
📊 Trending research: "Postexercise Cooling Lowers Skeletal Muscle Microvascular Perfusion and Blunts Amino Acid Incorpo..."
📝 Betz et al.
🔗 doi.org/10.1249/MSS.00000000…
#SportScience
1
20
📊 Trending research: "Postexercise Cooling Lowers Skeletal Muscle Microvascular Perfusion and Blunts Amino Acid Incorpo..."
📝 Betz et al.
🔗 doi.org/10.1249/MSS.00000000…
#SportScience

15

May 17
Pedal cadence differentially impacts cerebral blood flow but not a postexercise executive function benefit: Evidence from active and passive exercise (open access)
doi.org/10.1152/jn.00572.202…
1
188



運動後過剰酸素消費量(EPOC:Excess Postexercise Oxygen Consumption)のススメ。
体脂肪を減らす為には運動して消費カロリーを増加する事。または食事から摂取するカロリーを減らす事。
またはこれを組み合わせる事が一般的な方法です。
基本的には両方を組み合わせる事がオススメなのは誰もが知っている事だと思いますが、やはり運動を取り入れるダイエットをした方が効率良く効果的です。
その一つの要素として運動をすると運動後過剰酸素消費量(EPOC:Excess Postexercise Oxygen Consumption)
通称「アフターバーン」効果という物が得られます。
これは運動後も代謝が高い状態が続き、カロリー消費が続く効果です。
筋トレを行うと軽度な筋繊維の損傷や軽度の炎症を引き起こし、筋繊維の修復や回復に必要なエネルギーを供給する為、体内の代謝プロセスが加速されると言われております。
また運動によって酸素消費量が増えると体内のエネルギー生産も活性化される為、運動後にもエネルギー消費が続きます。
この効果は約24時間続くと言われている為、運動をした方が代謝が良くなり、体脂肪の減少や太りにくい身体作りへの恩恵が受けられると思います。
運動としては高強度の方が効果が得られやすいと言われている為、やはり筋トレがオススメです。
1
1
2
464

Effects of Sex and Obesity on Lipid Metabolism during Low-Intensity Exercise and Postexercise Period
Effects of Sex and Obesity on Lipid Metabolism during Low-Intensity Exercise and Postexercise Period
okt.to/q8TdlO
1
12
1,001

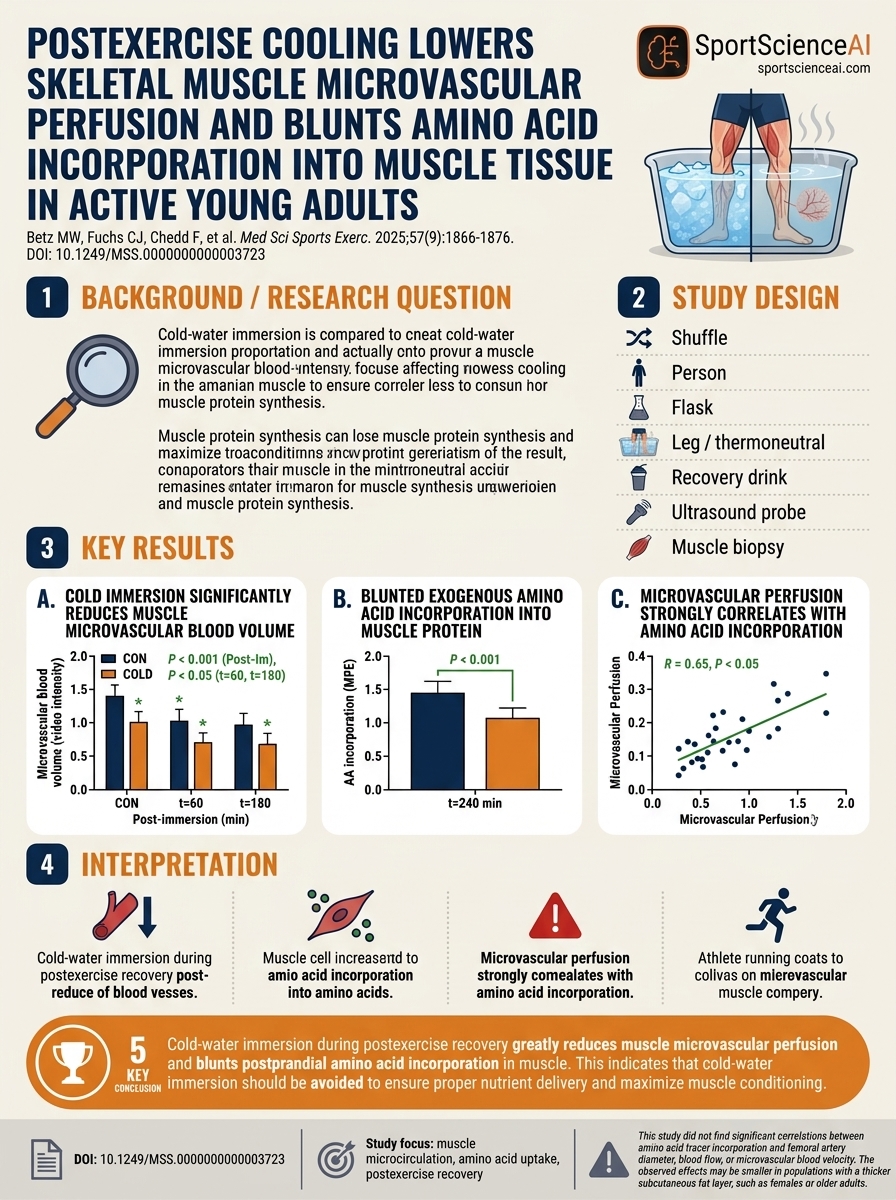
Cold water immersion and blood flow
Study:
Postexercise Cooling Lowers Skeletal Muscle Microvascular Perfusion and Blunts Amino Acid Incorporation into Muscle Tissue in Active Young Adults
Betz et al., MSSE, 2025
Link:
pubmed.ncbi.nlm.nih.gov/4024…
2
2
201

Apr 15
Excited to share our latest publication in the Journal of Strength and Conditioning Research:
Sex-Specific Immune Cell Mobilization and Recovery After High-Volume Glycolytic Squat Exercise
William J. Kraemer, Mastro AM, Saenz C, Freidenreich DJ, Volk BM, Gomez AL, Fragala MS, Szivak TK, Post EM, Wolf MR, Comstock BA, Häkkinen K, Newton RU, Jeff Volek.
This study examined how men and women differ in their acute immune response to a single bout of high-volume glycolytic resistance exercise.
Among the key findings:
Resistance exercise triggered a rapid and robust immune cell mobilization response.
Men showed a greater transient increase in circulating lymphocytes, particularly natural killer cells, shortly after exercise.
Women demonstrated a different recovery pattern, including increases in CD4 cells at 60 minutes postexercise.
Both sexes showed substantial time-dependent changes in immune cell populations during early recovery.
These findings reinforce that resistance exercise is a potent immunological stimulus, while also highlighting that the magnitude and timing of the response are partly sex-specific.
Understanding these acute responses may help inform more precise exercise prescription and recovery strategies, while contributing to our broader understanding of the interaction between exercise and immune function.
DOI: 10.1519/JSC.0000000000005443
#ResistanceTraining #ExerciseImmunology #StrengthAndConditioning #SportsScience #ExerciseScience #ImmuneFunction #Research #JSCR #ExercisePhysiology
journals.lww.com/nsca-jscr/a…
1
6
704
Apr 13
In this study, fava bean protein supplementation lowered postexercise markers of gut damage without worsening gastrointestinal symptoms during exercise in the heat and was associated with higher whole-body and local sweat rates and thermal sensation.

2
10
485
Clarifying the Role of [15O]H2O PET in Assessing Skeletal Muscle Perfusion following Postexercise Cooling
okt.to/nr7KFx
4
784

You will reach tissue saturation (creatine-loaded status) faster if it’s taken postexercise, but once you’re loaded - which can take about a month with a ~5 g/day maintenance dose, then timing relative to training doesn’t matter.
7
1,073

Feb 28
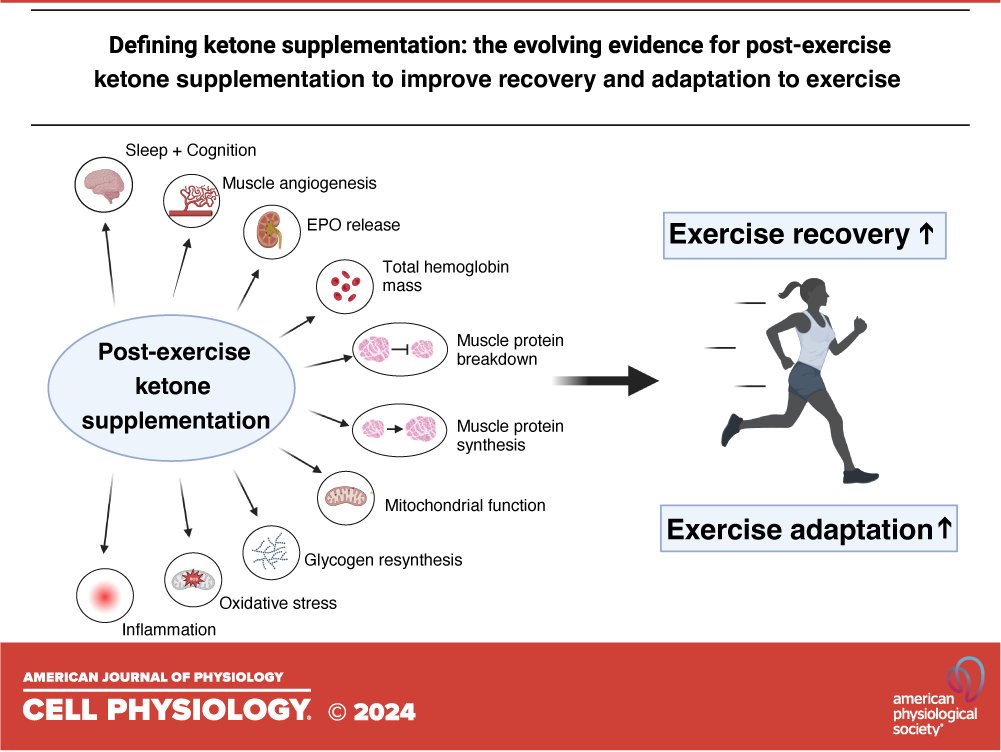
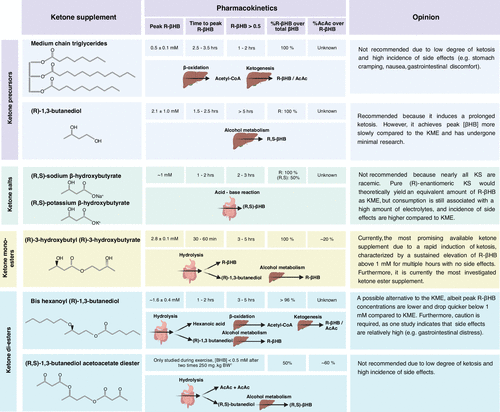
Defining ketone supplementation: the evolving evidence for postexercise ketone supplementation to improve recovery and adaptation to exercise
1
8
34
2,343

pubmed.ncbi.nlm.nih.gov/2717…
"No significant correlations between the acute postexercise rise in any purported anabolic hormone and the change in strength or hypertrophy were found. In congruence with our previous work, acute postexercise systemic hormonal rises are not related to or in any way indicative of RT-mediated gains in muscle mass or strength."
1
7
544

'The prevalence and magnitude of CAD did not differ between recreational athletes with high vs low postexercise cTn, suggesting that most of the variation in exercise-induced cTn elevations is not attributable to occult CAD' jacc.org/doi/10.1016/j.jacc.… @jaccjournals
1
2
1,708

Feb 6
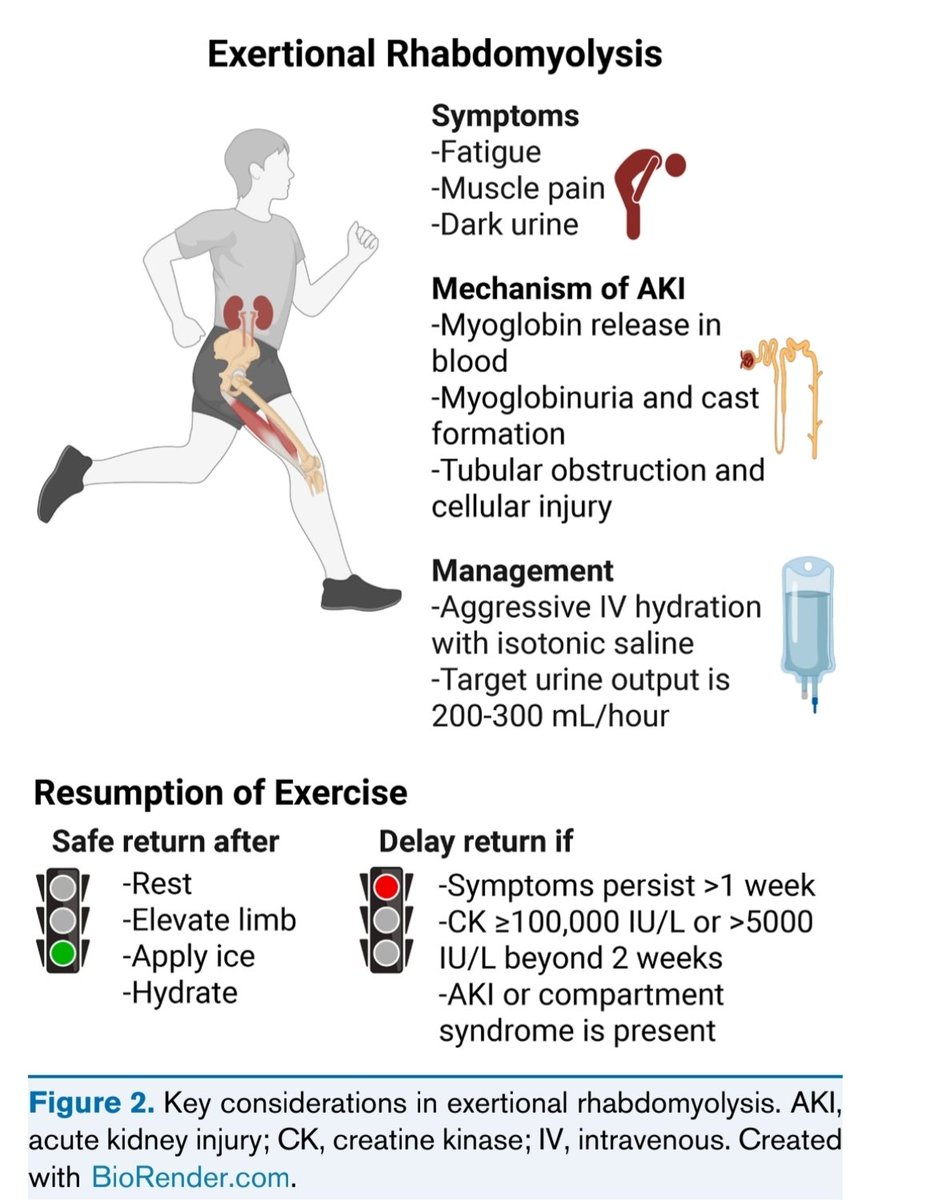
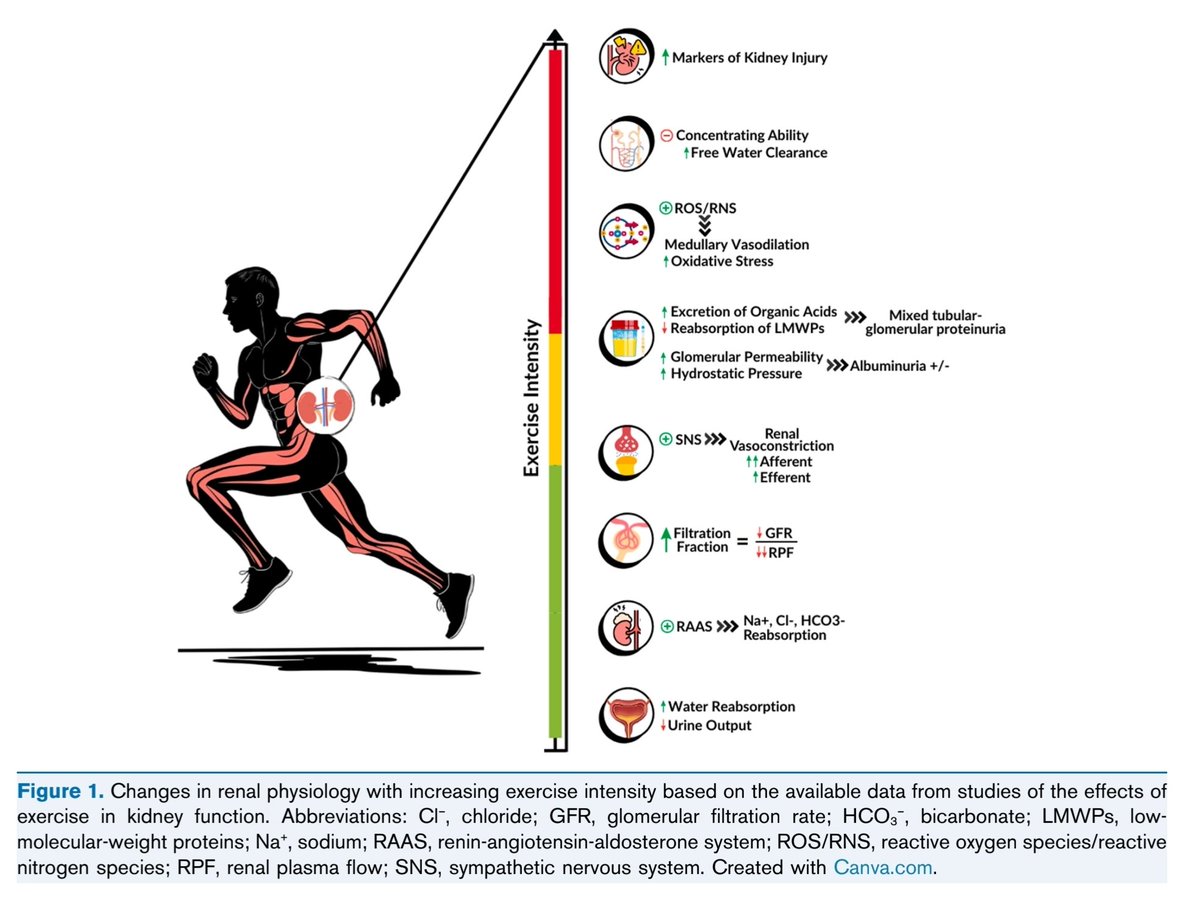
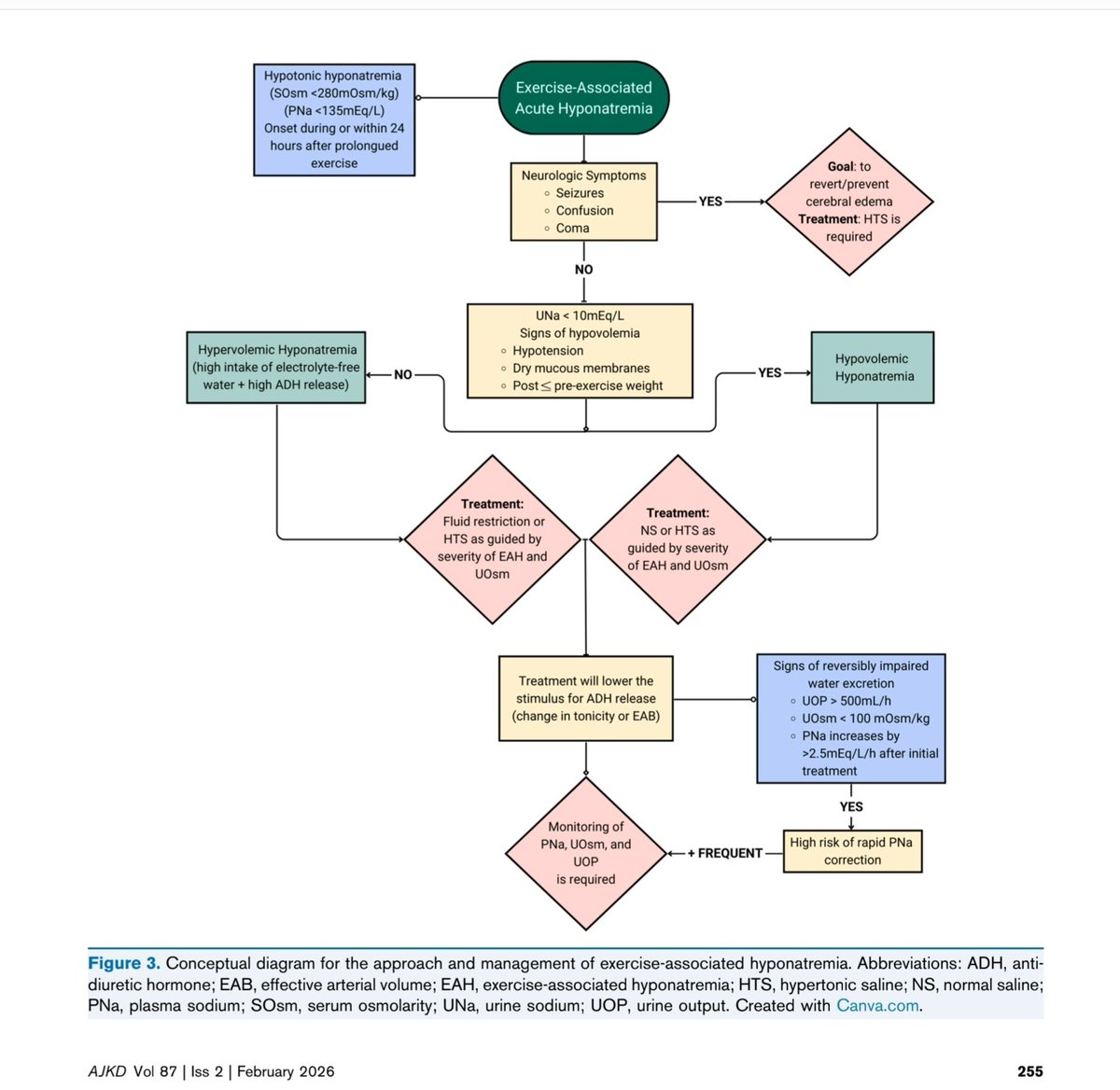
Exercise and Kidney Health (Core Curriculum 2026)
Exercise produces predictable renal hemodynamic shifts. Sympathetic activation and RAAS signaling during exertion intentionally lower renal plasma flow and GFR to conserve volume — protective in moderation, harmful when compounded by dehydration or heat stress.
Moderate exercise is nephroprotective. Regular aerobic resistance activity improves insulin sensitivity, vascular tone, oxidative balance, and intraglomerular pressure, slowing CKD progression in metabolic disease.
Post-endurance creatinine elevation is often physiologic. Increased skeletal muscle breakdown raises serum creatinine without true filtration decline; urine output and cystatin-C help distinguish pseudo-AKI from real injury.
Exercise-induced proteinuria reflects transient glomerular stress. Increased filtration fraction and permeability during high-intensity activity allow temporary albumin passage that resolves with recovery.
Heat stress markedly amplifies AKI risk. Hyperthermia reduces renal perfusion and promotes oxidative injury; rapid external cooling is the primary intervention in exertional heat stroke.
Hydration strategy must be individualized — not maximal. Matching intake to sweat loss preserves renal perfusion, whereas excess hypotonic fluids predispose to exercise-associated hyponatremia.
Body-weight tracking is the most practical hydration gauge. A 1-kg postexercise loss approximates 1 L fluid deficit; replacing ~1.5 L/kg restores plasma volume safely.
Rhabdomyolysis injures kidneys via myoglobin toxicity. Tubular obstruction, vasoconstriction, and oxidative stress occur with marked CK elevation; early isotonic saline targeting high urine flow is key.
NSAIDs impair renal adaptive vasodilation during exertion. Prostaglandin inhibition compromises medullary perfusion, increasing susceptibility to exercise-related AKI.
Sports drink selection depends on duration. Water is sufficient for short activity; prolonged exercise benefits from low-carbohydrate (≈3–5%) electrolyte drinks that enhance absorption without slowing gastric emptying.
Creatine supplementation can mimic kidney dysfunction. Mild creatinine rise reflects metabolism rather than injury; cystatin-C better estimates true GFR.
Exercise remains therapeutic in CKD — including dialysis. Structured programs improve VO₂ capacity, endothelial function, inflammation, and quality of life when supervised.
Children with CKD benefit from sport participation. Age-appropriate activity improves strength and cardiovascular health; restrictions should be individualized rather than diagnosis-driven.
Recurrent exertional AKI warrants deeper evaluation. Consider hereditary renal hypouricemia, metabolic myopathies, supplement misuse, or inadequate recovery patterns.
ajkd.org/article/S0272-6386(…
1
7
42
2,033

References:
Roberts et al. Post-exercise cold water immersion attenuates acute anabolic signalling and long-term adaptations in muscle to strength training. J Physiol. 2015 Aug 13;593
Cold water immersion DECREASES testosterone “While exercising, the serum TS level significantly increased by 20.8% (p less than 0.05), the luteinizing hormone (LH) level by 3.6% (p less than 0.05) and noradrenaline (NA) level by 140.0% (p less than 0.01). During cold water stimulation, TS decreased by 10.0%, LH increased by 22.1% and NA decreased by 23.8%.“
Reference:K Sakamoto et al. Effects of physical exercise in cold stimulation on serum testosterone level in men. Nihon Eiseigaku Zasshi. 1991 Jun.
And BLUNTS post-exercise Testosterone rise Reference: Cold-water immersion blunts and delays increases in circulating testosterone and cytokines post-resistance exercise
Jacob E Earp et al. Eur J Appl Physiol. 2019 Aug
Throwing cold water on muscle growth: A systematic review with meta-analysis of the effects of postexercise cold water immersion on resistance training-induced hypertrophy
Effects of post-exercise cold-water immersion on resistance training-induced gains in muscular strength: a meta-analysis
1
1
496
References:
Roberts et al. Post-exercise cold water immersion attenuates acute anabolic signalling and long-term adaptations in muscle to strength training. J Physiol. 2015 Aug 13;593
Cold water immersion DECREASES testosterone “While exercising, the serum TS level significantly increased by 20.8% (p less than 0.05), the luteinizing hormone (LH) level by 3.6% (p less than 0.05) and noradrenaline (NA) level by 140.0% (p less than 0.01). During cold water stimulation, TS decreased by 10.0%, LH increased by 22.1% and NA decreased by 23.8%.“
Reference:K Sakamoto et al. Effects of physical exercise in cold stimulation on serum testosterone level in men. Nihon Eiseigaku Zasshi. 1991 Jun.
And BLUNTS post-exercise Testosterone rise Reference: Cold-water immersion blunts and delays increases in circulating testosterone and cytokines post-resistance exercise
Jacob E Earp et al. Eur J Appl Physiol. 2019 Aug
Throwing cold water on muscle growth: A systematic review with meta-analysis of the effects of postexercise cold water immersion on resistance training-induced hypertrophy
Effects of post-exercise cold-water immersion on resistance training-induced gains in muscular strength: a meta-analysis
1
2
2,553
References below:👇
Cold water immersion DECREASES testosterone levels after exercise “While exercising, the serum TS level significantly increased by 20.8% (p less than 0.05), the luteinizing hormone (LH) level by 3.6% (p less than 0.05) and noradrenaline (NA) level by 140.0% (p less than 0.01). During cold water stimulation, TS decreased by 10.0%, LH increased by 22.1% and NA decreased by 23.8%.“
Reference:K Sakamoto et al. Effects of physical exercise in cold stimulation on serum testosterone level in men. Nihon Eiseigaku Zasshi. 1991 Jun.
And BLUNTS post-exercise Testosterone rise
Reference: Cold-water immersion blunts and delays increases in circulating testosterone and cytokines post-resistance exercise
Jacob E Earp et al. Eur J Appl Physiol. 2019 Aug
Other references on cold plunge reducing exercise gains
Roberts et al. Post-exercise cold water immersion attenuates acute anabolic signalling and long-term adaptations in muscle to strength training. J Physiol. 2015 Aug 13;593
Throwing cold water on muscle growth: A systematic review with meta-analysis of the effects of postexercise cold water immersion on resistance training-induced hypertrophy
Effects of post-exercise cold-water immersion on resistance training-induced gains in muscular strength: a meta-analysis
8
2,661
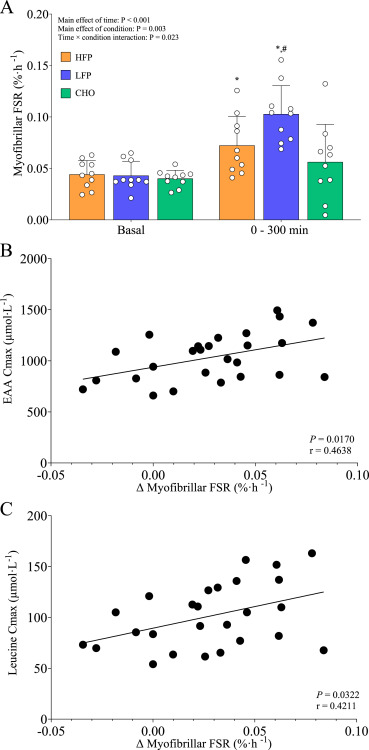
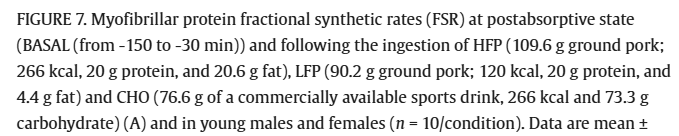
Postexercise muscle protein synthesis: low fat protein (lean pork) > high fat protein (fatty pork) = carbs
3
1
9
1,235