
Vice-Dean: Research and Postgraduate Students, Faculty of Science, Stellenbosch Univ; Honorary prof: Univ of Liverpool Research: coagulation, inflammation
Joined April 2011
- Tweets 2,335
- Following 269
- Followers 29,081
- Likes 12,040
124 Photos and videos






Resia Pretorius retweeted

🔗 Paper
COVID-19 as a Modifier of Genetically Determined Coagulation Phenotype: Implications for Precision Risk Stratification After Infection
FYI/@resiapretorius
link.springer.com/article/10…
4
12
455
Resia Pretorius retweeted

Jun 17
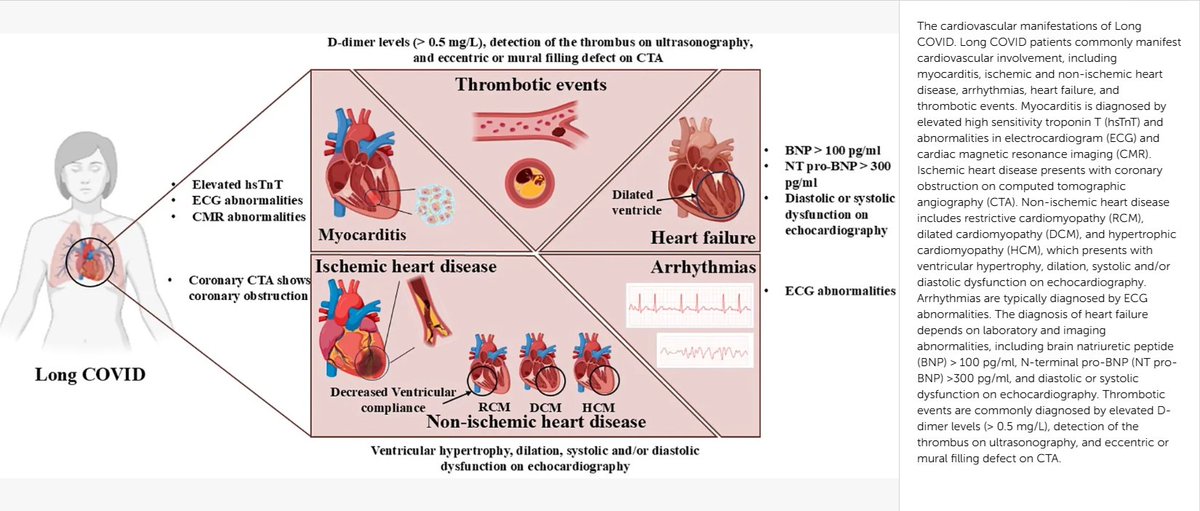
Cardiovascular sequelae of Long COVID: immune dysregulation inflammation as central drivers
🚨Your heart may still be under silent attack, even years after 'recovering' from COVID. #L0ngC0vid
➡️Another interesting Chinees review sadly bringing the same message!
➡️L0ngC0VID (symptoms >3 months post-SARS-CoV-2) features prominent CV complications including myocarditis, ischemic/non-ischemic heart disease, arrhythmias (including POTS), heart failure, and thrombosis, with elevated risks persisting 1 years in large cohorts (e.g, US Veterans Affairs data showing increased HRs for multiple outcomes).
➡️Central mechanisms:
- Ongoing innate immune activation (PRRs like TLRs/RIG-I, NETs, complement, NLRP3 inflammasome) causing endothelial injury, thrombo-inflammation, and adverse remodelling
- Plus, adaptive issues (T-cell exhaustion, subset imbalances, B-cell dysregulation).
➡️Evidence integrates clinical cohorts, autopsies, and mechanistic studies showing persistent inflammation even after viral clearance.
➡️Vaccination is explicitly linked to lower Long COVID risk and CV sequelae (e.g, incidence 9.5% vs 14.6% vaccinated vs unvaccinated, HR 0.59, overall Long COVID HR 0.85 post-vaccination, reduced referrals, and chronic symptoms).
➡️No discussion of reinfections or breakthrough infections
➡️The paper calls for biomarkers targeting these pathways, personalized surveillance for high-risk patients (especially those with comorbidities), and therapies against persistent inflammation.
‼️So, AGAIN, even “recovered” hearts stay under silent siege from never-ending immune fires, endothelial sabotage, micro-clots, and remodelling fuelled by persistent inflammation long after the virus is gone.
Vaccines measurably cut the damage, yet this brand-new review is completely silent on what repeated infections might do to an already dysregulated system.
If one infection can leave lasting CV scars via immune chaos, what happens with reinfections? Urgent studies on cumulative hits are needed before more hearts pay the hidden ugly price!
MEANWHILE ONE ADVICE :
#AvoidSars2 #AvoidReinfections
#L0ngC0VID #HeartHealth #YouOnlyHaveOneHeart
frontiersin.org/journals/imm…
3
98
222
3,694
Resia Pretorius retweeted
Beyond brain fog: viral proteins as convergent drivers of neuroinflammation and proteinopathy
🚨“COVID-19 never really leaves your brain.”
New science review proposes SARSCoV2 viral proteins stay behind as long-lived toxins, triggering chronic neuroinflammation and planting the seeds of Alzheimer’s and Parkinson’s, even after mild infection.
This very interesting and eye-catching GERMAN review reframes post-viral neurological syndromes( L0ngC0vid) as driven by persistent viral proteins acting as long-term toxins ("protein-as-pathogen" model), not just the active infection!
➡️Core mechanisms:
- SARSCoV2 Spike and OTHER viral proteins activate glial TLR4/TLR2 receptors, triggering chronic neuroinflammatory cascades via NLRP3 inflammasome,
- They also disrupt autophagy, allowing toxic protein aggregates (tau, amyloid-beta, α-synuclein) to accumulate and seed neurodegeneration,
➡️SARSCoV2 specific evidence:
- Animal studies show Spike protein alone (without live virus) induces TLR4-mediated cognitive deficits, memory impairment, synaptic loss, and sustained neuroinflammation, recapitulating post-COVID syndrome,
- Spike binds α-synuclein, accelerating Parkinson-like clumps,
➡️Human data evidence:
- Millions experience "brain fog,"
- Post-COVID patients exhibit measurable brain damage: cortical thinning, hippocampal iron accumulation, and biomarkers of ongoing neuronal injury,
➡️Broader risks:
- Even mild infections leave lingering proteins that promote Alzheimer’s and Parkinson’s-like pathology via shared pathways,
- Same pathways seen in influenza, dengue, West Nile etc,
- Mild infection = no protection,
‼️So, according to this review, the “protein-as-pathogen” model makes it crystal clear: every new SARSCoV2 infection (even mild or asymptomatic) deposits more of these long-lived toxic viral proteins into the brain. They don’t fully clear. They accumulate.
Each reinfection reloads the TLR4/TLR2 → NLRP3 inflammasome trigger and further collapses autophagy, speeding up the tau/amyloid/α-synuclein proteinopathy and neurodegeneration.
SARS-CoV-2 does not just infect.
It weaponizes its own proteins as long-lived intracellular saboteurs.
Millions are probably already carrying this hidden payload.
This is not brain fog.
This is a silent, population-scale reprogramming of human brains toward dementia-like decline.
The long-term neurological cost will probably dwarf the acute pandemic itself!
#AvoidSars2 #AvoidReinfections
sciencedirect.com/science/ar…

15
295
681
23,456
Resia Pretorius retweeted

Jun 14

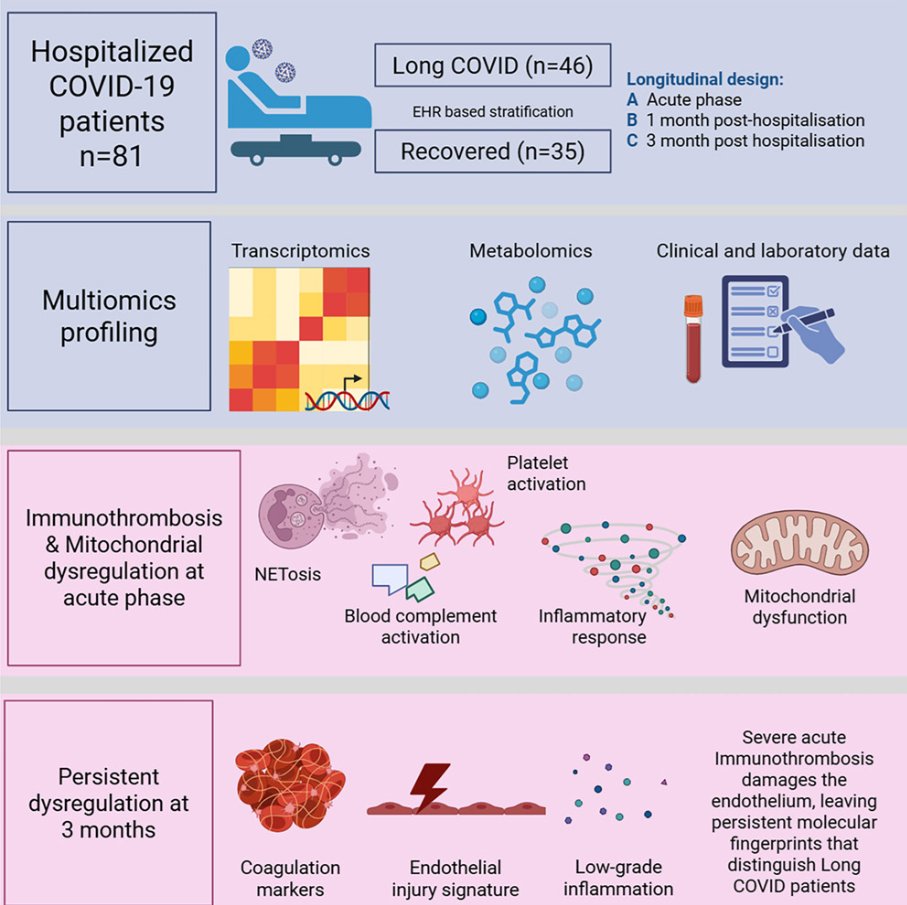
Immunothrombosis in hospitalized COVID-19 patients identified by multiomics profiling and linked to postacute complications
🚨INTERESTING New Latvian/Swedish multi-omics study shows immunothrombosis never fully switched off in longC0VID patients: 3 months after COVID hospitalization, your blood is still biologically “clot-ready.”
➡️What makes this study so important:
1. It reinforces that immunothrombosis (the interplay of complement, NETs, and platelets) is a central driver in severe acute COVID-19 and can persist in longC0VID,
2. It confirms persistent endothelial Dysfunction/Endotheliopathy in longC0VID patients, consistent with earlier studies on vascular damage and microclots,
3. It aligns with prior evidence of mitochondrial dysfunction during the acute phase, followed by partial repair mechanisms,
4. The persistent complement activation they observed fits with other recent multi-omics studies showing ongoing complement dysregulation in longC0VID.
➡️Study:
1. Prospective longitudinal multi-omics study of 81 hospitalized COVID-19 patients tracked whole-blood transcriptomics, urine metabolomics (46 analytes), and 13 kidney-injury biomarkers at acute admission, ~1 month, and ~3 months post-hospitalization,
2. Patients stratified by EHR into recovered (n=35) versus long COVID (n=46) groups based on a PASC diagnoses within 12 months,
3. None of the 81 hospitalized patients were vaccinated,
4. Acute phase dominated by interconnected immunothrombosis: strong upregulation of complement (C1QA/B/C), NETosis (PADI4, MPO), and platelet-activation genes (ITGA2B, ITGB3), plus mitochondrial dysfunction (HIF1A/EPAS1 up, OXPHOS down, Warburg-like glycolysis) and elevated renal injury markers (KIM-1 etc.),
5. Most immune, mitochondrial, and metabolomic changes largely normalized by 1–3 months, with rebound in mitophagy/heme genes (PINK1, OPA1, FECH) indicating repair,
6. At 3 months, longC0VID patients showed a distinct transcriptional signature of persistent endothelial activation (↑VWF, PROS1, ITGA2B/ITGB3), complement dysregulation (CFH), and low-grade vascular inflammation/platelet reactivity (CXCL5, ALOX12) that was absent in recovered individuals,
7. No significant late differences in urine metabolomics or kidney biomarkers between groups.
➡️They conclude with their Highlight-points:
• Severe COVID-19 induces immunothrombosis-associated molecular programs,
• Acute COVID-19 is associated with mitochondrial metabolic dysregulation,
• Urine profiling indicates gradual renal recovery after hospitalization,
• LongC0VID patients retain endothelial-associated activation signatures.
‼️So, even after apparent clinical recovery, immunothrombosis leaves a persistent molecular scar of endothelial activation and prothrombotic signalling in longC0VID patients at three months, revealing that the acute vascular battlefield never fully quiets in those who remain symptomatic.
→Three months post Covid-19, longC0VID patient’s blood is still biologically primed to clot!
#AvoidSars2 #AvoidReinfections
cell.com/iscience/fulltext/S…
4
13
804
Resia Pretorius retweeted

Jun 9
Here's my first post about that Wired story: virology.ws/2026/06/09/trial…
5
48
149
10,210
Resia Pretorius retweeted

58 organisations. 1,200 individuals
We're incredibly grateful to everyone who supported our open letter to the Royal College of Psychiatrists.
This coalition brings us together from across the community. A powerful reminder of what solidarity can achieve.
Update & full 💌👇🎙️

ALT Open Letter update graphic featuring a black-and-white photograph of two hands gently clasped in support. Large white text reads: “Open Letter Update: Solidarity, Engagement, and Next Steps.” Smaller text below states: “58 orgs & 1200 individuals sign regarding the framing of Long Covid in the Royal College of Psychiatrists 2026 International Congress.” The website “LONGCOVIDADVOCACY.SUBSTACK.COM” appears at the bottom. The image conveys solidarity, collective action, patient advocacy, Long Covid awareness, disability rights, and community engagement.
1
18
66
1,748
Resia Pretorius retweeted

dear all,
thank you, i’m sure you will love it.
let me try it for a few more patients and if it keeps confirming that amazing I will share it with you soon

guys i’m so excited that this model of clinical assessment is working ibcreadibly well for the first ppl with #longcovid #mecfs !
im confident this will become a standard of care preliminary assessment for these patients.
and as always I’ve made it free for all, while clinics charge you hundreds of dollars each time.
you can just select a little tip when you use it to cover my costs and keep it always free
you want me to share the link?
5
5
56
2,494
Resia Pretorius retweeted

Jun 5
I've been watching discussions this week and I have a few thoughts I'd like to share as a disease research expert who worked for years in precision medicine oncology, as well as a caregiver of a complex chronic illness patient.
1. The complex chronic illness community is one of the strongest and most vocal in all of medicine. This is a superpower, and we must use it to help move science forward.
2. Years of neglect have led our community down countless rabbit holes. As a result, we are often drawn to those who believe, when belief alone isn't enough. We now have an opportunity to channel that energy toward the strongest science.
3. We know many of the problems with healthcare in our space. It's time to focus on better scientific solutions. We have years of study under our belt. It needs to be put to use. Let's get it out of the labs and into the hands of patients.
4. To do this, we must create and demand a coordinated system built on scientific rigor that focuses on high-impact translation at scale and reflects the medical diversity of our population.
5. While these conditions are multisystemic, that does not mean they are untreatable. In fact, every diagnosis, every pathway, every communication across systems is a clue.
6. The field of neuroimmunology has tremendous potential to help our patient population. Again, let's focus on communication across systems.
7. AI has changed the game. We need full systems in place to maximize this technology. Data analytics, signal reduction, and more.
8. So what is our goal? Learn quickly from clinicians and scientists who have already identified the strongest hypotheses. Fund the experts who can prove or disprove these hypotheses and translate findings into patient care. Develop clear patient subtypes. Test treatments against those subtypes. Enlist support, both investment and philanthropic. Find the right treatment for the right patient.
9. This doesn't have to move slowly. In fact, there is so much information from other disease states that we can apply to ours. But we need systems-based approaches.
10. Expertise. Scientific rigor. Collaboration. Focus on the patient.
Again and again.
We've got work to do together. Stay tuned - more specifics to come.
5
9
58
2,320
Resia Pretorius retweeted

May 18
ABSTRACT DEADLINE EXTENDED!
Over the past weeks, we have received over 125 highly interesting submissions across biomedical, clinical and impact-focused research related to #LongCOVID and Post-Acute Infection Syndromes (#PAIS) for the ISLC-PAIS Conference 2026 (26-29 August) in Amsterdam.
At the same time, we have received multiple requests from researchers and interdisciplinary teams asking whether submissions could still be accepted due to ongoing analyses, internal review processes and timing constraints.
As an independent non-profit initiative focused on strengthening international collaboration and accelerating real-world impact, we want to make participation possible for as many relevant contributions as we can.
Because more knowledge leads to better outcomes, we have decided to extend the abstract submission deadline until:
📅 28 May 2026
We welcome submissions from researchers, clinicians, healthcare professionals and experts from related disciplines. Early-career researchers are especially encouraged to contribute.
Accepted abstracts will be considered for:
• oral presentations
• poster sessions
• panel discussions
If you are working on #LongCOVID, #MECFS or related #PAIS conditions, we warmly encourage you to submit your work and help shape the international conversation in Amsterdam.
👉 Abstract Submission - lnkd.in/e5gMriXZ
We are also very grateful to the members of our International Abstract Committee for helping shape the scientific quality and interdisciplinary scope of the conference, including #DannyAltmann | @DaniBeckman | @surf4children | @jencurtinmd | @Sunny_Rae1 | @AndrewEwing11 | @DrMark_Faghy | @drMHellemons | @DavidJoffe64 | @PutrinoLab | @satish_r_raj | @resiapretorius | #IleneRuhoy.
#MedicalResearch #ScientificConference #CallForAbstracts #ClinicalResearch #Immunology #ISLCPAIS2026

3
23
46
10,972
Resia Pretorius retweeted

Particularly damning data in Eckey, M., Li, P., Morrison, B., Bergquist, J., Davis, R. W. and Xiao, W. (2025) Patient-reported treatment outcomes in ME/CFS and long COVID. Proc Natl Acad Sci U S A. 122, e2426874122. doi.org/10.1073/pnas.2426874…
1
4
15
857
Resia Pretorius retweeted
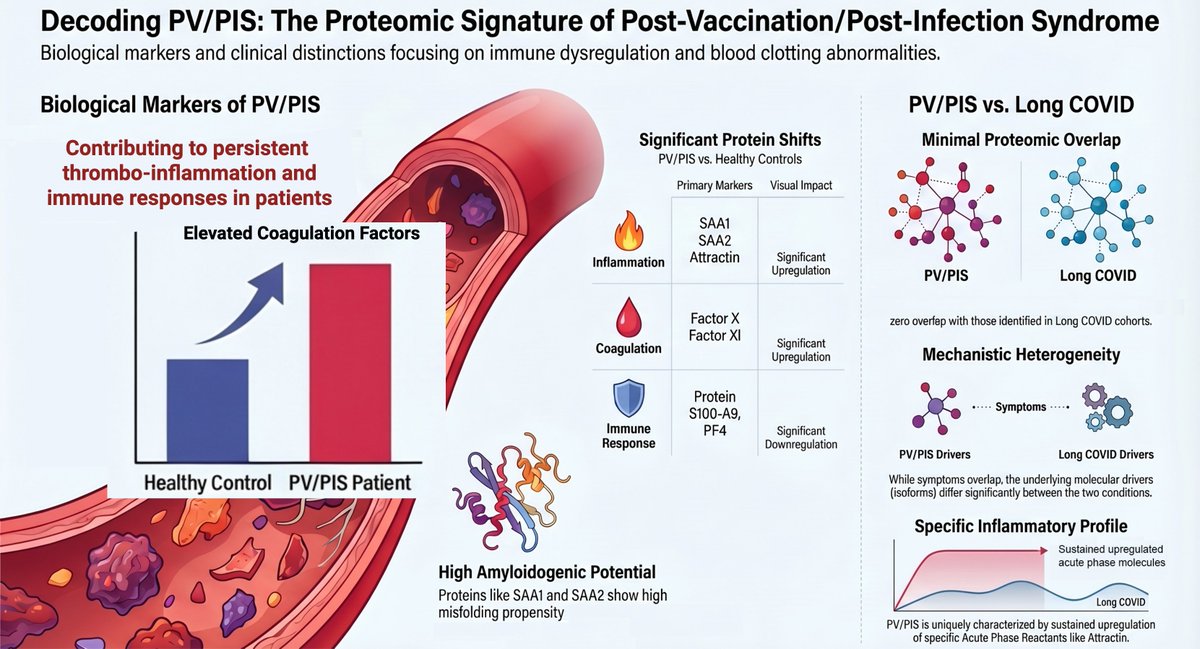
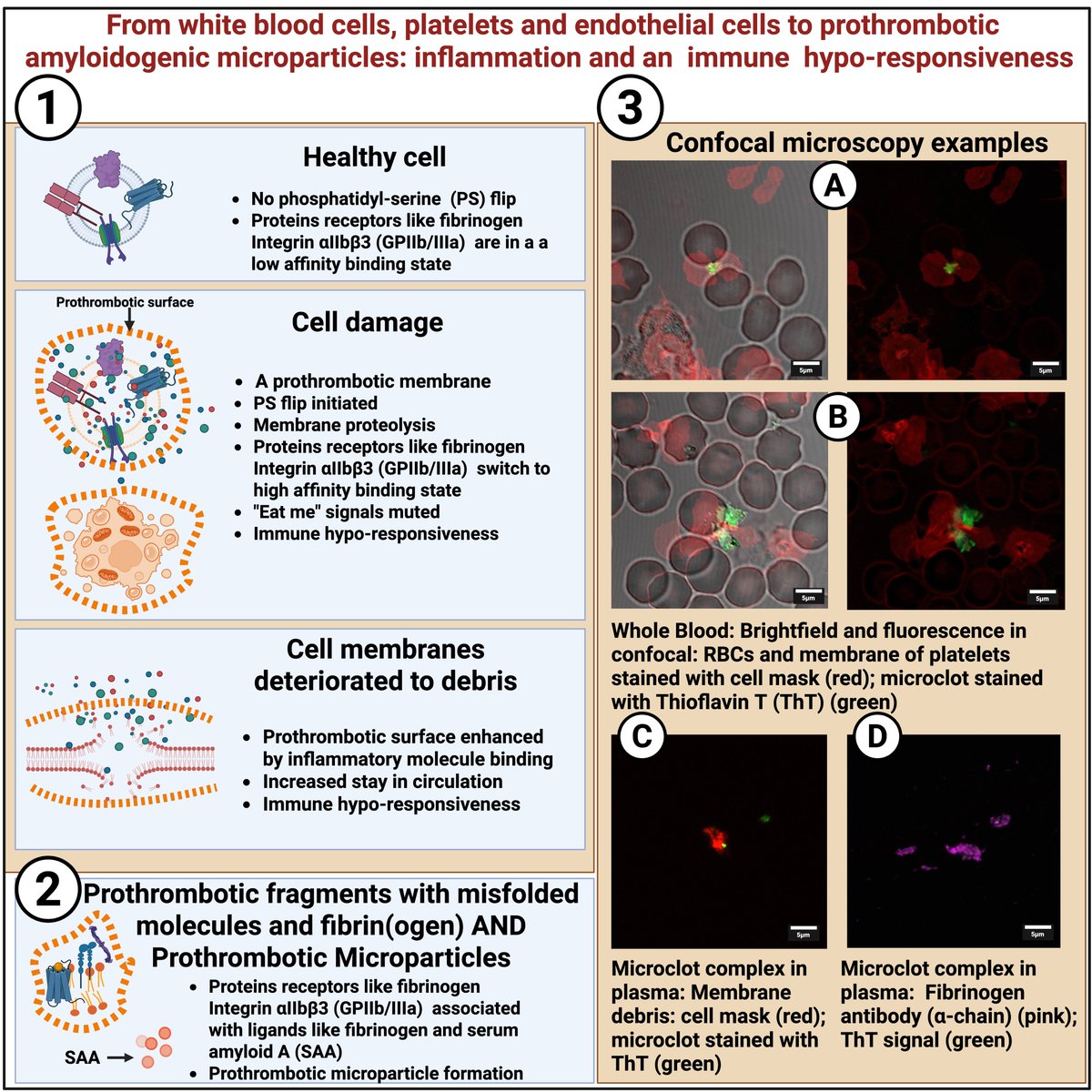
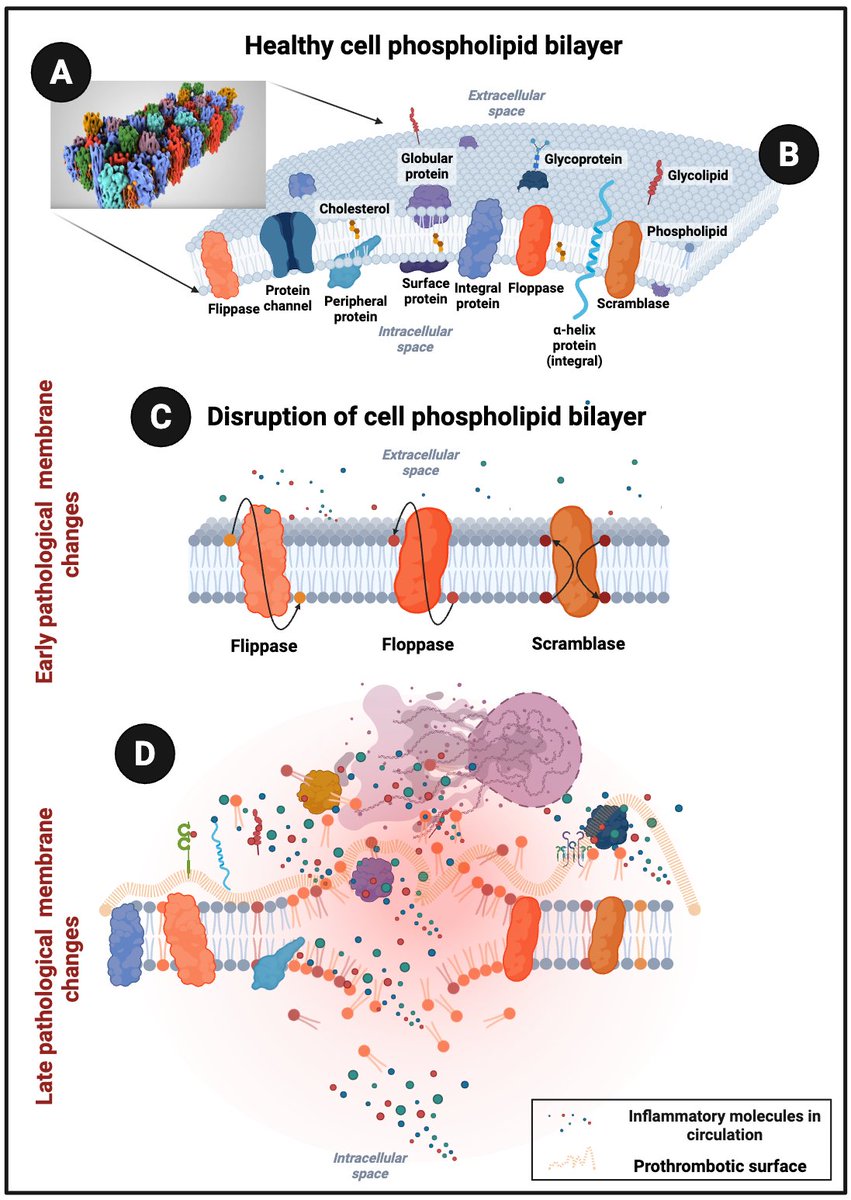
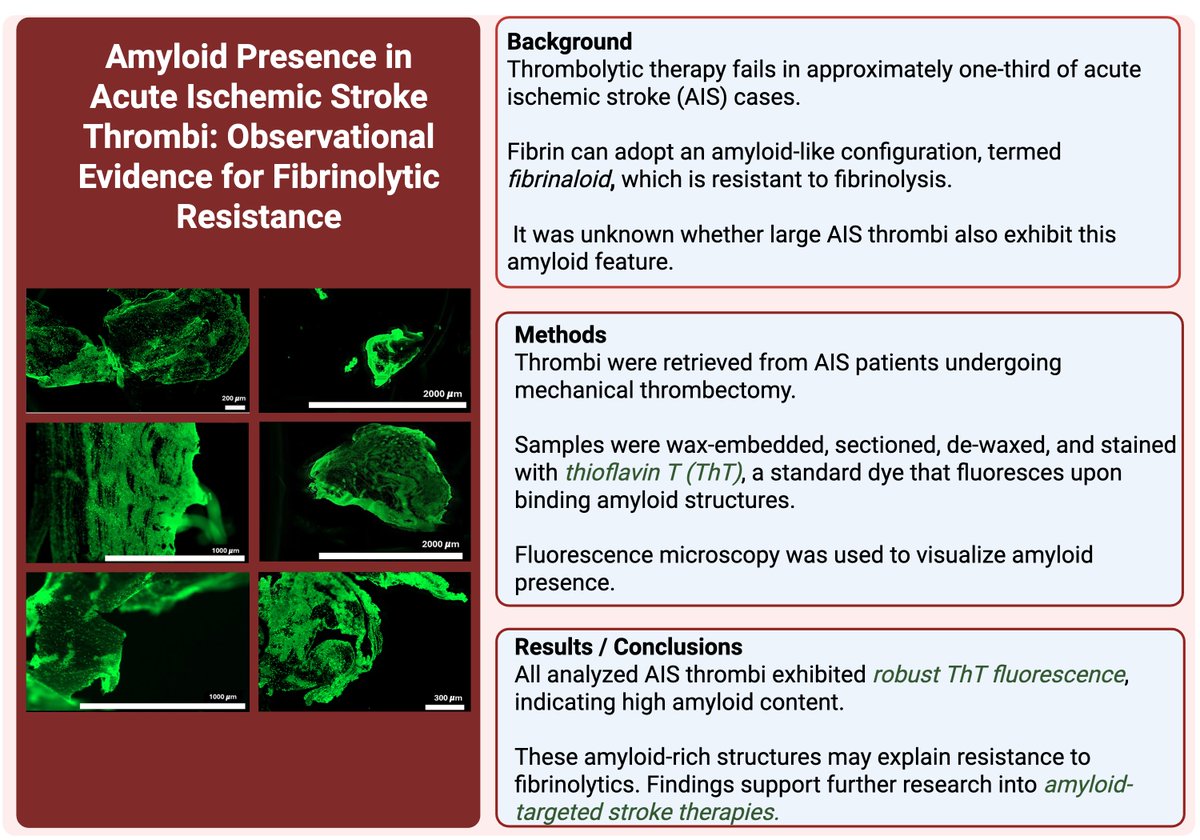
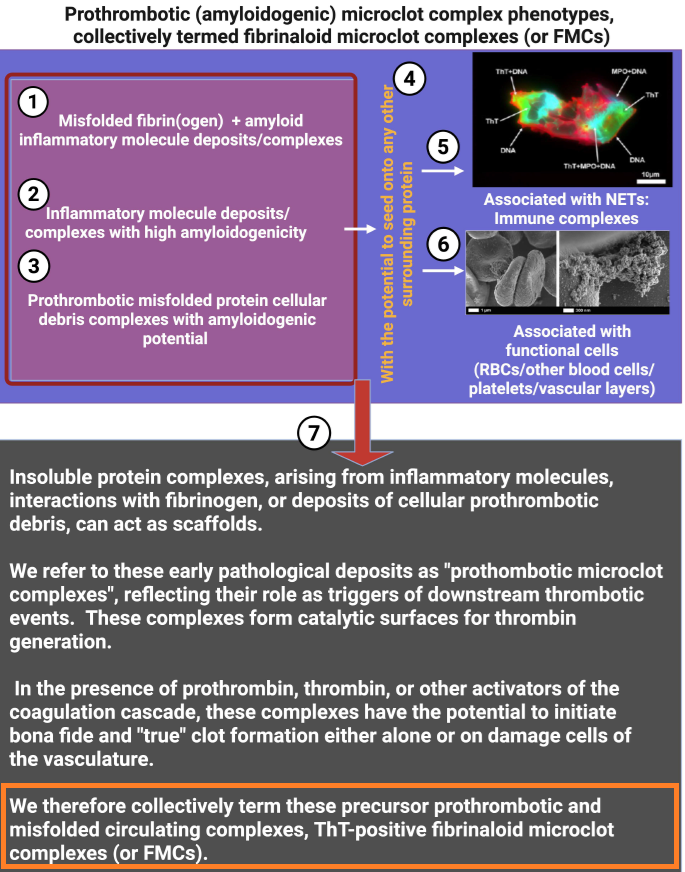
Surface cues shape procoagulant properties of amyloidogenic microclots
🚨YOUR ATTENTION: FMCs!
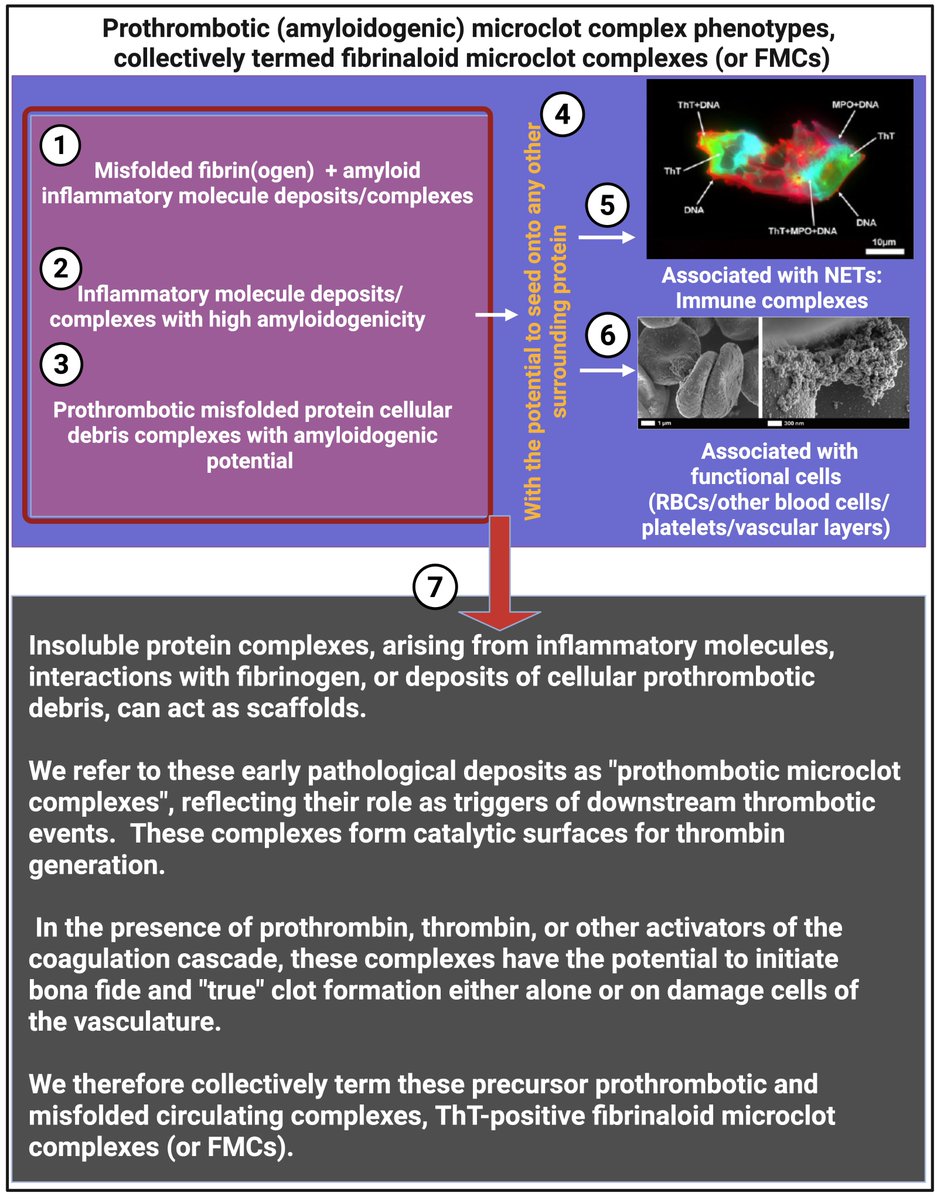
➡️This EVOLUTIONARY review synthesizes how cell-membrane surface changes during inflammation and cell death drive the formation of procoagulant, amyloidogenic microclots termed fibrinaloid microclot complexes (FMCs).
➡️FMCs are heterogeneous (1–200 μm), Thioflavin T (ThT)-positive complexes of fibrinogen, serum amyloid A (SAA), von Willebrand factor, neutrophil extracellular traps (NETs), and cellular debris/microparticles.
➡️The exceptional article introduces FMCs as a unifying conceptual framework that elegantly integrates membrane biophysics, protein misfolding, and coagulation, previously viewed in isolation, into a single membrane-centric model of thrombo-inflammation. Science, step by step!
➡️Its novelty lies in distinguishing these amyloidogenic, fibrinolysis-resistant complexes from both microparticles and canonical clots, while providing mechanistic evidence (PS exposure, SAA/fibrinogen cross-seeding, ThT positivity) for their role across inflammatory and post-infectious diseases.
➡️🤔By positioning FMCs as both pathological drivers and potential biomarkers/therapeutic targets (e.g, via anti-misfolding or NET-clearing strategies), the work offers a transformative lens for understanding and treating hypercoagulability in Long COVID and related syndromes, with broad implications for vascular medicine.
‼️In conclusion, this exceptional review offers a simple new way to understand how damaged cell surfaces during inflammation create tough, sticky microclots that clog blood vessels and drive long-lasting problems like those seen in Long COVID, opening the door to better tests and treatments that could help millions.
GREAT WORK, Thank you @resiapretorius et.al and your additional explanation fig’s are really excellent!
nature.com/articles/s41419-0…
32
71
2,313

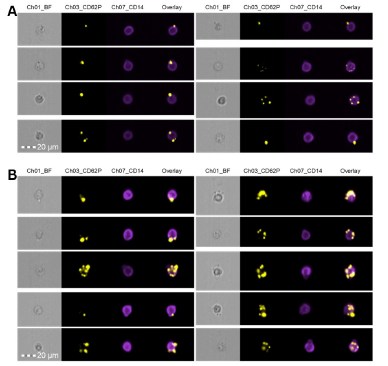
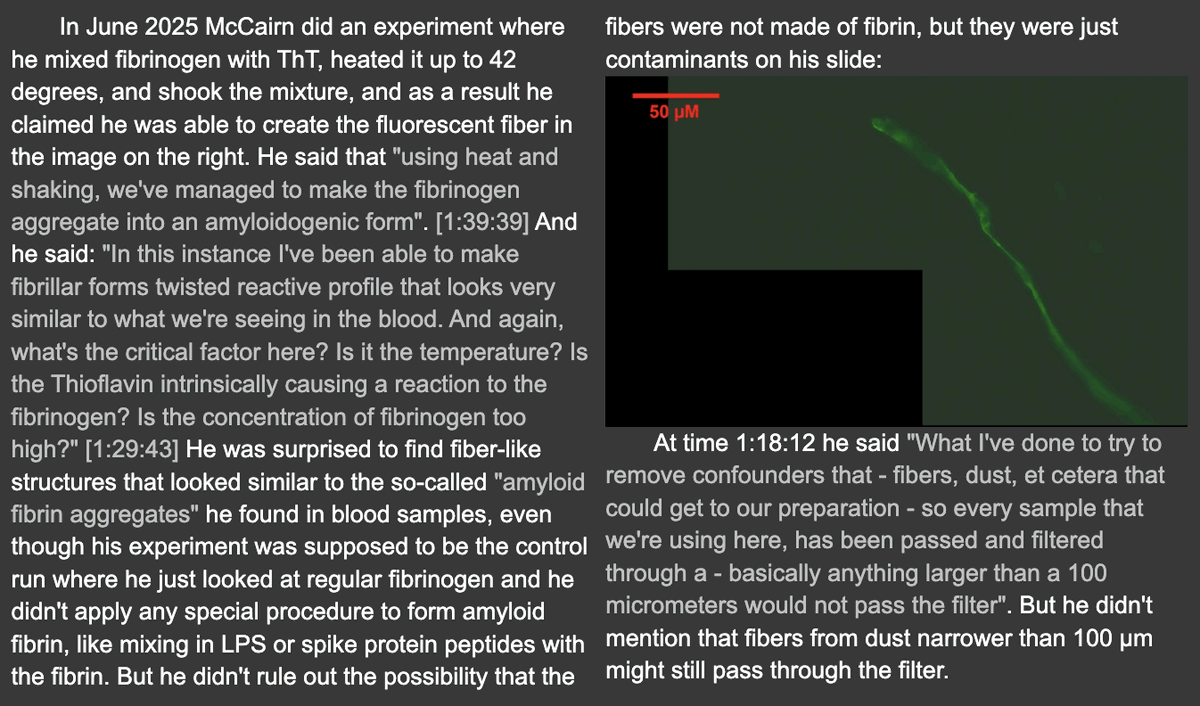
We and others looking for fibrinaloid microclot complexes, always do analysis on fresh blood plasma samples or plasma spun and stored at -80. We do not support dried sample analysis and any shipment at room temp. One must also be careful, as tissue paper fibers can show autofluorescence. However, we cannot comment on this exact photo.
Jun 3

Have you ever found one of these fibers that look like textile fibers but that have been stained by fibrinogen antibodies? (sars2.net/clot3.html#Further…) McCairn claims this string-like fiber somehow formed spontaneously when he simply mixed fibrinogen with ThT and shook the mixture:
5
16
1,636
Resia Pretorius retweeted
May 30
This week my 90-year-old mother was in the hospital being treated for a serious infection.
It made me think about how long and well she's lived. Her life has not been without hardship, nor without health challenges.
But each time she faced a medical obstacle, there was an answer. And she healed.
This week was the same, thankfully.
That is a blessing. It is also a reflection of what science can make possible for so many people: restored health.
It's all I work for. For my child. For the millions of people living with Long COVID, ME/CFS, POTS, and related conditions. For every family searching for answers: Real treatments. Real solutions.
#Research
1
6
50
1,369
Resia Pretorius retweeted
exactly why I think trials will fail
3
17
1,945
Resia Pretorius retweeted
Jun 1
Is there anything @CortDoesScience won't do for patients and research? A PhD who has devoted her work to deepening the understanding of complex chronic disorders. She's also running 50 miles to support @CODA_research research! So inspiring!!

We are thrilled to recognize @CortDoesScience for joining the CODA 50 Challenge and committing to run 50 miles in support of funding research for patients living with complex disorders.
As a scientist and patient living with complex chronic illness, Cortney brings an extraordinary perspective to this mission. She understands both the urgent need for answers and the importance of rigorous research designed to create meaningful impact.
We're incredibly grateful for her passion, leadership, and commitment to accelerating answers for patients.
Donate to support Cortney’s CODA 50 Challenge:
givebutter.com/CODA50/cortdo…
5
32
2,427
Resia Pretorius retweeted
May 24
Another powerful, heartbreaking piece on the destruction of lives caused by complex chronic disorders.
400 million people suffering. $1 trillion in financial cost. Long COVID has brought renewed attention to the human suffering caused by multisystem diseases that have devastated patients for decades.
We now move beyond proving the problem to focus on the solution.
Cancer research shows the world what becomes possible when science responds with urgency.
Systems now exist that address the specific needs of cancer as a whole, individual cancers and then patients within each type of cancer: cancer genome sequencing, sophisticated imaging, massive, well-constructed longitudinal datasets, collaboration across best-in-class science, and investment at both philanthropic and societal scale. That has led to effective targeted treatments that extend and save lives.
CODA brings the same level of urgency, a full scientific model and systems-based thinking to complex chronic illness.
For while we learn from other diseases. Complex disorders require their own disease research model.
Multisystem disease requires multisystem research.
That means integrating and investing in best-in-class science, clinical data, AI technology, deep phenotyping, sophisticated testing and translational focus into a coordinated model designed around the complexity of these patients and the biology driving their illness.
Follow @CODA_research.
blog.brittanijamesmd.com/p/l…
3
68
204
6,810
Resia Pretorius retweeted
If folk are interested, I am giving a @BiochemSoc talk on our work with @resiapretorius on Fibrinaloid Microclot Complexes in Long Covid and ME/CFS on June 17 at 2pm. Registration needed but free register.gotowebinar.com/reg… #TeamClots #pwLC #pwME
4
26
76
1,820
Resia Pretorius retweeted

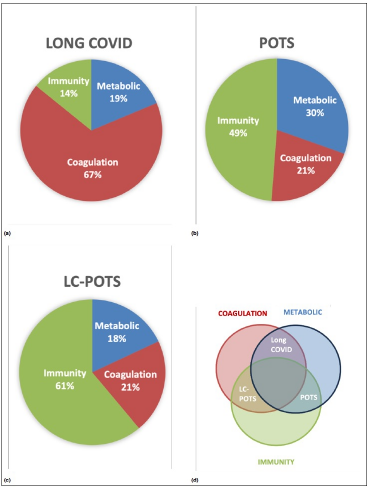
Whether you’re navigating life with a chronic illness like #POTS or simply supporting someone who is, the desire to be seen and understood is universal.
Take a moment today to truly listen to someone’s story. It makes all the difference.
#awareness #chronicillness #invisible

1
3
12
608
Resia Pretorius retweeted

May 15
Sticky Nets and Damaged Blood Vessels: A Long COVID Subset is Born? #longCOVID healthrising.org/blog/2026/0…
4
19
66
2,787
Resia Pretorius retweeted

This isn't a new theory just being put out there in this paper:
@resiapretorius @dbkell and @Sunny_Rae1 have been explaining this to WHO & medical community since 2022/3
The microclots fingerprint has been seen in their work and @KraterMartin's for years...
Listen to Prof Klaus Wirth talk to Gez Medinger about the mitochondrial damage leading in from the endothelial damage ➡️ microclots ➡️
microvascular damage ➡️ muscle & organ damage ➡️ calcium and magnesium overload in muscle cells ➡️ mitochondrial damage ➡️ PEM loops each PEM causing further mitochondrial damage..
They know the mechanism
Blood clots causing microvascular damage causing nerve damage causing autonomic dysfunction POTS
We need something that stops the endothelial damage and microclots formation that prevents organ damage and muscle damage and mitochondrial damage and nerve damage!
6
14
775