
Joined January 2021
- Tweets 278
- Following 135
- Followers 121
- Likes 156
30 Photos and videos

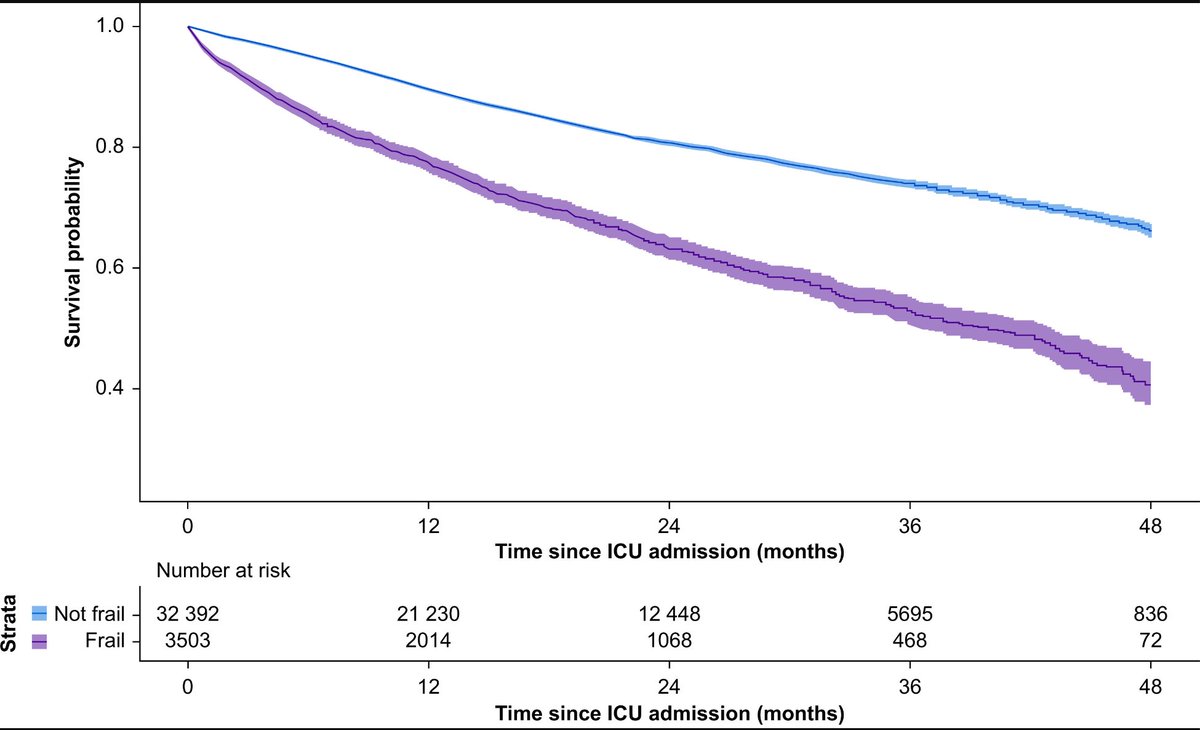






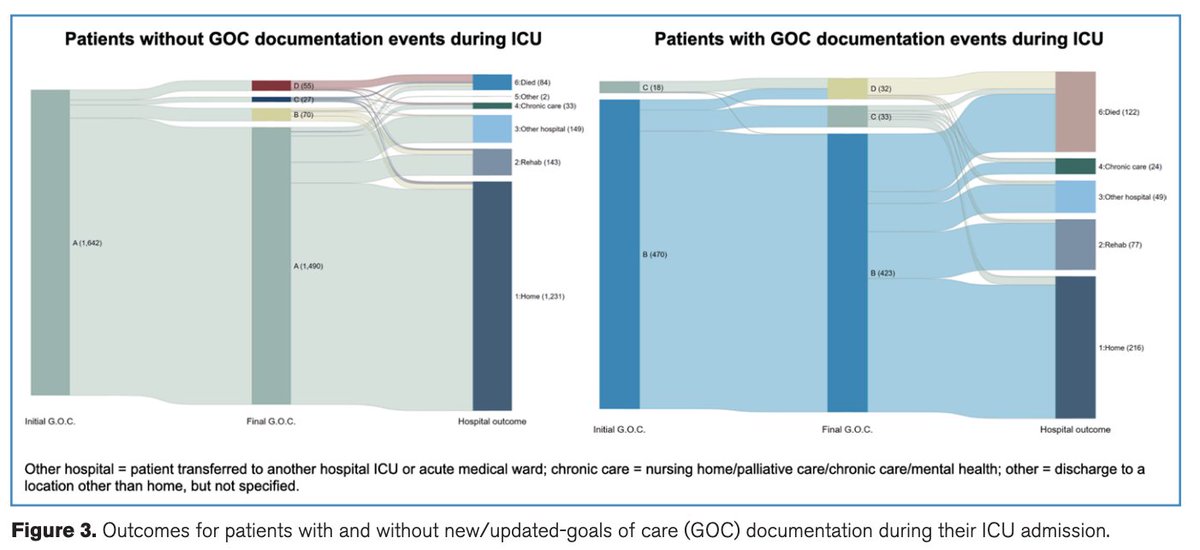
Increasing frailty was associated with increasing one-year mortality in ICU patients admitted from a MET review.
To read the full article in ‘Resuscitation’:
authors.elsevier.com/a/1mdSY…
DOI: 10.1016/j.resuscitation.2026.110995
Frailty and one year survival in patients admitted to the intensive care unit following a medical emergency team review: a retrospective registry-based study.
#ANZICSCORE
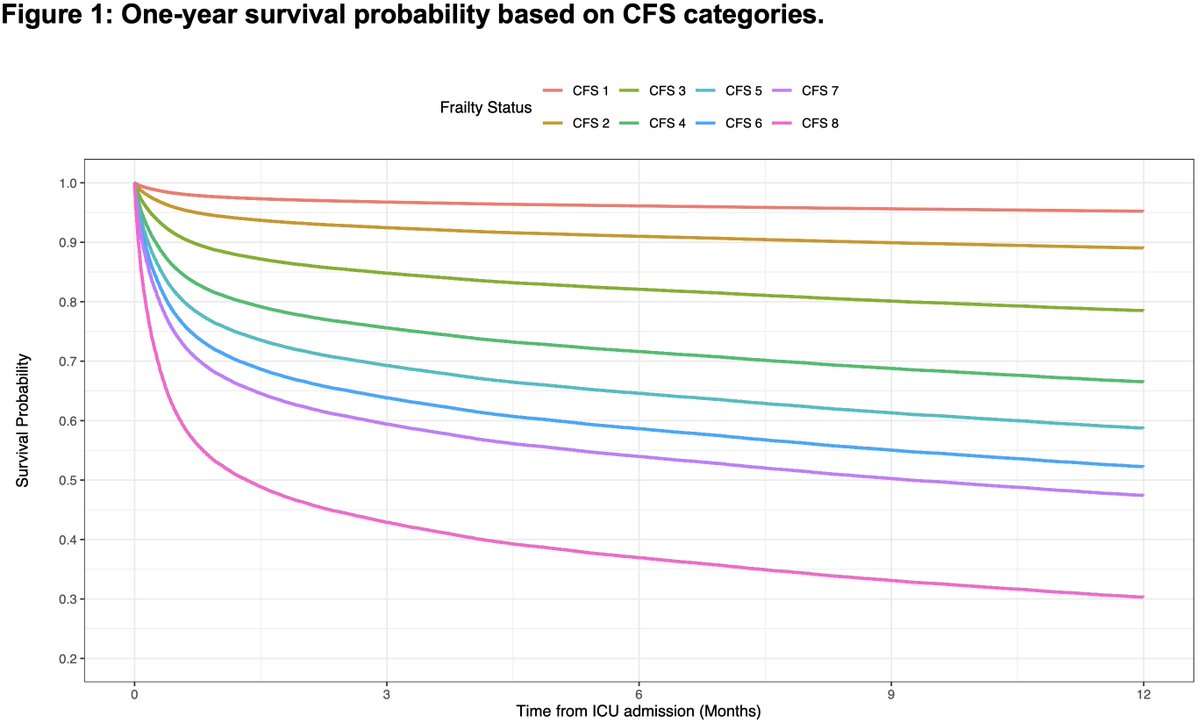
ALT Increasing frailty was associated with increasing one-year mortality in ICU patients admitted from a MET review.
4
9
541

10 Oct 2025
Had the privilege of working with Dr Bishoy Zakhary, @KrKrramanathan, @kshekar01 and @ELSOeducation team on #simulation-based education in its implementation in #ECMO. Excited to see what the future holds in this rapidly developing field!
7 Oct 2025

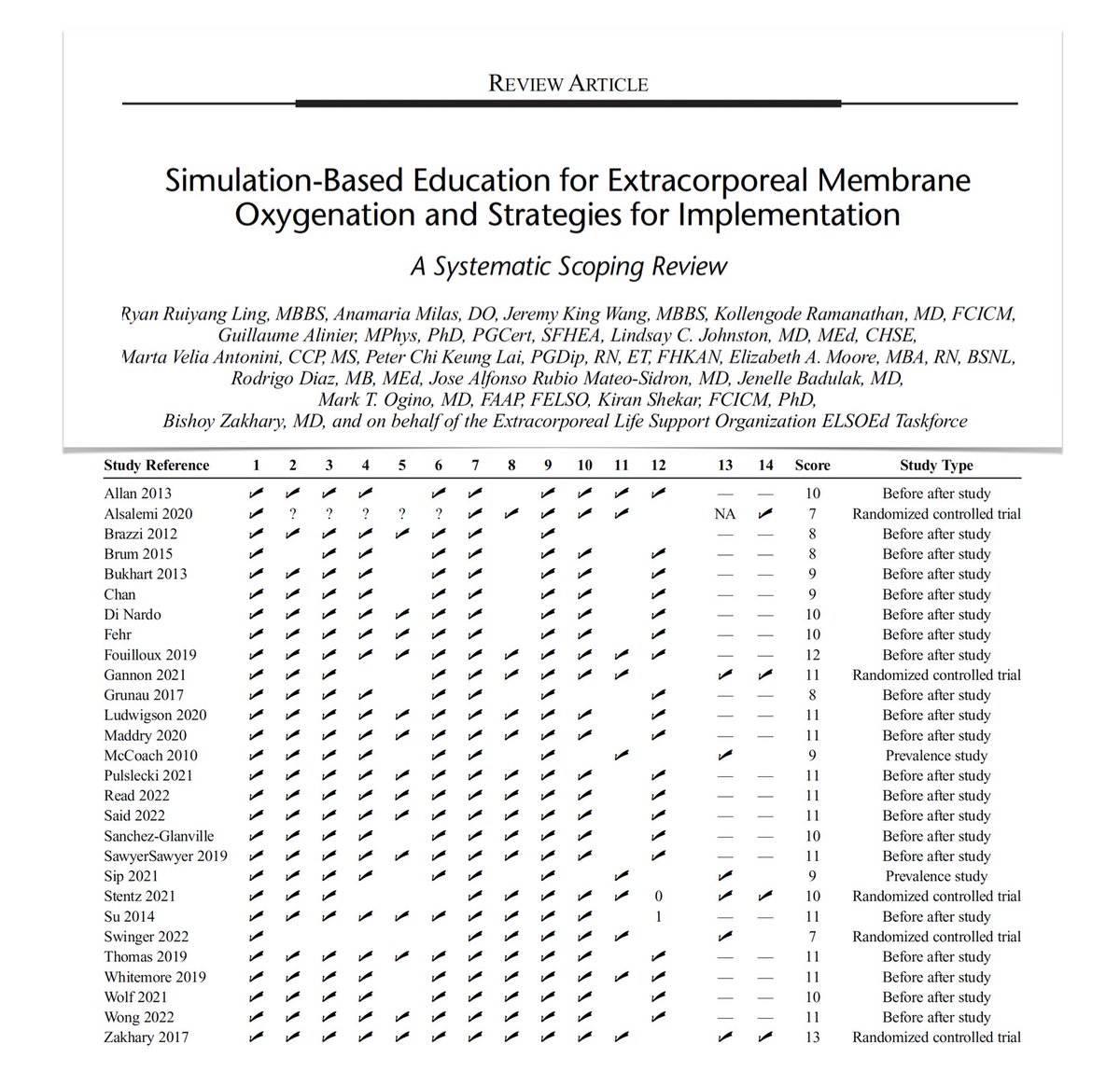
Simulation-based education for #ECMO & strategies for implementation: a systematic scoping review
🎓 SBE beneficial, improving competency scores, confidence, teamwork, troubleshooting, outcomes as times to critical actions and cannulation
🎓 retention of knowledge and skills over time unclear; regular simulation training may be beneficial
🎓 establishing standardized ECMO curricula, of which SBE should be a core component, crucial
🔗 bit.ly/48P6xYj
1
7
525
Ryan Ruiyang Ling retweeted

9 May 2025
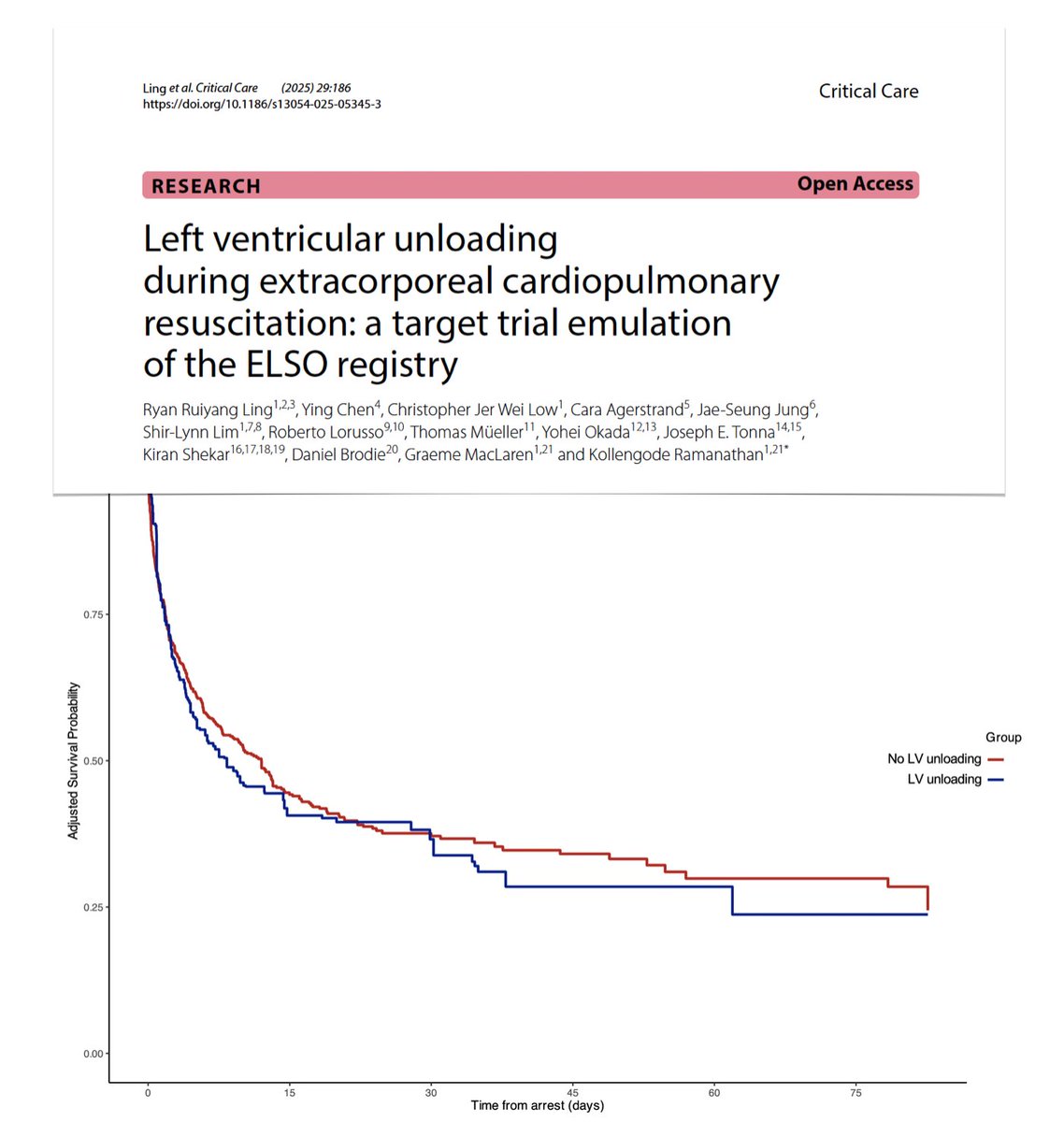
Left ventricular unloading in #ECPR
🔎 > 3.2K pts from ELSO Registry, 2020-2023
⚖️ 621 pairs (LV unloading /-) matched
🚧 LV unloading associated with higher complications
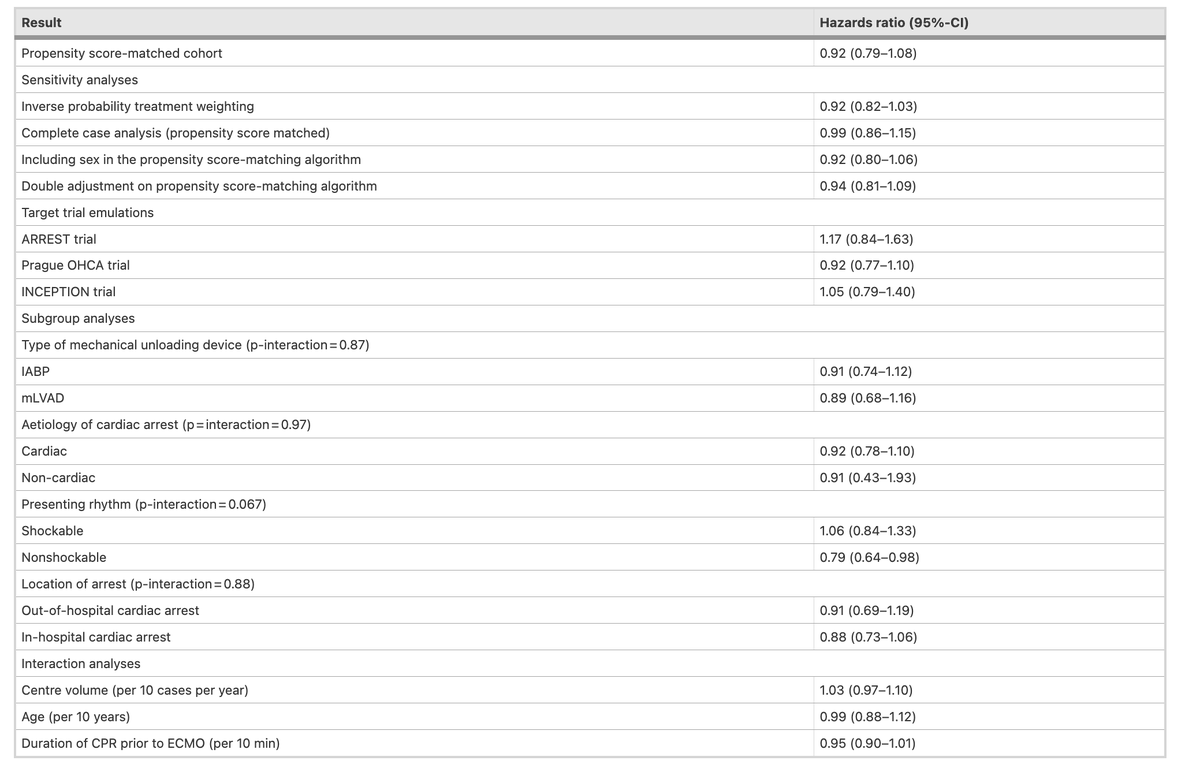
🫀not associated with improved survival/functional outcomes in context of #ECMO assisted CPR regardless of unloading device, etiology of CA, presenting rhythm, demographic or centre characteristics
#FOAMcc @Crit_Care
🔓rdcu.be/eln4M
20
35
4,053
9 May 2025
What is the impact of #LV #unloading during #ECPR? Target trial emulation using #ELSO registry:
🏥 300 centres, 621 matched pairs
❌ LV unloading NOT a/w survival benefits
💘 More CNS, CVS, and metabolic complications, and longer #ECMO durations!
link.springer.com/article/10…

8
11
1,395
Ryan Ruiyang Ling retweeted

31 Mar 2025
Takeaways from #ACC2025. Late breaking trials - take home points
@ACCinTouch
1. WARRIOR Trial : Intensive medical therapy did not significantly impact the rate of serious cardiovascular events at five years in women with suspected ischemia with nonobstructive coronary arteries (INOCA).
5
130
356
62,431
31 Mar 2025
Last year, I had the privilege of spending 2 months in Australia at @MonashHealth and @anzicrc under @catchdrash and @IntensiveDave.
One of the studies that we came up with was just published! @CritCareMed
journals.lww.com/ccmjournal/…
#intensivecare #FOAMcc #ICU
3
5
1,572
Ryan Ruiyang Ling retweeted

1 Feb 2025
This 🧵 is inspired by a conversation that @sundar__raghav and I recently had. This is for all of the trainees who will sign their first offer letter. As one that is almost 3 years to the date from the day I signed here are my tips 🧵1/6
1
6
13
2,810
Ryan Ruiyang Ling retweeted

30 Jan 2025
Excited to share our tool Resub that automatically formats your manuscript for any journal.
We designed Resub for clinical researchers who:
1) Hate wasting time formatting papers
2) Want to save hours per manuscript
3) Are committed to productivity and impact
You can trial it for free at resub.app/
Appreciate the repost and you sharing with any researchers you know 🙏
13
100
256
58,556
Ryan Ruiyang Ling retweeted

31 Jan 2025
🩸 Preoperative anemia and anemia treatment in cardiac surgery
📃: buff.ly/4cTBmcY
#anemia
3
5
152
Ryan Ruiyang Ling retweeted
23 Jan 2025
(1/x) High quality CPR, early defibrillation, and treating the underlying cause saves lives in cardiac arrest, but what else can we do?
Here are 7 advanced therapies for cardiac arrest👇
A🧵
Caution: Bleeding edge - evidence 'light' zone.
8
88
293
58,123
Ryan Ruiyang Ling retweeted
3 Jan 2025
Five predictions for critical care research in the next 5 years.
🧵(1/6)

2
27
94
23,763
Ryan Ruiyang Ling retweeted

7 Dec 2024
pEEG and ketamine
If youve spent any time around TIVA and EEG
You'll know that ketamine can increase the BIS number - Perhaps you never use ketamine because every time you do your processed EEG keeps telling you the patient's 'awake'
1/12
10
51
149
27,335

ICU Resuscitation Thoughts:
Every 2 y this time of the year I have to provide my hospital-employer w proof of ACLS recertification. I usually take an on-line course which I finish in a few hours. Sadly, this biennial ritual is also a reminder that we keep following the same #CPR

18
131
707
154,613
Ryan Ruiyang Ling retweeted
19 Nov 2024
(1/x) Here are the top things I think of when a patient with sepsis is worsening despite 'appropriate therapy'.
(note: it rarely is that the bug developed resistance..)
A 🧵
#medtwitter #foamed

8
75
298
70,763
Ryan Ruiyang Ling retweeted

23 Oct 2024
I struggle a lot conceptually with the fact that in some countries we give CAR-T, give 5th line expensive treatments, dialysis in 80 y, but find a bridge to decision LVAD in a 40 year old a too big investment if eg, egfr 30 ml/min or only 1.5 years after curative cancer treatment
3
5
49
11,543

My ARDS patient deteriorates and is now haemodynamically unstable, what do we do?
With Prof Luigi Camporota @Luigi_ICM @OliverHunsicker Jean-Louis Teboul and Lise Piquilloud
@ESICM #LIVES2024
4
18
54
14,875
Ryan Ruiyang Ling retweeted

18 Sep 2024
Why are haemodynamics so complicated and why have critical care physicians made such a mess of haemodynamic management over the years (eg aiming for high CVP)? A circular system means that a change at 1 point affects all the other points...
3
26
98
17,595
Ryan Ruiyang Ling retweeted
9 Sep 2024
🌊 When #ECMO-dependent patients are no longer candidates for destination therapy, should #ECLS be continued indefinitely? It would eventually serve only as a bridge to fatal complication. Complications might prolong suffering and affect quality of life. Beyond ethical dilemma/moral distress, continuing ECMO indefinitely would siphon resources away from
others who might benefit more.
With current technology, it is unlikely that indefinite ECMO in #ICU is the solution. However, maybe, in the future, ECMO will offer a comprehensive range of exit options including long-term care or home-based care in a cost-effective way. We eagerly await that future.
@TheLancet
🔗 bit.ly/4e0ifiQ
🕯️ Refers to comment on justifiability (or not) of unilateral withdrawing of ECMO when recovery or transition to final therapy no longer feasible. Continuing support without prospect of transition can be legitimate preference-sensitive choice for some patients?
🔗 bit.ly/3ToMk3g
1
17
36
8,384
8 Sep 2024
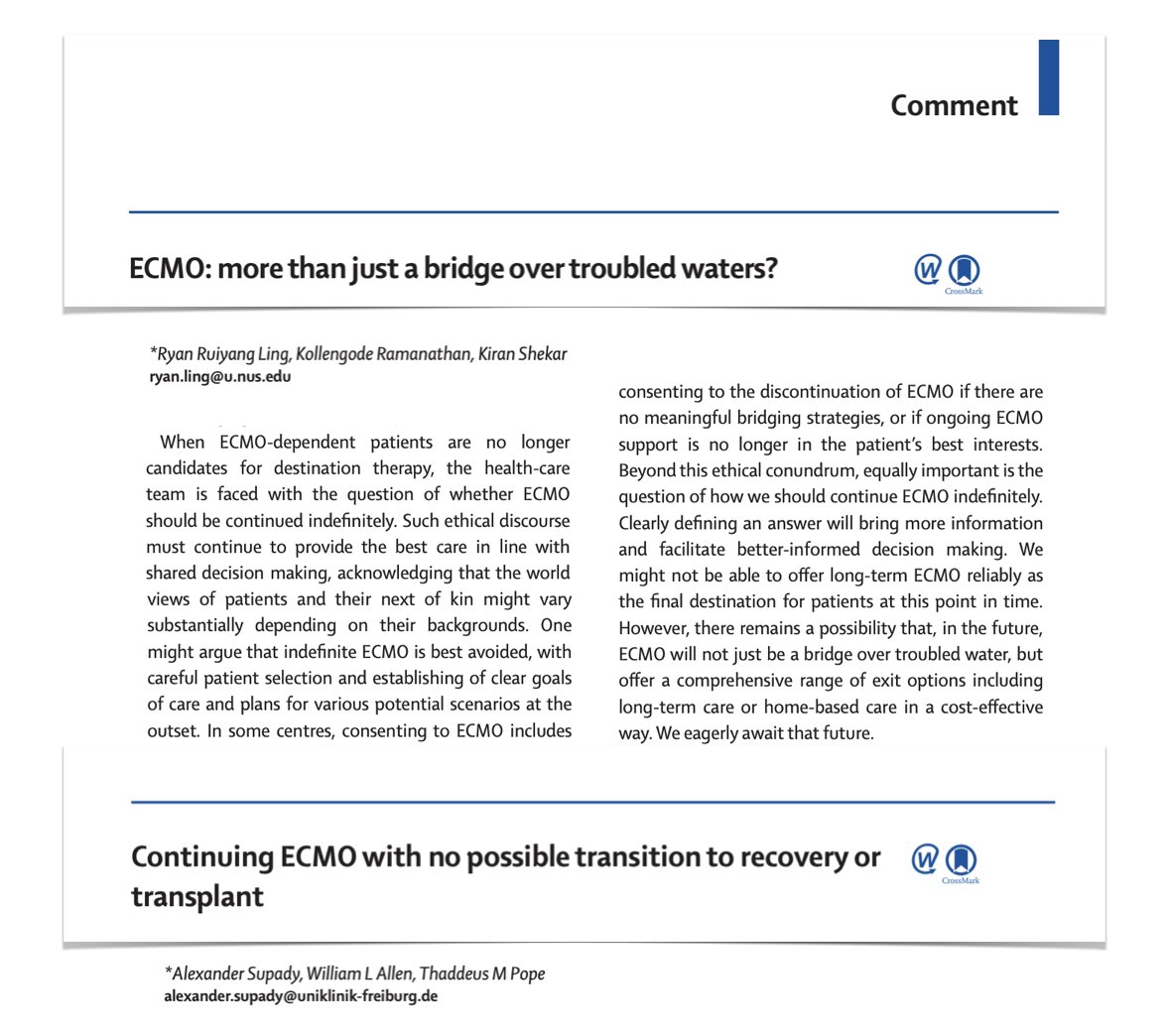
I believe that #ECMO is a life-saving temporising intervention. Yet, there are ethical dilemmas when it appears "futile".
In @LancetRespirMed, @kshekar01 @KrKrramanathan and I envision a future where ECMO can be reliably used as a long-term device.
thelancet.com/journals/lanre…
3
10
947
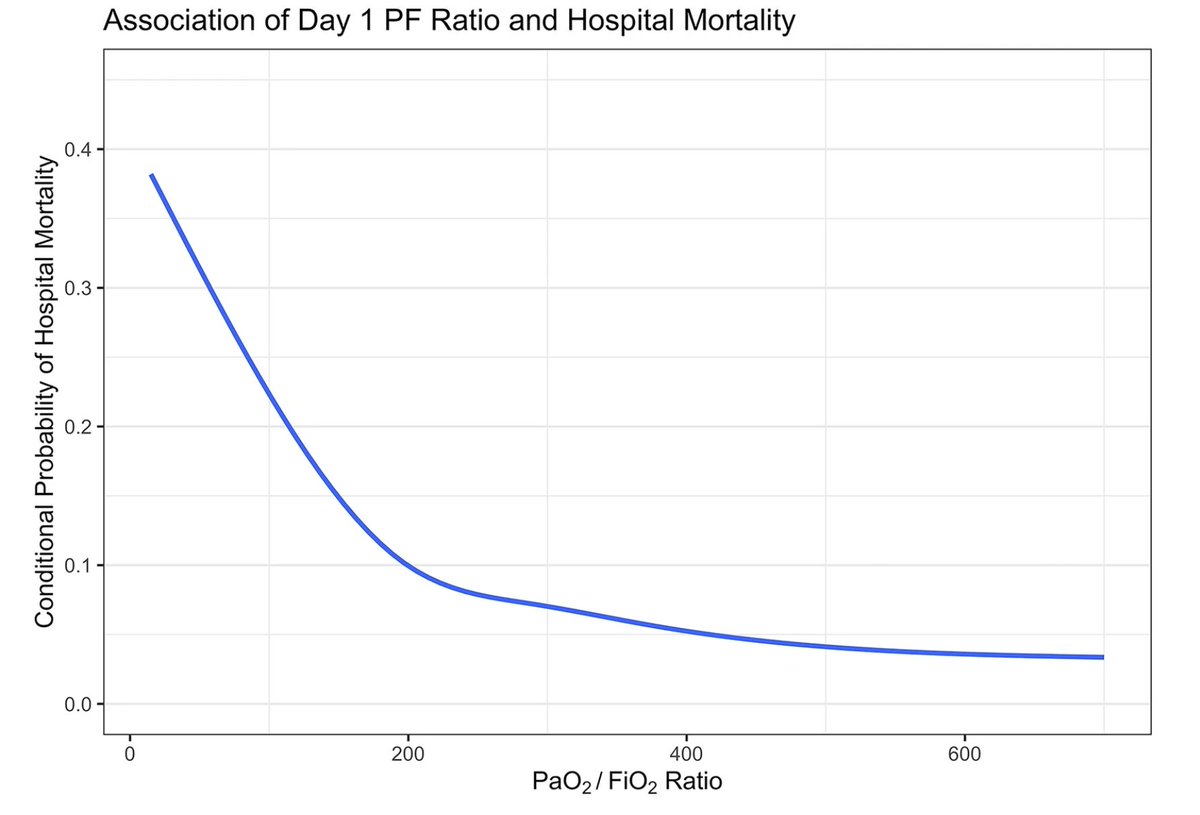
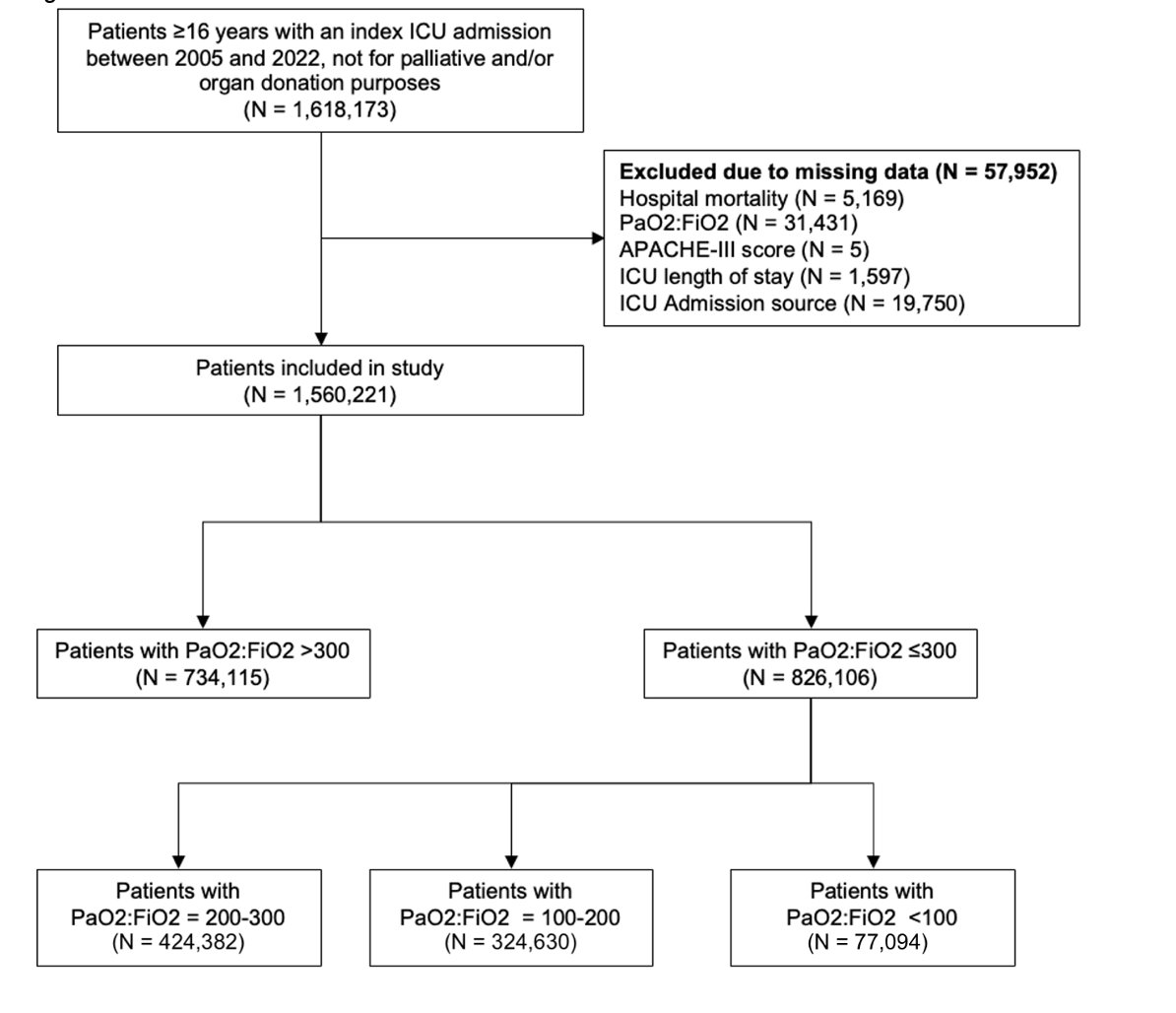
3 Sep 2024
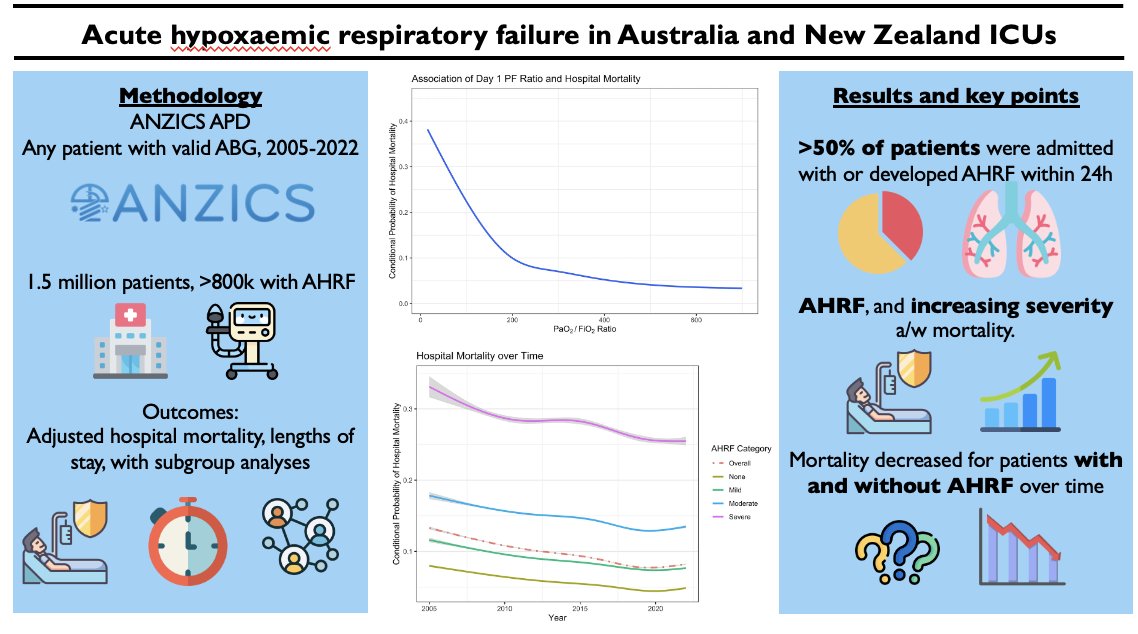
🧐 What is the burden of AHRF in ICUs?
🫂 ANZICS APD 2005-2024: 1.5m patients with ABGs
🫁 >50% had AHRF within 24h of ICU admission!
🪦 Mortality ⬆️with worsening P/F ratios, esp <200.
⏲️ Mortality ⬇️ with time, but not unique to AHRF alone...
🔓 bit.ly/3Xrdh8E
#FOAMed

1
6
10
804
3 Sep 2024
3
105