
Immunologist. Author of the blog and book FEAR OF A MICROBIAL PLANET amazon.com/dp/1630695831/…
Joined June 2009
- Tweets 4,490
- Following 707
- Followers 5,218
- Likes 22,128
69 Photos and videos










Pinned Tweet

13 Apr 2023
Do you have friends that just can't quite quit the pandemic? Do you have family members that believe food dropped on the floor for more than five seconds will kill them? Do you think the experts have always been right throughout history? If yes, my book is for them. And you. Just published by @brownstone.
amazon.com/dp/1630695831/ref…
29
62
267
76,951
Steve Templeton retweeted

Jun 6
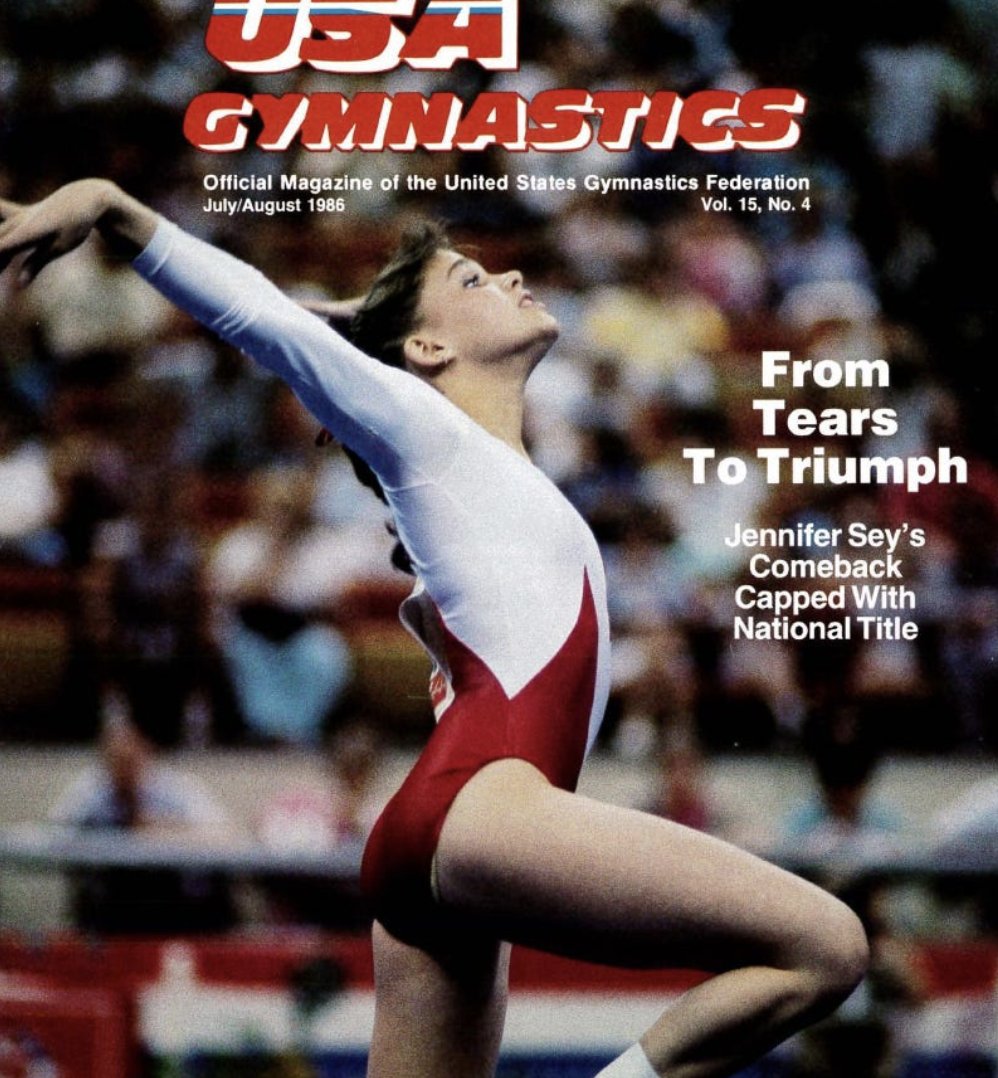
In 1985 I made the USA World Championships Gymnastics Team. I placed 3rd at the Trials, my highest placement to date as a young gymnast.
At Worlds, on my 8th and final event I fell. It was a devastating fall. I missed a release move and tumbled to the ground. My right foot was stuck while my body spun around the knee. I knew it was bad. I screamed, or thought I did. No one came. It felt like forever on the raised platform, no coach, no trainer, no doctor while I writhed.
Eventually my coach realized I wasn't getting back up. They rushed to me. The trainer thought my knee was dislocated and he attempted to push it back in place. It wasn't dislocated though. My femur was broken - we didn't know that yet - and he was pushing bone against bone.
My dad joined me in the ambulance. I remember sobbing -- "What am I going to do now? I don't know how to do anything else. This is all I want to do."
He cried too. We assumed my career was over. He said: "You can do anything you want to do. You're smart and you can be anything you want to be. You're just getting started." He was right in so many ways.
But all I wanted then was to be a gymnast.
I was taken to the nearest hospital and rushed into surgery. It was a French speaking hospital and we didn't fully understand what anyone was telling us.
When I came out of surgery a doctor who spoke English told us "It was a broken femur. Not her knee." We cheered. We were all so happy. My coaches, my parents, me. Bones often heal better than joints.
I left Canada on crutches with a full leg cast. When I got home to Pennsylvania, my doctor changed the cast to a lighter one, with a hinge at the knee. And I went back to the gym. I started training right away.
8 months later, in June 1986, I walked into the arena in Indianapolis for USA Championships. No one thought I'd be there. Everyone thought I was done. Forever.
I knew I wasn't done. Not yet.
I won. I became the National Champion less than a year after breaking my femur on the world's stage.
Never give up. Never.

266
1,163
11,779
355,156
Steve Templeton retweeted

In the normal, sane world of my childhood, this wouldn’t have been extraordinary. But this was November, 2022, and the world was just beginning to recover from the insanity of the Covid-19 response.
~@stemplet74
Education Shrinkflation
brownstone.org/articles/educ…
3
5
12
1,004
Steve Templeton retweeted

May 22
I don’t know what was behind Makary’s resignation, but if I can piggyback on this essay, when I found out I had cancer, my coworker @GeorgiaMaeHowe urged me to reach out to Marty Makary to see if he might offer some advice.
We had interviewed him on Morning Wire, so I had his contact information. But I thought, my goodness, the man has just taken over the FDA! I can’t imagine how busy he is—I can’t bother him with my garden variety cancer diagnosis!
But, I also had some decisions to make. And it can be hard to know what treatment path to choose as an ordinary person with no medical expertise. So I bit the bullet and called him, a little nervous that he might find me presumptuous.
Not only did he give no hint that it was an imposition that I called him, he stayed on the phone with me for about 45 minutes, walking me through all the variables. Then he asked me who I was considering for my surgical oncologist. I mentioned a couple of names and he said, “Let me look into them and get back to you.”
This was far more than I was expecting from someone in his position with the kinds of demands he has on his time. But he called back a few days later and had vetted my surgical options and highly recommended one in particular. He had made calls to other oncologists he knew in Charlotte to ensure that it wasn’t just someone well trained surgically who looked good on paper, but also someone who had a great reputation for being ethical.
(and let me just say, I took Makary’s advice on which surgeon to choose, and it turned out to be a massive blessing because that guy wasn’t only an amazing physician, he also turned out to be a strong Christian, who goes to Kevin DeYoung’s church, so he was really encouraging spiritually through the process as well!)
Then Makary encouraged me to call him anytime if I needed further advice. Which I did, and on those occasions, he once again stayed on the phone with me for a long time, providing counsel and walking me through my options.
So all that to say, I’ve personally experienced Marty Makary’s character and I have to agree with this assessment. He’s a good man.
May 22

Marty Makary used to ambush a Virginia courthouse every other Friday.
That was the day the local tax-exempt hospital reserved the docket to sue its poorest patients.
Marty would show up at the door with a lawyer and intercept them on the way in.
They were working-class people in job uniforms, embarrassed, grim-faced, expecting to lose.
He reviewed the bills on the spot, for free, as a medical expert. Pointing out fraud, upcoding, inappropriate care, contradictions to the court.
Then his counterpart, a young lawyer named Joey Kirchgessner, argued until the hospital cried uncle.
They won A LOT.
I drove down one Friday to watch. I was working in the Trump White House at the time. I was so proud of him I could barely stand it.
That's the man the WSJ op-ed page wants you to believe is the problem.
Read or listen to the full story here: katytalento.com/p/the-most-d…

72
433
3,227
351,255
Steve Templeton retweeted

May 22
Marty Makary used to ambush a Virginia courthouse every other Friday.
That was the day the local tax-exempt hospital reserved the docket to sue its poorest patients.
Marty would show up at the door with a lawyer and intercept them on the way in.
They were working-class people in job uniforms, embarrassed, grim-faced, expecting to lose.
He reviewed the bills on the spot, for free, as a medical expert. Pointing out fraud, upcoding, inappropriate care, contradictions to the court.
Then his counterpart, a young lawyer named Joey Kirchgessner, argued until the hospital cried uncle.
They won A LOT.
I drove down one Friday to watch. I was working in the Trump White House at the time. I was so proud of him I could barely stand it.
That's the man the WSJ op-ed page wants you to believe is the problem.
Read or listen to the full story here: katytalento.com/p/the-most-d…
142
2,627
9,782
711,441
Steve Templeton retweeted

May 12
When I was with MSU football, we traveled to Iowa for a game.
At one point, I got separated from the group, (long story) but I found myself walking toward the stadium in my Spartan jersey. I was walking through a massive group of Iowa fans tailgating.
I’d been to Ohio State already, so I was mentally ready for all the horrible stuff I was about to experience.
Before I had got 100 feet in, people had given me pork chop sandwiches, chips, all kinds of stuff.
I ended up chatting with a bunch of them and they were just the best fan base ever. They loved Iowa football and were just so dang pleasant.
Eventually, I got back to the stadium and a couple hours later the game started.
I was curious as to what these sweet people would be like once the missile launched.
When you’re on the sideline in Iowa, you are right next to the fans. The distance between you and them is very small.
I’ll tell you what, They hurled some of the best and most creative verbal abuse I’ve ever heard in my life.
Absolutely first rate.
They will always be my favorite fan base in the Big Ten.

160
299
7,448
769,905
Steve Templeton retweeted

May 12
Never again is now.
Never forget lies & propaganda they pushed to manufacture fear & hysteria.
Never forget horrific & irreparable harms they imposed
Never forget their evasion of transparency & accountability.
Never forget their crimes against humanity.
Never again is now.
24
344
1,087
12,557

Steve Templeton retweeted

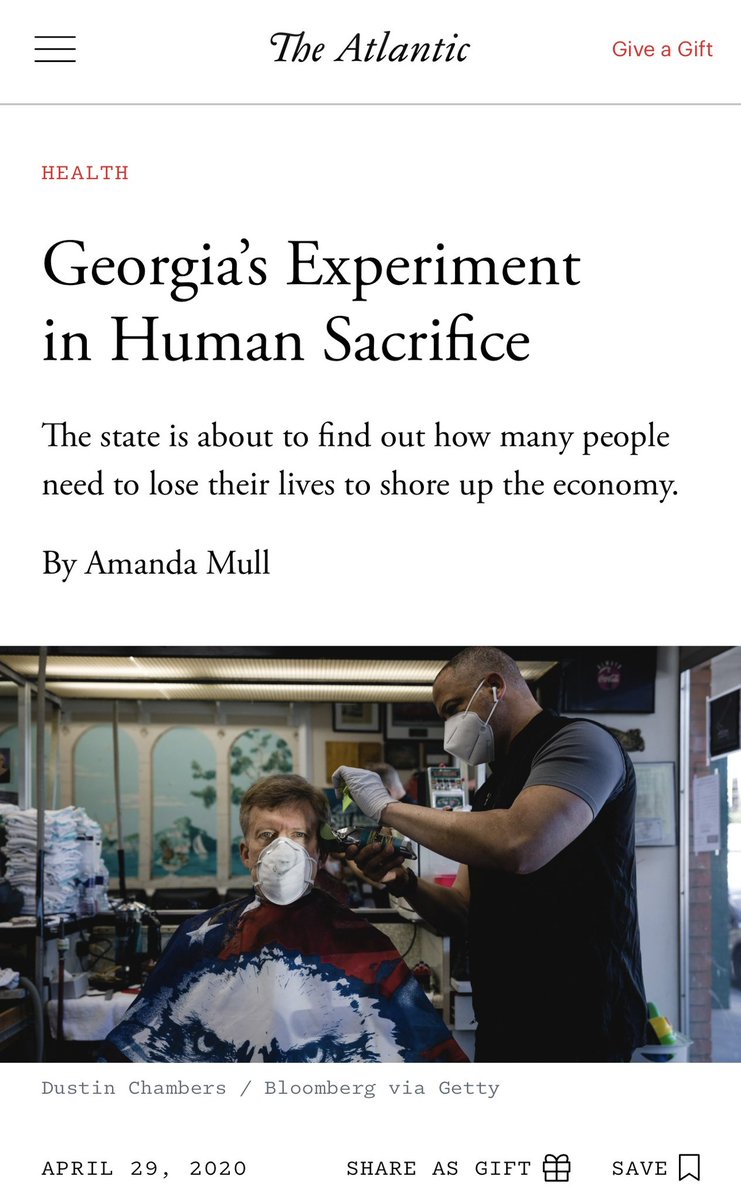
Apr 29
It's worse than just the headline.
A brief analysis from my book "An Abundance of Caution":
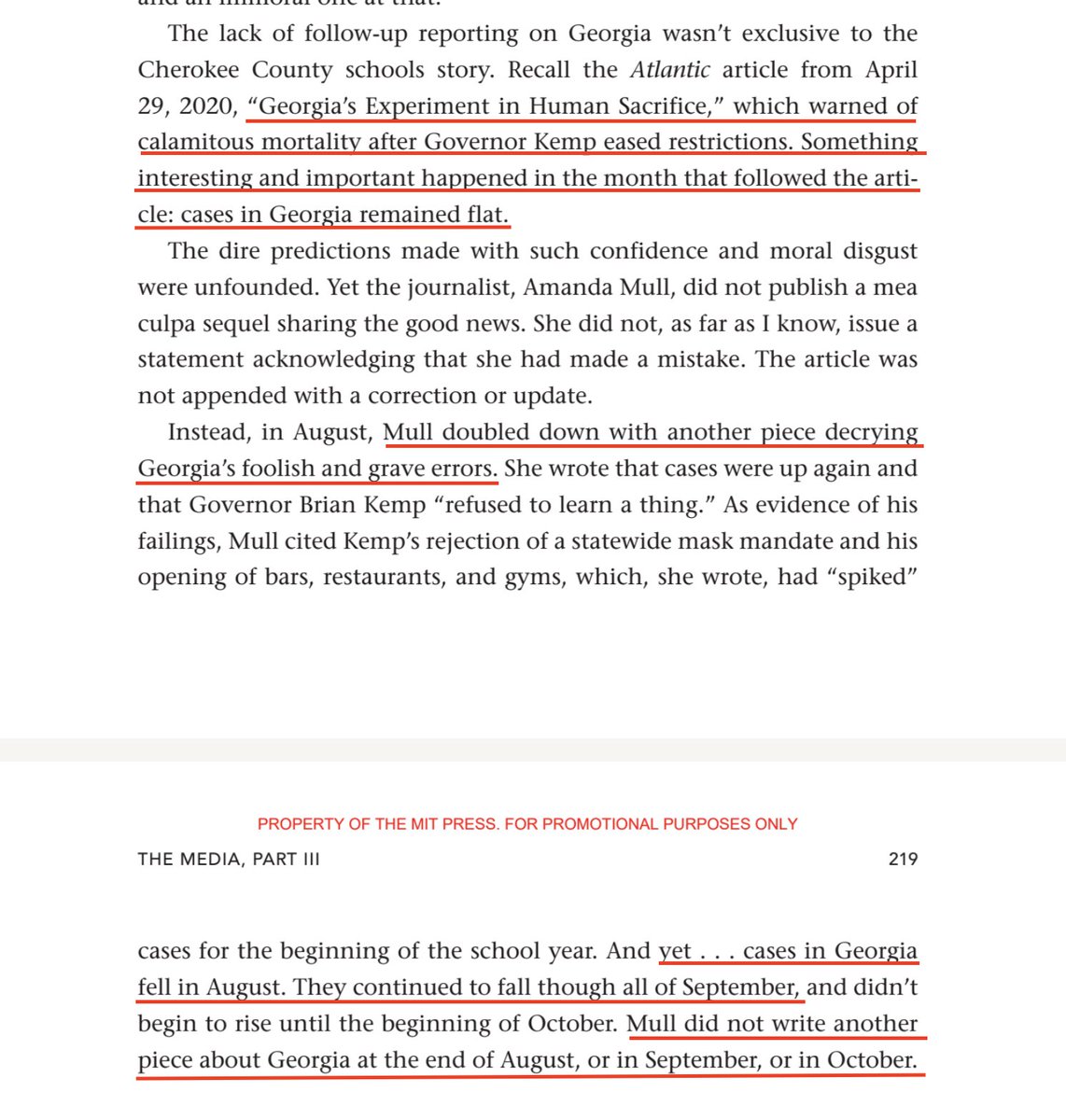
Apr 29

Six years ago today, the most egregious headline of Covid was published.
7
83
370
50,182
Steve Templeton retweeted

Apr 28
One year into cell phone bans, Dallas schools see 24% increase in library book checkouts.
👏👏👏
"Public school districts in Texas are almost one school year into the first statewide cellphone ban, and a North Texas school district is seeing positive impacts.
Dallas ISD officials said that, district-wide, they have seen a significant increase in library book checkouts, which they largely attribute to students no longer having cellphones with them during the school day.
"I started hearing, 'Oh, I'm so bored. I can't get on my phone after I do my work or during lunchtime,'" Hillcrest High School librarian Nina Canales said. "Once they lock into these stories, they don't seem to care about their phones at all."
From the first day of school to March 31, 2026, the district reported an increase of more than 200,000 additional books checked out compared to the previous year.
A look at the library checkouts for the previous year:
2025-2026 Total Circulation (1st day of school to March 31, 2026) – 1,084,837
2024-2025 Total circulation (1st day of school to March 31, 2025) – 872,430
Total library book checkout increase: 24.35%
At Dallas ISD's Hillcrest High, students are following this trend.
Canales said there were roughly 500 books checked out in the first nine weeks of the 2024-2025 school year. This school year, that number spiked to about 1,800 books.
"That floored me," Canales said. "I had to re-do the report again because I was like, 'What, are you kidding me?'"
Students felt the impact too.
"Now that I'm busy with a bunch of work and college, I don't find myself missing my phone that much, even at home," said Yamilet Jimenez, 9th grader."
By @laceybeasnews.
@JonHaidt @safe_screens
61
681
3,184
1,246,071
Steve Templeton retweeted

Apr 23
I see people say "why is there so much resistance to doing vaccinated vs. unvaccinated studies?" like the Henry Ford "Inconvenient" study.
The reasons "any vs. no vaccine" studies are problematic have nothing to do with any "resistance" — they reflect genuine methodological limitations. The completely unvaccinated cohort is typically small and differs from the vaccinated population in so many systematic ways that isolating causal vaccine effects becomes nearly impossible. That's why most researchers focus on more tractable questions: specific vaccines, different schedules, timing of events relative to vaccination, and dose-response relationships. It is not "resistance", it is an attempt to do good science.
There's a contingent that treats long-term saline placebo-controlled RCTs (possibly of all vs. no vaccines) as the only legitimate study design for assessing vaccine safety, and assumes the reason they aren't done is that researchers fear what they'd find. But this ignores the practical reality: no one advancing that argument has ever proposed a workable design, and if they tried, they'd quickly discover why it's infeasible. Even if such a trial were somehow conducted, it couldn't detect rare events, and its findings would still be constrained by whatever schedule was used in the active arm.
The same people advocate for "any vs. no vaccine" observational designs as the gold standard retrospective alternative — again implying the only barrier is fear of results. But well-known biases and confounders make these designs deeply problematic, and the versions typically promoted fail to adjust for them, dramatically overclaim the strength of their conclusions, and refuse to acknowledge fundamental limitations.
Most tellingly, this group dismisses the entire existing safety literature because it doesn't meet their preferred design criteria — effectively pretending no safety data exists. In doing so, they ignore the largest and most rigorous studies available, which happen not to support their conclusions.
29
48
167
10,154
Steve Templeton retweeted

Apr 9
Narrator: it wasn’t the pandemic.
@Rstorechildhood @AppletoZucchini
3
5
31
972
Steve Templeton retweeted

Apr 9
Goooooo, KANSAS!
Sunflower State becomes 13th to pass Reasonable Childhood Independence law!
It is NOT NEGLECT to take your eyes off your kids! Thank you, Gov. Kelly and Sen. Chase Blasi!
#LetGrow!
6
24
1,862

Steve Templeton retweeted

Mar 28
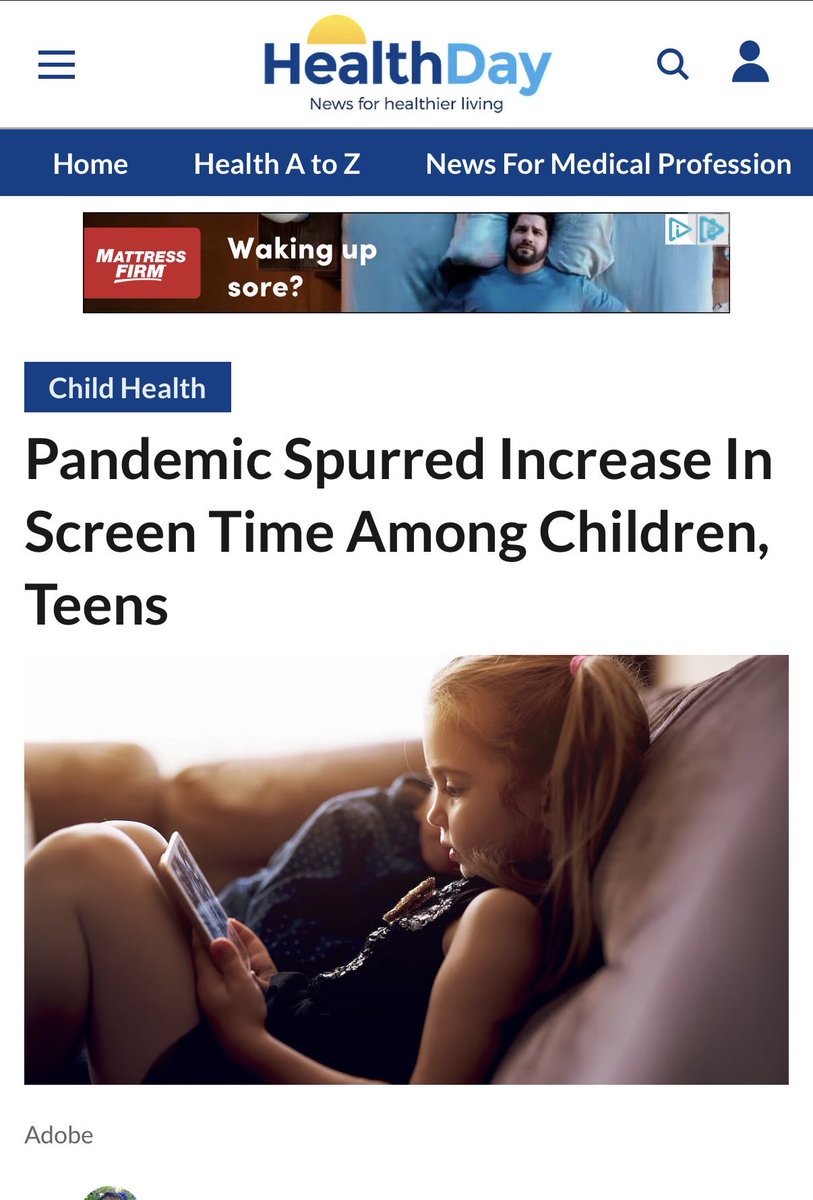
Jonathan Haidt dropped a pretty blunt warning about giving young kids iPads or phones.
He says we’ve all discovered how incredibly effective they are as pacifiers — they work almost instantly. But that’s exactly the problem.
40% of American two-year-olds already have their own iPad. Once a child gets used to constant stimulation, they basically never learn how to be bored. The moment they have even 30 seconds of downtime, they start screaming for the device.
Haidt’s advice is straightforward: If you haven’t started, don’t. If you already have, take it away. It might take 3–4 weeks for the brain to readjust, but it’s worth it.
He’s even hearing stories of preschoolers crying at drop-off — not because mom is leaving, but because the iPad is staying in the car.
It’s a sobering reminder of how quickly these devices rewire young brains and create real addiction patterns.
Have you noticed this with kids in your life, or are you trying to hold the line on screens with little ones?
76
666
2,564
276,478
Steve Templeton retweeted

Mar 29
If you're the mother who was reading Harry Potter and the Philosopher's Stone aloud to your child on the LNER train from London to Edinburgh yesterday, one of my grown up children was listening and says you did the voices brilliantly❤️🥹
3,001
14,478
314,959
6,154,246
Steve Templeton retweeted

Mar 28
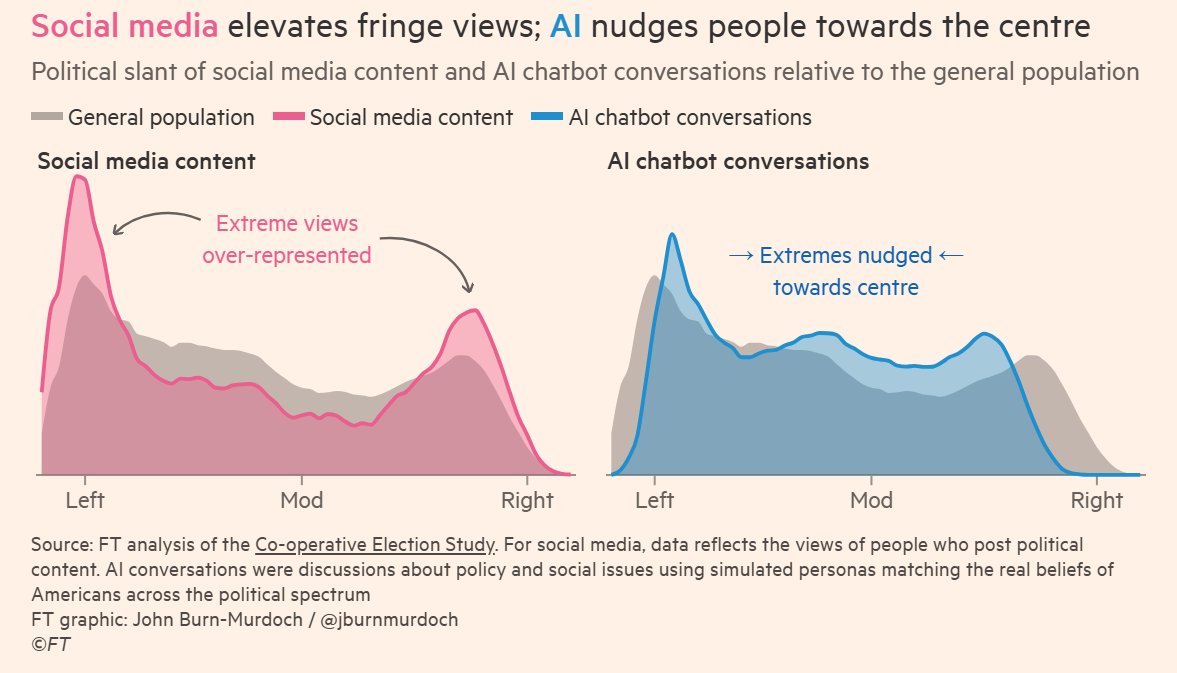
While social media is polarising, evidence suggests AI may nudge people towards the centre.
This holds true of all studied models. Grok is more right-leaning than other models, but also has depolarising effects.
By @jburnmurdoch.
234
1,022
6,143
1,227,600
Steve Templeton retweeted

Mar 20
This is sad. I know as a politician these companies are going to spend a billion dollars against me for saying it but 🤷🏽♀️
Pervasive gambling is not good for society. It turns life into a casino, traps people in addiction & debt, surges domestic violence, and fosters manipulation.
Mar 19

We’re honored to announce MLB has named Polymarket as their Exclusive Prediction Market Exchange Partner.
Polymarket 🤝 MLB
8,760
11,095
115,411
10,718,144
Steve Templeton retweeted

This is the funniest thing I’ve seen on the internet.
Afroman had his house raided by Ohio Adam County deputies… who found absolutely nothing… broke his door, trashed his place, allegedly had $400 go missing… and then they refused to pay for the damages.
So, like any reasonable rapper would do…
He turned his home security footage into music videos, mocking them.
And then, the deputies sued him for FOUR MILLION dollars… because they didn’t like being made fun of.
And Afroman’s response?
He dropped ANOTHER music video.
In his own words:
“Unconfidential informant lied to Police to get out of some trouble. Adam County Sherriff officers made a mistake by believing the lie. Raided my house, found nothing, refused to pay for the damages and filed a lawsuit against me, Afroman, for exercising my freedom of speech! This is me holding trial in one song. I hope you enjoy it.”
They said his videos “ridiculed” them… so he decided to show them what that actually looks like.
And the best part?
A jury basically said… yeah… you don’t get to raid someone’s home, end up in their surveillance footage, and then cry because they used it to make fun of you.
836
14,768
92,044
4,738,139
Steve Templeton retweeted

Mar 20
Normalizing remote school was a mistake.
Mar 19

Pittsburgh Public Schools will be closed for three days, and compel "asynchronous" remote learning, because of the NFL Draft.
Since the city will have a lot of visitors this will "ensure students can continue learning safely and effectively."
Unreal.
publicsource.org/pittsburgh-…
17
30
546
27,410