
Consultant Haematologist. Interested in haemato-oncology in general and multiple myeloma in particular.
Joined March 2015
- Tweets 1,718
- Following 313
- Followers 360
- Likes 996
70 Photos and videos








Simon Stern retweeted

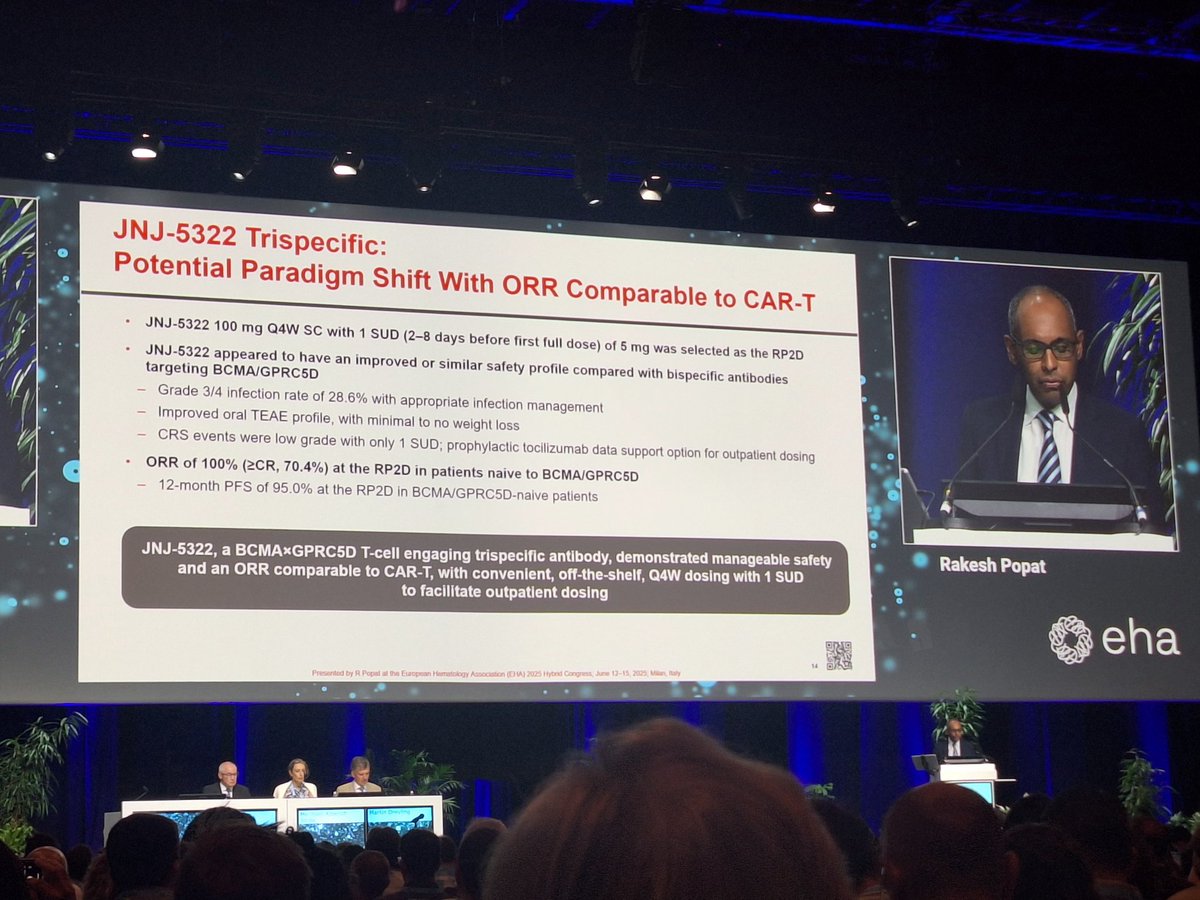
#mmsm #EHA26 MonumenTAL-3
Published @NEJM
➡️ nejm.org/doi/full/10.1056/NE…
✅RCT, phase 3: Tal-DP vs Tal-D vs DPd
✅ Treatment was until progression or intolerance (not time-limited)
✅ Early relapse ≥1 prior line including lenalidomide PI ( no anti-CD38 refractory)
✅allowed for T-cell redirecting >3 months
🧵
1
13
21
1,556
Simon Stern retweeted

Nagelsmann dressed like he’s going down Arnold’s Drive-In with Pottsy and Ralph Malph.
5
5
24
3,168
Rehydration break coming at a good time for the rattled Germans. #GERCUW
84
Simon Stern retweeted

Nigel Farage Listens to the News
102
1,370
5,333
303,578
Simon Stern retweeted

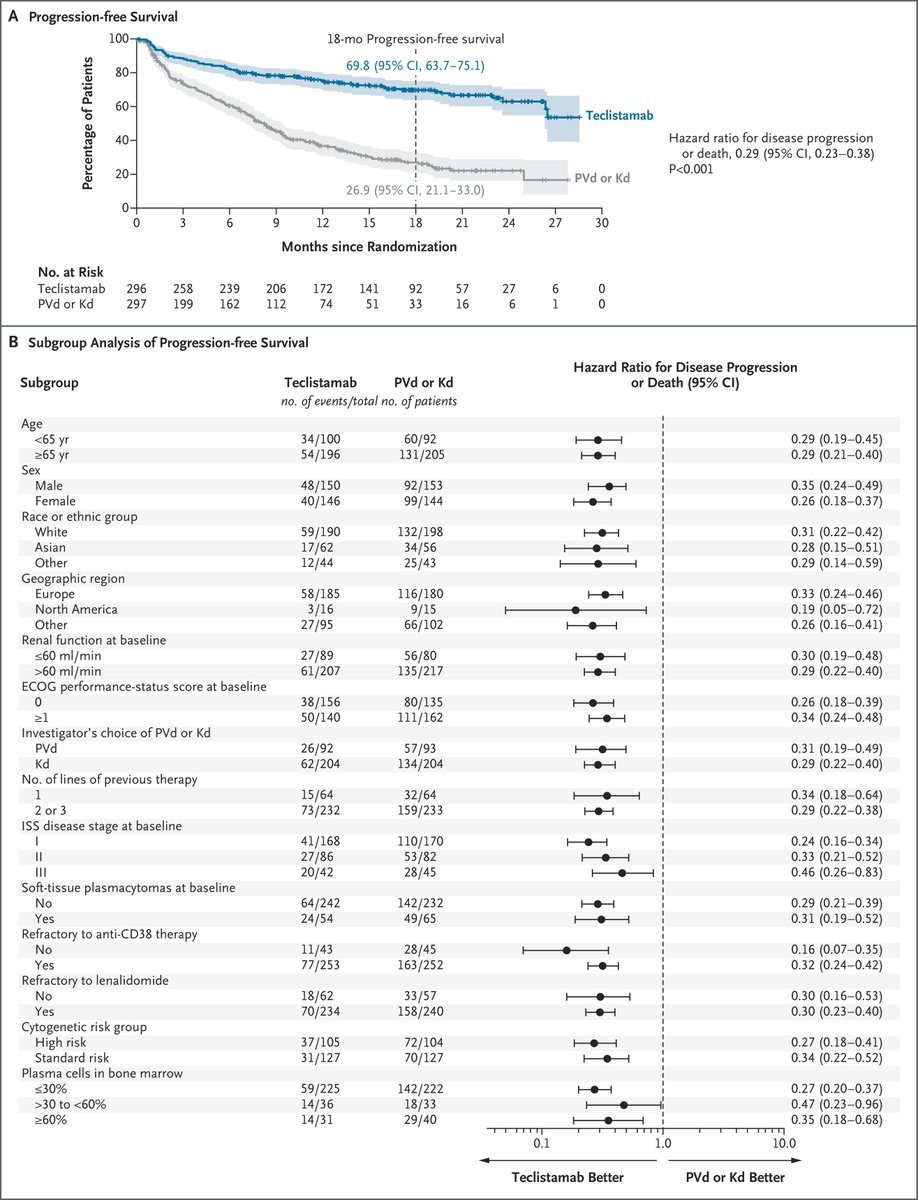
MajesTEC-9 trial: Teclistamab vs. VPd or Kd in RRMM, 1-3 prior lines. N=593, median F/U: 17.3 months. 18-month PFS 70% vs. 27%, HR: 0.29. 41% grade 3-4 infections, 6.5% deaths in Teclistamab arm #mmsm #ASCO26 @NEJM nejm.org/doi/full/10.1056/NE…
7
16
2,769

Simon Stern retweeted

May 28
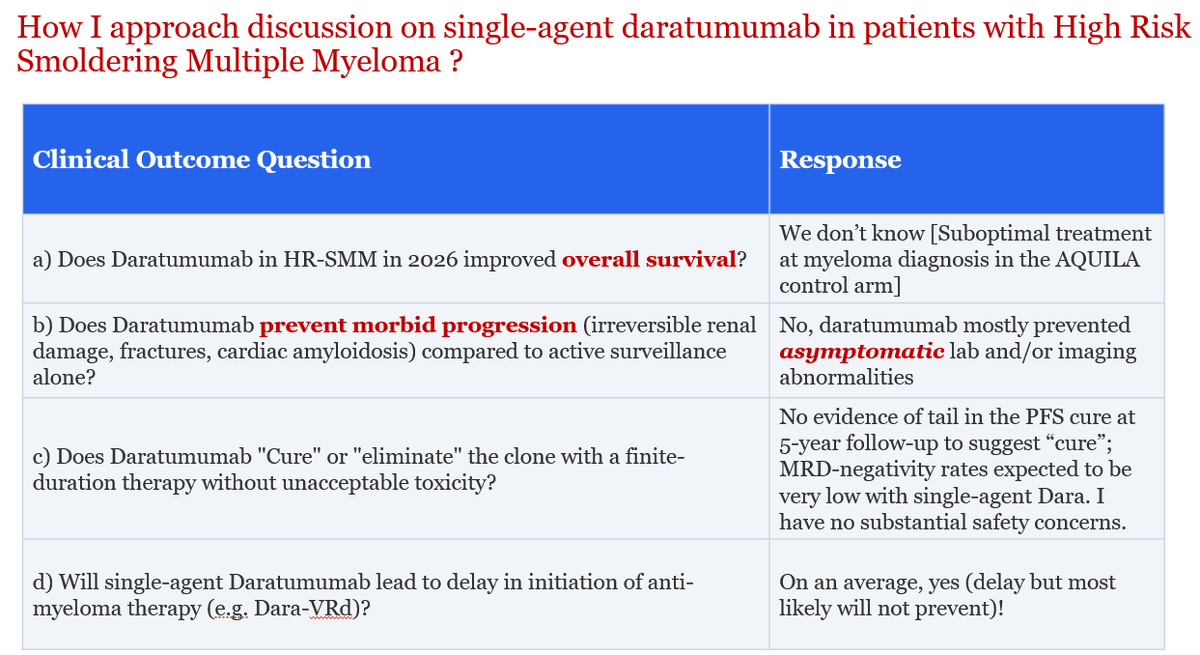
Since management of High Risk-Smoldering Multiple #Myeloma often comes up in clinic these days (and leads to spirited discussions with trainees and colleagues), sharing my approach here on how I counsel patients on the use of single-agent daratumumab.
I am genuinely excited though about fixed-duration BCMA BsAbs in selected patients, and looking forward to more data in coming years!
2
12
39
2,244
Simon Stern retweeted

May 23
AI reads almost everything.
But medicine is still practiced in the space between evidence and judgment.
That space remains profoundly human.
May 23

AI is not a medical expert. AI is a pseudo expert. It possesses incredible a capacity to scour all of the available information and put together a coherent answer or summary. This answer or summary will greatly help the general public and physicians who are not experts in a given disease by making search, retrieval, synthesis of available information. But it’s not an expert.
AI cannot be expected to know data that’s known to experts but is not yet published. It cannot know when data in published form differs from that experienced in real world practice by clinicians who see a large volume of patients with the same disease. Where the published data are wrong or exaggerate benefits or minimize risks. It cannot judge the right treatment option among similar competing treatment options (except superficially), especially based on what the patient evaluation reveals on history and examination.
AI appears to be an expert in everything in the world by knowing what experts have written and made public but lacks wisdom by the very nature of how it works to produce the answer. It’s not thinking. It knows as the famous saying where the puck is but not where it’s going to be.
That’s why the even the most ardent proponents of AI including the uber rich who own the models will always seek out the best human expert available for serious diseases. They may use AI to provide a summary of their disease for the expert but they are not going to mistake or substitute AI for the expert. I don’t see this changing. Because medicine is more than knowing everything that’s published or being able to retrieve it quickly.
We live in a world of medicine where it’s easy to confuse pseudo experts who have gained or granted prominence with real depth of expertise and wisdom. So it’s easy to see how a lot of us are mesmerized by the speed and eloquence of AI to answer queries. Yes it does that well (and is probably sufficient 90% of the time). But as you learn how LLMs and other AI tools work you know it’s no expert, but a useful side kick. I do think it can help both experts and non experts but we must know what it’s capable of and what it’s not.
5
5
17
5,586
Simon Stern retweeted

1/ 🧵 ANDROMEDA final analysis is practice-changing for newly diagnosed AL amyloidosis.
IMPORTANT tweets: 3/4 and 6 for clinicians who treats Amyloidosis
D-VCd = daratumumab bortezomib/cyclophosphamide/dexamethasone.
With 61.4 months median follow-up, D-VCd improved depth of response, organ recovery, MOD-PFS, and OS. 🔥
#USMIRC #MedEd #medtwitter #mmsm #myeloma @USMIRCNEWS @US_HMC @MedwatchKate @Larvol @OncoAlert
5
40
114
8,480
Simon Stern retweeted
2/ Key efficacy signal:
✅ Hematologic CR: 59.5% with D-VCd vs 19.2% with VCd
✅ OR 6.03; P<0.0001
✅ VGPR or better: 79.0% vs 50.3%
This is not just more responses — it is deeper responses. 🎯
#USMIRC #MedEd #medtwitter #mmsm #myeloma @USMIRCNEWS @US_HMC @MedwatchKate @Larvol @OncoAlert


1
2
6
891


Apr 17
Intriguing paper in
@ASHbloodjournal suggesting the delayed development of MRD negativity in transplant-eligible newly diagnosed myeloma patients with t(11:14) does not prevent the translocation's good prognosis.
ashpublications.org/blood/ar…
75
Simon Stern retweeted
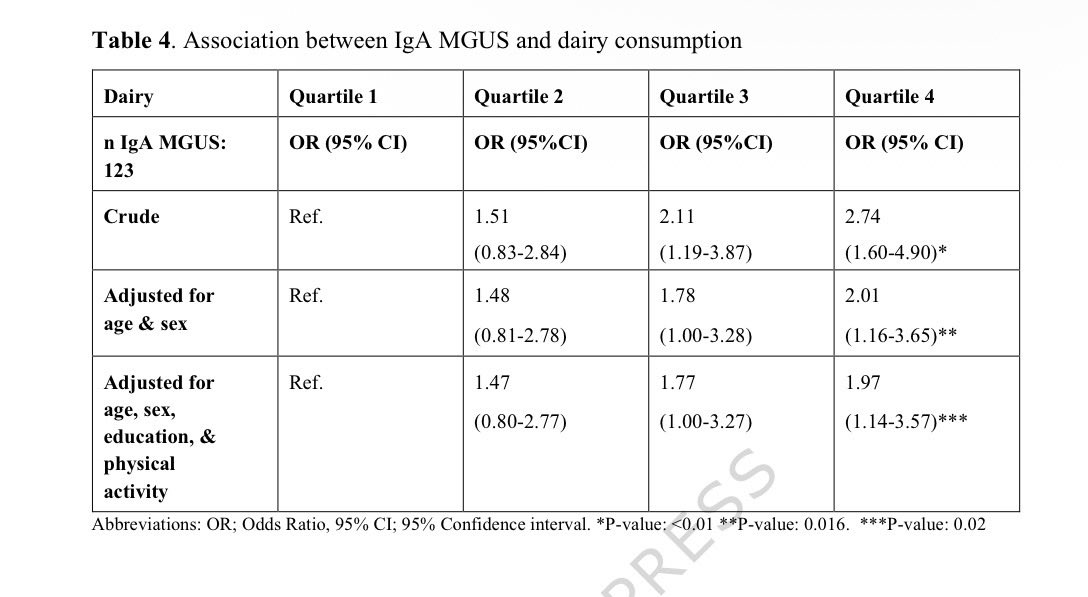
Glad this negative study was published by the @iStopMM group! No association of any dietary pattern with MGUS overall in this large population-based screening study. Before putting the burden of dietary intervention on our patients (beyond common sense), we must have randomized trials with clinically relevant endpoints.

Important work @iStopMM @BloodCancerJnl #mmsm
New study from iStopMM screened >75000 people for MGUS
✅ >27000 completed a food survey — 1,020 had MGUS
✅ Overall diet & dietary patterns are NOT major risk factors for MGUS(imp finding)
🛑Exception: High dairy intake was linked to 2x higher odds of IgA MGUS (OR 2.01)
Bottom line: What you eat likely isn't driving your multiple myeloma risk — but dairy's role in IgA MGUS is an interesting finding
➡️ nature.com/articles/s41408-0…
1
10
34
4,622
Simon Stern retweeted

Apr 1
Yes you can come, just don't be weird.
Me:
967
11,152
67,776
1,649,391
Simon Stern retweeted

Mar 29
Precision medicine in #myeloma demands precision imaging: is whole body MRI #WBMRI the solution?
@ProfMessiou
doi.org/10.1186/s40644-026-0…
2
8
354
Simon Stern retweeted
Mar 23
Grateful to @ASHClinicalNews for highlighting our article on sFLC>100 criterion for #Myeloma diagnosis!
This creates two problems: Potential over-treatment of a majority of patients in a heterogeneous group & driving PFS benefit in high-risk smoldering myeloma trials by events that are not clinically meaningful!

Researchers propose the removal of an sFLC ratio ≥100 as a standalone myeloma-defining event in the IMWG diagnostic criteria for #MMsm, as new findings indicate the previously cited 80% risk of disease progression at two years may be substantially lower: ow.ly/TpF750YwhlS
12
40
4,753
Simon Stern retweeted

As BsAbs move into earlier lines, infection risk is the elephant in the room!
Kim et al. @BloodAdvances: 75% cumulative infection rate at 24 mo.
Neutropenia and low IgG drove risk, early steroids did not.
IgG monitoring and timely IVIG remain key!
doi.org/10.1182/bloodadvance…
11
53
4,532
Simon Stern retweeted

Mar 5
Just in: Good news for the myeloma field.
FDA approves teclistamab plus daratumumab (Tec-Dara) combination for myeloma for patients who have had at least one prior line of therapy.
Note: Always use Tec-Dara with monthly IVIG. It’s not optional.
That was fast! And this is unprecedented curve is why.

7
89
299
26,352

Simon Stern retweeted

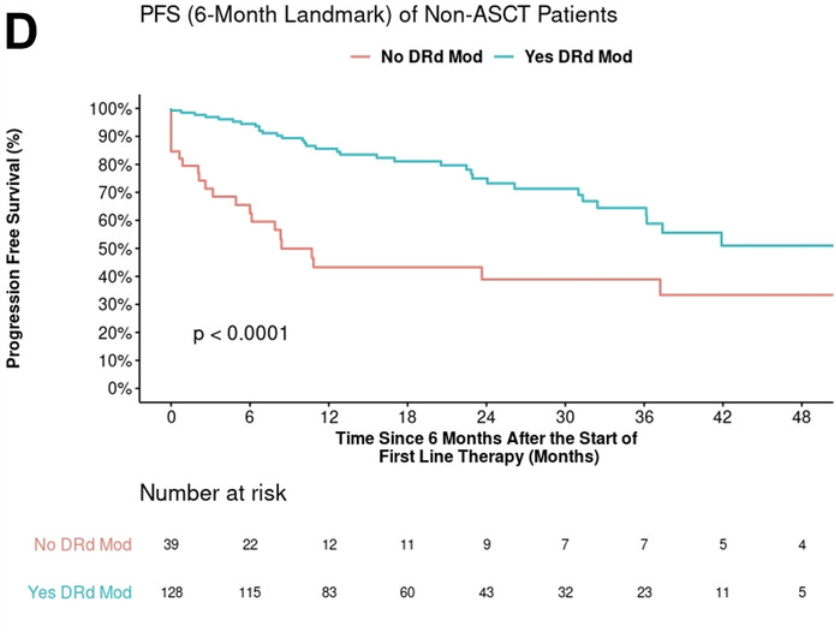
Picture worth a thousand words!
@AjHematology by Mayo myeloma: RW Dara-Rd in #MMsm
1️⃣ 2/3 pts required dose ⬇️, typically #downwithdex or #downwithlen
2️⃣ Landmarked PFS unequivocally better if so
My takeaway: Duration of Dara-Rd --> Dara(±R) more important than exact dose!
2
6
25
2,089