
Desarrollador de videojuegos en desarrollo (también hagos videos de deportes de motor)
Joined October 2021
- Tweets 513
- Following 45
- Followers 23
- Likes 50,676
95 Photos and videos











Pinned Tweet

May 18
#IsleofManTT is back this week 🇮🇲, the best motorsport event in the world.
My first video about it has reached 800k views, check it out, you might become a fan of the sport! 🏍️
9 May 2025

Besides working on my game I've found time to make a cool video about the Isle of Man TT 🇮🇲 #IsleofManTT
youtu.be/gktZOJZGR6w?feature…
84
Ramon Hernandez retweeted

We see the tower of Jesus Christ illuminated for the first time!
The light show, starting from the base up to the illumination of the cross, culminated with a composition of lights guided by drones that traced the figure of Gaudí and the phrase “first love, then technique”.
860
8,019
44,426
3,975,957
Ramon Hernandez retweeted

Beyond brain fog: viral proteins as convergent drivers of neuroinflammation and proteinopathy
🚨“COVID-19 never really leaves your brain.”
New science review proposes SARSCoV2 viral proteins stay behind as long-lived toxins, triggering chronic neuroinflammation and planting the seeds of Alzheimer’s and Parkinson’s, even after mild infection.
This very interesting and eye-catching GERMAN review reframes post-viral neurological syndromes( L0ngC0vid) as driven by persistent viral proteins acting as long-term toxins ("protein-as-pathogen" model), not just the active infection!
➡️Core mechanisms:
- SARSCoV2 Spike and OTHER viral proteins activate glial TLR4/TLR2 receptors, triggering chronic neuroinflammatory cascades via NLRP3 inflammasome,
- They also disrupt autophagy, allowing toxic protein aggregates (tau, amyloid-beta, α-synuclein) to accumulate and seed neurodegeneration,
➡️SARSCoV2 specific evidence:
- Animal studies show Spike protein alone (without live virus) induces TLR4-mediated cognitive deficits, memory impairment, synaptic loss, and sustained neuroinflammation, recapitulating post-COVID syndrome,
- Spike binds α-synuclein, accelerating Parkinson-like clumps,
➡️Human data evidence:
- Millions experience "brain fog,"
- Post-COVID patients exhibit measurable brain damage: cortical thinning, hippocampal iron accumulation, and biomarkers of ongoing neuronal injury,
➡️Broader risks:
- Even mild infections leave lingering proteins that promote Alzheimer’s and Parkinson’s-like pathology via shared pathways,
- Same pathways seen in influenza, dengue, West Nile etc,
- Mild infection = no protection,
‼️So, according to this review, the “protein-as-pathogen” model makes it crystal clear: every new SARSCoV2 infection (even mild or asymptomatic) deposits more of these long-lived toxic viral proteins into the brain. They don’t fully clear. They accumulate.
Each reinfection reloads the TLR4/TLR2 → NLRP3 inflammasome trigger and further collapses autophagy, speeding up the tau/amyloid/α-synuclein proteinopathy and neurodegeneration.
SARS-CoV-2 does not just infect.
It weaponizes its own proteins as long-lived intracellular saboteurs.
Millions are probably already carrying this hidden payload.
This is not brain fog.
This is a silent, population-scale reprogramming of human brains toward dementia-like decline.
The long-term neurological cost will probably dwarf the acute pandemic itself!
#AvoidSars2 #AvoidReinfections
sciencedirect.com/science/ar…

15
293
679
23,209
Ramon Hernandez retweeted

Jun 1
Maria is paralysed from the chest down after her sidecar crash at the TT.
Please support this GoFundMe by donating or sharing – every bit of help makes a difference. gofund.me/14dce969b
11
42
92
9,761
Ramon Hernandez retweeted

May 31
⚠️‼️ I came across this news in Spain, and this discourse keeps doing enormous harm.
The post literally says:
“A study from Hospital del Mar reveals a worrying connection between childhood trauma and physical diseases in adult life. From headaches to diabetes, adverse childhood experiences could leave marks on our health. Early prevention has never been so crucial.”
“A study from Hospital del Mar details numerous physical diseases linked to childhood trauma.”
Not because they literally said that most organic diseases are caused by childhood trauma, but because in practice, many of the diseases they attribute to or reduce to trauma end up being organic diseases whose biomarkers have not yet been discovered, or whose proper medical workup was never even done.
And that is the real problem.
For years, many patients are first filtered through the lens of trauma, psychosomatic illness, or somatization, when in reality what they have is an organic disease that has simply not yet been diagnosed. I would even go further and say that this also happens with diseases we now understand well: before reaching the right specialist and before the appropriate tests are performed, many patients are treated as if the origin of their symptoms were psychological or trauma-related, simply because nobody has investigated their case properly.
That is not precision medicine.
That is a way of covering diagnostic ignorance with a psychological narrative.
The history of medicine shows this again and again: many diseases that in their early stages were treated as “nervous,” “hysterical,” or “psychosomatic” later turned out to be well-defined organic diseases. This happened with multiple autoimmune, neurological, and inflammatory diseases. And it is still happening today.
That is why this discourse is so dangerous. Because it not only delays the real diagnosis, but also blames the patient, isolates them, sends them into the wrong clinical pathways, and steals years of serious medical investigation from them.
Most of these patients do not need their illness to be explained through trauma.
They need the right tests, the right specialist, and serious investigation of their real biology instead of convenient theories being projected onto them.
Enough of turning the absence of known biomarkers into a psychological explanation.
What some people today call trauma or somatization too often ends up tomorrow having a name, a mechanism, and a biological marker.
7
32
93
5,573
Ramon Hernandez retweeted

Me at The Met Gala...

19
26
316
5,283
Ramon Hernandez retweeted
We are deeply saddened to learn that Alex Zanardi has passed away at the age of 59.
Zanardi was a two-time IndyCar (CART) champion for Chip Ganassi Racing and competed in F1 for Jordan, Minardi, Lotus and Williams across 41 grands prix.
The Bologna-born Italian’s motor sport career took a dramatic turn in 2001 after an IndyCar (Champ Car) crash which led to him having his legs amputated.
He staged a remarkable sporting comeback to become one of Italy’s most successful Paralympic athletes - winning four gold medals and two silver at the London 2012 and Rio 2016 Games.
Sadly in 2020, Zanardi was seriously injured when he was struck by a truck while competing in a para-cycling relay in Tuscany. He suffered serious head injuries and spent several years undergoing treatment.
“It is with deep sorrow that the family announces the passing of Alessandro Zanardi, which occurred suddenly yesterday evening, 1 May,” his family said in a statement.
“Alex passed away peacefully, surrounded by the love of his family and friends.
“The family would like to express their heartfelt thanks to all those who are showing their support at this time and asks that their grief and privacy be respected during this period of mourning.”
Motor Sport sends its deepest condolences to the family, friends and former colleagues of Alex.
5
53
299
7,866
Ramon Hernandez retweeted

LAUNCH ANNOUNCEMENT
Forbidden Solitaire is out now!
We are immensely proud to release this awesome game made by two veteran indie studios and we hope you really like it.
Steam: tinyurl.com/ywj43ptj
GOG: tinyurl.com/2s3sv45j
Itch: tinyurl.com/3k4bjt8m
Plz share, thx!
40
186
609
76,096
Ramon Hernandez retweeted

Apr 24
2
4
192
Ramon Hernandez retweeted

Apr 23
En estos libros he dejado mis pensamientos, mis historias, mis reflexiones y pasiones. Ojalá seguir escribiendo toda mi vida y disfrutando de tantos libros como sea posible, porque a través de ellos uno puede vivir infinitas vidas.

1
3
11
239
Ramon Hernandez retweeted

Apr 23
Could too much criticism damage #F1 ?
Mark Hughes and Matt Bishop say they will keep speaking out against the 'farcical' racing in the latest episode of the Motor Sport F1 Show
Plus: Why Michele Alboreto deserves more credit
go.motorsportmagazine.com/4m…
9
2
38
2,105
Ramon Hernandez retweeted

Apr 17
A detailed look at how @FumiHQ created @mousethegame. I couldn’t be more proud to partner with them on this video!
Watch here → youtu.be/a3PqKF3dyYg
3
2
337
Ramon Hernandez retweeted

Don't fear making a 2 week game. Those 8 months will be the most fulfilling 2 years of your life!
107
1,965
26,102
1,205,366
Ramon Hernandez retweeted

🚨MY GAME IS OUT NOW!!! OMG!!!🚨
I spent 4 weeks to make a fun party game about writing short stories based on 4 random words and rating each others stories afterwards... 😱
The Game is called "Cool Story, Bro!" and OUT NOW for 2,39€ 🥳😍 Pls Retweet 🙏
#Indiegame #Steam
28
54
260
51,165
Ramon Hernandez retweeted
Apr 9
A detailed look at how @nomadastudiobcn created #Gris and turned grief into gameplay.
Watch here → youtu.be/ajkOWlGGYgY

1
4
299
Ramon Hernandez retweeted

The philosopher of science, Karl Popper, has been one of the biggest influences on my thinking. You might not know who he is, but I guarantee his ideas have impacted your life in some way.
When it comes to COVID, two of his concepts seem especially relevant:
1. Falsifiability - it was Popper who wrote that in order for something to be considered science, it must be falsifiable. Unfortunately, most "Long COVID science" doesn't meet this bar.
I'm not talking about alternative medicine, but the actual studies masquerading as science.
Take, for example, the recent fluvoxamine trial, which claimed to test the hypothesis that the SSRI could benefit people with Long COVID by reducing inflammation in the nervous system. But the study was designed in such a way that nothing relevant was measured - regardless of the result, the study was never capable of falsifying the hypothesis it supposedly set out to test.
Or, take the lumbrokinase trial they're currently recruiting for. It supposedly tests the microclot hypothesis, yet the study doesn't measure anything having to do with microclots. No matter what happens, the microclot hypothesis cannot be disproven by the study. If the drug works, it could be placebo effect. If it doesn't work, maybe it was the wrong dose, the wrong group of patients or the wrong duration. Nothing will be falsified, and so nothing will change.
A recent vagus nerve stimulation trial stimulated a nerve for 4 weeks and measured whether patients felt less tired. They never verified the nerve was actually being stimulated. No heart rate variability was checked. No inflammatory markers of any kind were measured. How can you falsify "vagus nerve stimulation helps Long COVID" if you never confirmed the vagus nerve was even stimulated in the first place? The answer is you can't.
Popper would reject all of these studies. Not because the hypotheses are wrong (they may be right), but because the trials, as currently designed, aren't science. They're theater.
2. Now, here's where Popper's other idea comes in, and it connects directly to the political environment around Long COVID that determines which trials get funded: his notion of "Historicism" - the idea that history moves in a predictable pattern. Most people subscribe to some form of historicism, even if they can't articulate it. Liberals, for example, often think that, over the arc of time, history bends towards justice.
But the truth is that it doesn't. You don't have to study history for very long to see that this idea is pure nonsense. History is unpredictable. It moves in both directions: Iranian women had more rights in 1975 than they do today. Afghan girls attended school for twenty years until they couldn't. Weimar Germany was the most progressive democracy in Europe before it produced the Nazis. Roe was settled law for fifty years until it wasn't.
So when someone tells you "awareness is growing" and "research is progressing" and "eventually we'll find treatments" you should ask: who specifically is making that happen, by when, and what happens if they fail? Unless they can tell you that, then this is just historicism.
The idea of historicism also applies more generally to people's attitudes towards the pandemic, and what the future has in store for us all. Early on, we saw pandemic deniers practice a form of historicism - "Pandemics come and go. Humanity survives. This is just another flu." In other words, history moves in a pattern. The pattern is everything, and it is inevitable.
But I've seen other versions of this, as well. Take Iwasaki's "Lingering Shadow of Epidemics" paper, which documents how post-viral illnesses have followed every major pandemic for the last 100 years.
On the surface this seems helpful. But think about what the framing actually does. It recasts COVID and Long COVID from an urgent emergency that must be solved to just the latest permutation in a long, historical pattern. When it's a historical pattern, no one is responsible because this was always going to happen.
But if Popper was still alive, he would say this is nonsense. We don't know the future. History doesn't repeat in predictable ways. One pandemic is never exactly like the last.
Post-polio syndrome disabled people decades after they thought they had successfully recovered from their polio infection. Nobody saw it coming during the acute polio era. We still don't really understand it.
EBV sits in your body for 20 years before it triggers MS in some people. The latency period spans a full generation.
Think about what we've done with COVID. We have infected billions of people, multiple times, with a neurotropic virus that crosses the blood-brain barrier, causes vascular damage, and persists in tissue. We have six years of data. Anyone who tells you they know what this looks like 20 years from now is lying to you. There is no "shadow" of this pandemic - this pandemic is still ongoing.
20 years from now, maybe nothing will happen. Or maybe large numbers of people will develop serious neurological diseases. We have no idea, and we're not even trying to stop it.
The future is open. People are making choices right now about funding, research priorities, and accountability that will determine whether millions of people get treatments or get abandoned.
Those choices are, and have been made, by specific people with names. Not by history, patterns, or "lingering shadows."
Stop telling me this "isn't new". Instead, tell me who is going to fix it, by when, and what happens to them if they don't.
13
55
227
9,814

Ramon Hernandez retweeted

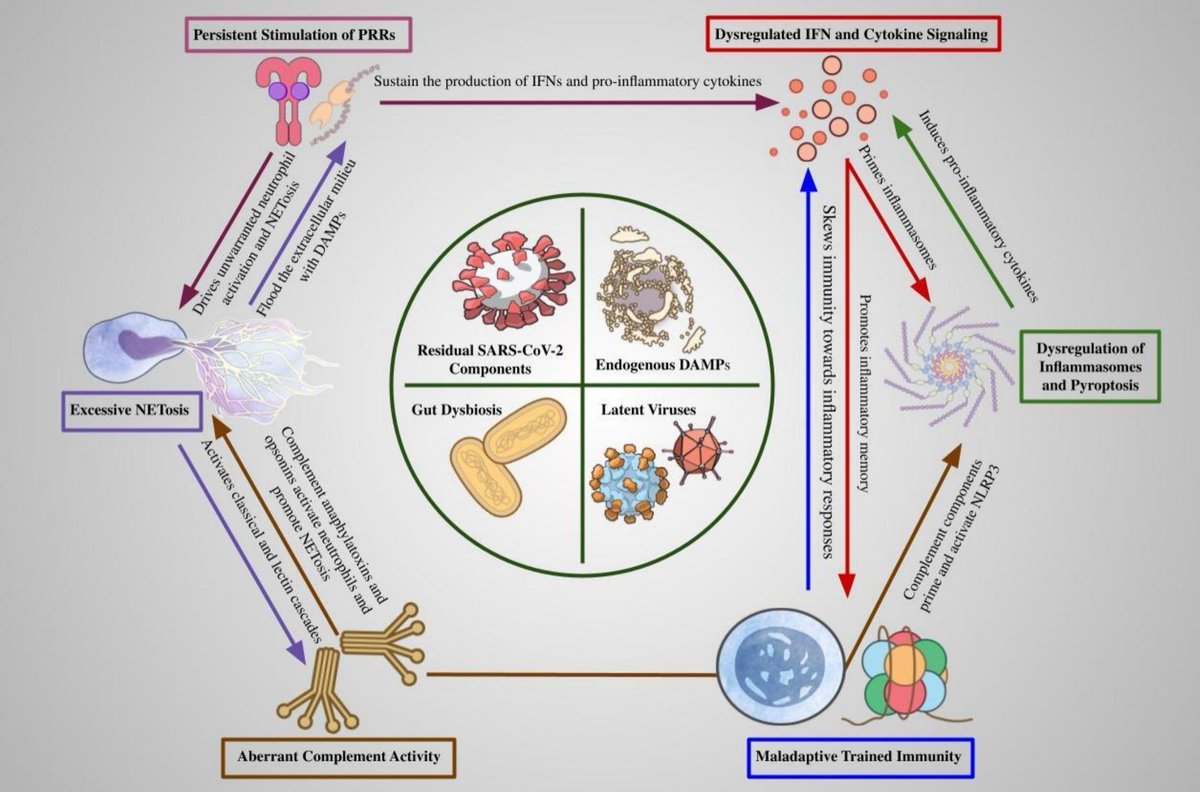
🔺🔻🔺"Persistent activation further promotes maladaptive trained immunity, reinforcing innate dysregulation and driving chronic cycles of inflammation and tissue injury".
@fitterhappierAJ
sciencedirect.com/science/ar…
1
21
50
9,220

Ramon Hernandez retweeted

Mar 15
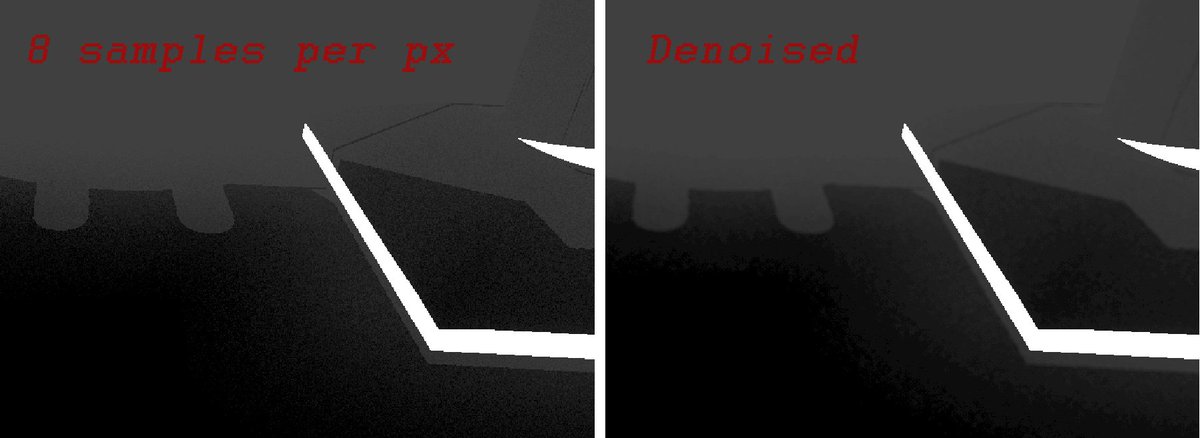
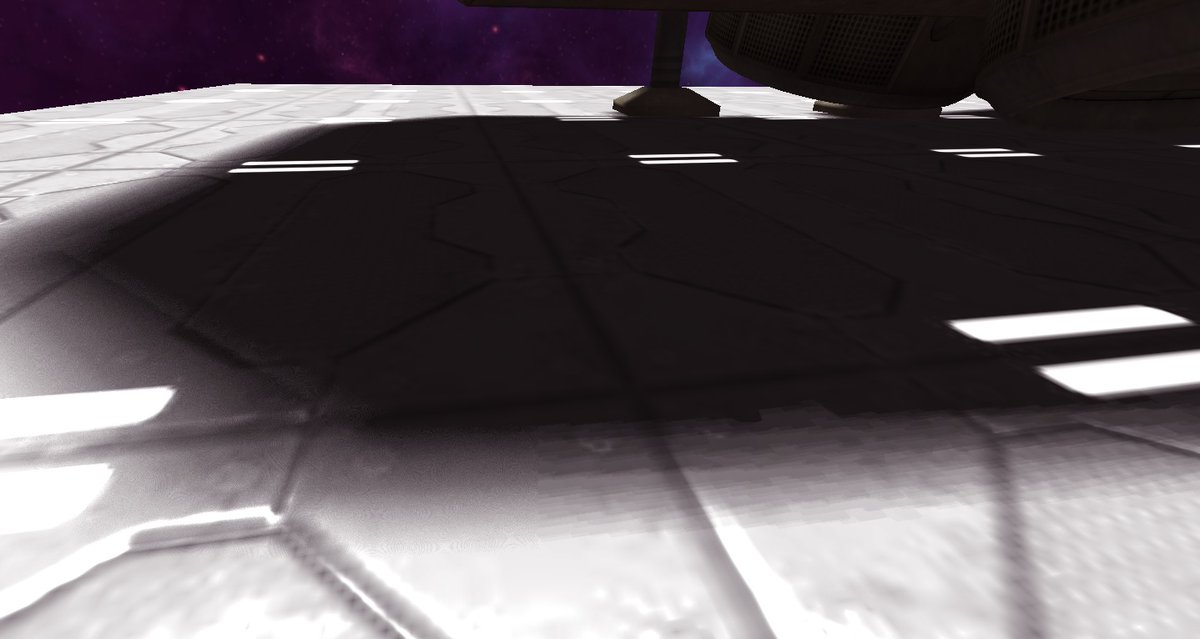
Physics-Based Simulation v1.0.3 is now live!
phys-sim-book.github.io
This release features @zzigakovacic's awesome coding examples on MPM viscoplastic flow, PBD cloth and elastic bodies, and PBF!
Huge thanks to all!
#Physics #Simulation #Animation #ComputerGraphics #MPM #PBD
1
44
248
13,590