
hypnotiseur, amoureux du pouls radial et respirant à votre rythme...
Joined October 2012
- Tweets 5,893
- Following 237
- Followers 34
- Likes 7,664
1 Photos and videos

imran robleh retweeted

Jun 12
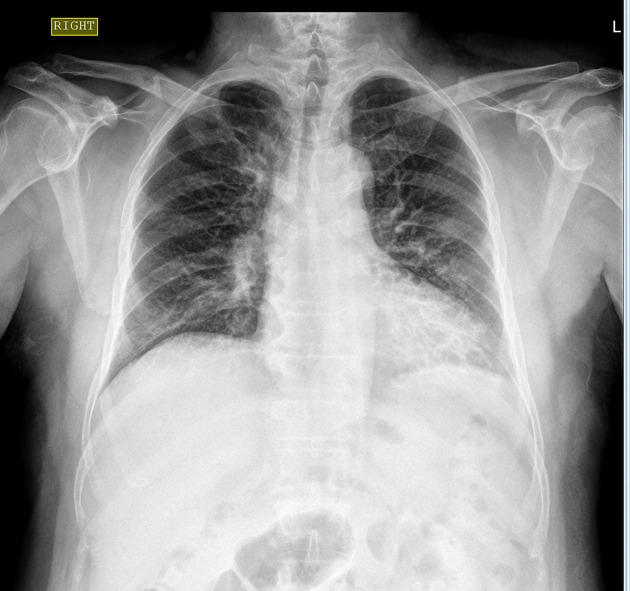
A man in his 60s presented with complaints are cough with sputum, cold, body ache for 3 days.
No fever, or difficulty in breathing.
What can be seen here?
4
8
36
4,467
imran robleh retweeted
Jun 11
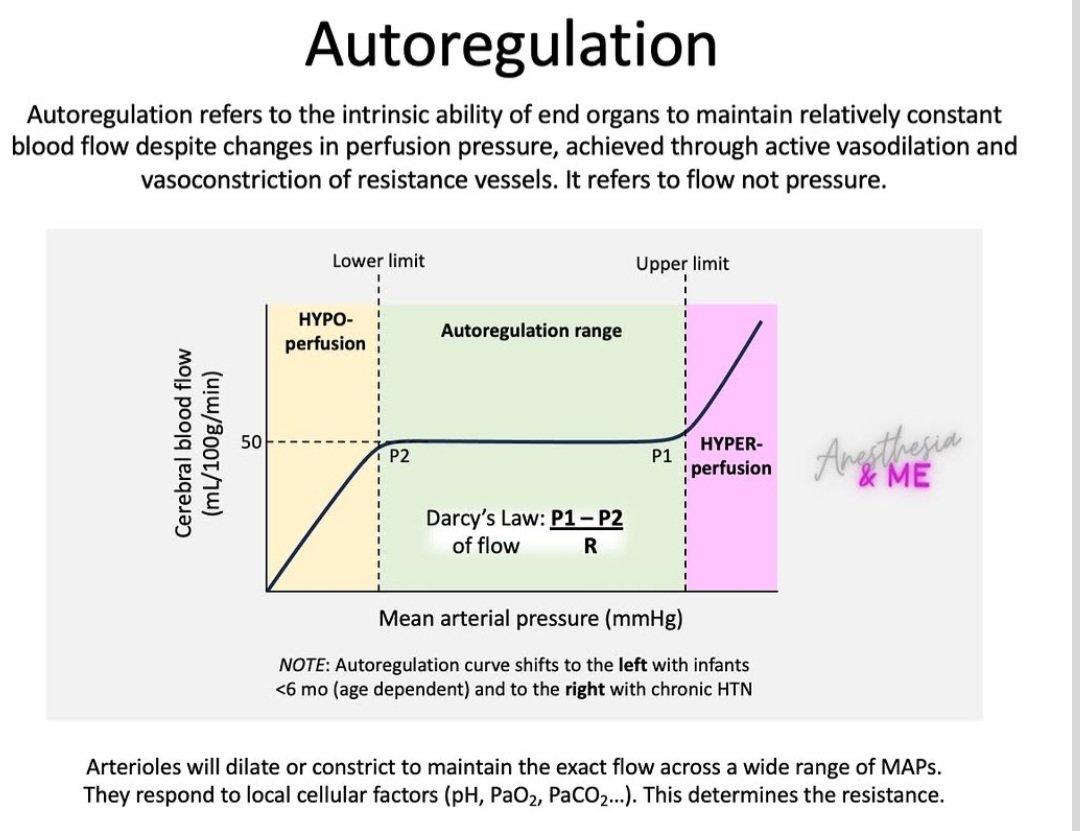
Cerebral autoregulation is the local mechanism that keeps cerebral blood flow (CBF) stable despite variations in mean arterial pressure (MAP).
*Autoregulation allows end organs, such as the brain, to maintain consistent blood flow despite fluctuations in perfusion pressure.
*This mechanism relies on active constriction or dilation of resistance vessels based on local factors like carbon dioxide levels.
*The curve shifts to the right in cases of chronic hypertension, meaning higher pressures are required to maintain flow.
*Conversely, the curve shifts to the left for infants younger than six months due to immature adaptive mechanisms.
instagram.com/p/DZaJPTFILuF/…
13
37
1,233
imran robleh retweeted
Jun 11
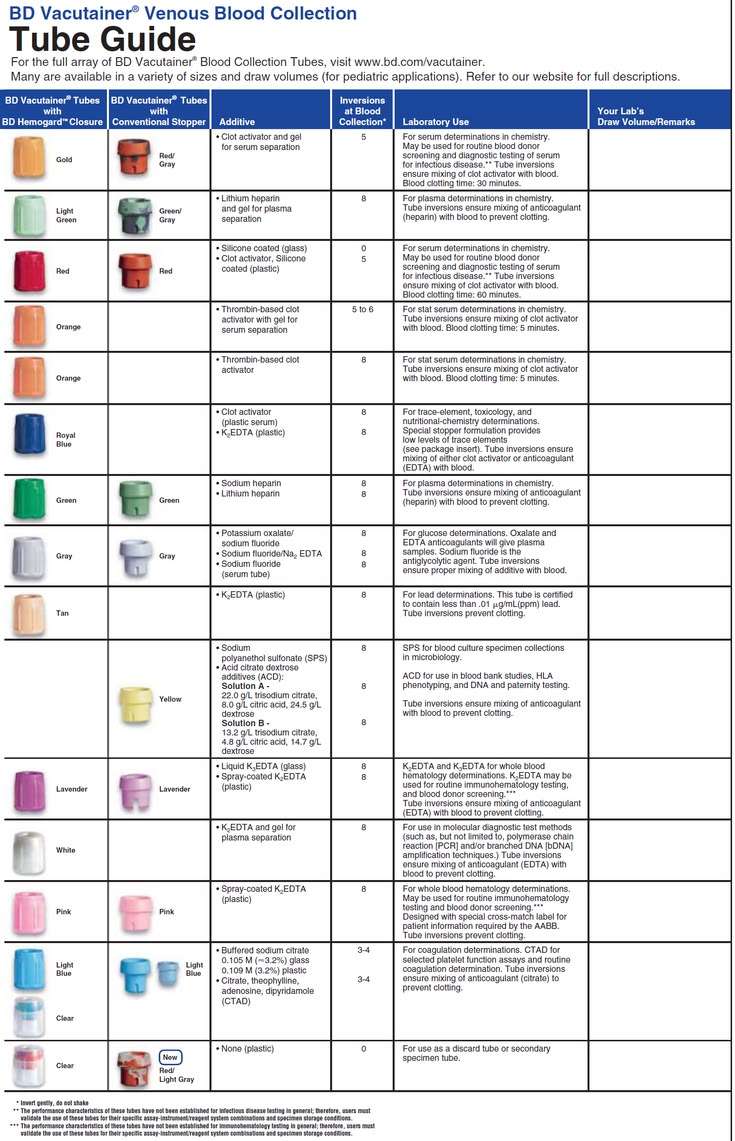
BD Vacutainer Venous Blood Collection Tube Guide.
interpathlab.com/bd-vacutain…
7
12
660
imran robleh retweeted
Jun 11
A highly structured pharmacology summary chart for diuretics.
@ManualOMedicine

2
36
111
3,492
imran robleh retweeted

🫁 𝗣𝗦𝗩, 𝗖𝗣𝗔𝗣 𝘆 𝗡𝗜𝗩: 𝗲𝗻𝘁𝗲𝗻𝗱𝗲𝗿 𝗹𝗮𝘀 𝗽𝗿𝗲𝘀𝗶𝗼𝗻𝗲𝘀 𝗲𝘀 𝗲𝗻𝘁𝗲𝗻𝗱𝗲𝗿 𝗹𝗮 𝘃𝗲𝗻𝘁𝗶𝗹𝗮𝗰𝗶𝗼́𝗻.
⬇️⬇️⬇️⬇️
🔹 𝘾𝙋𝘼𝙋 = 𝙪𝙣𝙖 𝙨𝙤𝙡𝙖 𝙥𝙧𝙚𝙨𝙞𝙤́𝙣 𝙘𝙤𝙣𝙩𝙞𝙣𝙪𝙖
✅ Aumenta la capacidad residual funcional.
✅ Recluta alvéolos y mejora la oxigenación.
💡 Útil en edema agudo cardiogénico de pulmón y apnea obstructiva del sueño.
🔹 𝘽𝙞𝙋𝘼𝙋/𝙉𝙄𝙑 = 𝙙𝙤𝙨 𝙣𝙞𝙫𝙚𝙡𝙚𝙨 𝙙𝙚 𝙥𝙧𝙚𝙨𝙞𝙤́𝙣
📈 𝙄𝙋𝘼𝙋: ayuda a la inspiración y aumenta el volumen corriente.
📉 𝙀𝙋𝘼𝙋: mantiene el reclutamiento alveolar y mejora la oxigenación.
🧮 𝙎𝙤𝙥𝙤𝙧𝙩𝙚 𝙙𝙚 𝙥𝙧𝙚𝙨𝙞𝙤́𝙣 = 𝙄𝙋𝘼𝙋 − 𝙀𝙋𝘼𝙋
Ejemplo:
➡️ IPAP 15 cmH₂O
➡️ EPAP 5 cmH₂O
➡️ Soporte = 10 cmH₂O
🔹 𝙋𝙎𝙑 𝙚𝙣 𝙫𝙚𝙣𝙩𝙞𝙡𝙖𝙘𝙞𝙤́𝙣 𝙞𝙣𝙫𝙖𝙨𝙞𝙫𝙖
⚙️ El soporte de presión se suma a la PEEP:
🧮 𝙋𝙧𝙚𝙨𝙞𝙤́𝙣 𝙥𝙞𝙘𝙤 = 𝙋𝙀𝙀𝙋 𝙋𝙎𝙑
Ejemplo:
➡️ PSV 15 cmH₂O
➡️ PEEP 5 cmH₂O
➡️ PIP ≈ 20 cmH₂O
📈 ¿𝙌𝙪𝙚́ 𝙙𝙚𝙩𝙚𝙧𝙢𝙞𝙣𝙖 𝙚𝙡 𝙫𝙤𝙡𝙪𝙢𝙚𝙣 𝙘𝙤𝙧𝙧𝙞𝙚𝙣𝙩𝙚?
⬆️ Mayor soporte de presión (ΔP).
⬆️ Mayor tiempo inspiratorio.
⬆️ Mejor compliance pulmonar.
⬆️ Mayor esfuerzo inspiratorio del paciente.
⚡ 𝙈𝙚𝙣𝙨𝙖𝙟𝙚 𝙘𝙡𝙖𝙫𝙚:
🔵 𝘾𝙋𝘼𝙋 𝙢𝙚𝙟𝙤𝙧𝙖 𝙥𝙧𝙞𝙣𝙘𝙞𝙥𝙖𝙡𝙢𝙚𝙣𝙩𝙚 𝙡𝙖 𝙤𝙭𝙞𝙜𝙚𝙣𝙖𝙘𝙞𝙤́𝙣.
🟢 𝘽𝙞𝙋𝘼𝙋 𝙖𝙣̃𝙖𝙙𝙚 𝙨𝙤𝙥𝙤𝙧𝙩𝙚 𝙫𝙚𝙣𝙩𝙞𝙡𝙖𝙩𝙤𝙧𝙞𝙤 𝙮 𝙚𝙡𝙞𝙢𝙞𝙣𝙖 𝘾𝙊₂.
🟣 𝙋𝙎𝙑 𝙥𝙚𝙧𝙢𝙞𝙩𝙚 𝙖𝙨𝙞𝙨𝙩𝙞𝙧 𝙚𝙡 𝙚𝙨𝙛𝙪𝙚𝙧𝙯𝙤 𝙙𝙚𝙡 𝙥𝙖𝙘𝙞𝙚𝙣𝙩𝙚, 𝙖𝙟𝙪𝙨𝙩𝙖𝙣𝙙𝙤 𝙥𝙧𝙚𝙨𝙞𝙤́𝙣 𝙮 𝙨𝙞𝙣𝙘𝙧𝙤𝙣𝙞́𝙖.
🧠 𝘕𝘰 𝘴𝘦 𝘱𝘳𝘰𝘨𝘳𝘢𝘮𝘢 𝘶𝘯𝘢 𝘱𝘳𝘦𝘴𝘪𝘰́𝘯; 𝘴𝘦 𝘵𝘳𝘢𝘵𝘢 𝘶𝘯𝘢 𝘧𝘪𝘴𝘪𝘰𝘭𝘰𝘨𝘪́𝘢. 𝘈𝘫𝘶𝘴𝘵𝘢 𝘐𝘗𝘈𝘗, 𝘌𝘗𝘈𝘗 𝘺 𝘗𝘚𝘝 𝘴𝘦𝘨𝘶́𝘯 𝘭𝘢 𝘮𝘦𝘤𝘢́𝘯𝘪𝘤𝘢 𝘱𝘶𝘭𝘮𝘰𝘯𝘢𝘳, 𝘦𝘭 𝘪𝘯𝘵𝘦𝘳𝘤𝘢𝘮𝘣𝘪𝘰 𝘨𝘢𝘴𝘦𝘰𝘴𝘰 𝘺 𝘦𝘭 𝘦𝘴𝘧𝘶𝘦𝘳𝘻𝘰 𝘳𝘦𝘴𝘱𝘪𝘳𝘢𝘵𝘰𝘳𝘪𝘰 𝘥𝘦𝘭 𝘱𝘢𝘤𝘪𝘦𝘯𝘵𝘦.
#VNI 🫁⚡
‼️Si te sirve: ❤️ Me gusta | 🔁 Repost | ➕ Follow para más👇🏼👇🏼👇🏼👇🏼
📚📖#ClubCrit👨🏻⚕️👨🏻🏫🧠🫶
#ClubCrit #EvidenceBasedMedicine #CriticalCare #CriticalCare #FOAMed #FOAMcc #CuidadoCrítico #MedTwitter #CritCare #icu #intensivecare #diagnosis #management #UCI #MedicinaBasadaEnEvidencia #MedEd #MedX #IntensiveCare #MedIntensiva #MedXCommunity #MedED #ICUmanagement #MustRead #LecturaRecomendada

28
64
1,168
imran robleh retweeted

🧠 Hypertonic Saline vs Mannitol in Severe Traumatic Brain Injury: Is There a Winner?
Hyperosmolar therapy remains a cornerstone of intracranial hypertension management after severe TBI, but the optimal agent is still debated.
A recent systematic review including 9 studies and 979 adult patients compared hypertonic saline (HTS) with mannitol. HTS demonstrated several potential advantages:
🔹 Faster and more sustained reduction of intracranial pressure (ICP).
🔹 Lower recurrence of intracranial hypertension episodes.
🔹 Reduced treatment failure rates in refractory ICP elevation.
🔹 More prolonged osmotic effect compared with mannitol.
However, not all studies showed superiority. Nearly half reported similar efficacy between both agents regarding ICP control and clinical outcomes.
Importantly:
✅ HTS may provide better maintenance of cerebral perfusion by expanding intravascular volume without the diuretic effects of mannitol.
✅ Mortality differences were not consistently demonstrated.
✅ Functional neurological outcomes remain uncertain.
The practical message for intensivists and neurocritical care clinicians is that both agents remain reasonable options, but current evidence increasingly favors HTS when sustained ICP control is the primary therapeutic goal.
Further large, multicenter randomized trials are still needed to define whether physiological advantages translate into meaningful improvements in long-term neurological outcomes.
#NeurocriticalCare #TBI #ICP #CriticalCare #Trauma #NeuroICU #HypertonicSaline #Mannitol #BrainInjury #IntensiveCare
Reference 📚
Expósito A, Silva AN, Capelo NM, Zamora CF, Cuji DG. Efficacy of hypertonic saline versus mannitol in adult patients with severe head trauma: systematic review. Revista Gregoriana de Ciencias de la Salud. 2026;3(1):186-202. DOI: 10.36097/rgcs.v3i1.3213.

ALT
2
15
60
1,910
imran robleh retweeted

Jun 14
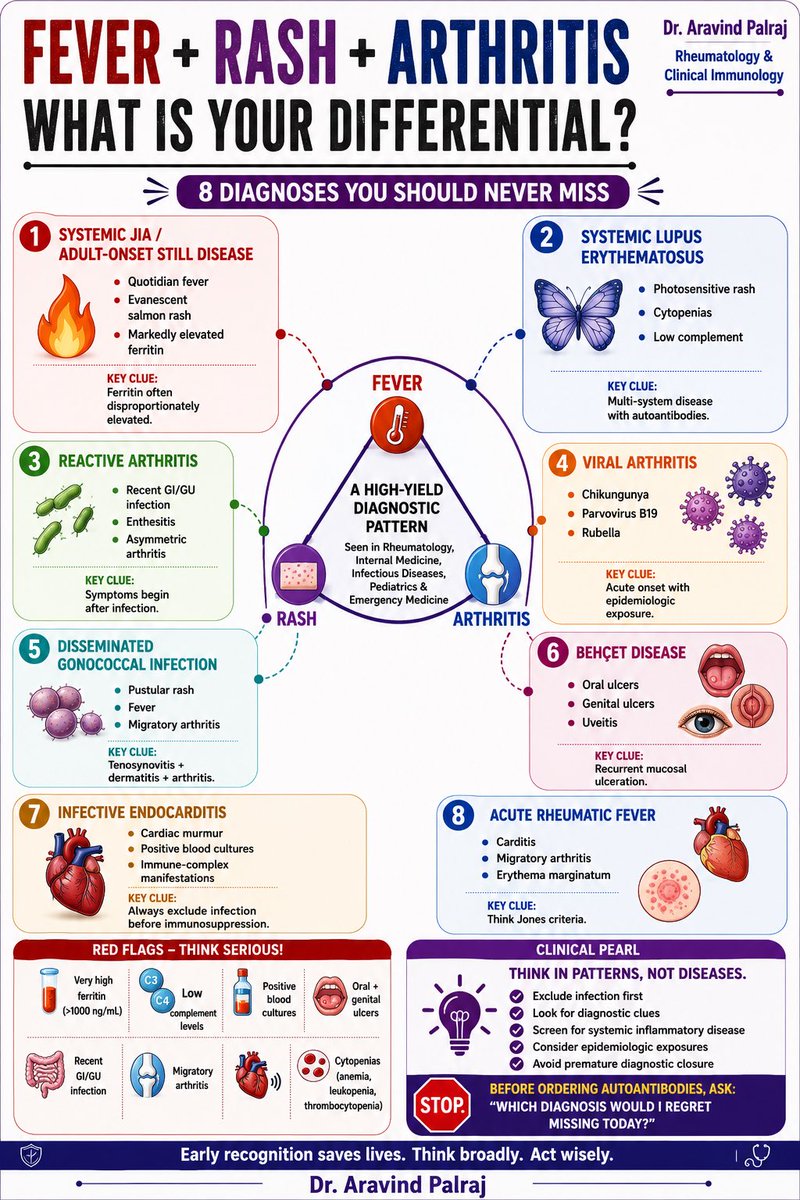
FEVER RASH ARTHRITIS
One of the most important diagnostic patterns in medicine.
When these three features occur together, the differential diagnosis extends far beyond rheumatology and includes infection, systemic inflammatory disease, autoimmunity, and post-infectious syndromes.
Key diagnoses you should never miss:
• Adult-onset Still disease / Systemic JIA
• SLE
• Reactive arthritis
• Viral arthritis
• Disseminated gonococcal infection
• Behçet disease
• Infective endocarditis
• Acute rheumatic fever
Before ordering a large autoimmune panel, ask yourself:
Which diagnosis would I regret missing today?
What would be your first differential when faced with a patient presenting with fever, rash, and arthritis?
Infographic by Dr. Aravind Palraj
#Rheumatology #InternalMedicine #MedicalEducation #MedEd #FOAMed #ClinicalReasoning #DifferentialDiagnosis #AutoimmuneDisease #MedTwitter #RheumTwitter #InfectiousDiseases #MedX #MedicalStudents #Residency #Medicine @IhabFathiSulima @docakx
2
47
94
2,976

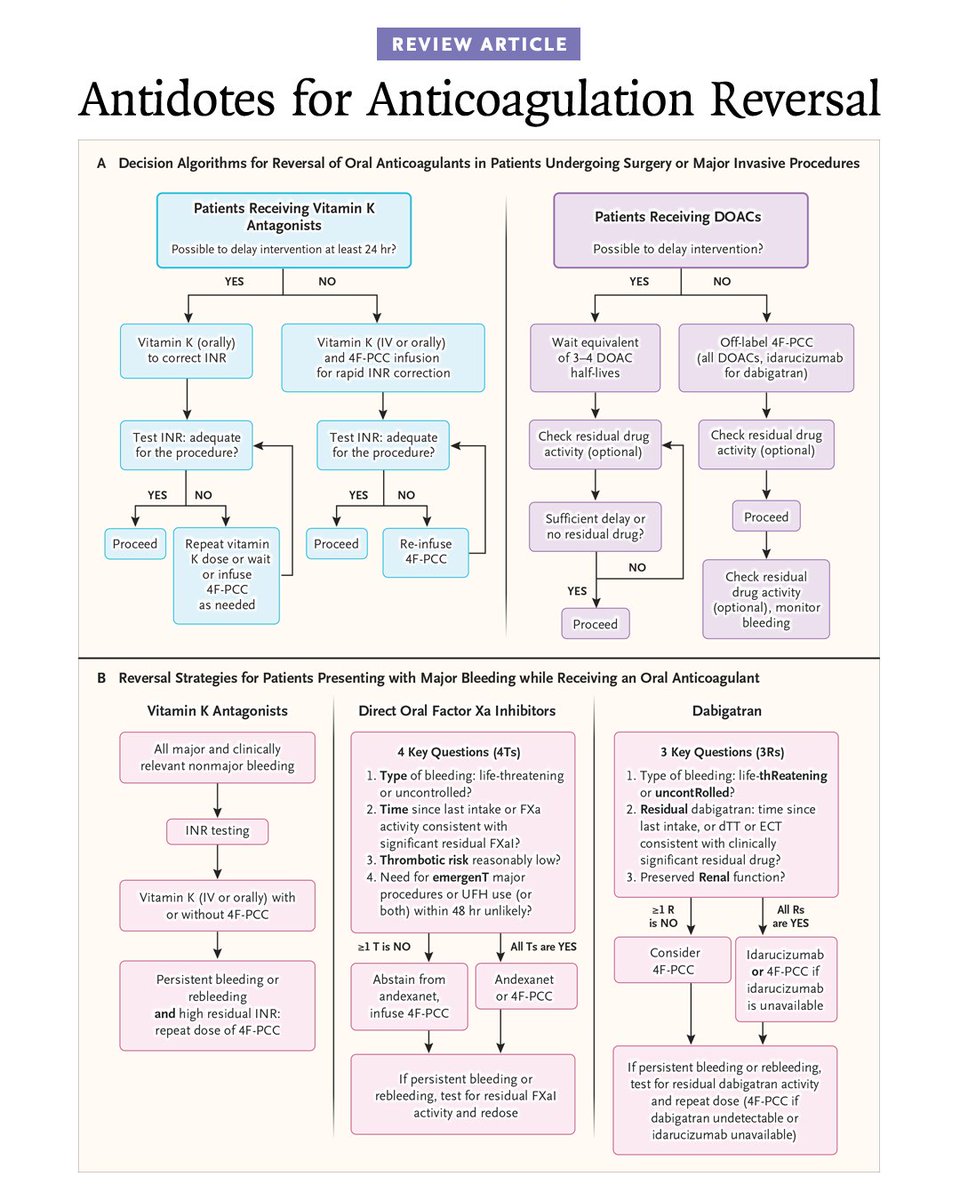
𝗦𝘂𝗴𝗴𝗲𝘀𝘁𝗲𝗱 𝗥𝗲𝘃𝗲𝗿𝘀𝗮𝗹 𝗦𝘁𝗿𝗮𝘁𝗲𝗴𝗶𝗲𝘀 𝗼𝗳 𝗢𝗿𝗮𝗹 𝗔𝗻𝘁𝗶𝗰𝗼𝗮𝗴𝘂𝗹𝗮𝗻𝘁 𝗨𝘀𝗲 𝗳𝗼𝗿 𝗠𝗮𝗷𝗼𝗿 𝗕𝗹𝗲𝗲𝗱𝗶𝗻𝗴 𝗮𝗻𝗱 𝗯𝗲𝗳𝗼𝗿𝗲 𝗘𝗺𝗲𝗿𝗴𝗲𝗻𝗰𝘆 𝗦𝘂𝗿𝗴𝗲𝗿𝘆.
As shown in Panel A, reversal management depends on the urgency of surgery or the invasive procedure. Reversal management includes administration of oral or intravenous (IV) vitamin K with or without 4F-PCC, depending on the timing of the procedure (emergency or urgent), baseline international normalized ratio (INR) value, and presence (or absence) of active bleeding. For patients receiving direct oral anticoagulants (DOACs), the decision also depends on time to surgery. Decision making is informed by DOAC type, time since last dose, half-life, presence (or absence) of active bleeding, and renal function tests to estimate residual drug activity.
Panel B shows reversal strategies for patients presenting with major bleeding while receiving an oral anticoagulant. The reversal strategy of vitamin K antagonists includes vitamin K given intravenously or orally, combined with 4F-PCC and INR testing. Management of anticoagulant reversal of direct oral FXaIs is based on four key factors (shown as the 4Ts): type of bleeding, timing of the last dose, thrombotic risk, and need for invasive procedures in the next 48 hours that would result in the administration of UFH. These factors may facilitate the use of specific (e.g., andexanet alfa) or nonspecific (e.g., 4F-PCC) antidotes. The reversal of dabigatran is informed by three clinical variables (shown as the 3Rs) — the type of bleeding, time of the last dose of dabigatran, and preserved renal function.
Learn more in the Review Article “Antidotes for Anticoagulation Reversal” by Bianca Rocca, MD, PhD, and Hugo ten Cate, MD, PhD: nej.md/4xgOUdI
NEJM subscribers: Explore this article deeper with AI Companion.
84
275
19,747
imran robleh retweeted

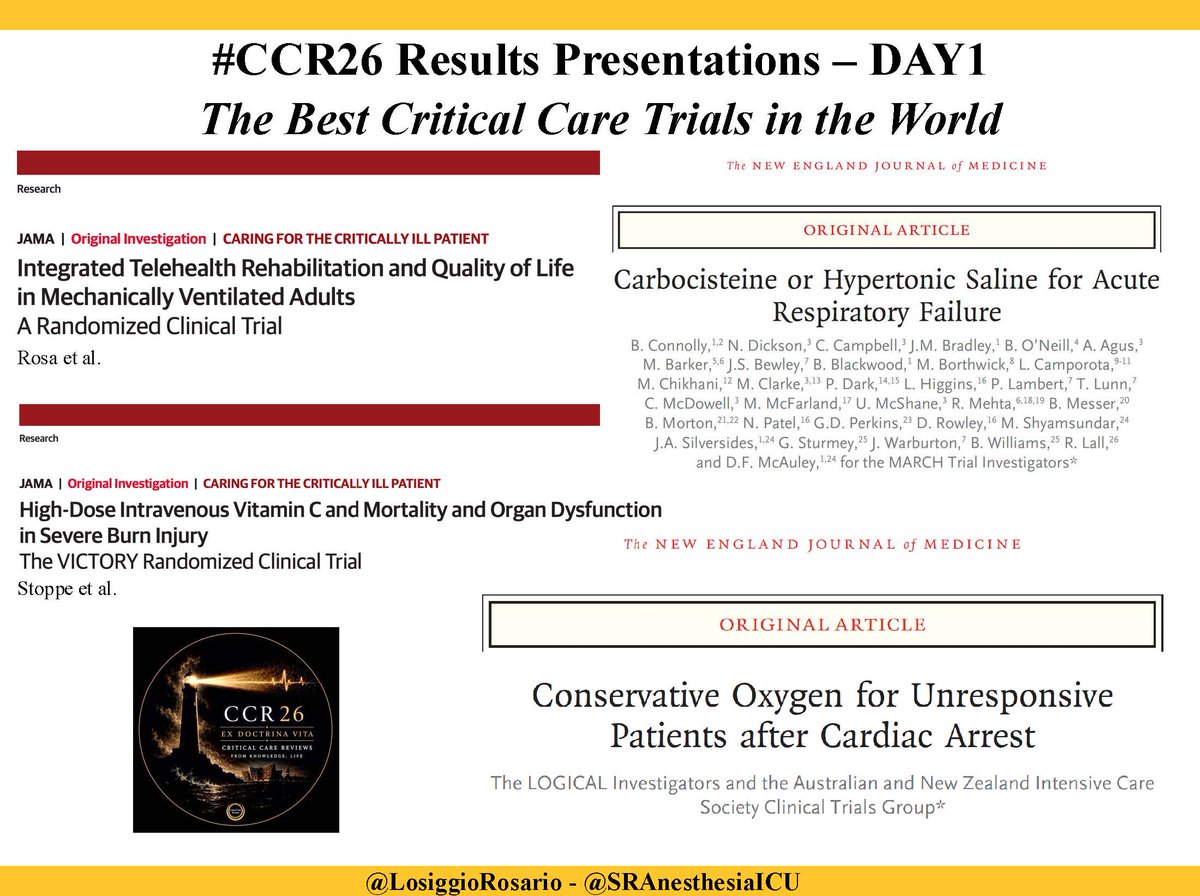
Day1 at #CCR26
#LOGICALtrial: conservative O₂ after cardiac arrest
#MARCHtrial: carbocisteine /or HTS for airway secretions
#VICTORYtrial: high-dose IV vitaminC in burns
None improved outcomes; MARCH and VICTORY➡️possible harm!
✅#TeleRehabTrial: in AHRF pts, ⬆️QoL ⬇️mortality
2
12
25
2,421
imran robleh retweeted

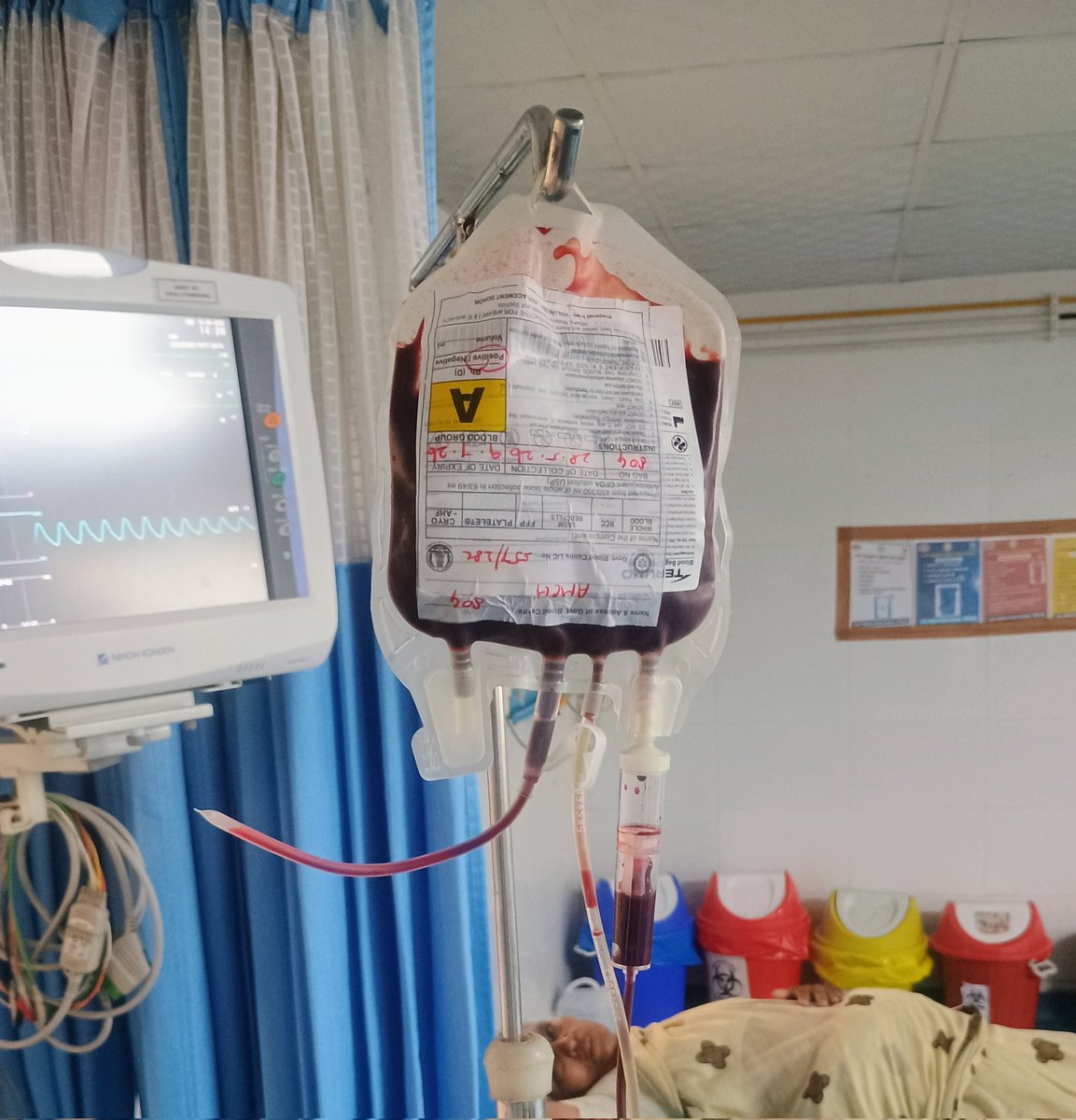
Jun 12
This blood 🩸 bag 🛍️ has 4 ports at the bottom.
Why does a single unit of blood need so many access points? 🤔
24
17
215
86,319
imran robleh retweeted

Jun 12
DKA Patient. Blood sugar 650 mg/dL.
If the intern reaches for IV insulin & i would stop him first
❌ Wrong first move why?
Always assess ABCD first:
Airway
Breathing (Kussmaul respirations?)
Circulation
Disability (mental status)
Then the real priority:
IV Fluids FIRST (0.9% Normal Saline) before even starting IV insulin.
In DKA, the patient is profoundly dehydrated (often 5–8 L fluid deficit) from osmotic diuresis. The high sugar is only part of the problem.
Giving insulin immediately can be dangerous because:
➡️ Insulin drives glucose AND potassium into cells.
➡️ Serum K⁺ can crash suddenly :- fatal arrhythmias.
➡️ Rapid fall in serum osmolality can pull water into brain cells :- cerebral edema (especially in children).
The sequence is:
✅ Aggressive IV fluids
✅ Check potassium
✅ Replace K⁺ if needed
✅ Then start IV insulin infusion
DKA isn’t just a sugar high problem we need to address the dehydration electrolyte acid-base abnormality

2
20
146
14,916
imran robleh retweeted

Jun 11
But medicine is cruelly deceptive sometimes.
Pulse oximetry only tells you one thing:
➡️ What percentage of hemoglobin is carrying oxygen.
It does NOT tell you:
❌ How much hemoglobin the patient actually has
❌ Whether oxygen is reaching tissues
❌ Whether cells are even able to use that oxygen
That’s why a patient can have “perfect saturation” and still be critically hypoxic in conditions like:
• Severe anemia → no oxygen carrying capacity
• Carbon monoxide poisoning → falsely normal/high SpO₂
• Cyanide poisoning → oxygen cannot be utilized by cells
• Septic or cardiogenic shock → oxygen never reaches tissues adequately
This is the moment juniors realize:
A monitor showing “100%” does not always mean the patient is safe.
Real medicine starts when you stop treating numbers… and start understanding physiology.
2
18
127
8,388
imran robleh retweeted
❤️ Pressure-Volume Loops at the Bedside: Are We Finally Measuring What Really Matters in Cardiogenic Shock?
For decades, cardiogenic shock management has focused on cardiac output, blood pressure, filling pressures, lactate, and cardiac power.
A fascinating multicenter study published in the ASAIO Journal proposes a practical bedside method to estimate pressure-volume (PV) loop energetics using only pulmonary artery catheter and echocardiographic data, avoiding the need for invasive conductance catheters.
Why does this matter?
Traditional hemodynamic variables tell us about flow and pressure.
PV-loop analysis tells us about:
📌 Ventriculoarterial coupling (VAC)
📌 Ventricular efficiency
📌 Stroke work (SW)
📌 Potential energy (PE)
📌 Pressure-volume area (PVA)
📌 Myocardial energetic demand
These parameters may provide a much deeper understanding of whether a therapy truly unloads the failing ventricle.
Key Findings
🔹 Microaxial flow pump support in AMI-related cardiogenic shock
The most striking observation was a reduction in arterial elastance and improved ventriculoarterial coupling, accompanied by increased stroke work but decreased pressure-volume area.
This translated into an improvement in estimated ventricular efficiency from approximately 32% to 40%, suggesting genuine ventricular unloading and lower energetic expenditure.
🔹 IABP support in AMI-related shock
IABP improved ventriculoarterial coupling and reduced filling pressures but produced a more modest energetic effect compared with microaxial support.
🔹 Heart failure-related cardiogenic shock
The physiological response was far more heterogeneous. Changes in pressure-volume area and ventricular energetics were inconsistent, highlighting that device effects may depend strongly on shock etiology.
Why This Study Is Important
This work reinforces a concept increasingly discussed in advanced heart failure and shock programs:
The goal is not simply increasing cardiac output.
The goal is improving systemic perfusion while simultaneously reducing myocardial oxygen consumption and ventricular workload.
A patient can have a higher cardiac output while still operating at an unfavorable energetic state.
Pressure-volume analysis may reveal this hidden physiology.
Practical ICU Takeaway
When evaluating mechanical circulatory support, we should ask three questions:
1️⃣ Is systemic perfusion improving?
2️⃣ Is ventricular filling pressure decreasing?
3️⃣ Is ventricular energetic demand falling?
Only when all three occur simultaneously can we confidently say that true ventricular unloading has been achieved.
The future of cardiogenic shock management may be less about isolated hemodynamic variables and more about understanding the complete interaction between the ventricle and the arterial system.
Reference 📚
Ortega-Hernández JA. ASAIO Journal. 2026. DOI: 10.1097/MAT.0000000000002737.

ALT
1
21
55
2,354
imran robleh retweeted

Jun 12
A family member in the casualty was furious. "Doc, my father is unconscious from liver failure and you are just giving him a laxative to make him poop? He needs brain medicine!"
I had to explain that the laxative is the brain medicine.
27
29
483
66,066
imran robleh retweeted

24 Nov 2025
🧵 Albumin in Critical Care: 70 Years, 700 Papers… Zero Benefit
1/
Albumin is the most studied fluid in critical care.
Decades of trials. Endless meta-analyses.
And yet – not a single clinically meaningful benefit.
Here’s why the entire theory collapses once you understand Extended Starling. 👇
20
132
360
69,523
imran robleh retweeted

Jun 10
Version 2 of our ShockCalcs hemodynamics simulator is live. I've refined the physiology a ton, added new meds, and also a real-time Frank Starling curve that responds to fluids vasopressors.
Check it out (link in reply), and reply here with feedback on how to improve further!
4
21
120
9,490

imran robleh retweeted

facebook.com/share/r/1CfLffS…
📈 ECG Cheat Sheet 🎯
Drop a ❤️ if you find this helpful! Feel free to share!
#ECG #EKG #Cardiology #MedStudent
7
25
488
imran robleh retweeted

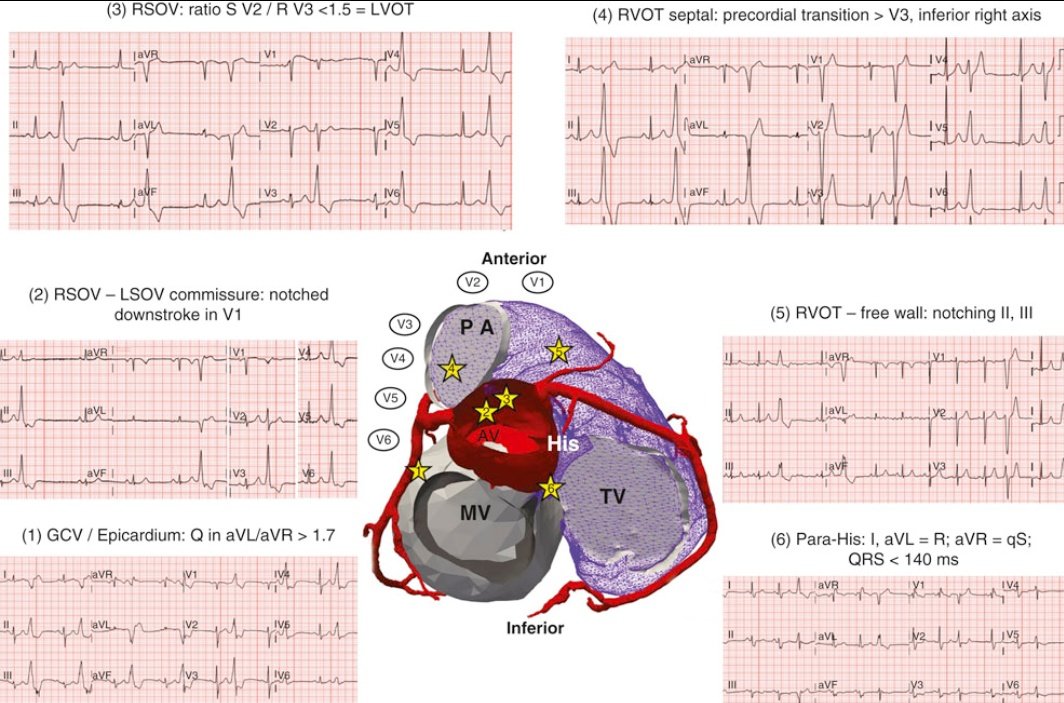
🧵 1/12
A PVC is not just an ectopic beat.
With careful analysis of the 12-lead ECG, it is often possible to predict where a PVC originates before entering the EP lab.
This figure summarizes key ECG clues for PVCs arising from the ventricular outflow tracts and ... ⬇️
1
43
136
6,452
imran robleh retweeted

A gift from us to you
Try this Ventilator Simulator, calculate total System and Trans-Pulmonary work/energy, its components
societymechanicalventilation…


8
14
1,312