
Joined June 2011
- Tweets 36,339
- Following 891
- Followers 10,353
- Likes 76,814
1,795 Photos and videos




Pinned Tweet

1 May 2025
1) OMG we did it‼️‼️
In this film for #MEawarenessmonth, five medical doctors open up about living with #PAIS/#IACC conditions like ME, #longCOVID, and chronic #Lyme. It’s a format that I believe has never been shown before, not just in the Netherlands
youtu.be/J0ywwLIfH_w?si=FGIv…
61
491
1,073
160,123
Anil van der Zee © retweeted

Jun 13
"Een mens mag dromen". Alsof rechtop zijn een bijna brutale wens is. Een tekening van Barbara Jansma
tinyurl.com/3jr4kcub
#pwME #MyalgicE #art

1
3
4
137
Anil van der Zee © retweeted

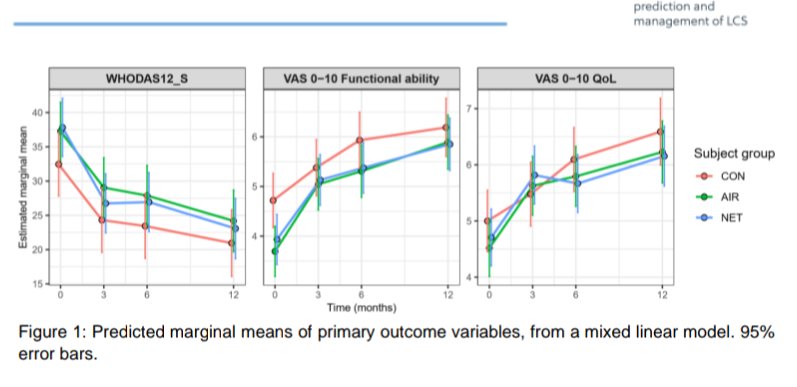
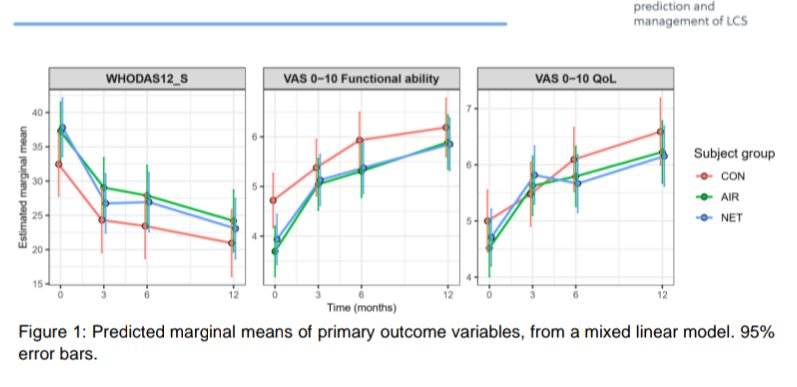
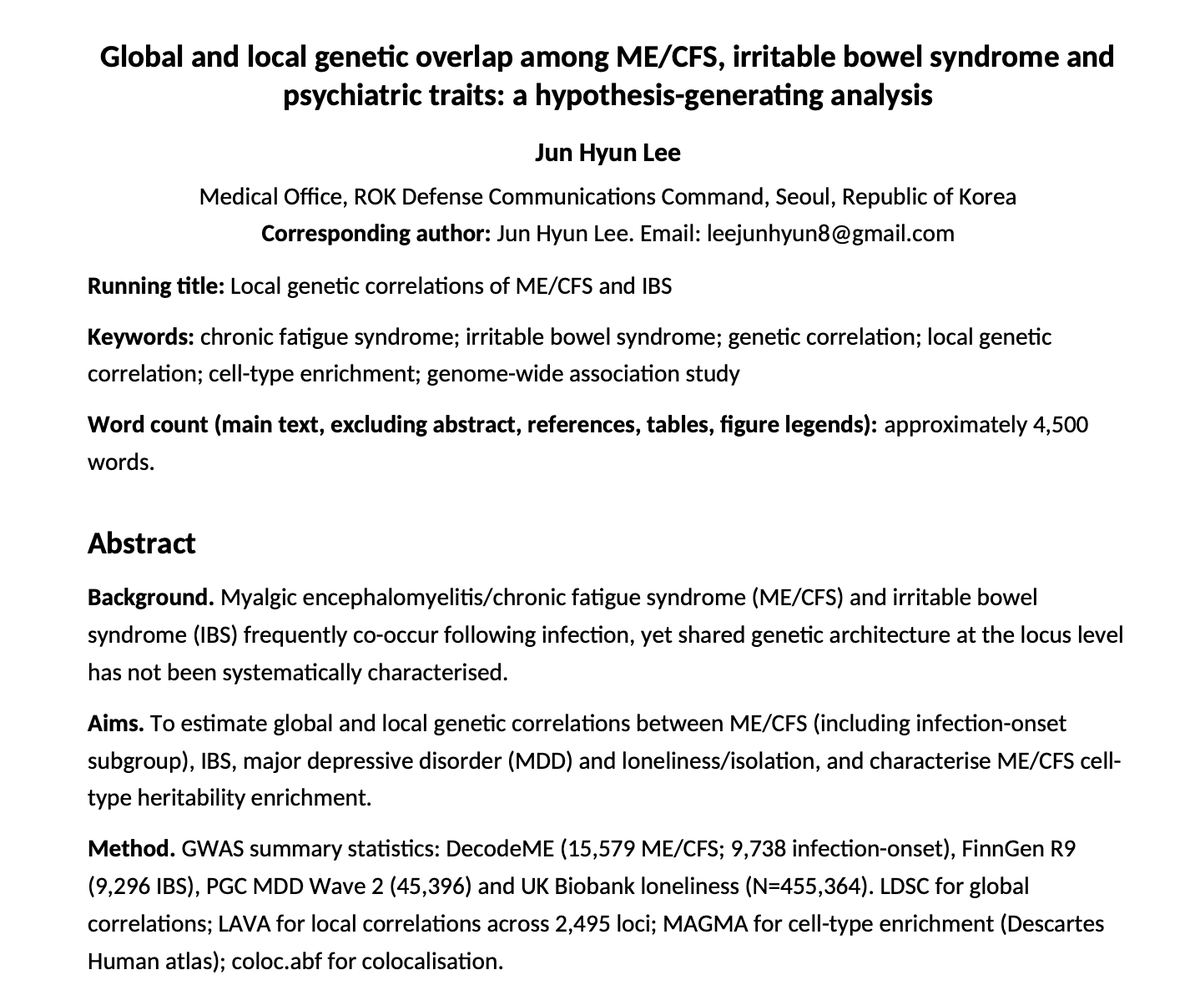
1) 🇰🇷 There's another preprint by a single author (Junhyun Lee) analysing the DecodeME genetic dataset.
It found substantial genetic correlations with Irritable bowel syndrome and depression, and a link with inhibitory neurons from the Descartes Human single-cell atlas.
1
13
35
1,837
Anil van der Zee © retweeted

Jun 12
C-support nieuwsbrief: reclame voor "de stilte schreeuwt", kom lekker kijken naar de (Long) Covid ontkenningsfilm en dat verdienmodel ondersteunen.
Ik onderstreep het belang van het erkennen en mainstreamen van chronische ziekte door vaccinatie. Hiermee doet C support her tegenovergestelde: ze duwen het verder in de complothoek.
7
7
24
1,038
Anil van der Zee © retweeted

Jun 12
Nieuwe studie ontwikkelt een nauwkeurig biomarkerpanel voor #MEcvs
Chris Ponting zal concentraties van ongeveer 1100 eiwitten meten in plasmastalen van mensen met ME/cvs en controlegroepen
Bespreking @MEResearchUK
me-gids.net/nieuwsartikel/ni…
3
2
198
English subtitles have been added to the care clinic for people with severe ME and very severe ME in Norway.
youtube.com/watch?v=-KX12ztZ…
1
12
24
1,122
Anil van der Zee © retweeted

Jun 10
Save Caroline Roberts’ Life now: A very severe #ME/CFS patient with high mortality risk. - Sign the Petition! c.org/sQhHQ9BLRb via @UKChange
It’s the same terrible story. Caroline was admitted to hospital last week. The hospital refuses to offer any nutritional support 😡
7
66
97
4,354
Anil van der Zee © retweeted

Jun 11
From Germany 🇩🇪
Impaired microvascular reactivity in post-COVID-19 syndrome is independent of cardiorespiratory fitness
journals.physiology.org/doi/…
#LongCovid #PASC
1/
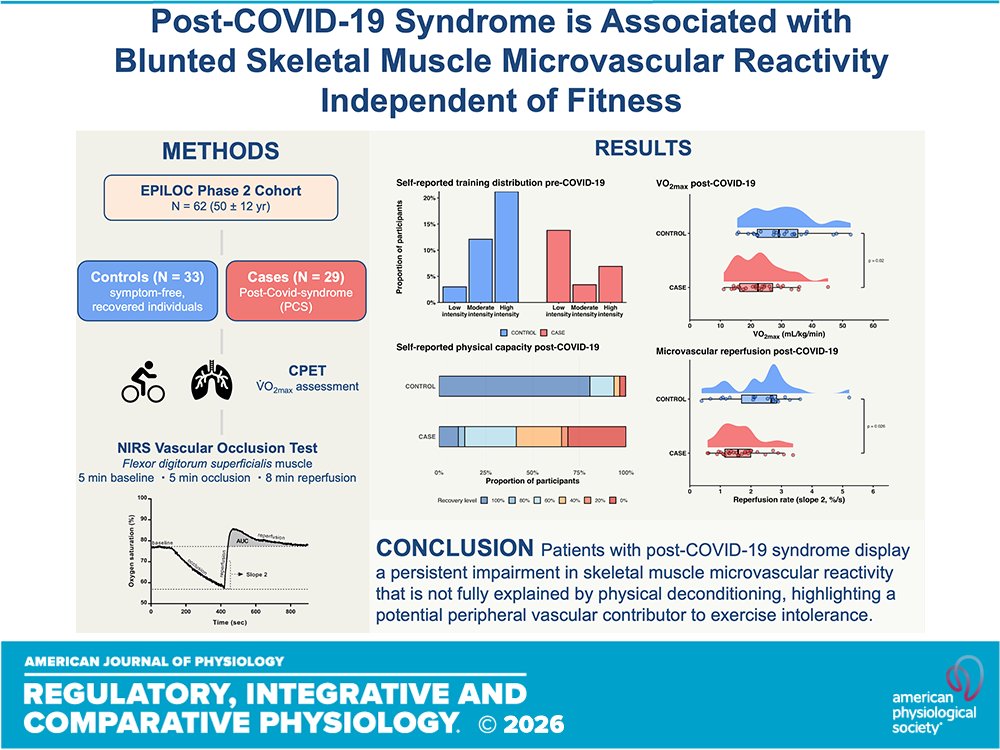
ALT Graphical abstract
1
9
23
3,155
Anil van der Zee © retweeted

Jun 10
@mecfsskeptic, where are the critical notes?
This is the prototypical whitewashing of mind-body and CBT studies.
By flooding them with mostly (stress-related) biomedical tests,
and hiding the old school methodological mistakes essential to keeping these views alive:
Jun 10

1) 🇧🇪 Researchers from Leuven and Hasselt university published a protocol for an extensive ME/CFS study.
It includes cytokine measurements, MRI and PET scans, gut microbiome analysis, and salivary cortisol following a stress test.
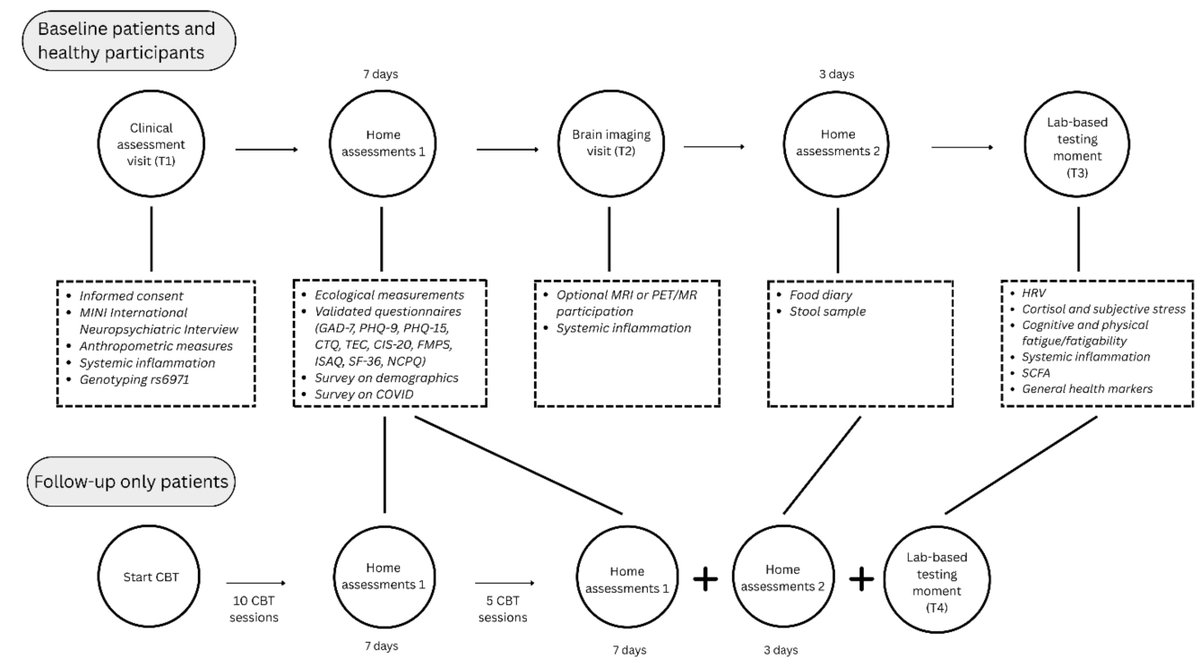
ALT Figure 1. Overview of the cross-sectional and longitudinal parts of the study design
3
5
21
1,635
Anil van der Zee © retweeted

Jun 8
Just sharing again. It’s so good. Thanks Adam youtu.be/RiwX9Y0NbiQ
2
13
39
1,944
Anil van der Zee © retweeted

Jun 9
Here's my first post about that Wired story: virology.ws/2026/06/09/trial…
5
49
146
10,056
Anil van der Zee © retweeted

Jun 10
Congratulations to Gemma Samms, who has now submitted her thesis and is awaiting viva, for PhD level research funded by ME Research UK: meres.uk/samms.
Gemma has also been included in the 300 Faces of Edinburgh Medical School for work in ME/CFS: bit.ly/4vnF9Zr

4
16
87
1,411
Anil van der Zee © retweeted

Jun 4
Thank you to @Invest_In_ME for 20 years of conferences and all the hard work done by volunteers.
Full video
youtu.be/IWr4eCeRYWc?si=Cf07…
Press release
investinme.org/IIMER-PR-2026…
1
18
52
1,674
Anil van der Zee © retweeted
Jun 9
My post about the @WIRED story by @AlanLevinovitz clocked in at 3,000 words--not quite half the length of the story itself. Sorry!!--I tried to keep it shorter, but there was just so much to say. And more likely to come. virology.ws/2026/06/09/trial…
5
45
143
3,492
Anil van der Zee © retweeted
Jun 9
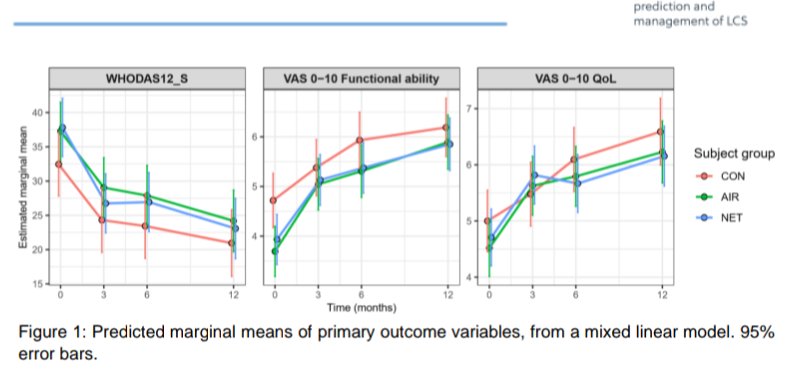
In a 7,600-word piece in @WIRED on unhinged patients having essentially blocked research into mind-body stuff, @AlanLevinovitz failed to mention two major clinical trials. Can someone explain to me how that happened? What will Wired do about it? Is it bias, incompetence, or both?
21
69
325
23,395
Anil van der Zee © retweeted

Zij kunnen niet meer. Het is asociaal dat deze mensen de rekening moeten betalen van het kabinetsbeleid.
D66, VVD en CDA moeten deze plannen
wijzigen. Chronisch zieken, mensen met een beperking en hun familie, verdienen onze steun, geen extra rekening. nos.nl/artikel/2617752-mense…
293
118
445
33,531
. @davidtuller1 about the Wired article @AlanLevinovitz.
*Levinovitz calls for robust research into mind-body interventions. But he fails to mention two major clinical trials that pertain directly to his argument—a perplexing omission."
virology.ws/2026/06/09/trial…
3
11
74
1,931
Anil van der Zee © retweeted

On a voulu interroger Alexander Zverev sur les réserves d'une partie du public et des médias, eu égard aux accusations de violences conjugales de deux anciennes compagnes. Ça s'est très mal passé.
➡️ Zverev : "Je pense qu'on devrait arrêter, c'est mieux"
lequipe.fr/Tennis/Article/Al…
215
718
3,457
639,467
Anil van der Zee © retweeted

Jun 6
⚠️After seeing the response from patients, clinicians and scientists, I think this needs to be said clearly:
Re-promoting an article that has caused so much harm to the Long COVID community is not brave journalism.
It is irresponsible.
This article did not simply “open a difficult conversation.” It amplified a deeply damaging frame: that maybe patients are rejecting the uncomfortable truth that CBT, exercise and “mind-body” approaches are the way forward.
But when you present a complex post-infectious disease through that lens, without properly separating psychological support from biological treatment, you are not helping patients.
You are making their lives harder.
These narratives do not stay inside an article.
They reach families.
They reach employers.
They reach disability assessors.
They reach doctors who already know very little about Long COVID.
They reach people who are looking for an excuse to say: “maybe it is just anxiety,” “maybe you are afraid of exercise,” “maybe you are keeping yourself sick.”
That has consequences.
Social consequences.
Medical consequences.
Workplace consequences.
Psychological consequences.
Patients with Long COVID are already fighting disbelief, lack of biomarkers in routine care, lack of approved treatments, disability, isolation and medical neglect.
Using their suffering to generate clicks while repackaging old psychosomatic narratives in modern “mind-body” language is not courageous.
It is cruel.
The problem is not talking about the nervous system.
The problem is turning nervous system involvement into a story about beliefs, fear, trauma or patients refusing to accept recovery.
The problem is using recovery anecdotes as if they establish causality.
The problem is ignoring those who worsened with exercise.
The problem is presenting PEM caution as dogma.
The problem is being much more generous with “brain retraining” narratives than with the biomedical evidence already showing immune, vascular, autonomic, metabolic and muscular abnormalities in Long COVID.
If a journalist wants to write about Long COVID, they have a responsibility to understand the history of harm done to post-infectious patients.
Because this is not new.
ME/CFS patients have lived this for decades.
“Unexplained” became “psychological.”
“Normal routine tests” became “nothing is wrong.”
“Supportive care” became “cure.”
“Exercise” became “rehabilitation,” even when patients were crashing.
And now the same mistake is being repeated with Long COVID.
Patients are not angry because they reject science.
They are angry because they recognize the pattern.
They have seen what happens when medicine turns biology it cannot yet measure into psychology.
So no, this is not “a way forward.”
A way forward would be stratification, biomarkers, mechanistic trials, antivirals, immunology, dysautonomia research, PEM-safe protocols, autoantibody studies, vascular biology, tissue persistence, metabolism and serious clinical phenotyping.
A way forward would be listening to all patients, including those harmed by exercise and psychologizing narratives.
A way forward would be scientific humility: admitting what we still do not know without turning unexplained biology into psychology.
Not click-driven repetition of the same ideas that have already harmed post-infectious patients for decades.

There might finally be a way forward for long Covid treatment—if only you were allowed to talk about it. wired.com/story/the-painful-…
24
181
653
17,316
Anil van der Zee © retweeted

Wait… people know “brain retraining” programs don’t have ANY sound scientific support, right? All of the studies I’ve seen were so poorly designed I wouldn’t count them as evidence and they were conducted by people making tons of money off of marketing these “treatments” to vulnerable communities (i.e., heavy bias). Is that really what the guy is referencing in that long covid article?? I haven’t had the energy or time to read it
6
28
149
3,096
Anil van der Zee © retweeted

Think you go of by gut feeling and source X when you say “the community thinks & says,..”
……
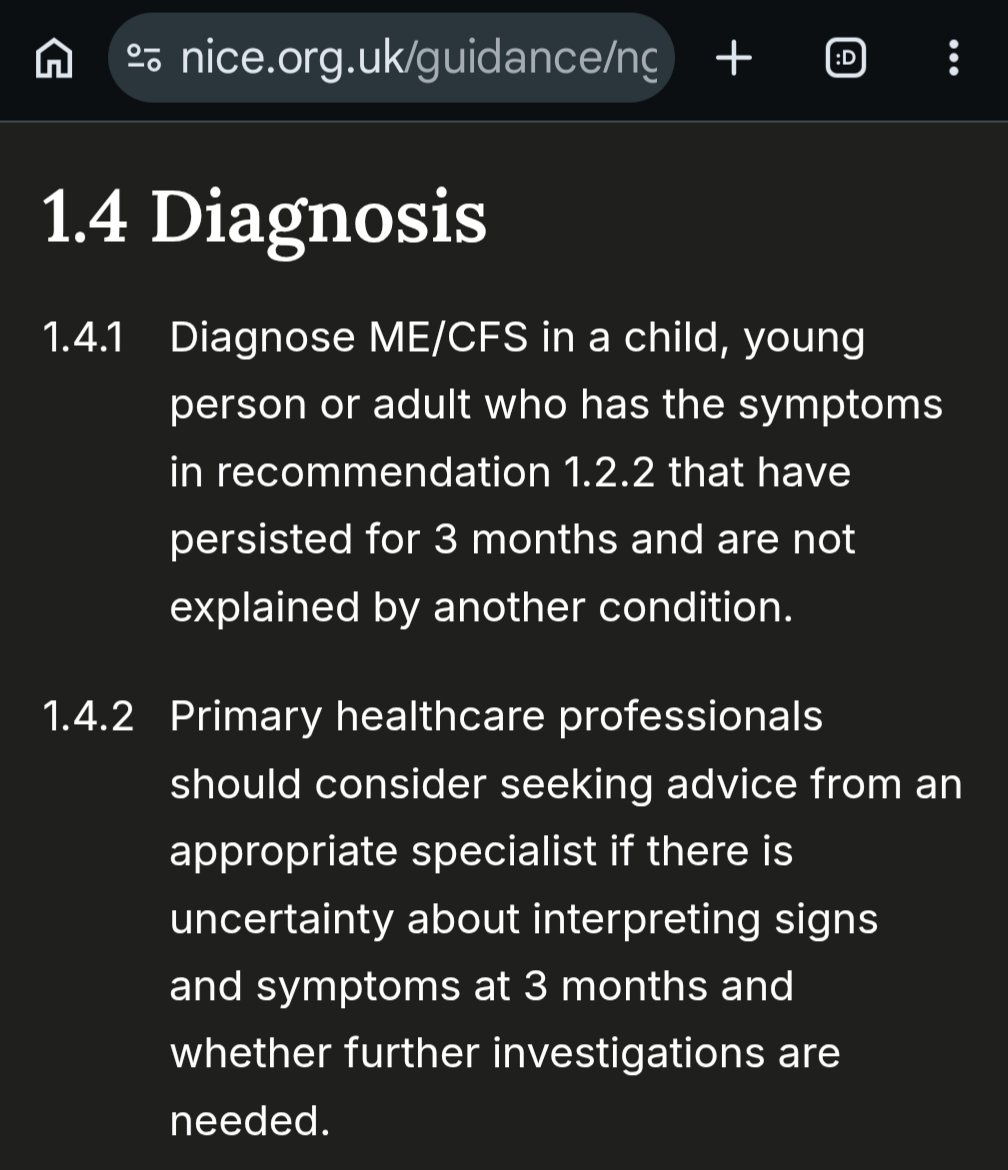
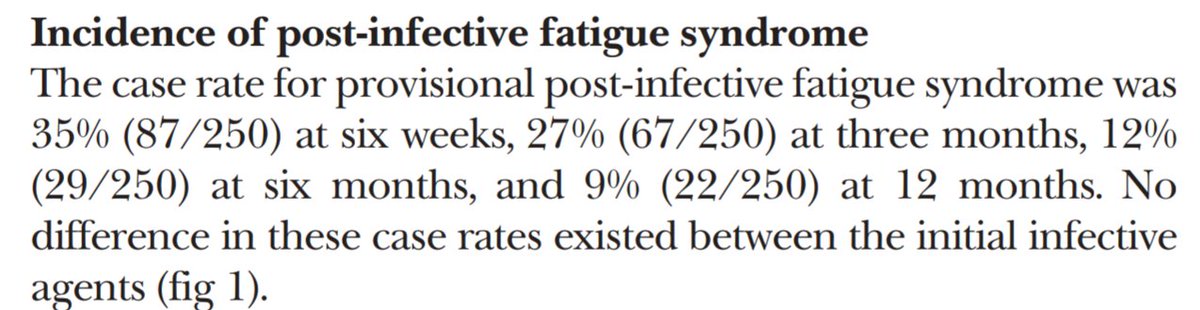
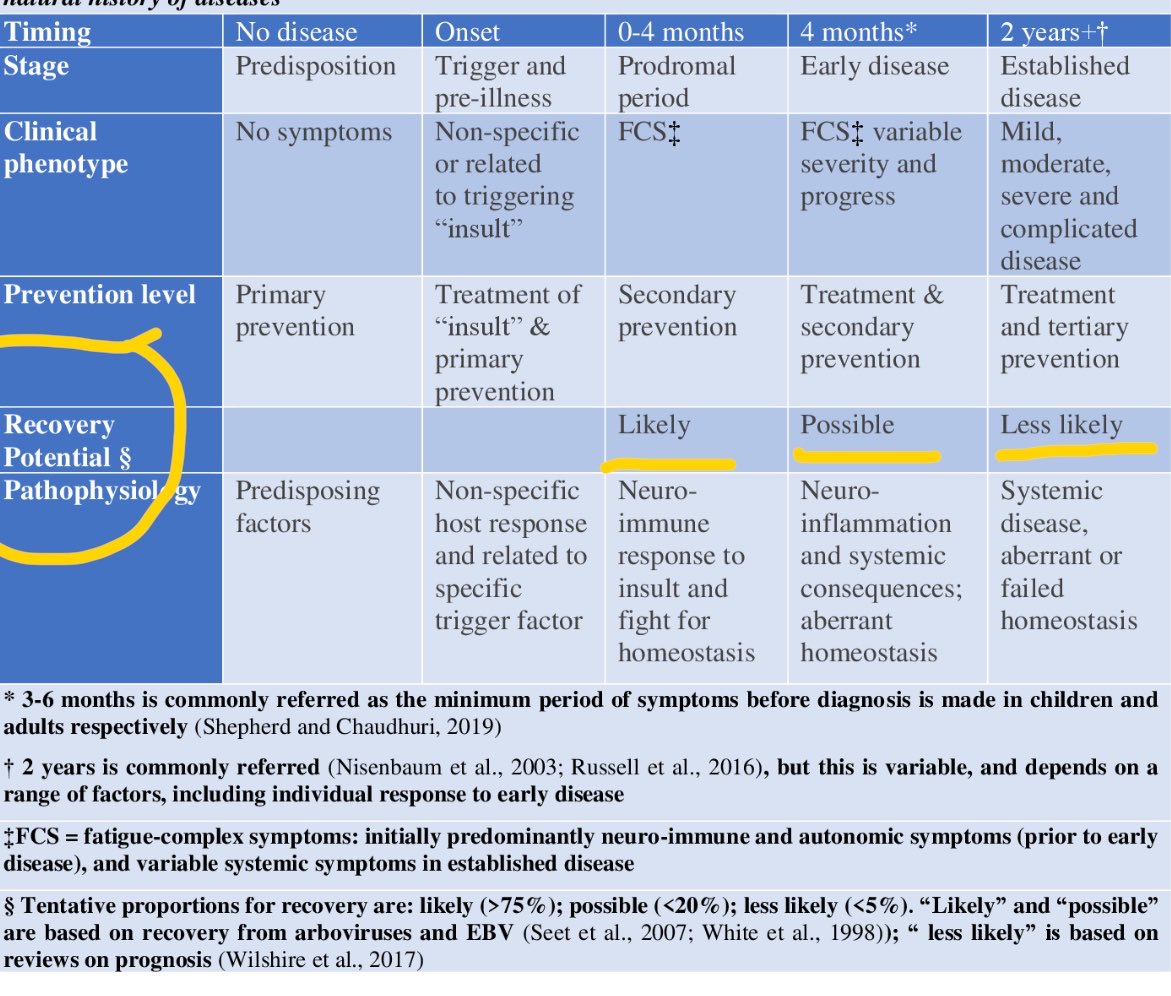
Anyway, veteran ME already knew beforehand that many LC would recover.
Also see study from 2019:
- recovery from PAIS ➜ less likely per month/year
- but recovery still happens !
1
2
14
467