
Chair, Radiation Oncology, University of Vermont Health
Joined January 2014
- Tweets 6,997
- Following 1,368
- Followers 4,600
- Likes 42,311
1,361 Photos and videos










Nat Lester-Coll, MD retweeted

Delighted that our STAMPEDE paper on abiraterone therapy selection with MMAI in high risk M0 HSPC now out. kwnsfk27.r.eu-west-1.awstrac…
4
25
83
11,185
Nat Lester-Coll, MD retweeted

Jun 2
Kidney SABR on the front cover of @TheLancetOncol. A well-deserved recognition for @_ShankarSiva for his work and efforts over the past 10 years.
thelancet.com/journals/lanon…
2
37
97
27,937
Nat Lester-Coll, MD retweeted

May 31
#ASCO26
Talk about real-time updates. NEJM paper now online and my predictions and inferences appear true.
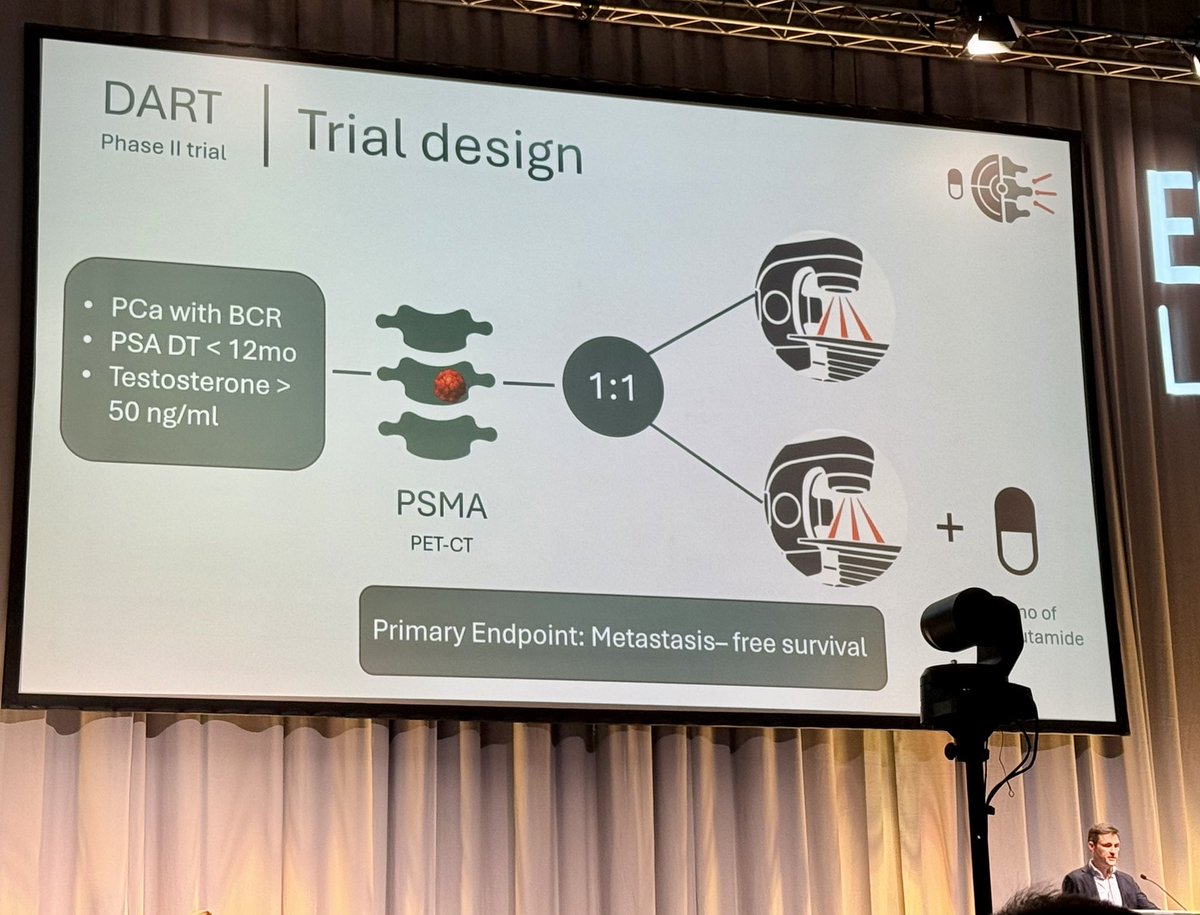
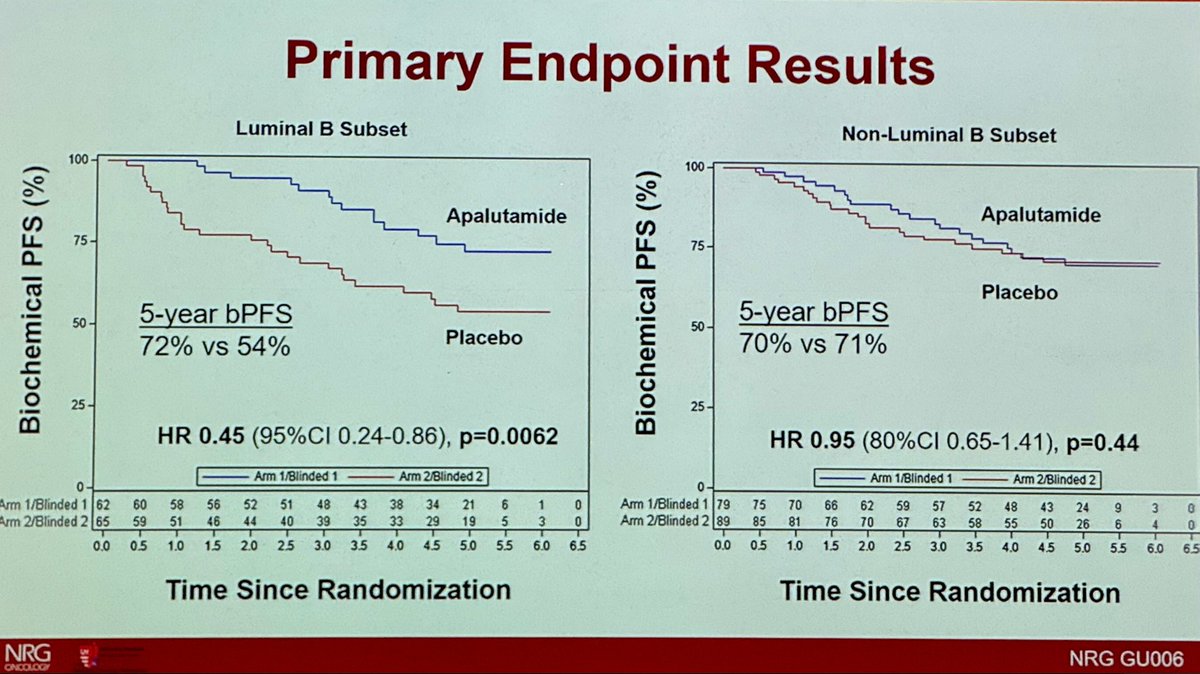
Majority of MFS events were by PET not conventional imaging. "Most distant metastases were identified by PSMA PET (53.0% of those in the apalutamide group and 60.7% in the placebo group)"
VERY IMPORTANTLY: "No significant between-group difference was observed in metastasis-free survival assessed with conventional imaging alone (hazard ratio, 0.84; 95% CI, 0.67 to 1.07)"
Not only does MFS cross 1, but the HR also crosses the surrogate threshold effect (0.81).
@urotoday @PCF_select @US_FDA
May 31

#ASCO26
The PROTEUS trial results are now online...buckle up as we wait to see the full presentation. This is going to be a trial that is likely highly controversial until the full results are published.
Some may call this a homerun, others may call this the largest negative trial @ASCO 2026. Up to you to interpret!
@urotoday @EricTopol @DrChoueiri @neerajaiims @ASCO @US_FDA @NCCN @myESMO @ASTRO_org @PCF_Science @declangmurphy @mcuban
3
30
74
12,396
Nat Lester-Coll, MD retweeted

May 31
Trials in localized prostate cancer are incredibly difficult to pull off, especially given the rapidly changing imaging and therapeutic landscape, so major congrats to the investigators.
For me, top line results: small MFS benefit when MFS is defined by either conventional imaging or PSMA PET. No MFS benefit by conventional imaging.
Critically, there were significant differences in PSMA PET utilization. Post hoc analysis showed that 686 patients (64.9%) in the apalutamide group and 755 patients (71.8%) in the placebo group underwent PSMA PET at least once.
That difference is greater than the absolute MFS benefit (when MFS is defined by either conventional or PSMA imaging) and may mean that the MFS benefit is confounded by the differential use of PSMA PET at biochemical recurrence. The extent of that confounding will depend on the comparative probability of detecting Mets at BCR using PET vs conventional imaging in the trial cohort. Would be interested in that data.
Does PROTEUS change practice? Given the above, I'm not sure the argument is there to go from RP alone (the current standard) to RP ADT ARPI. Will be interested in the substudy results.
#ASCO26 #radonc #medtwitter #pcsm
nejm.org/doi/full/10.1056/NE…
7
18
66
6,577
Nat Lester-Coll, MD retweeted

May 30
JUST In: TALAPRO-3 published in @NEJM
Adding #talazoparib to enzalutamide/ADT
=>3-year rPFS: 77% vs 56% in HRR-deficient metastatic prostate cancer !
Looking forward to full presentation by @neerajaiims who keeps changing SOC, one trial at a time.
@ASCO #ASCO26 @OncoAlert


3
67
157
18,752
Nat Lester-Coll, MD retweeted
May 30
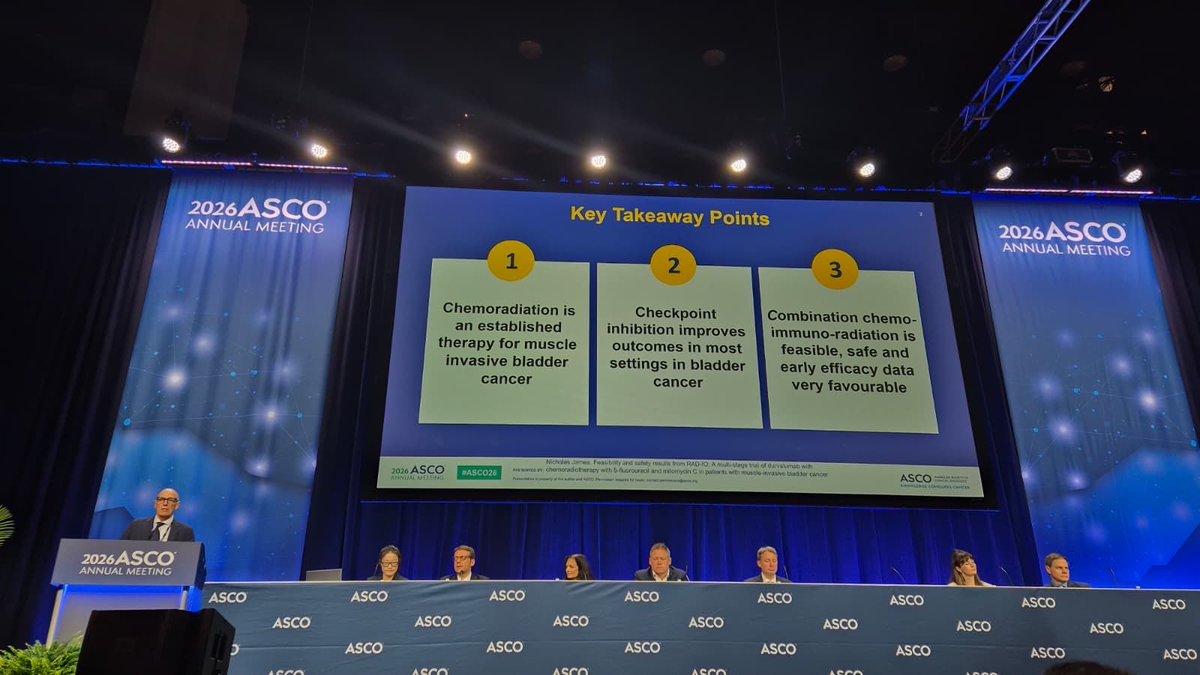
Bladder-preserving IO-CRT strategy shows encouraging early results in RAD-IO presented by #NicholasJames: durvalumab chemoradiotherapy achieved 1yDFS 79%, 12-mo PFS 83%, and OS 96% with manageable toxicity in MIBC.
#ASCO26 #BladderCancer
@OncoAlert @ASCO @OncBrothers


1
29
47
2,441
Nat Lester-Coll, MD retweeted

May 30
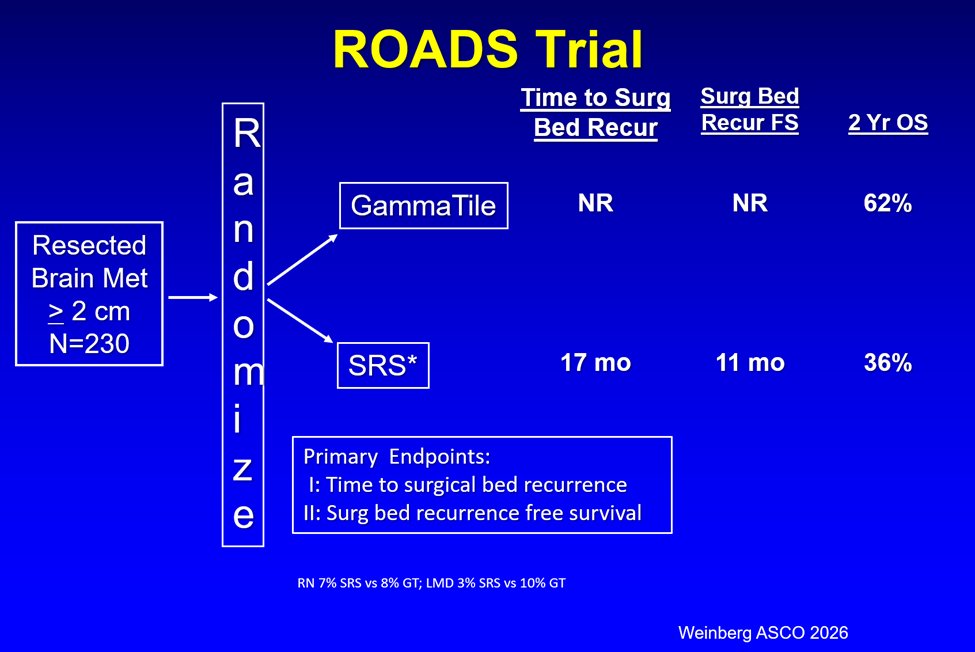
🚨🚨 ASCO 2026 Final Results Randomized trial resected brain met Brachytherapy vs Post-Op SRS🚨
- Incredible Surg Bed Control with Brachy (↑↑OS as well)
- Surg bed recurrence 12% SRS vs 1% GammaTile
7
46
105
6,294
Nat Lester-Coll, MD retweeted

May 26
This trial represents a decade of work—hypothesis → design → accrual → follow-up → data lock → Presented at @ASTRO_org 2025 plenary →publication in @JCO_ASCO
ascopubs.org/doi/10.1200/JCO…
🙏 To the patients, families, clinicians, and my team: A BIG thank you.
6
46
157
8,957
Nat Lester-Coll, MD retweeted

May 18
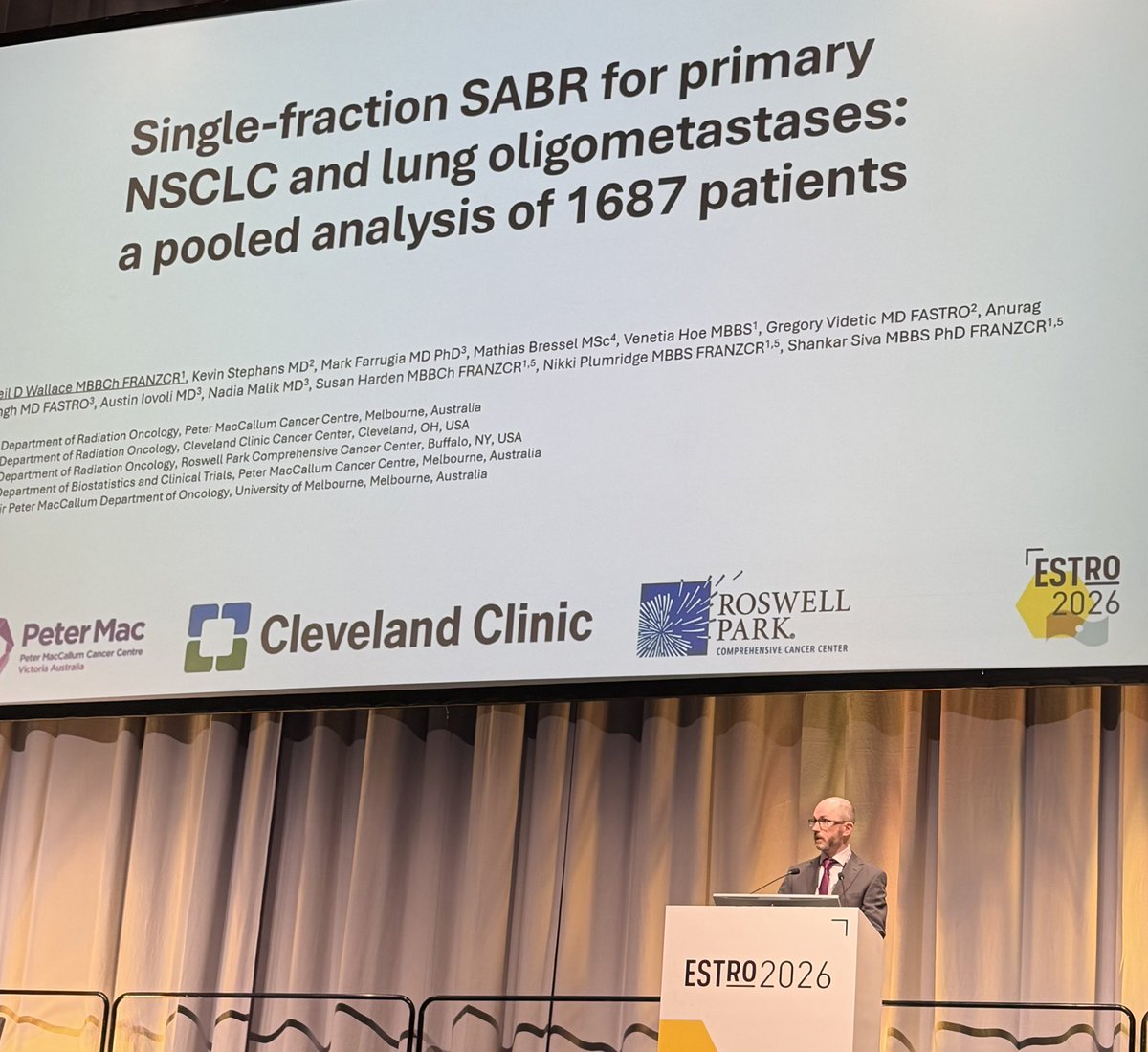
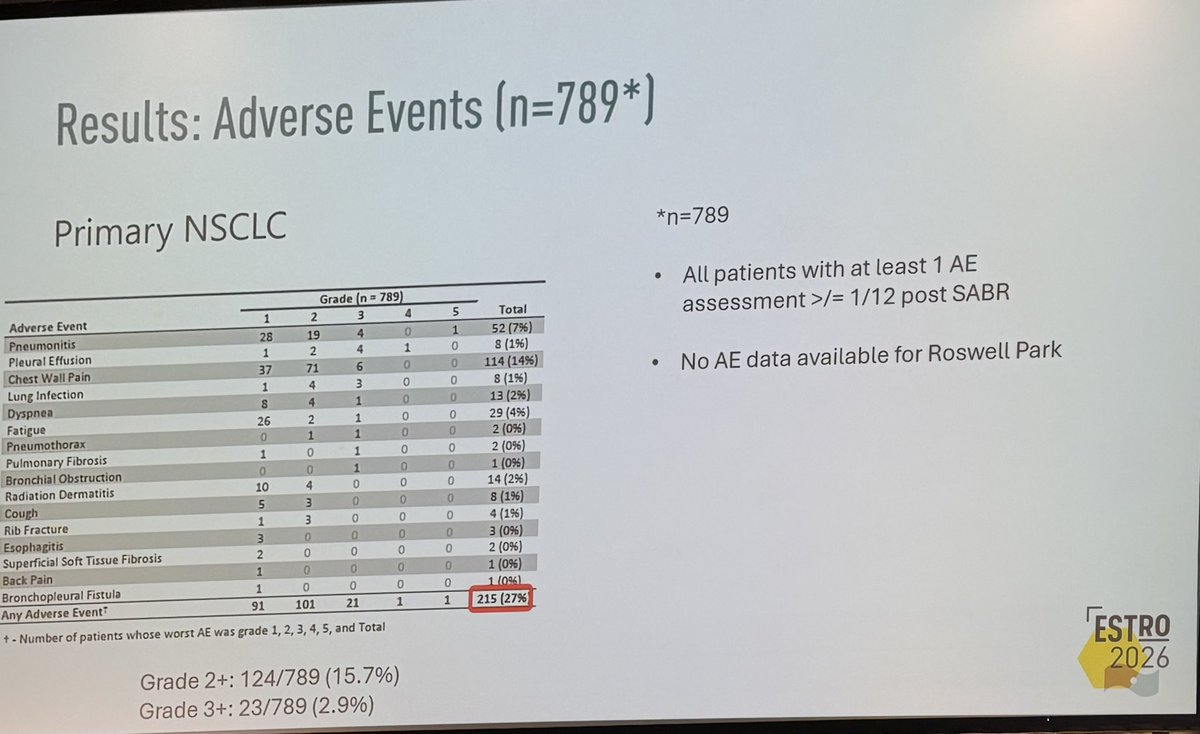
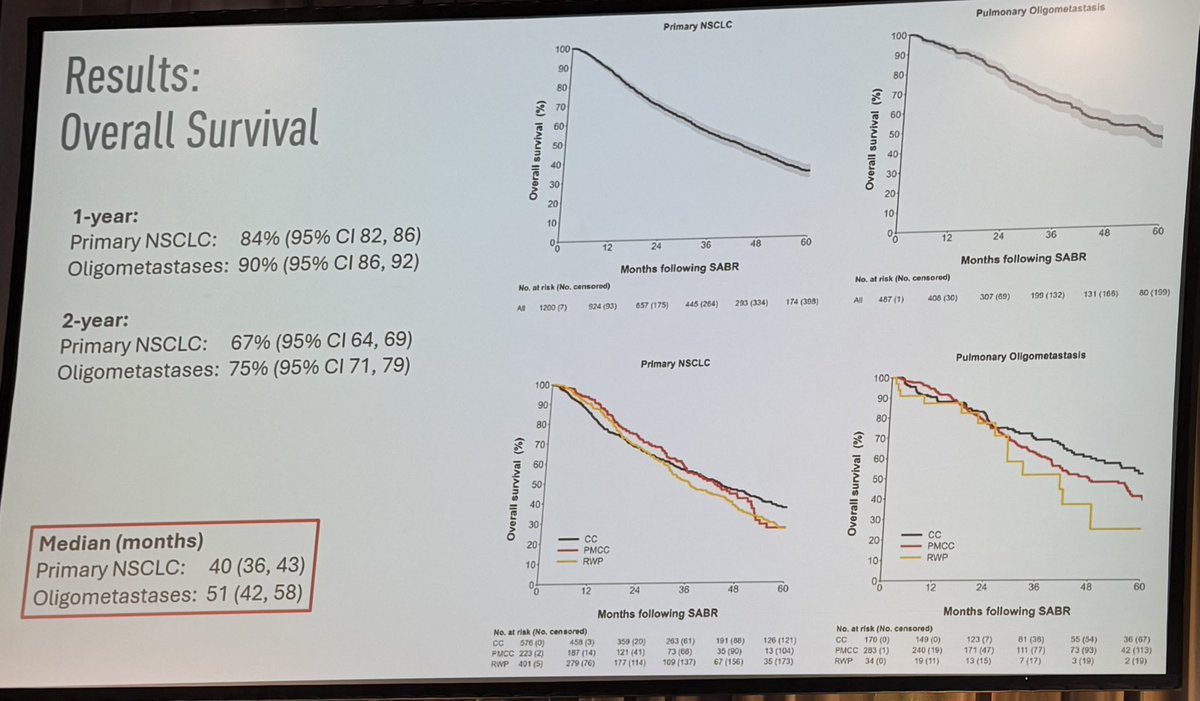
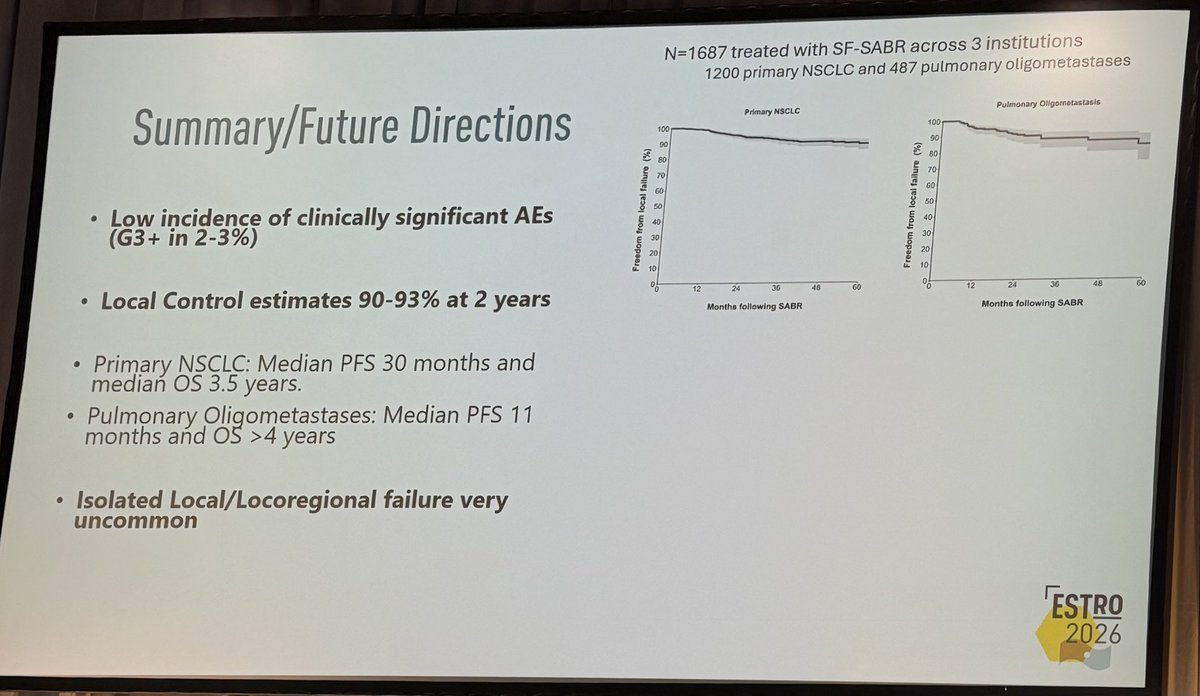
👏🏽👏🏽👏🏽@neildwallaceie at #ESTRO26 - 1687 patients receiving single fraction SABR for #lungcancer and pulmonary oligomets, @PeterMacRadOnc / @ClevelandClinic / @RoswellPark. Fantastic local control, and low adverse rates. Should we be using “one stop” SABR more often #radonc ?
5
41
81
10,124

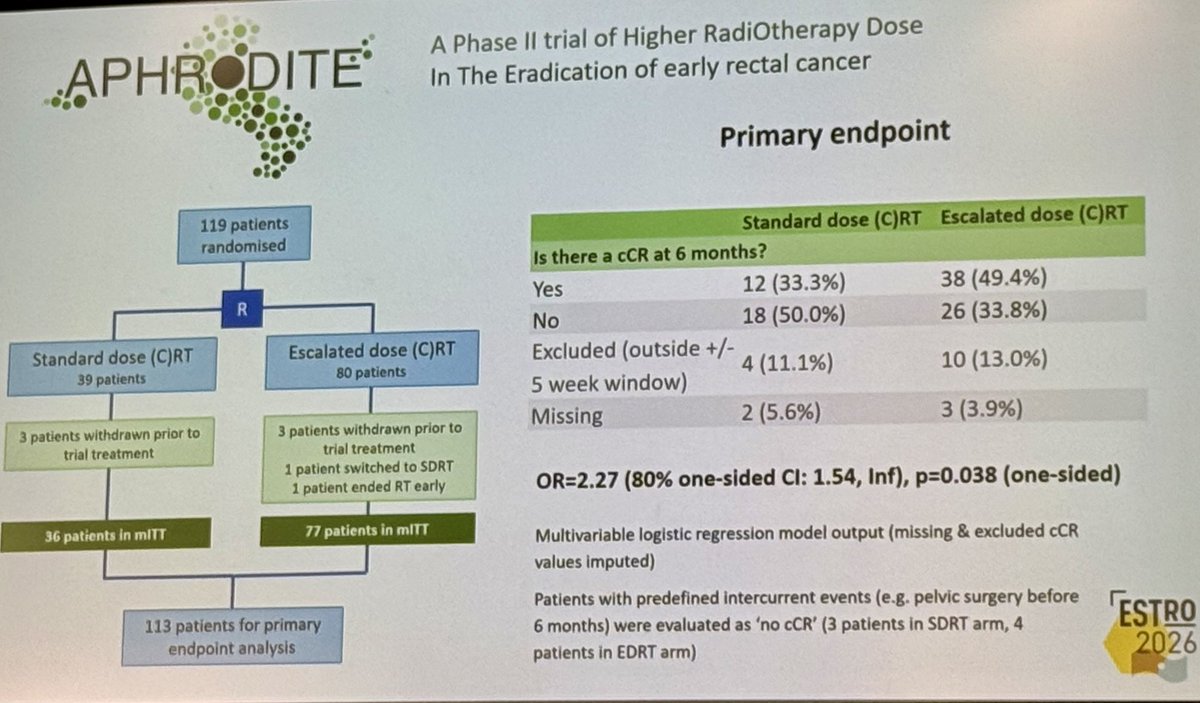
#ESTRO26 @cancerphysicist APHRODITE trial: EDRT (62Gy SIB) boosted 6-mo cCR to 49.4% vs 33.3% with SDRT in early rectal cancer ( 16%; OR 2.27, p=0.038). First RCT evidence for dose escalation benefit low toxicity!

1
37
53
3,703
Nat Lester-Coll, MD retweeted
May 17
@VedangMurthy is one of the smartest prostate oncologists out there and, when he presented at MSKCC grand rounds, he made the important point that, in India, the local disease they're seeing is much more advanced than in the US (and presumably Europe).
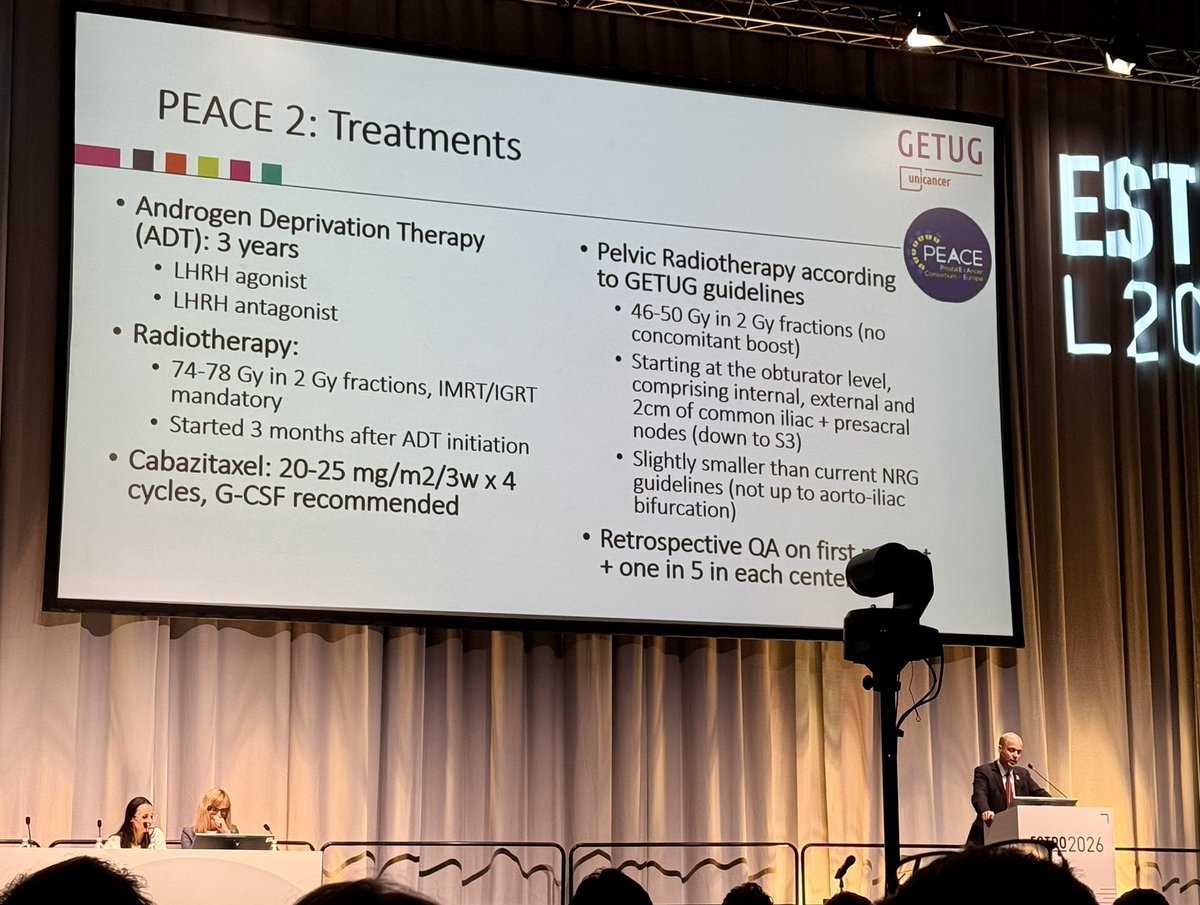
Recall, PEACE2 included MRI-defined T3 disease.
My conclusion, integrating PEACE2, the NRG data presented at ASTRO, and POP-RT, is that in screen-detected HR or VHR localized PCa, especially where PSMA PET is NED in the pelvis, the benefit of elective pelvic nodal irradiation is de minimis. Once these trials are published, I think SOC, in screen detected, PSMA PET imaged HR or VHR N0 disease, is prostate-only RT.
That said, when you have PSMA PET N0 HR/VHR disease that is so locally advanced that it's causing symptoms or where you have GS9 disease where an MRI shows EPE/SVI apparent to even a 1st year medical student, only then should one consider elective pelvic nodal RT.
My two cents.....#ESTRO26
May 17

This is mostly STAMPEDE HR staged with CT Bone scan... And surely surprised by the results! Would love to see the effect cabazitaxel is having in sterilising micro mets..
Biological interaction?
Food for thought!

5
11
49
6,406
#ESTRO26 the pendulum continues to swing—this time against against pelvic RT in high risk prostate ca
⛔️ improvement in MFS, PCSS, OS !
Presentation of PEACE2 by @PBlanchardMD



13
26
1,499
Nat Lester-Coll, MD retweeted
Apr 27
5-Abstract 4500: RADICAL
RADICAL brings radium-223 into RCC; pairing bone-targeted radiotherapy with cabozantinib for pts with bone mets. Much needed efforts to overcome a major challenge in RCC.
@DrRanaMckay @ASCO @OncoAlert
1
6
14
1,683
Nat Lester-Coll, MD retweeted
Mar 13
Wanted to highlight our AASUR trial. Was an awesome multi-institutional collaboration. Especially grateful to @ThePCCTC and @UMichRadOnc team (@DrSpratticus, Jason Hearn, et al were our 2nd leading accruers). But a true team effort.
And many thanks to @JNJInnovMed and @PCFnews for funding.
TL;DR: in VHR localized PCa, a short course (6mo), ADT/ARPI regimen combined with 40/5 prostate-only SBRT had favorable toxicity profile, rapid T return, and, despite not meeting superiority threshold, BCR rates that looked similar to long course ADT historical controls. These patients were not DECIPHER-selected or PSMA PET staged.
It may be that scADT/ARPI RT would provide equivalent results in the vast majority of RT-treated VHR, localized dz. Obviously this would require confirmation in an appropriately sized NI trial. #radonc #pcsm
3
13
37
3,056
Nat Lester-Coll, MD retweeted
Feb 27
#GU26 and #fengsymposium was a blast to see progress.
Hoping it eventually moves away from San Fran 😁. Another red eye on the books back home.
My observations from PCa sessions:
- the field continues to push for over tx and many fail to recognize high risk dz is not high risk anymore for most patients. Enzarad negative, Rtog 0924 neg, ascend-RT neg for MFS/OS, peace2 neg. RT ADT plenty for most. Many need even less. Select trials paving the way.
- for mHSPC not all patients need doublet let alone triplet; age matters
- continuous ADT can often be more harmful than helpful now with MDT
-most BCR patients post RP do not need ADT—> get biomarker testing to help
-many have jumped on bandwagon that OS too hard to improve and settling for early non-surrogate endpoints; peace3 should remind us it’s possible
-sequential PARPi /Abi often just as good as combination
-early germline/somatic testing for all high risk disease remains without data to support it; even testing in mHSPC unclear benefit as can give PARPi in mCRPC setting (earlier not better than later).
-actinium RLT promising but toxicity remains concern
-neoadj before RP remains largely ineffective, adds costs and toxicity and most still need postop tx.
8
32
96
12,645
Nat Lester-Coll, MD retweeted
Feb 19
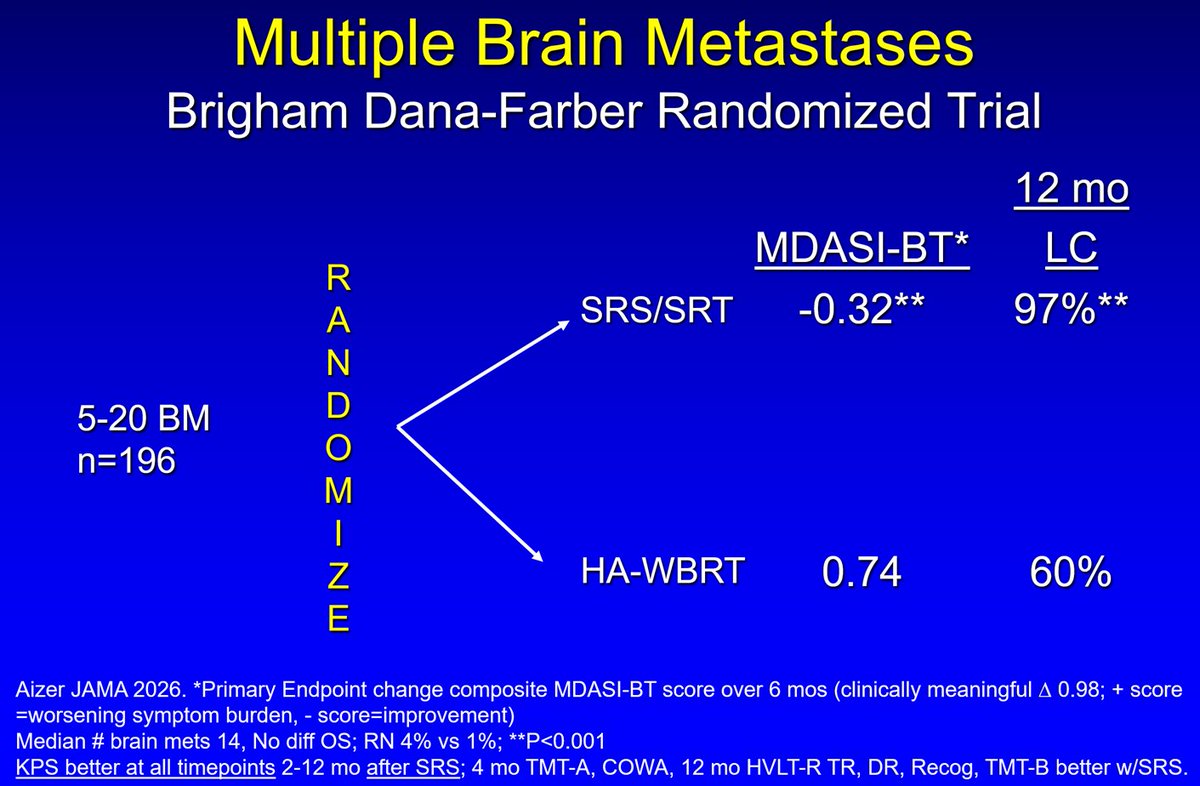
🚨🚨Multiple Brain Mets Randomized Trial🚨
· Significantly less symptom burden with SRS compared to HA-WBRT
· Better ADL, cognition & KPS after SRS
· SRS Standard of Care 5-20 brain mets
jamanetwork.com/journals/jam…
7
55
120
18,596
Nat Lester-Coll, MD retweeted

Feb 18
Full free-text link to the ASTRO GU Resource Panel's response to the IRRADIATE publication @RicBertolo @EurUrolOncol
authors.elsevier.com/a/1mdSX…
@NehaVapiwala @ASTRO_org
4
24
70
9,432
Frustrating @UHC @Optum #priorauth Peer-to-peer requested during my admin time multiple days this week, but “no doctor available”? Now expedited to a random unscheduled call today-Monday. We’re not available 24/7. Figure out how to schedule properly…unnecessary delays & waste!
2
8
1,003