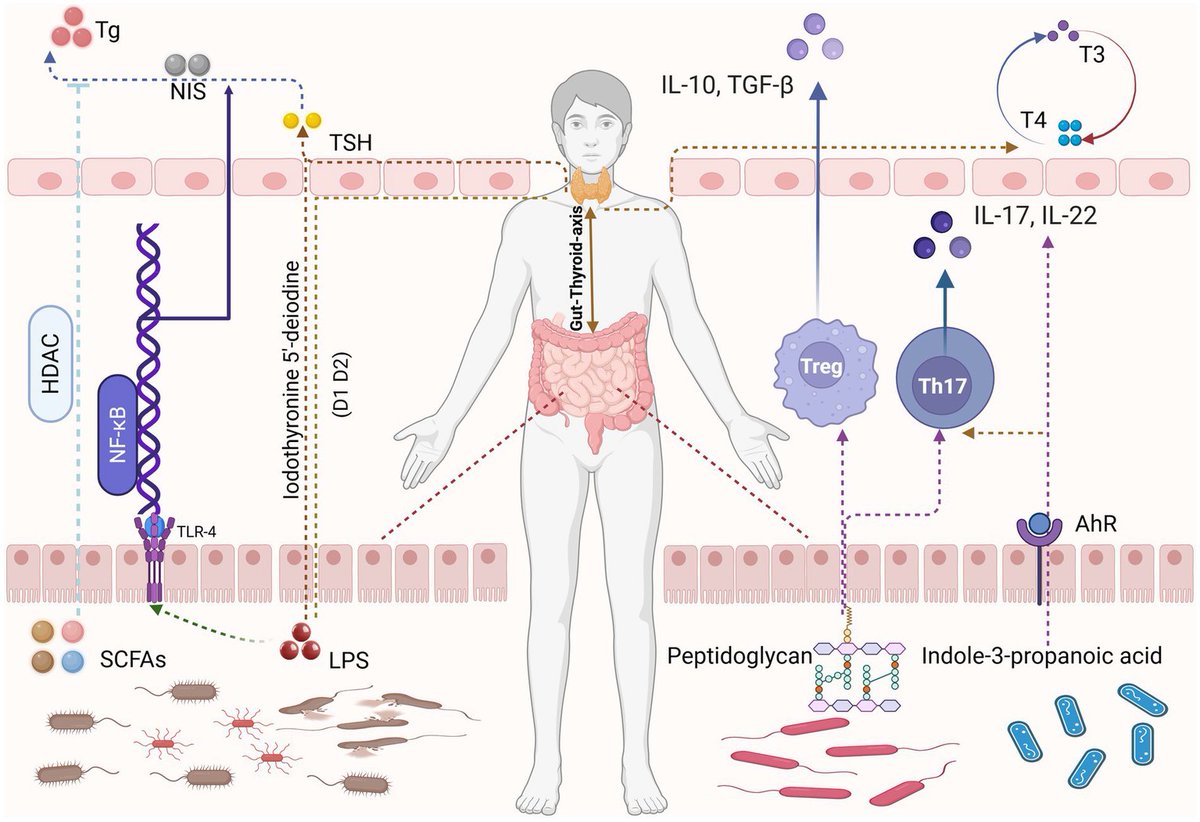
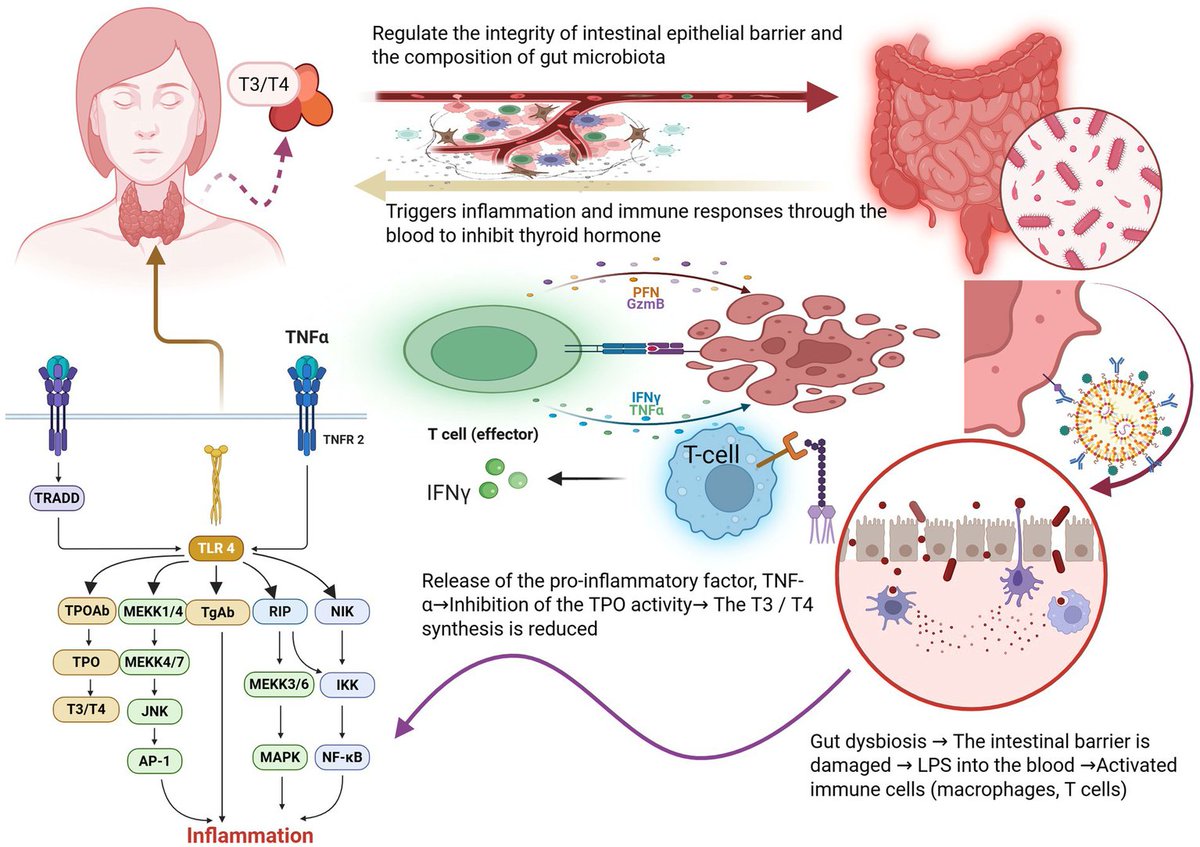
"In hypothyroidism patients, Akkermansia muciniphila numbers are upregulated, which may be a compensatory response of the body facing the impaired intestinal barrier. On the one hand, Akkermansia muciniphila enhances the junction strength between intestinal epithelial cells by regulating the expression of tight junction proteins, such as ZO-1, Occludin, and Claudin-1, to attempt to repair the disrupted intestinal barrier (). On the other hand, Akkermansia muciniphila can activate immune cells in the intestine, such as macrophages and dendritic cells, to secrete the anti-inflammatory cytokine IL-10 and inhibit the inflammatory response (). However, when Akkermansia muciniphila proliferates excessively, it breaks the intestinal immune homeostasis. The structure of lipopolysaccharide (LPS) on the surface of Akkermansia muciniphila is different from other Gram-negative bacteria, which has immunomodulatory effect at low concentrations. But it will be recognized by the immune system in excess, activating the Toll-like receptor 4 (TLR 4) signaling pathway, and promoting the release of immune cells to release a large number of pro-inflammatory cytokines, such as TNF- α and IL-6 (). These pro-inflammatory factors enter the blood circulation and trigger systemic inflammation that interferes with the synthesis and secretion of thyroid hormones. At the same time, the hyperactivated immune system mistakenly attacks thyroid tissue, producing thyroid autoantibodies, such as TPOAb and TgAb, which further damage thyroid function."
"Dysbiosis-induced increased intestinal permeability allows the translocation of bacterial endotoxins, notably LPS, into the systemic circulation, triggering inflammatory cascades that compromise thyroid tissue integrity and hormone synthesis. Moreover, the imbalance in microbiota composition skews immune cell differentiation toward pro-inflammatory phenotypes, particularly Th 1 and Th 17 cells, and concurrently diminishes the function and numbers of regulatory T cells, thereby enhancing the risk and severity of autoimmune thyroid diseases "
"prebiotics such as fructose oligosaccharides and galactose are able to significantly promote the proliferation of Bifidobacteria and Lactobacillus, while inhibiting the growth of harmful bacteria such as Clostridium and Escherichia coli "
1
1
5
151

Random Shooting attacks on Indians in USA is happening because of Lone Wolf Racists getting Hyperactivated by Bot accounts Amplifying Hatred initiated by Pakis @nikitabier & @elonmusk Innocent🩸🩸is on Your Hands.Take Course correction before Govt of India Bans you Permanently.
1
69

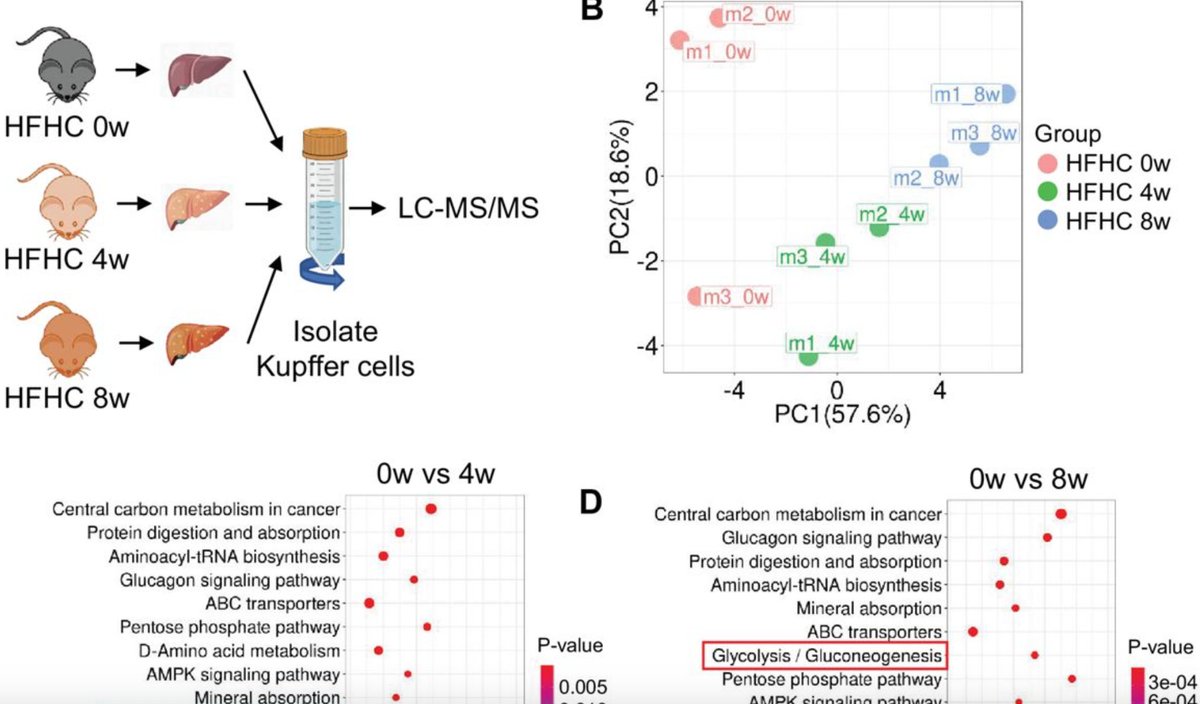
Hyperactivated glycolysis drives spatially patterned Kupffer cell depletion in #MASLD @eLife elifesciences.org/articles/1…
4
12
539

Aside the fact your hair remind me of a mouse, I'd ask why is ours easily hyperactivated? Does it mean they don't have allergies?

2
3
65

Jun 5
In mice immune system doesn't get hyperactivated, so they can go on with their life! a long living host, constantly spreading the infection =͟͟͞(꒪ᗜ꒪ ‧̣̥̇)

1
1
13
249

Neuroinflammation. Hyperactivated immune cell signalling has got everybody's wires crossed, resulting in ATP energy depletion. Welcome to the BioPsyOp!
1
10
342

The problem seems to be you didn't seem to read your link. Not only is that research concerning influenza but that matters because influenza never has transient persistence. The problem here is not stimulating humoral immunity; the problem is hyperactivated humoral immunity.
1
3
57
Spike Protein fragments & debris that turn non-classical monocytes into hyperactivated zombie cells. Dr Bruce Patterson's work as reported by Dr. Mobeen Syed and many others x.com/WildKraken1/status/205…
21 Feb 2024

A Potential Role of the Spike Protein in Neurodegenerative Diseases: A Narrative Review
"compelling evidence that the spike glycoprotein of SARS-CoV-2 contains extended amino acid sequences characteristic of a prion-like protein"
ncbi.nlm.nih.gov/pmc/article…
1
1
3
837

The diagnosis here is Hemophagocytic Lymphohistiocytosis (HLH) — one of the most dangerous hematological emergencies to miss.
The clues are all there: persistent fever not responding to antibiotics, severe pancytopenia, extremely elevated ferritin, and rapid progression to multi-organ dysfunction.
HLH is basically an uncontrolled cytokine storm where the immune system becomes hyperactivated and starts damaging the body itself.
Key findings commonly seen:
• Persistent high fever
• Cytopenias affecting multiple cell lines
• Ferritin often massively elevated
• Hepatosplenomegaly
• Liver dysfunction
• Coagulopathy/DIC
• Hemophagocytosis on bone marrow examination
Common triggers include:
• EBV and other viral infections
• Lymphoma/leukemia
• Autoimmune diseases
• Severe infections
Management cannot wait for every confirmatory test.
Immediate treatment usually involves:
• High-dose dexamethasone
• Etoposide in severe cases
• ICU-level supportive care
• Treating the underlying trigger simultaneously
The biggest mistake is assuming it’s just “sepsis not responding to antibiotics.”
Delayed recognition is what makes HLH so lethal.
1
3
1,417

An AI scribe listened to a patient say "I became ill with something viral." It wrote that the patient had taken "hyperactivated antibiotics" — a drug that doesn't exist — into a permanent health record. This is happening at scale. 🧵 #MedicalAI #AIScribes
3
3
3
156


May 21
And here is the important paradox.
The neutrophils seem hyperactivated.
At baseline, they produce more NETs.
But at the same time, they respond less effectively to viral signals through TLR7/8!
That is not a stronger immune system.
It is a dysregulated one.
1
9
86
1,507

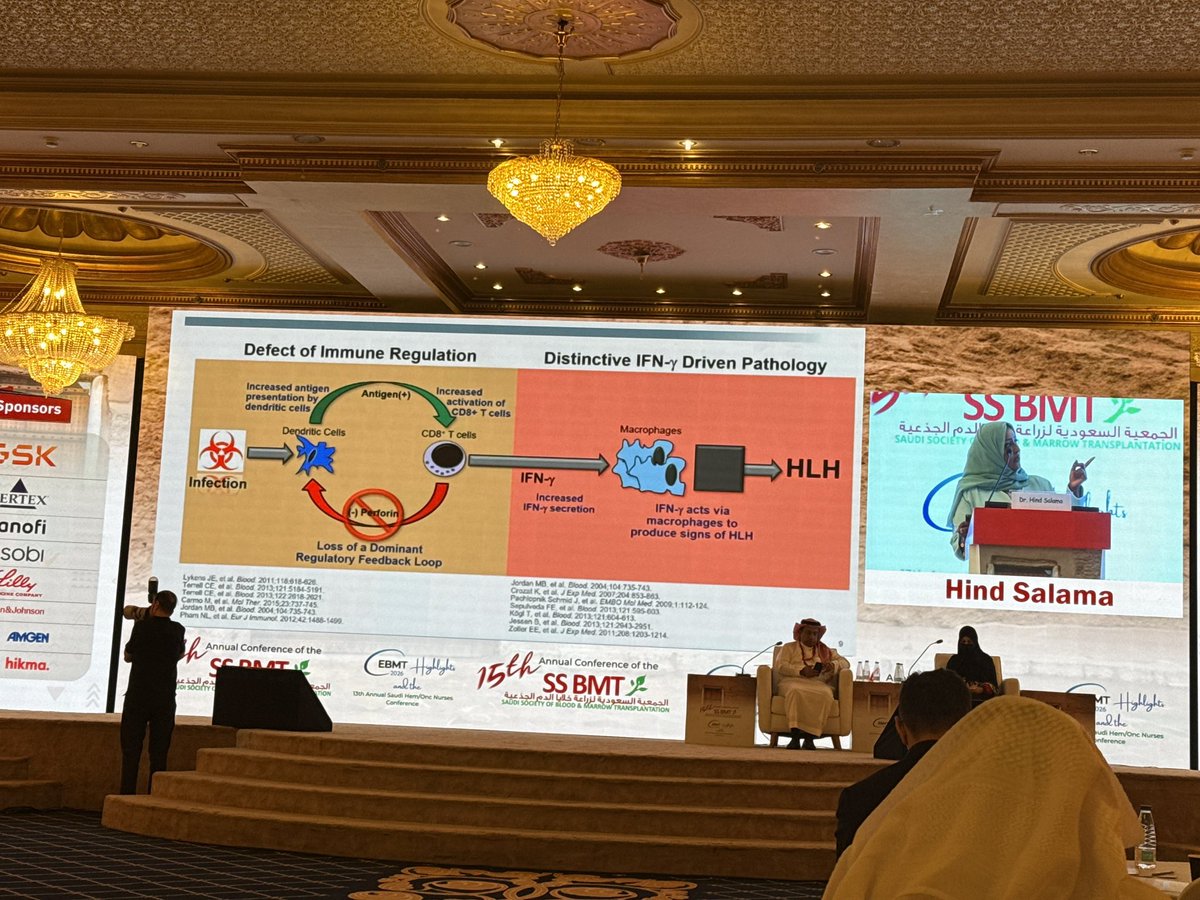
🔥 Pathophysiology of Hemophagocytic Lymphohistiocytosis (HLH)
When Immune Regulation Fails
Credits for sharing: Dr. Hind Salama 🌟
⸻
🧬 Normal Immune Response
🦠 Infection triggers antigen presentation by dendritic cells.
⚔️ CD8⁺ T cells and NK cells kill infected cells using:
🗡️ Perforin
💥 Granzymes
🛑 This cytotoxic function shuts down immune activation once the threat is cleared.
⸻
❌ Defect in Immune Regulation
🧬 Genetic or acquired defects in:
Perforin (PRF1)
MUNC13-4 (UNC13D)
STX11
STXBP2
Other cytotoxic pathway genes
➡️ Impaired killing of activated immune cells.
➡️ Persistent antigen stimulation.
➡️ Uncontrolled CD8⁺ T-cell activation.
⸻
🚨 IFN-γ–Driven Pathology
🔥 Hyperactivated CD8⁺ T cells release massive amounts of interferon-gamma (IFN-γ).
IFN-γ causes:
🧲 Macrophage activation
🩸 Hemophagocytosis
🌡️ Hyperinflammation
🫀 Multi-organ dysfunction
➡️ Clinical HLH develops.
⸻
🧠 Cytokine Storm Cascade
IFN-γ stimulates production of:
IL-1β
IL-6
IL-18
TNF-α
CXCL9
sCD25
Result:
🔥 Fever
🩸 Cytopenias
🫛 Splenomegaly
🧪 Hyperferritinemia
🧬 Elevated soluble IL-2 receptor
🩸 Coagulopathy and hypofibrinogenemia
⸻
🧬 Primary vs Secondary HLH
Primary (Familial) HLH
👶 Germline defects in cytotoxic machinery.
Secondary HLH
Triggered by:
🦠 EBV, CMV, HSV, fungal infections
🩸 Lymphoma/leukemia
💉 Immunotherapy (CAR-T, checkpoint inhibitors)
🧬 Autoimmune diseases (MAS)
⸻
🎯 Targeted Therapies
Steroids
🛑 Broad cytokine suppression.
Etoposide
💥 Eliminates activated T cells.
Emapalumab
🎯 Neutralizes IFN-γ directly.
Ruxolitinib
🔌 Blocks JAK1/2-mediated cytokine signaling.
Anakinra
🛡️ IL-1 receptor blockade.
⸻
🧪 Biomarkers Reflecting IFN-γ Activity
📈 Ferritin
📈 CXCL9
📈 sCD25 (soluble IL-2 receptor)
📉 Fibrinogen
📈 Triglycerides
⸻
❓ MCQ
Which cytokine is the central driver of HLH pathogenesis?
A. IL-4
B. IFN-γ
C. Erythropoietin
D. VEGF
✅ Answer: B. IFN-γ
⸻
💎 Clinical Pearl
HLH is fundamentally a disease of failed immune termination. The immune system is activated appropriately but cannot switch itself off.
⸻
📌 Bottom Line
🧬 Defective cytotoxic function → persistent antigen stimulation.
🔥 Excess IFN-γ → macrophage overactivation.
🩸 Cytokine storm → hemophagocytosis and organ failure.
🎯 Modern therapies increasingly target IFN-γ and JAK-STAT signaling.
⸻
References
HLH-94 and HLH-2004 Protocol Overview (Histiocyte Society)
Blood Journal Review on HLH
FDA Emapalumab Approval
#HLH #HemophagocyticLymphohistiocytosis #IFNgamma #Emapalumab #Ruxolitinib #Ferritin #CytokineStorm #Hematology #KFSHRC #SSBMT2026
1
3
11
438

outside your window of tolerance, you're either hyperactivated (scanning, spiraling, checking his location) or shut down (numb, disconnected, "i don't even care anymore").
neither state can hold a new assumption. the nervous system won't allow it.
1
12
878

May 12
What is "Suicidal Empathy" ? Popularized by evolutionary psychologist Gad Saad, the concept describes scenarios where empathy is "hyperactivated" toward the wrong targets, like favoring outsiders or wrongdoers at the expense of one's own community
a.co/d/0fKjHyDo
1
4
229

May 10
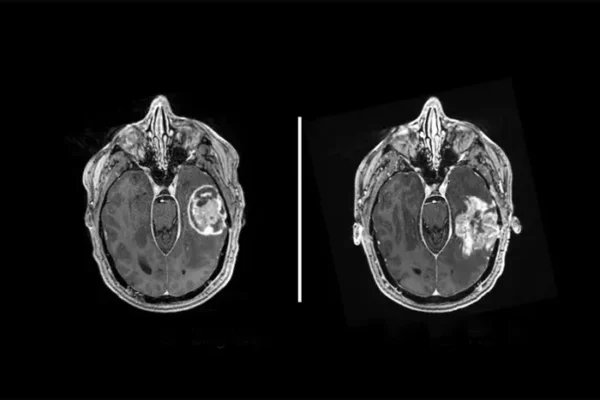
Testosterone Slows Brain Tumor Growth, Overturning a Decades-Old Cancer Assumption | Ben Sullivan, ScienceBlog
Everything oncologists thought they knew about testosterone and cancer pointed one direction. The hormone suppresses the immune system, shields tumors from attack, makes things worse. Strip it away and patients do better. That logic held across lung cancer, bladder cancer, melanoma, and dozens of studies. It was, by most accounts, one of the cleaner narratives in cancer biology. Then Juyeun Lee’s team at Cleveland Clinic started removing testosterone from mice with brain tumors, and the tumors grew faster.
The finding, published in Nature , doesn’t just complicate the testosterone-in-cancer story. It rewrites it in a way that could matter directly to patients with glioblastoma, the most common and lethal primary brain tumor in adults.
Lee, a veterinarian-turned-cancer-researcher now based at Cleveland Clinic’s Florida Research & Innovation Center, had started from a reasonable premise. Glioblastoma is more common in men than in women, more aggressive in men, and kills them faster. Sex hormones seemed a plausible culprit. “There are other findings on non-brain tumors that show that testosterone is basically the bad guy, suppressing the immune response and making the tumor grow faster,” she says. “This has been shown in multiple cancers, like lung and bladder cancer and melanoma. We wanted to know if the same result would occur in glioblastoma.” The team castrated male mice, implanted brain tumors, and watched survival times collapse rather than improve.
Collapse. Not improve. Which meant something particular to the brain was flipping the normal hormone logic on its head.
The researchers ran several checks to rule out the obvious alternatives. Perhaps testosterone was simply toxic to glioblastoma cells directly? But when the same tumor cells were implanted under the skin, in the flank, castration worked exactly as expected: tumor growth slowed. Bladder cancer and melanoma cells, implanted directly into the brain, also grew faster in castrated animals, ruling out a glioblastoma-specific cell effect. Whatever was happening had nothing to do with the cancer type. It had everything to do with where the tumor was sitting.
A Chain Reaction Starting in the Brain
Justin Lathia, who leads the Cleveland Clinic lab that conducted the research, describes what the team uncovered as a cascade with unusually long reach. “In cancers outside of the brain, blocking androgens can improve immunity,” he says. The brain reverses that logic entirely, he argues, because the effects travel far beyond the tumor site itself, reshaping neuroendocrine function in distant regions including the hypothalamus. “The location of a tumor significantly changes how hormones affect immunity.”
The mechanism, pieced together through spatial transcriptomics, single-cell RNA sequencing, and several knockout mouse strains, runs roughly like this: without testosterone, the brain’s resident immune cells, known as microglia, become hyperactivated at the tumor site. They ramp up production of two inflammatory signals, IL-1beta and TNF, which travel to the hypothalamus and jolt a circuit most people associate with stress rather than cancer. That circuit, the hypothalamic-pituitary-adrenal axis, responds by flooding the bloodstream with glucocorticoids, the body’s stress hormones. Glucocorticoids then suppress T cells throughout the body, not just in the brain, and the immune system’s capacity to fight the tumor drops. The team confirmed each link: mice missing receptors for IL-1beta or TNF didn’t show the castration effect at all. Blocking the glucocorticoid receptor with a drug called mifepristone extended survival in castrated mice. Microglia depletion reduced the inflammatory signals. The whole chain held together.
Particularly striking was what happened in the hypothalamus, a brain region that physically doesn’t touch the tumor. Transcriptomic analysis of hypothalamic tissue showed that castrated tumor-bearing mice had a distinct gene expression signature compared to their intact counterparts, one enriched for cytokine signaling pathways. The tumor, it seems, was reaching across the brain to reshape neuroendocrine function in a hormone-deprived setting.
The effect also worked in immunodeficient mice, which retain microglia but lack adaptive immune cells, pointing at the brain’s innate immune system as the initiating event rather than T cells directly. Microglia, it turned out, have a hair trigger for inflammasome activation when androgens are absent: in lab experiments, treating macrophages with dihydrotestosterone sharply reduced the condensation of ASC “specks,” a marker that the NLRP3 inflammasome is firing. Without the hormone, the specks multiplied.
Evidence from Patients
Whether any of this translates to people is, of course, the question that matters. The team went looking for an answer in the SEER-Medicare linked database, which tracks cancer outcomes for older Americans. Among men diagnosed with glioblastoma between 2008 and 2019 who received standard chemotherapy, those who also happened to be on testosterone supplementation (61 patients) had a median overall survival of about 16 months, compared with roughly 12 months for those receiving chemotherapy alone (more than 1,200 patients). After adjusting for age, disease burden, and other variables, the survival advantage translated to about a 38% reduced risk of death. Small numbers, retrospective data, all the usual caveats. But the direction matched the mouse experiments precisely.
Clinical translation faces real obstacles. Glioblastoma patients are frequently treated with dexamethasone, a potent glucocorticoid used to control brain swelling, particularly around surgery and radiation. That drug already suppresses the HPA axis and the immune system; adding testosterone supplementation to that picture creates interactions the current study hasn’t addressed. The mouse models also used young animals, which doesn’t capture the immunological and hormonal landscape of a typical glioblastoma patient in their late sixties.
Lathia is careful about what the findings claim. “What excites me about our findings is the new insight we are contributing to the growing field of cancer neuroscience,” he says. “This study looks beyond the tumor at the interaction with the nervous system, in addition to the immune system.” The lab’s position is that supplemental testosterone warrants formal evaluation as a glioblastoma therapy, not that it’s ready to prescribe. “We see so much potential for the future of glioblastoma treatment. Our ultimate assertion is that supplemental testosterone could be evaluated as a therapy, marking an important opportunity to advance our fight against cancer.”
What’s harder to qualify is the conceptual shift the paper forces. For anyone developing cancer immunotherapies, the assumption that androgen deprivation is reliably helpful, that removing testosterone always frees T cells to do their job, may now need a geographic footnote. Where the tumor lives, it seems, determines what the hormone does to the body trying to fight it.
Read more:
scienceblog.com/testosterone…
2
4
30
2,781

Fleur Ferguson, PhD at @UCSanDiego is creating a new class of drugs that selectively eliminate the hyperactivated, cancer-driving forms of proteins while leaving their healthy counterparts untouched.
1
7
598
Damaged/distended from the back pressure and degraded by zombie‐fied hyperactivated monocites?
1
2
23

May 1
Agreed. Coding with agents feels similar to using tiktok or twitter in a weird way. Like my dopamine circuits are hyperactivated?
7
1,744

There is no relationship between being smart and being wise.
Jordan Peterson: “Many of the wisest people I’ve known were intellectually impaired.”
Smart people hate hearing this.
Because the smarter you are, the better your excuses.
He spent 5 minutes explaining why smart people fail:
"There is no relationship between being smart and being wise."
"They are not the same thing. There's no quick pathway from smart to wise."
"Many of the people I've known who were very wise were intellectually impaired. And were still wise."
Here's what blocks intelligent people.
"The arrogance of the intellect. The thing the Catholic church had warned about for centuries."
"If you're smart, you tend to think: I'm so smart, everything should just come to me."
"Sorry. That's not how the world works."
"And that attitude is immediately evident to people when they talk to you."
Nietzsche described this perfectly.
"In Thus Spoke Zarathustra, Zarathustra comes down from the mountain into a public square."
"There's a crowd around this dwarf who's only about this high. But he has a gigantic ear. Everyone is marveling at him."
"That's what the modern intellect is like."
"A dwarf with a giant mouth. The being is underdeveloped. But the intellect is hyperactivated."
"It makes the person extraordinarily unbalanced."
Here's why they're bitter.
"They can't compete outside the intellectual realm."
"That makes them very bitter. Because they think everything should just come to them."
"But it doesn't."
Peterson watched this play out in real time.
"I had friends in the United States. Very smart people."
"Some of them were talking about the Trump voters. With contempt."
"I thought: you better watch that. Because that's 50% of the damn population."
"It might be convenient to think they're stupid and beneath you. But it's not conducive to a civil state."
"And there's no evidence that it's true. Because there isn't a straight line between intelligent and wise."
The solution for intelligent people.
"If your character is developed, you can have your siloed creative community."
"But you develop enough wisdom to see all the things people can do that are of high ethical utility outside the intellectual domain."
"There's every reason to have respect for decent working-class people."
"It's on their labor that the entire edifice of the culture is resting."
On finding your people.
"Not everybody is equipped to or interested in engaging in high-level discussion of abstract and creative ideas."
"You hear this idea that everyone's creative. That's a lie. It's as straightforward as that."
"True creativity is very very rare."
"If you happen to be a creative person or someone profoundly interested in ideas, you are in a pronounced minority."
"What you do is find like-minded people who are capable of engaging."
"Heavyweight weightlifters compete with heavyweight weightlifters for a reason. Everyone thinks that's fine."
"The same thing applies to intellectual and creative endeavors."
"You can have your cake and eat it too."
"But you have to not assume that your niche makes you superior."
"And it's very difficult for smart people."
19
98
468
20,251