
Mom of 2 college students looking for internships and jobs now! Also, researching treatments for Long-Covid, POTs, and longevity.
Joined July 2018
- Tweets 1,333
- Following 499
- Followers 164
- Likes 7,203
15 Photos and videos






CollegeBoundMama retweeted

Apr 19
"Heart disease runs in my family."
Four words I heard my whole life. Four words millions of people say.
They're describing their genes without knowing it.
I ignored those words until they nearly killed me at 52.
Then I did what nobody had ever told me to do. I tested my genes.
What I found changed everything. For me and for my son David. 🧵
3
5
22
15,416
CollegeBoundMama retweeted

Why we STILL have no FDA-approved therapies for #POTS and #dysautonomia:
❓ Where did we go wrong???
Here is MY take on WHY:
🧠 Labeling it as "complex, multi-systemic, multi-factorial." All true, but in reality -- it creates ambiguity, lack of focus, broad range of phenotypes and etiologies ➡️ Mechanistically, where do you even begin to develop targeted therapies?!
🧠 Trying to add POTS to "autonomic disorders," most of which are RARE by definition -- it creates a huge shortage of physicians who specialize in autonomic disorders ➡️ You want many doctors to diagnose and treat it, not a few, to increase and diversify therapeutic options.
🧠 Excluding POTS from neurologic education: this is a major mistake because the autonomic NERVOUS system is involved ➡️ When most neurologists are not well-versed in diagnosing and treating POTS, patients lose: neurology is not only about migraine or neuropathy!
❓ How to fix this???
Here is MY take on HOW:
🧠 Refocus POTS and dysautonomia on one mechanism instead of "it's everything" ➡️ Consider "neuroimmune" angle and try existing therapies that we have for other neuroimmune conditions (neurologic Sjogren's, lupus, MS)
🧠 Make tilt table tests, QSARTs and skin biopsies accessible and affordable for every community practice/hospital/clinic ➡️ Better diagnostic capabilities and precision diagnosis
🧠 Embrace POTS/dysautonomia as part of neurology residency curriculum - not just autonomic fellowship! ➡️ All neurologists would be required to diagnose and treat POTS in the same way that all neurologists are required to be able to diagnose and treat Parkinson's, diabetic neuropathy, migraine, etc.
🧠 Fund POTS research led by researchers with diverse and multidisciplinary backgrounds ➡️ When research money is going only to the few scientists and academic centers, you lose diversity of ideas and experiences, resulting in "more of the same" research studies.
🧠 Engage with Pharma more and better! ➡️ Learn from our headache medicine colleagues and what they have achieved in partnership with Pharma. Migraine and other headaches have no biomarkers and negative MRI of the brain, but there are over 30 FDA-approved medications and devices for treatment of migraine!
ALT https://www.dovepress.com/postural-orthostatic-tachycardia-syndrome-myalgic-encephalomyelitischr-peer-reviewed-fulltext-article-ITT
8
29
166
6,973
CollegeBoundMama retweeted

Useful Victorian phrases for saying no to things. #TuesdayMotivation

104
1,982
7,768
223,203
CollegeBoundMama retweeted
We wrote a paper on what not to say to patients with complex chronic illness.
mdpi.com/1660-4601/22/2/275
2
14
73
5,878
CollegeBoundMama retweeted
🧠 Love that list by Dr. @adamcifu. Here is my "Please do not do that research" list related to #Dysautonomia: 🗒️
1. Please no studies on exercise and rehab programs in patients with #POTS, #MECFS or #LongCOVID. We get it... exercise is good for you and helps a good subset of patients, but self-selection and other biases in these studies preclude sweeping generalizations. Some patients cannot exercise, period.
2. Please no studies on psychological correlates, personality traits, anxiety, depression or childhood trauma in patients with #Dysautonomia, #MECFS and #LongCOVID. If you don't have at least one control group consisting of patients with MS or lupus, then your findings are useless.
3. Don't waste your time to study psychotherapy in patients with #POTS, #MECFS and #LongCOVID. It'll only work on patients with significant anxiety, poor coping mechanisms and inadequate social support. It won't work for the underlying pathophysiology of these disorders.
4. We get it: salt and compression are good for you if you have #Dysautonomia so we can stop doing these studies, except one.... is long-term increased salt intake associated with a higher risk of autoimmune disorders in patients with #Dysautonomia? We don't have this study and need one to estimate the risk in a population already prone to autoimmune disorders.
5. I really could care less if breathwork, meditation, music therapy or acupuncture are beneficial in patients with #POTS, #MECFS or #LongCOVID. Those things are beneficial for many stressed and overworked individuals, regardless of health or disease. Waste of time and money....
6. Demographics, phenotypes, loss of smell and taste and other such things that have been studied ad nauseam in #LongCOVID do not need to be repeated in any cohorts from any country. Enough is enough.
7. As an editor and reviewer of many studies on POTS, some comparisons among groups are unnecessary and useless: I don't want to see outcome comparisons between POTS and VVS vs. POTS alone or POTS and EDS vs. POTS alone groups. The more disorders one has, the worse. We know!
8. No offense to my basic science colleagues: love and appreciate your work, but honestly, if you find that muscle sympathetic nerve activity in patients with POTS is higher than in healthy controls, thank you, but it helps nothing and no one.
9. Subjective vs. objective mismatch in patients with POTS/dysautonomia or Long COVID: don't want to hear about it. The autonomic function tests were not designed to assess patients with common autonomic disorders so yes, they will look amazing on the autonomic function tests, scoring 0-1 on CASS score, but they will be very sick and debilitated regardless, and no, it's not because they have anxiety, depression or deconditioning.
10. Finally... when you talk about VO2max as a marker of deconditioning, you're talking about research from decades ago. Reduced VO2max is not caused only by deconditioning: in our patients, it's most likely from mitochondrial and endothelial dysfunction, decreased organ perfusion and cellular metabolism problems.
Thank you for reading my list! Please do sensible, logical and clinically relevant research! 👩🔬🔬🧬
Feb 10

Grateful that Dr. @adamcifu is saying aloud what many of us are thinking about #ResearchWaste and perverse incentives.
We need Sensible Research.
sensible-med.com/p/please-do…
14
48
190
9,399
CollegeBoundMama retweeted
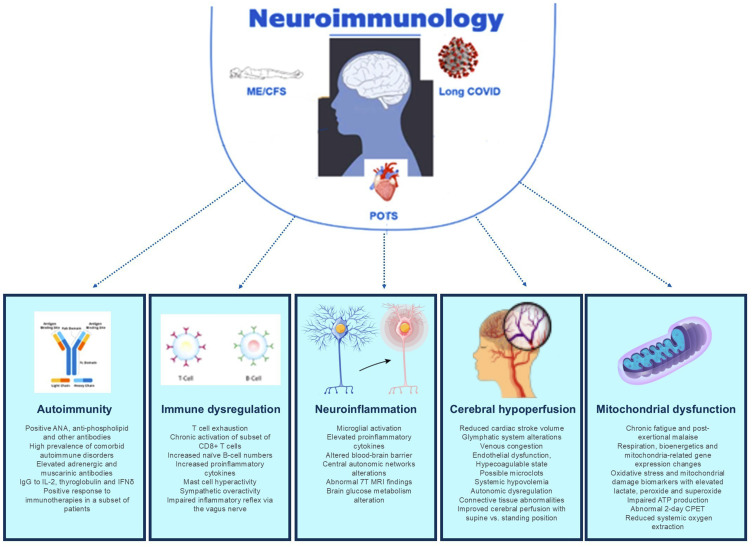
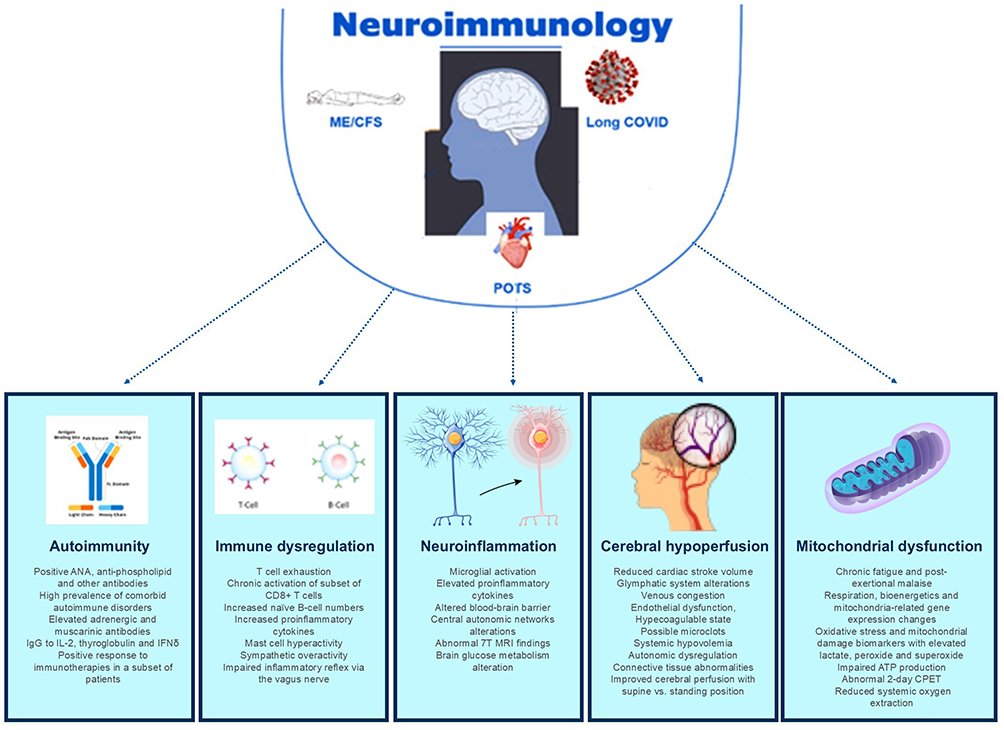
🚨 Hot off the press: my new paper that moves this field forward 🚀 and changes the narrative on what #POTS, #MECFS and #LongCOVID are... Neuroimmune Disorders!
🧠 The brain and the autonomic nervous system are involved in the immune system regulation.
🧠 There is evidence of autoimmunity, immune dysregulation, cerebral hypoperfusion, neuroinflammation and other mechanisms in all three disorders.
🧠 #Neuroimmunology is a field that should embrace these disorders: #MultipleSclerosis, the staple of neuroimmunology, used to be called hysterical paralysis before CT and MRI were invented. We're at the same crossroads with these disorders.
❌ These disorders are not "mysterious", "anxiety", "deconditioning," "functional neurologic" etc. etc.
‼️ Classifying these disorders as neuroimmune and including them as part of neuroimmunology training is critical.
🛌 #PatientCare and lives of millions of people living with these disabling conditions are at stake!
Thanks to my esteemed colleagues and co-authors, Dr. @TaylorDoherty8, immunologist from UC San Diego and Dr. Lawrence Steinman, neuroimmunologist from @StanfordMed, for their support!
Read open-access paper here: 👇
dovepress.com/postural-ortho…
38
259
757
30,785
CollegeBoundMama retweeted

Jan 19
30
60
239
23,111
CollegeBoundMama retweeted

29 Dec 2025
High-Class Social Intelligence:
1. Remembering names
2. Introducing people properly
3. Giving credit publicly
4. Correcting privately
5. Leaving conversations gracefully
6. Making others feel at ease
7. Asking thoughtful questions
8. Respecting boundaries
9. Thank-you notes that mean something
10. Never embarrassing others
121
1,476
11,752
494,181
CollegeBoundMama retweeted
Time and time again I see a lot of misconceptions about #POTS and #dysautonomia among physicians of all specialties. I'll repeat as many times as necessary:
‼️ POTS is not a psychiatric or psychological disorder
‼️ POTS is not a functional neurologic disorder or hysteria
‼️ POTS is not the same as anxiety or panic attacks
‼️ POTS is not due to past trauma or childhood adverse experience
‼️ POTS is not caused by deconditioning or laziness: elite athletes can develop POTS.
‼️ POTS is not the latest fad diagnosis: you see more of it because of #COVID, which can cause POTS as part of #LongCOVID.
‼️ POTS patients are no more difficult or whiny or anxious than any other patients with complex, disabling and multisystemic conditions.
‼️ Women with multiple sclerosis used to be labeled as hysterical, anxious and having past trauma: nobody says that about MS anymore so... use the same logic in POTS.
#BrainHealth #MedTwitter #NeuroTwitter
frontiersin.org/journals/neu…
18
116
362
13,050
CollegeBoundMama retweeted

31 Oct 2025
How to Heal from a Dysregulated Nervous System:
This is not your cliché list and this stuff works:
- 3x/week Epsom bath (2 cups magnesium sulfate, 104°F)
- Vagus Ear Pulls (finger in ear, tug down/back 30 sec/side)
- Coherence breathing everyday (Hand on heart)
- Left-right eye tracking (Comment CONCUSSION)
- 1 Nature Day/Week (No Phone, grounded, hydrate)
- Neurogenic tremoring (TRE floor sequence, 15 min, 3x/week)
- TRE Forward fold 3 mins/3 sets (Let legs shake)
- TRE Backward bend 3 mins/3 sets (Arms up, shake)
- Red light panel (15 min body, 660 850nm, 12" away, eyes closed)
- Seal the Gut (Comment GUT)
- VORTEX BREATHWORK (Comment VORTEX)
- Sour taste trigger (lemon wedge bite, 30 sec to activate parasympathetic)
- Big 6 Lymphatic drainage every AM
- Humming regularly (Long exhales)
- Somatic shaking (feet planted, soft knees, 60 sec bounce to tremor)
- Weighted blanket breath (15 lb, 10 min, belly rise only)
- Cold shower cycles (30 sec cold/90 sec hot x3, end cold)
- TWIM meditation (Comment SMILE)
- Sungazing (first 10 min sunrise, no glasses)
- Sauna vocal toning (20 min 160°F, sustained "voo" exhale)
I dare you to be dysregulated after doing this protocol for 4 weeks.
94
170
1,296
76,184
CollegeBoundMama retweeted

16 Oct 2025
Long Covid Is Real — And It’s Changing an Entire Generation
Hundreds of thousands of kids in America are struggling with an illness that many doctors and schools refuse to recognize.e
Feature: rollingstone.com/culture/cul…

259
3,481
7,642
1,667,758
CollegeBoundMama retweeted

25 Jul 2025
Find the beauty in the people and
places around you as well as
in you and watch it
all multiply!
🙏☀️🌷
You are enough.
Remember
that.
❤️
#WellnessJourney #selfcare #love #beauty #FridayFeeling

3
6
13
708
CollegeBoundMama retweeted

19 Apr 2025
"Why are US taxpayers funding Harvard?"
These grants aren't charity. They're highly competitive contracts where the US government determines Harvard is the best institution for conducting specific research, and then pays Harvard for services rendered to US taxpayers.
32
213
1,512
76,524
CollegeBoundMama retweeted

8 Mar 2025
Today is International Women’s Day. Thank you to all of the women in our lives making the world a better place.
#InternationalWomensDay #IWD2025
94
1,754
4,674
292,742

13 Feb 2025
RT @KJM_withaview: From a man named Jordan Levick. Incredible must read:
I am not a Swiftie, but I am a human being, a Dad AND, a Monstrous…
8,656
CollegeBoundMama retweeted

11 Jan 2025
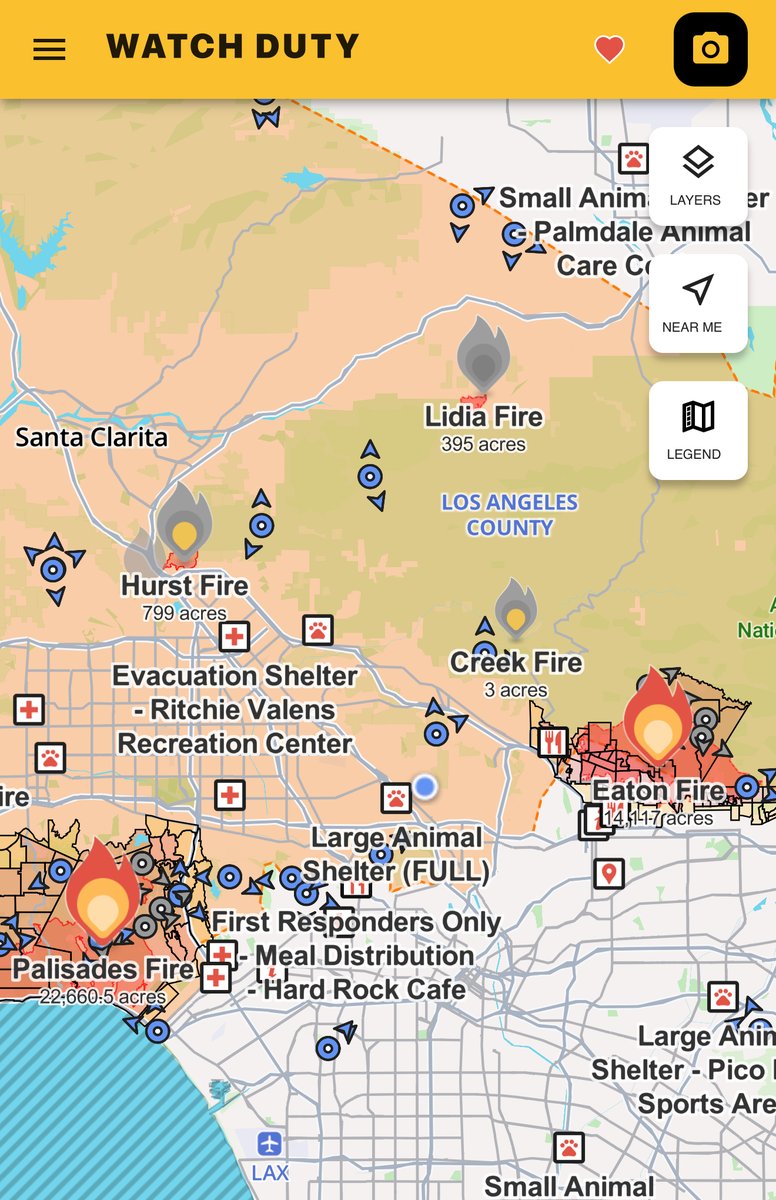
We talked to the cofounder of Watch Duty, which has become an essential app in LA for tracking the wildfires:
- It's a 501(c)(3) nonprofit largely supported by volunteers
- Has had 100% uptime (and no mistaken evac notices vs the local gov sending THREE accidentally)
- Over 1m downloads this week with plans to expand to more of the US/oversees
- “We view what we are doing as a public service.”
191
1,602
8,389
759,208
CollegeBoundMama retweeted

1 Jan 2025
Good morning
Happy New Year 🎉
Hopefully it will be a good one 🤞🏻
4
5
13
2,404
22 Dec 2024
Yes! And for those who aren’t getting it, time to explore media literacy and examine your unconscious bias #mysogyny #patriarchy #believewomen
#IStandWithBlake
22 Dec 2024

Every woman that has ever complained about misogyny and systemic unfairness that benefits those in power, and has been punished & shamed for talking about it, is finding the silencing strategy used against #BlakeLively very interesting - and very familiar - indeed
#patriarchy
322
CollegeBoundMama retweeted

26 Nov 2024
Gratitude.
A simple "thank you!"
regenerates your body,
opens your mind,
fills your heart with love,
expands your soul.
Focus on
deliberately, actively
and intensely finding
even the smallest thing
to appreciate.
Happy Thanksgiving! 🍁

38
183
507
41,658
CollegeBoundMama retweeted

25 Oct 2024
Our nervous system didn't evolve to handle constant stimulation.
However, today's world floods us with constant stimuli—causing chronic dysregulation.
To fix it, you need a nervous system reset.
And it starts with these 15 simple lifestyle changes: 🧵

266
3,492
18,240
4,565,094