
Joined January 2025
- Tweets 2,765
- Following 735
- Followers 56
- Likes 2,663
32 Photos and videos















CommunityRSC retweeted

Jun 13
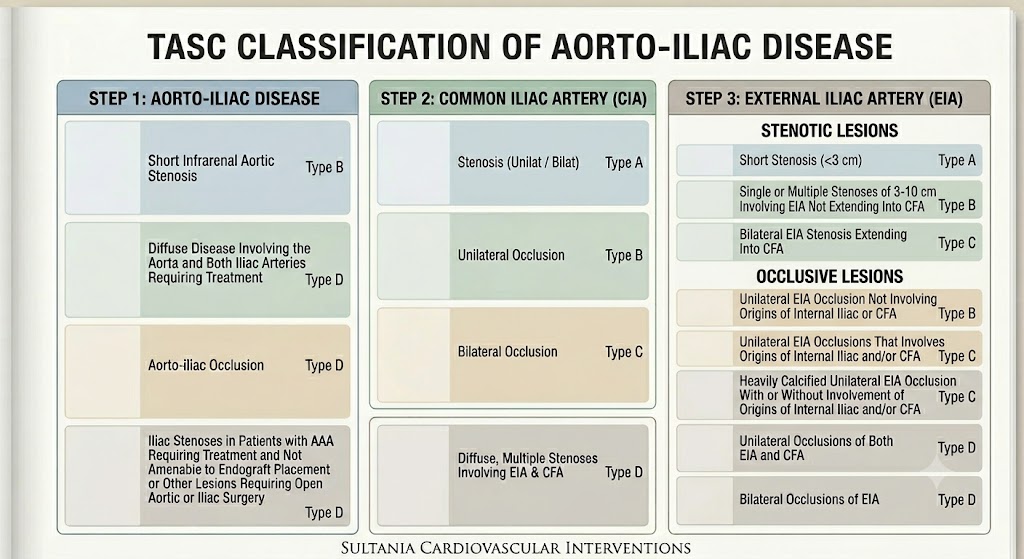
#Vascular interventions
#Peripheral vascular interventions
A way to know TASC class practically .
See segement from Aorta to CIA to EIA ,then use this
@AlkashkariWail
@mirvatalasnag
6
13
716
CommunityRSC retweeted

Jun 13
Systematic Review
Prognostic Role of Left Atrial Reservoir Strain for Risk
Stratification in Aortic Stenosis doi.org/10.3390/jcm15114304 #cardiology #echofirst

4
14
1,024
CommunityRSC retweeted
For those who want to stay ahead, #SEOULVALVES2026 offers a unique opportunity to learn and engage in high-level discussions and connect with leading experts. Register by Friday, July 24, to secure the best available rate before it disappears!
🔗Register: seoul-valves.com/2026/attend…


2
3
57
CommunityRSC retweeted
Jun 12
Review
Categories of Aortic Stenosis: What’s New and the
Clinical Implications doi.org/10.3390/medicina6205… #echofirst #cardiology

13
32
1,904
CommunityRSC retweeted

Jun 12
How To Read A Contrast Microinjection?
Every injection gives valuable info about the CTO. Things to look for
👉🏼 Does contrast persist?
👉🏼 Where does it collect?
👉🏼 Is there reflux?
👉🏼 Are there new side branches?
👉🏼 Is the distal lumen seen?

2
5
23
1,499
CommunityRSC retweeted

Jun 12
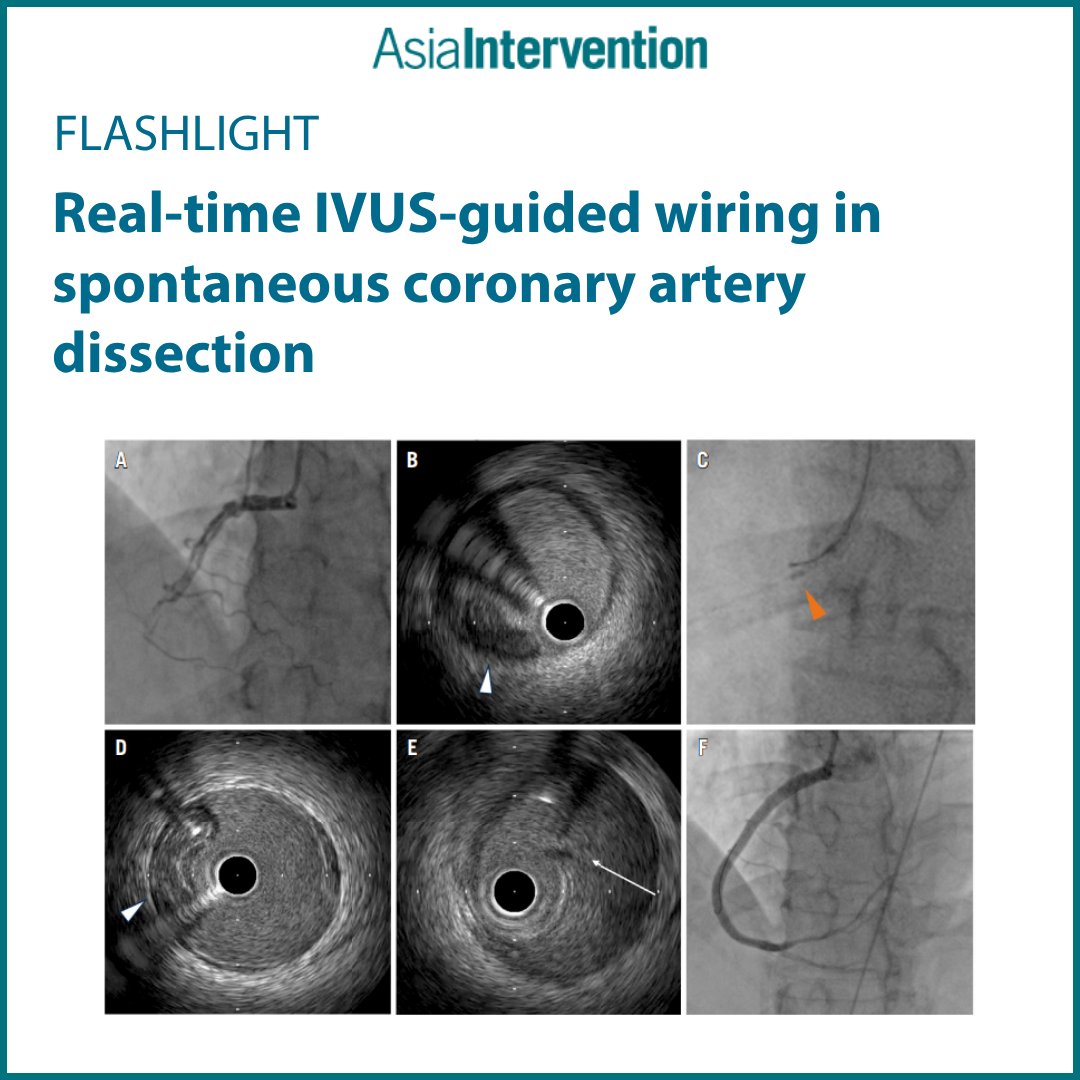
Spontaneous coronary artery dissection remains one of the most delicate scenarios in #PCI 🔬
Real-time IVUS guidance can be decisive in ensuring safe wiring and avoiding complications.
🔗 brnw.ch/21x3hJX
#SCAD #IVUS #ClinicalResearch #InterventionalCardiology #CardioEd
8
16
937
CommunityRSC retweeted

Hybrid revascularization DES &DCB.
Double bifurcation. LAD D1, LMS LAD RI. Both minicrush.
DCB to mid distal LAD
x.com/i/status/2064737003321…

Morbidly obese diabetic young male with NSTE ACS.
Diffusely diseased LAD, D1, and high OM/ RI.
Then, there was cath induced non flow limiting LMS dissection.....
2
10
42
7,057
CommunityRSC retweeted

Jun 10
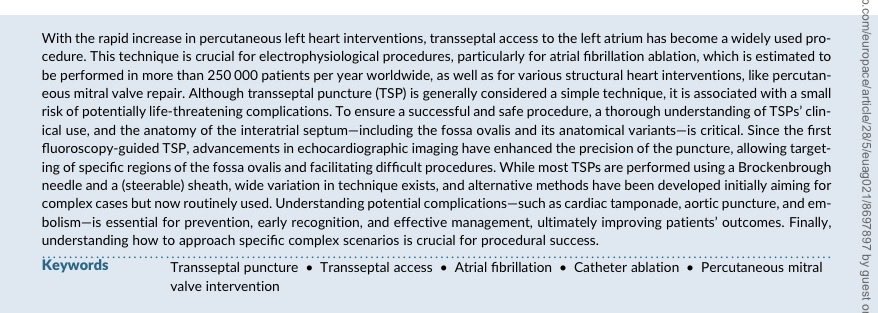
Transeptal puncture in cardiovascular interventions: a clinical consensus statement.
doi.org/10.1093/europace/eua…

1
21
65
2,869
CommunityRSC retweeted

Jun 11
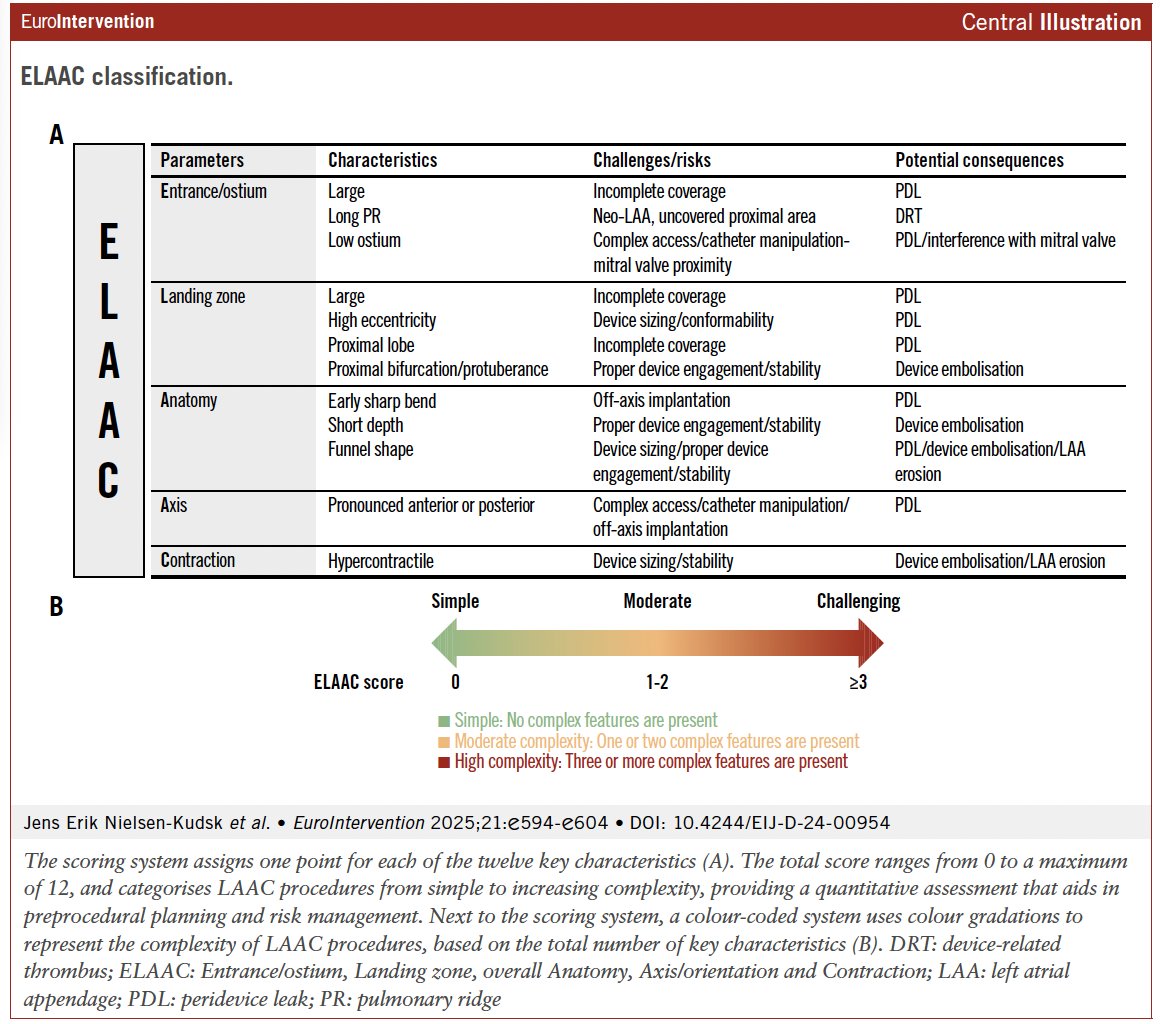
How can we better describe procedural complexity in left atrial appendage closure?
This implanter classification integrated key anatomical and functional features to provide a common language between operators and imagers, helping distinguish standard from complex anatomies and anticipate procedural challenges.
eurointervention.pcronline.c…
#LAAO #StructuralHeart
@Nielsen_Kudsk @freixa_xavier @RaberLorenz @icruzgonzalez @DrGarot
1
8
16
1,301
CommunityRSC retweeted

Jun 11
#IVUS practice #Episode 1
Artery: a big #LCx
Intramural hematoma: moving blood/stagnant blood
#InterventionalCardiology #cardiology #intracoronaryimagine #CardioX #CardioTwitter
@esbrilakis @realarainmd @stefan_harb @sbrugaletta @dautov_MD @jbspadoni @NievesGonzalo1 @Pooh_Velagapudi @evandrofilhobr @ziadalinyc @rotamonster @Laserrman @AlbertoCereda1 @FranceskAlbs @MohammedAlo @Hragy @mmamas1973 @aspergian1 @mirvatalasnag @Abdul_alkindy @TWilsonMD @abadkhan2002 @ogoktekin @ShadiYaghi2 @jedicath @rotamonster @Laserrman @Sh_Zaynobidinov @Obisht @Murmur_MD @GopalKkoduru @DrMarthaGulati @nadig_cardio @iamritu @ANazmiCalik @GoranEBC @shaoliang_chen @KambisMashayek1 @AgostoniPF @DFCapodanno @GreggWStone @brown_rye @SarahFairley7 @LAzzaliniMD @luciotpadilla @PCRonline @nicolasamabile @BSCCardiology
17
88
6,011
CommunityRSC retweeted

Jun 11
📰New #TCTAP2026 articles are now online!
Read more about the latest expert insights on CTO PCI, cardiogenic shock, mechanical circulatory support, and carotid artery disease, all in one place!
Visit our website and catch up on the news updates today.
🔗summitmd.com/html/conference…

3
4
131
CommunityRSC retweeted

Jun 10
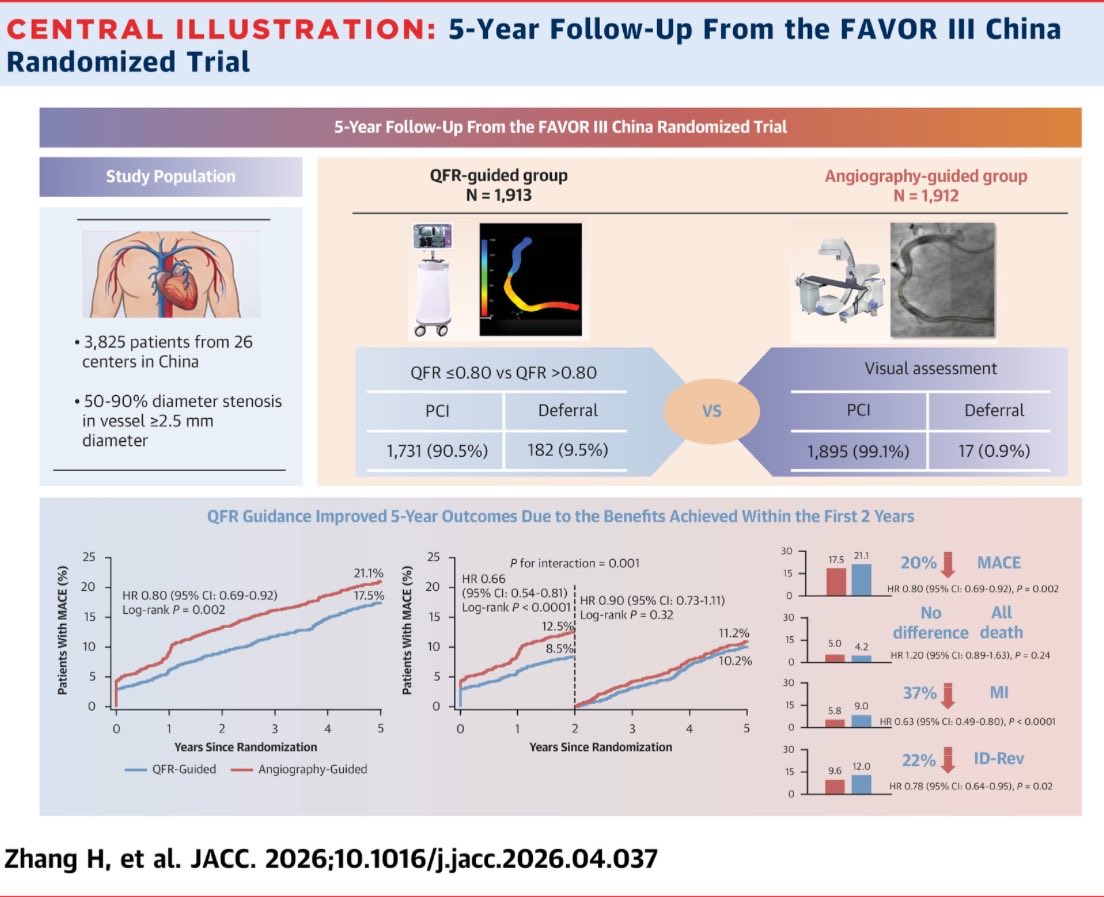
#CoronaryPhysiology
#AngioDerivedPhysiology
FAVOR III China 🇨🇳
PCI guided by
QFR-
vs
ANGIOGRAPHY:
E F F E C T I V E N E S S
& S A F E T Y
at 5 years
👇
jacc.org/doi/10.1016/j.jacc.…
👋
Han Zhang
Ajay Kirtane
Shengxian Tu
@GreggWStone
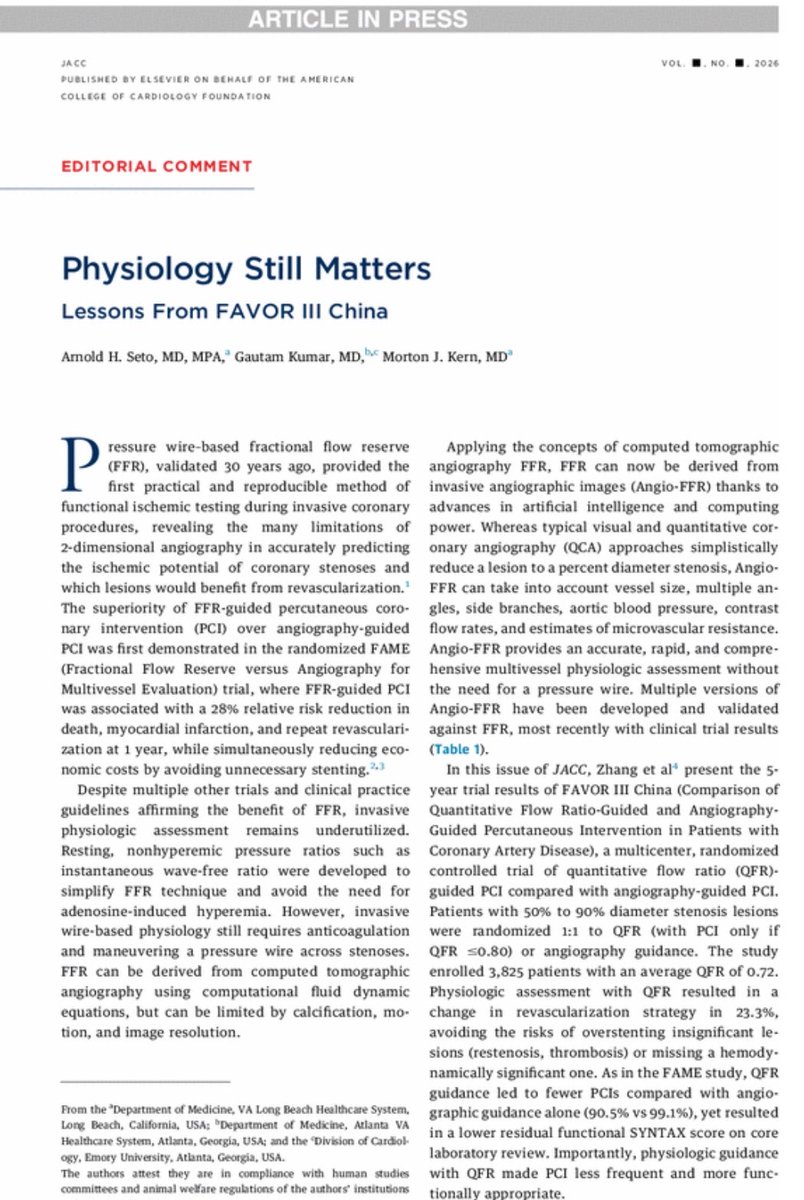
EDITORIAL
👇
jacc.org/doi/10.1016/j.jacc.…
3
5
442
CommunityRSC retweeted

Double barrel LAD following guideliner-induced dissection.
Teaching point: Don’t inject through GL, if the pressures are damped.
4
22
71
5,172
CommunityRSC retweeted
Jun 10
Coronary protection remains a key challenge in TAVI for complex anatomies.
This Flashlight reports the use of the UNICORN technique in native-valve TAVI, highlighting both the feasibility of leaflet modification and the procedural challenges that may arise, including valve migration and focal aortic dissection.
eurointervention.pcronline.c…
@Jmparadis27

18
45
4,041
CommunityRSC retweeted

Jun 10
We performed Syracuse’s/Upstate’s first BASILICA (Bioprosthetic or native Aortic Scallop Intentional Laceration to prevent Iatrogenic Coronary Artery obstruction)-facilitated transcatheter aortic valve implantation (TAVI) in an end-stage renal disease patient, who was deemed inoperable and had low left main stem (coronary) ostium. Her sinuses were not large enough, and simply performing TAVI without BASILICA would have occluded the left main stem ostium (and resulted in cardiac arrest on the table). In the appended Video, you will see the following (clockwise from top to bottom):
1. Gooseneck snare in the left ventricular outflow tract.
2. An electrified guidewire perforating the left cusp leaflet of the aortic valve.
3. Lasso creation (by snaring the guidewire that perforated the leaflet into the other guiding catheter) prior to electrifying a “flying V” to lacerate the aortic scallop.
4. “Flying V” ready to lacerate the aortic scallop.
5. Successful laceration as the “flying V” cuts through the left cusp leaflet.
This was followed by concluding the TAVI procedure. The second video demonstrates pre- and post-procedure hemodynamics with the final valve position on the transesophageal echocardiogram. The patient is extubated and doing well, and we anticipate discharge on post-operative day 1.
2
12
34
2,177
CommunityRSC retweeted

Jun 9
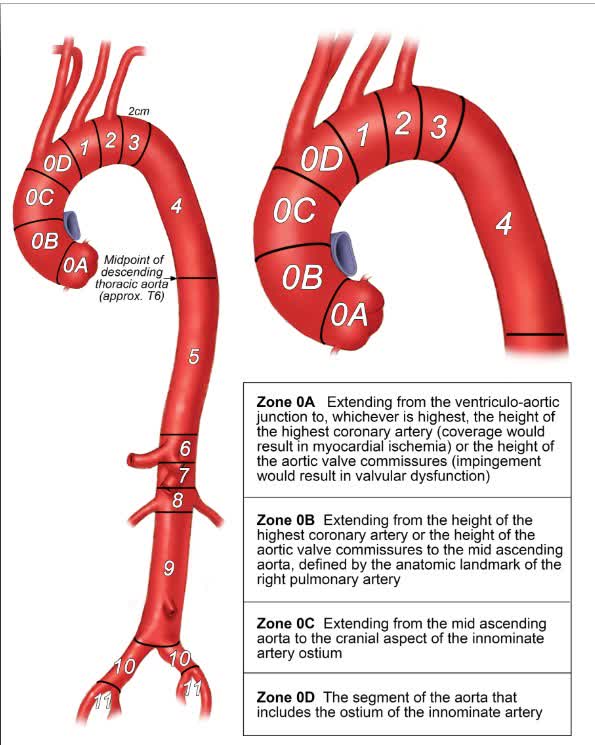
#InDepth on the global, multidisciplinary ARCH-ARC consensus statement to standardize reporting for thoracic aortic repair. ahajrnls.org/4dXF6xP
1
57
145
17,213
CommunityRSC retweeted

In awe of the remarkable expertise and dedication reflected in this work. Deeply grateful to the authors for contributing such a wealth of knowledge that will undoubtedly shape and advance the future of structural heart interventions.
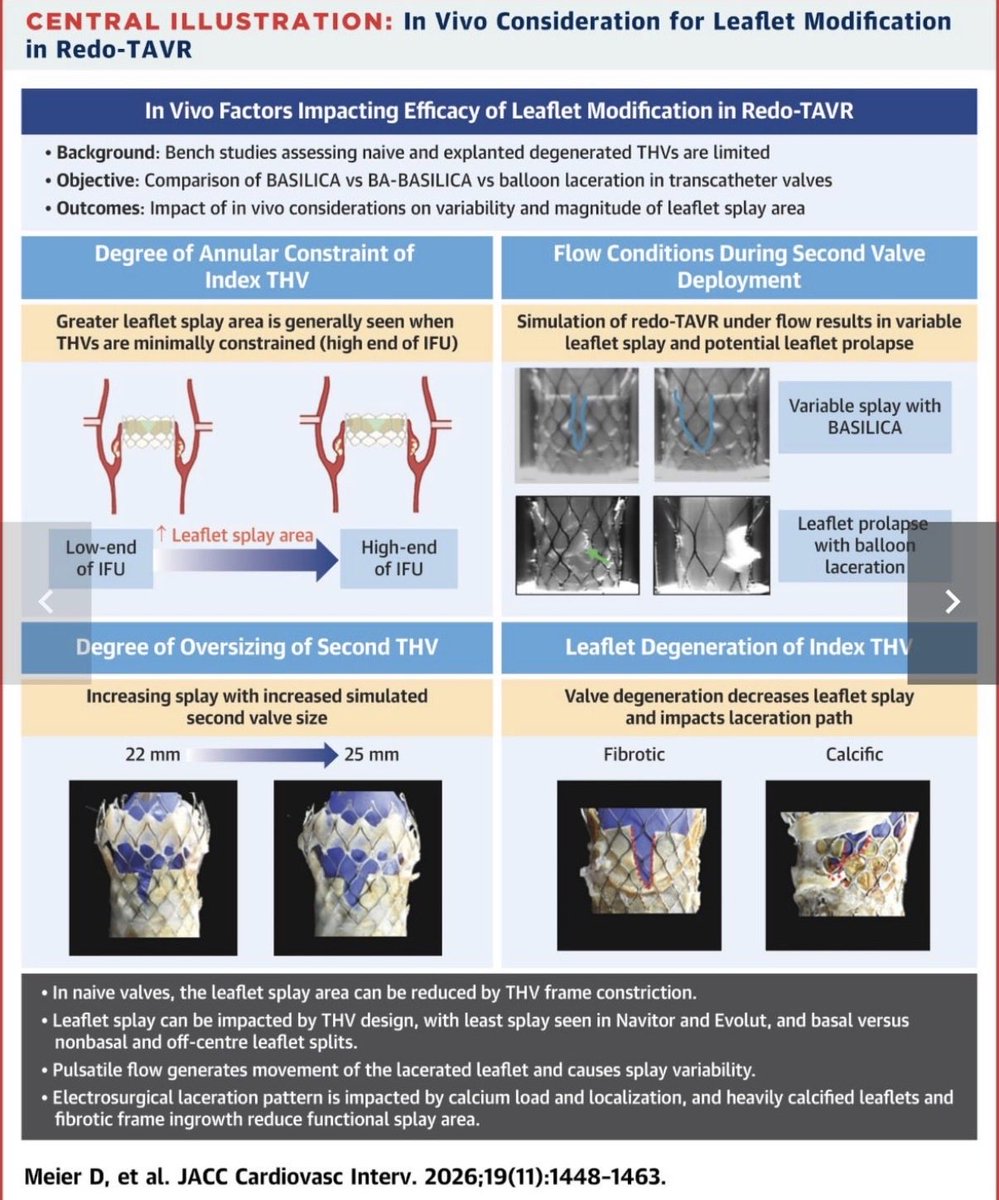
Leaflet Modification for Redo-TAVR: Impact of Valve Type, Expansion, and Failure Mode—A Bench Study
jacc.org/doi/10.1016/j.jcin.…
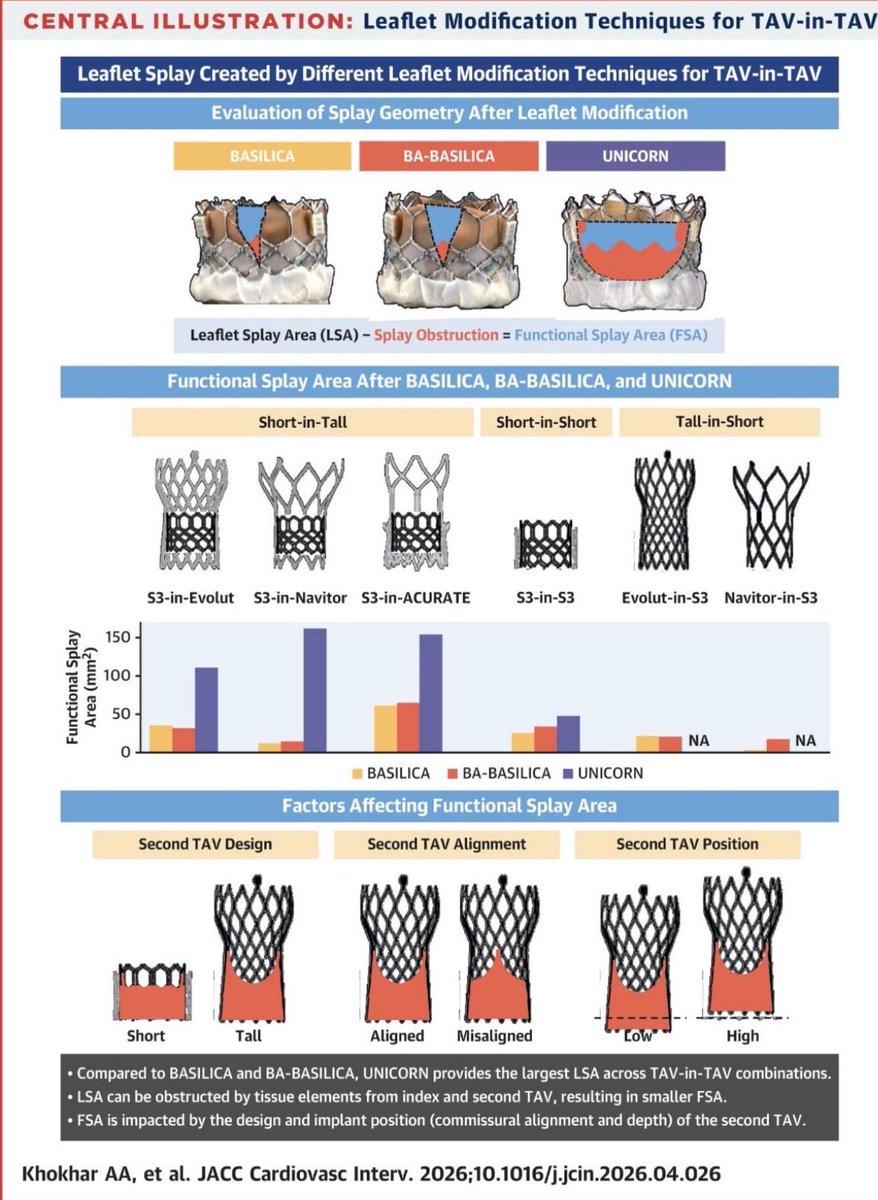
Comparison of Leaflet Modification Techniques for TAV-in-TAV: Insights From Bench Testing
jacc.org/doi/10.1016/j.jcin.…
A Proposed Anatomical-Fluoroscopic Workflow to Identify the Optimal Split Line for Leaflet Modification in Redo-TAVR
jacc.org/doi/10.1016/j.jcin.…
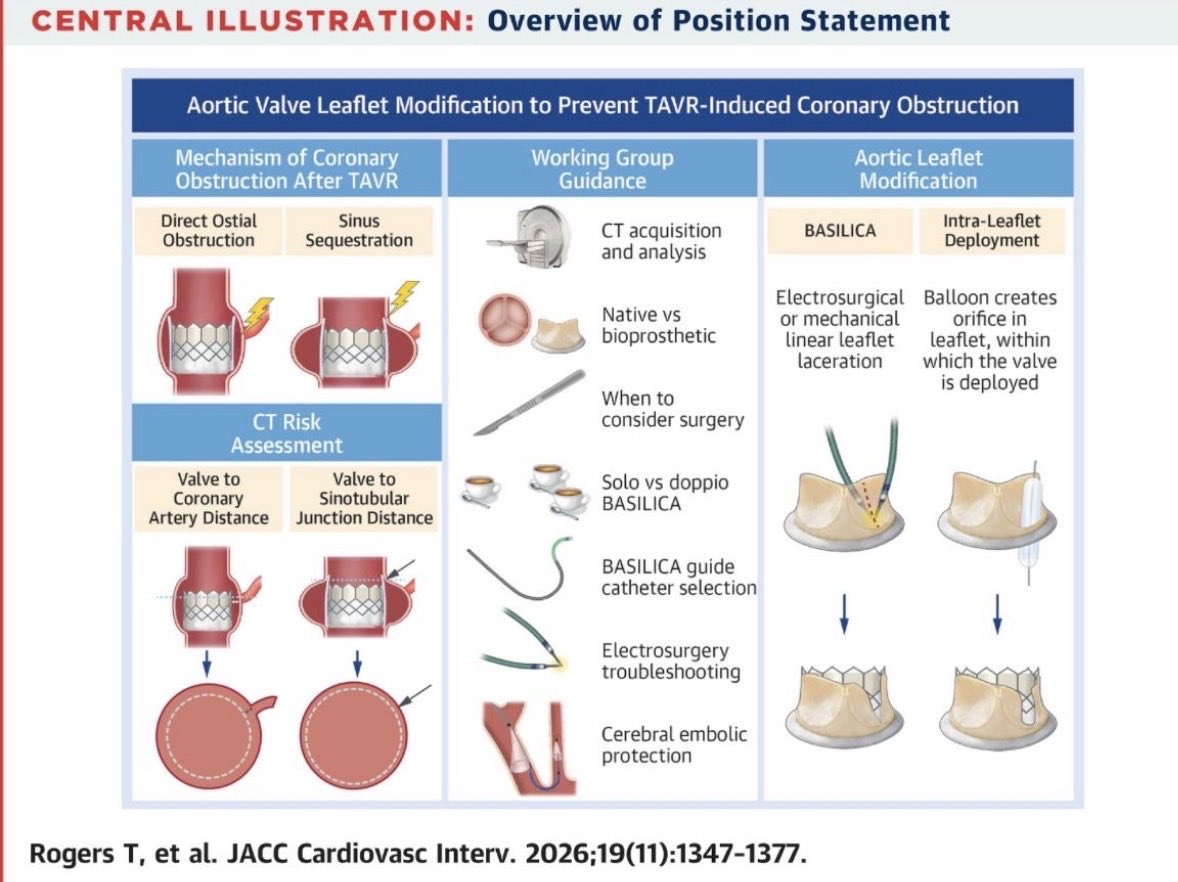
Aortic Valve Leaflet Modification: A Working Group Position Statement on Best Practices and Step-by-Step Guide
jacc.org/doi/10.1016/j.jcin.…
Impact of Leaflet Modification on Redo-TAVR Feasibility: A Computed Tomography Simulation Study
jacc.org/doi/10.1016/j.jcin.…
S3UR vs S3U: Bench Performance in TAVR, ViV, and Redo-TAVR
jacc.org/doi/10.1016/j.jcin.…
@akcmahi @DrArifK @jtsaxon @jamiemccabeMD @azeemlatib @CathElectroSurg
#CardiovascularResearch #HeartTeam #CardioInnovation #StructuralHeartDisease #AcademicCardiology

1
14
38
3,645
CommunityRSC retweeted
Four days,
Thousands of connections,
Countless Memories✨
🎬The #TCTAP2026 Sketch Video is here!💙
Take one more walk through the venue, revisit the excitement of the sessions, and celebrate the people and experiences that made this year's TCTAP so special.
4
5
376

NEW ASE Recommendations for the Intraprocedural Imaging for M-TEER bit.ly/ASE_M-TEER @SLittleMD @ASE360 @JournalASEcho @ACCinTouch @SCAI @purviparwani @iamritu
1
73
213
17,537
CommunityRSC retweeted

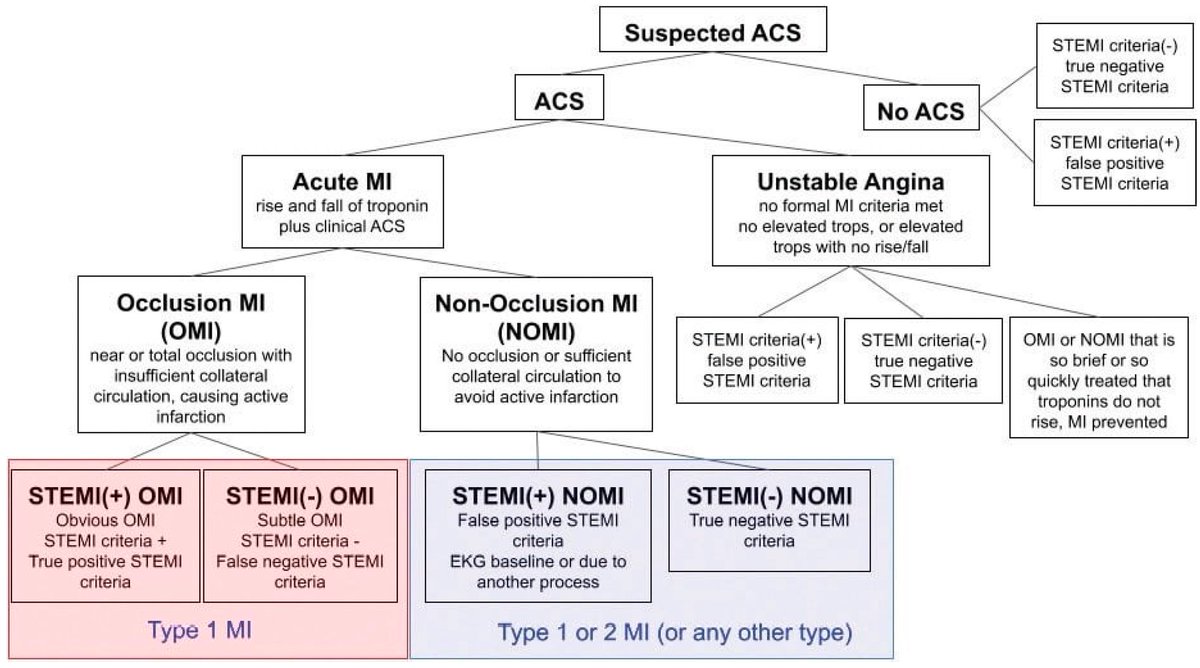
Acute epicardial Coronary artery Occlusion Myocardial infarction (#ACOMI): this is going to be highlighted as the subset of #ACS needing immediate #PCI regardless what #EKG shows…persisting symptoms, increasing #Troponin & #echofirst (regional LV contraction impairment) pivotal

The STEMI vs NSTEMI paradigm may be missing the real target.
Occlusion Myocardial Infarction (OMI) refers to an acute myocardial infarction caused by a culprit coronary artery that is completely or nearly completely occluded, resulting in critically reduced blood flow to the myocardium. In simple terms, OMI identifies the patients who need urgent reperfusion because an artery is blocked, regardless of whether the ECG fulfills STEMI criteria.
A 2024 study of 334 ACS patients found that 40% of OMI patients did NOT meet STEMI criteria. Despite having an acutely occluded coronary artery, these patients were often classified as NSTEMI and experienced major delays in treatment.
Among STEMI-negative OMI patients, only 11% underwent PCI within the first 12 hours, compared with 77% of STEMI-positive OMI patients.
The concerning part is that both groups had remarkably similar disease severity:
🔺 Similar rates of PCI
🔺 Similar rates of mechanical complications
🔺 Similar rates of electrical complications
🔺 Similar angiographic evidence of acute coronary occlusion
In other words, many patients without classic ST-elevation had the same dangerous pathology that traditionally prompts emergency cath lab activation.
The authors argue that focusing solely on STEMI criteria can cause clinicians to miss a substantial number of patients with acute coronary occlusion. Instead, ECG interpretation should focus on identifying OMI patterns, including hyperacute T waves, de Winter pattern, posterior MI, reciprocal changes, modified Sgarbossa criteria, and other STEMI equivalents.
The artery does not care whether the ECG meets STEMI criteria.
Time is myocardium. The goal is not simply to find ST elevation. The goal is to identify acute coronary occlusion and restore blood flow before irreversible myocardial injury occurs.
Perhaps it is time to shift the conversation from STEMI vs NSTEMI to what truly matters: OMI vs NOMI.
5
29
4,306