
T, B, & NK cells and Stem cell scientist for 50 yrs , Commercialized CD4/IL-2r, CD34 Mabs at BDMC &ABI TaqMan mRNA Gene Expression during human genome project.
Joined September 2010
- Tweets 23,964
- Following 839
- Followers 1,020
- Likes 42,843
70 Photos and videos

Pinned Tweet

1 Nov 2020
A couple of California stem cells supporters..... Colby Leis my grandson making a statement YESon14.com with Grandpa
14
21
91
Andy Blidy retweeted

I broke down the full science in this week's Substack — what the peer-reviewed evidence actually says, who benefits most, and the dosing questions researchers are still working through.
Link in bio. #BrainHealth #Neurodegeneration #Creatine
1
2
2
171
Andy Blidy retweeted

6
32
658
Andy Blidy retweeted

#DCVax is a #paradigmshift in #cancer from $NWBO for all #solid tumor. It is #autologous meaning ...
#moral - no questionably sourced cells
#safe - no deadly side-effects
#effective - customized just for you
#REPEATABLE - do it again overcoming resistance from mutations

$NWBO #DCVaxForBraelyn @SecKennedy @MHRAgovuk #GBM @AlMusella @glioblastf @glioblastomaorg @GBCancerStudy #DCVax x.com/HollensbeAmanda/status…
2
26
400
Andy Blidy retweeted
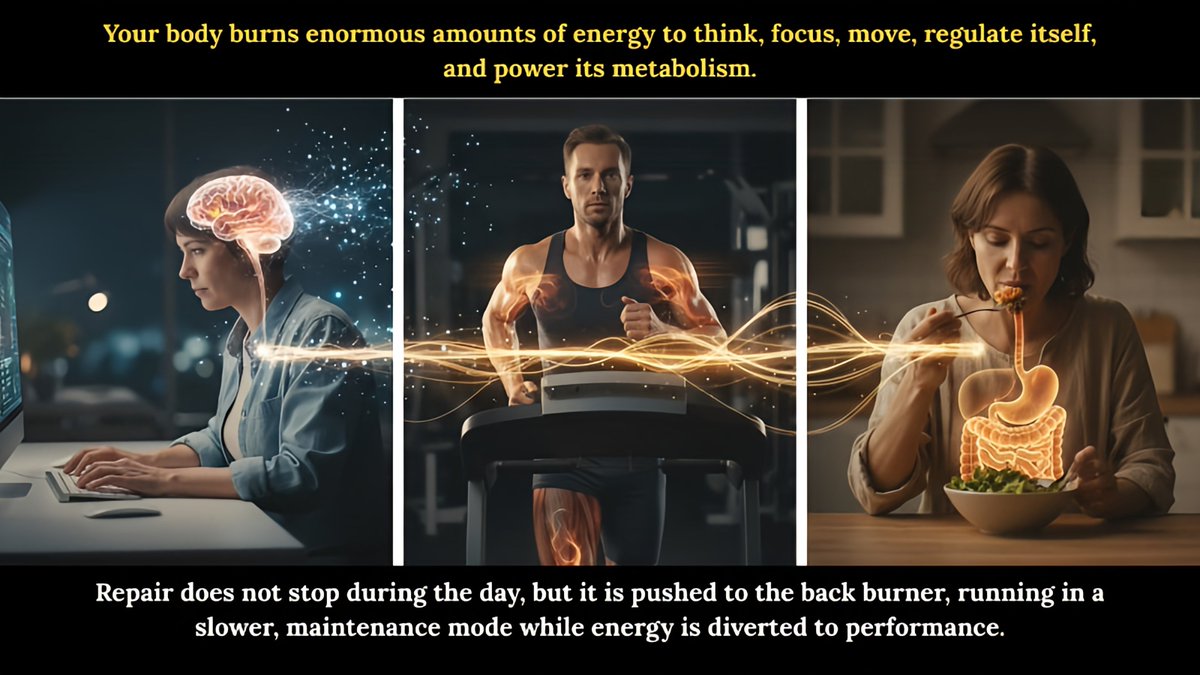
Sleep is not passive rest.
It is active biological maintenance. It also regulates inflammation and circadian DNA repair genes.
Diet and exercise help, but they cannot fully compensate for daily repair deficits caused by poor sleep.
3
4
145
Andy Blidy retweeted
#Glioblastoma immunotherapy has not failed. Checkpoint monotherapy has, and this study shows why.
This is the right paper to be reading, and the read here is accurate. It is also bigger than a biomarker for some future trial. Ghannam and colleagues did not just find a way to choose patients. They showed why checkpoint blockade fails in glioblastoma, and the biology they isolate names the one thing a working therapy must supply. The platform built to supply it already has Phase 3 data.
What predicted survival. Set against 365 standard-of-care tumors, the 181 checkpoint-treated cases told a clean story. The mesenchymal tumors, the most aggressive and the worst under chemoradiation, lived the longest on immunotherapy. That reversal is the tell. What separated the survivors was not mutation count but visibility: high HLA class I on the cancer cells, the badge a T cell reads to see what is inside, paired with T cells already sitting in the tumor. The group with the most mutations gained nothing. The group with the fewest lived longer. Tumor mutational burden, the workhorse biomarker everywhere else, was useless here. Dexamethasone at the start erased the benefit, and only in the mesenchymal tumors, while concurrent bevacizumab tracked with worse survival (HR 1.65). This was never an antigen shortage. It is an instruction problem, not an arithmetic one.
The escape route the post names. The resistance finding is the key. Tumors that started visible went dark. They shed the mesenchymal program, dropped their HLA, and lost their T cells. That is the ceiling of checkpoint blockade. A checkpoint inhibitor lifts a brake off a T cell. It cannot build a target, install instruction, or force a tumor into the light, and a freed T cell still cannot act on a tumor it cannot see. Alone, the brake had nothing to release.
The vaccine builds what the brakes release. That is the whole misread. The checkpoint did not fail. It was handed nothing to free. A response has to be built first, and building it is what the vaccine does. DCVax-L takes the patient’s own dendritic cells, the immune system’s professional teachers, matures them outside the tumor’s reach, and loads them with whole tumor lysate. A CD4 helper licenses the loaded cell through a CD40L-CD40 handshake, and the licensed cell pours out IL-12 to arm a killer against the entire tumor rather than one engineered target. The honest limit is where the design earns its place: a primed killer still needs the tumor to show its badge to kill it, so no vaccine beats a tumor that erases its display outright. The interferon those T cells release turns the badge back up, pushing tumors toward the visible state this study rewards, and natural killer cells, which hunt by scent rather than sight, take the badge-less escapees. The response is broad, so losing one target does not end it, and it widens as the fight goes on.
Now the checkpoints have a job, and there are two of them because the response has two phases. CTLA-4 is the brake on priming, where the army is built, and an anti-CTLA-4 antibody frees it early. PD-1 is the brake on killing, where the armed cell meets the tumor, and an anti-PD-1 antibody frees it after. The mechanism predicts the order: free priming while the army forms, free killing once it reaches the target. The neoadjuvant result that looks contrary is about timing relative to surgery, not to priming. Both brakes act only on what the vaccine builds. Take out the vaccine and there is nothing to release.
The combination already follows from the record. It does not need a new trial to be argued, only three things already published. The mechanism above. The vaccine’s own Phase 3 result, where DCVax-L added to standard care extended survival in newly diagnosed and recurrent glioblastoma. The trial used external controls, the sound and ethical choice here, because glioblastoma kills on a timetable that has barely shifted in a generation, and a course so uniform and so lethal makes a natural-history comparison reliable while sparing dying patients a placebo arm. And this study itself, with Kunz independently confirming the DCVax-L survival figures and finding that checkpoints added to chemoradiation did nothing, for want of a built response to free. Put those together and the combination is not a hope but the obvious next assembly. There is also a first direct look at it: an interim UCLA analysis, unpublished, in which adding one PD-1 inhibitor to the vaccine pushed median survival in recurrent disease past the point of being reached, against 275 days for the other arm. That is a single brake freed on a built response, and the mechanism predicts the second brake adds more, though that part remains rationale. Throw the slide out and the argument stands. Keep it and the prediction already has an early yes. One structural fact explains why the full regimen is not already in a trial: the PD-1 inhibitor in that data is Merck’s, and the established drug for the other brake is Bristol-Myers Squibb’s ipilimumab. Competitors do not co-sponsor one registration trial, so the combination will reach patients through clinical practice before a protocol catches up.
It is already being treated. Checkpoint monotherapy failed because it freed a brake on a response no one had built. Build it with DCVax-L, the only immunotherapy with positive Phase 3 survival data in this disease, and the brakes have something to release. In 331 patients it raised median survival in newly diagnosed disease to 19.3 months from 16.5 (HR 0.80, P=0.002) and five-year survival to 13.0% from 5.7%, and in recurrent disease to 13.2 months from 7.8 (HR 0.58), with methylated-MGMT patients doing better still. It is under review by the UK’s medicines regulator now. The post asks the field to read the tumor’s state of mind. The platform that gives the tumor that state of mind, and gives both brakes something to release, already exists.
Scientific analysis of published work, not investment advice; the mechanism and its link to $NWBO #DCVax-L are interpretation, not claims of the cited authors, and the UCLA combination data are interim and unpublished.
Sources: Ghannam et al., Nature Cancer 2026 (doi.org/10.1038/s43018-026-0…); Liau et al., JAMA Oncology 2023 (doi.org/10.1001/jamaoncol.20…); Kunz et al., Journal of Clinical Neuroscience 2026 (doi.org/10.1016/j.jocn.2026.…). Full reference list on request.

3
14
396
Andy Blidy retweeted
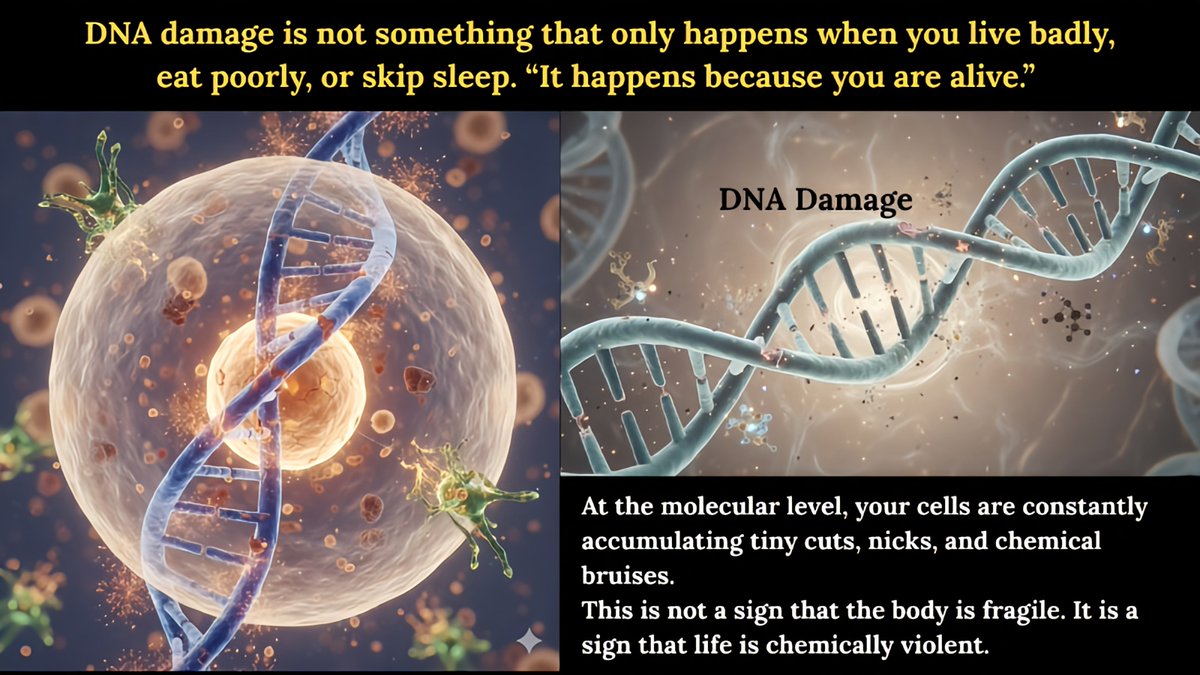
Every day, each of our cells experiences ~10,000 to 100,000 DNA lesions from normal metabolism, reactive oxygen species, and other endogenous processes.
Many of these repair processes (DNA repair, autophagy, protein clearance) are prioritized and more efficient during deep sleep.
Also ... Our DNA repair systems (homologous repair, non-homologous repair, base excision repair, autophagy, etc.) are highly active during sleep ...
Most energy-demanding repair processes are prioritized and more efficient during deep sleep.
1
5
172
Andy Blidy retweeted
NewLimit’s liver result is real, and it proves my point, not theirs. One dose and the aged hepatocyte behaves young again. That only happens if the cell was never broken. Aging is not damage. It is a stuck signal sitting on intact machinery, and a stuck signal can be lifted. NewLimit has paid 435 million dollars to demonstrate the premise of the upstream fix, then aimed the platform one level too low.
Here is the stuck signal, exactly. In a senescent cell, leaking mitochondrial DNA and RNA get read by the cell’s own viral sensors, cGAS and MAVS, as an infection that is not there. The cell is hearing its oldest symbiont in its oldest enemy’s voice. That false alarm drives NF-κB into the nucleus, and 30 of the 32 canonical SASP genes are direct NF-κB targets. The entire inflammatory output we call aging traces to a misreading the body keeps acting on. It is not entropy. It is misperception, and misperception is correctable.
Now the part the field keeps walking past. Evolution already solved longevity, three separate times, in lineages that have not shared an ancestor in 300 million years. The naked mole rat lives 32 years, almost never develops cancer, and carries no NK cells at all. The bowhead whale lives past 200. The Galapagos tortoise lives past a century. They share almost nothing ecologically. They share one feature: preserved IL-12 output from dendritic cells deep into late life, feeding type-one cytotoxic effectors that do not senesce. The downstream effector is interchangeable. The mole rat runs a single γδ clonotype where we run NK and CD8. The conductor and the score never change: dendritic cell, to IL-12, to type-one killer. That circuit is not one mechanism among many. It is the answer natural selection converges on every time it builds a body that lasts.
And the conductor has no understudy. The cDC1 is the only cell that delivers the full instruction, and when it is silenced, every disease that requires its silence moves onto the empty stage: cancer, chronic viral reactivation, the Th1-deficient phase of autoimmune disease, neurodegeneration, and aging itself. One slot, one failure mode, many names.
So look at what each program is choosing to trial. NewLimit rejuvenates one downstream cell type, in place, and will need a separate campaign for the next tissue, and the next, because LNPs home to the liver and nowhere convenient. The conductor sits above all of them. Restore it and the surveillance that clears senescent cells runs across dermis, fat, marrow, vasculature, and brain at once, from a single intervention. Reprogramming rebuilds the instruments one section at a time. The circuit rebuilds the instruction. Only one of those scales to a whole body.
In-place rejuvenation also has to win a fight it cannot win. The silenced cDC1 is held shut by seventeen locks: seven epigenetic loops on the IRF8 gene, ten more at the tissue level, redundant and so tightly coupled that a single gene, GRIM-19, severs the brake line at three levels at once. It is induced by IRF8, it inhibits nuclear STAT3, and it builds the Complex I that makes the cofactor the demethylases need. Lose it and all three locks engage from one event. Drugs hit one target. You cannot drug seventeen redundant locks, and you cannot reset a cell in place while the inflammatory field that installed the locks is still reinstalling them in real time. So you stop trying to pick the locks. You manufacture the corrected cell outside the body, in a chamber where the locks were never installed, and you deliver it back running. That is the move neither the small-molecule field nor the in-place reprogramming field has made.
The effector arm for this is already inside the patient, and it does not age. Every adult carries between fifty and five hundred million Vγ9Vδ2 cells that look identical at ninety and at twenty: telomeres intact, function intact, IL-12 receptor locked permanently open and unable to be turned down. Their numbers fall with age, and that decline was misread for years as the cells wearing out. They do not wear out. Each new wave reaches the periphery, activates against the first stress it meets, finds no IL-12 rescue signal waiting, and dies within days by design. The veterans on the wall are perfect. The reinforcements have been dying for forty years for want of one signal. The intervention does not just wake the veterans. It restores the signal that stops every future reinforcement from dying.
This is also why no cytokine shortcut works. Soluble IL-12 pushed into a vein killed two patients in the 1990s, and the field read it as a dose problem. It was a geometry problem. The same molecule delivered cell-to-cell at a synapse, with CD2 engaged, flips the receiving cell from the death pathway to the survival pathway. The dendritic cell is not a delivery vehicle for IL-12. It is the geometry that makes IL-12 survival instead of death. No injection reproduces it.
And the product is buildable now, which it was not until weeks ago. A May 2026 single-cell readout finally explained two decades of failed γδ trials in one figure: the αDC1 product everyone infused was one to two percent the correct instructing cell and ninety-eight percent cells that quietly recruit the suppressive side of the immune system. The patients’ γδ cells were not weak. They were handed the wrong instruction by the wrong ninety-eight percent. The correct cell, Cluster E, is sortable on defined surface markers. The human safety is already bought and paid for: the αDC1 platform has existed since the early 2000s, DCVax-L cleared Phase 3 (Liau, JAMA Oncology 2023, hazard ratio 0.58 at recurrence), and γδ trials have dosed hundreds of patients with no dose-limiting toxicity, no cytokine release syndrome, and no graft-versus-host disease. Only the integration is new, and the company that would run it already holds every piece. Northwest Biotherapeutics $NWBO carries #DCVax-L, the αDC1 platform in-licensed from Roswell Park, and a closed perfusion manufacturing line at Sawston. The instructor arm, the effector rescue, and the manufacturing chassis sit co-located in one company, not scattered across a hundred papers waiting to be assembled. The integration this post describes is a protocol decision away, not a discovery away.
Run it the way the biology dictates, which the failed trials did not. Enroll patients just past the second aging crest near sixty, the transition where the silencing turns from intermittent to durable, because those are precisely the patients whose own conductor can no longer hold up its end. Give both arms, the instructing αDC1 and the rescued effectors, not one. Then ask the single question that settles the entire theory: does IRF8 demethylate in marrow dendritic-cell progenitors at six and twelve months. If it does, the niche has thawed, endogenous IL-12 production resumes on its own, and the therapy retires itself, a cure rather than a subscription. If it does not, the architecture is wrong, and one bone marrow biopsy will say so. Almost no longevity program can name the measurement that would refute it before dosing. This one can, and that is the difference between a hypothesis and a wager.
Anticipate the obvious objection: LNP delivery is improving, extrahepatic targeting is coming. Grant it entirely. Even perfect delivery still leaves you reprogramming each cell type, in place, inside the exact inflammatory field that reinstalls the locks. The circuit’s targeting is biological, not engineered. A partially matured αDC1 is built to sample whatever the tissue is broadcasting and convert it to a clean type-one output after injection, so a single standardized product is meant to cover every indication while the patient’s own tissue supplies the antigens. The delivery problem NewLimit has to solve tissue by tissue, this architecture answers once.
Nature already ran the proof. Hambleton’s 2011 patient was born with both copies of IRF8 disabled, developed no cDC1, suffered the exact disseminated infections this circuit exists to prevent, and partially recovered on exogenous IL-12 alone. The aged adult is the easier case, not the harder one, because the child’s machinery was absent and the adult’s is merely silenced. The DNA is intact. The proteins are intact. Only the modification state has to come off. That is the oldest claim in osteopathic medicine made molecular: the physician does not supply the healing, the physician removes the obstruction, and the body resumes what it always knew how to do. The αDC1 does not heal aging. It lifts the silencing. Given a working conductor, the body does the rest.
The cells were never broken. They have been waiting forty years for an instruction that stopped arriving. The trial that matters is the one that sends it.
x.com/andrewcaravello/status…
1
4
307
Andy Blidy retweeted

Andrew Caravello, DO
@andrewcaravello @alphavestcap
$NWBO #DCVax runs on the exact mechanism this post is describing. The whole-body response from one local shot is not luck. It is the principle behind Pawel Kalinski’s αDC1, the dendritic cell technology Northwest Biotherapeutics licensed and is carrying forward. Your immune system fights cancer through a conversation between two cells. The first is the teacher, a dendritic cell, or cDC1. It picks up pieces of a tumor and shows them to the killers, the T cells that do the fighting. For that lesson to land, two things click into place, like a handshake. A helper cell gives the teacher permission to speak, a signal called CD40. Then the teacher speaks, and its words are IL-12, the broadcast that arms the killers and sends them through the whole body. CD40 is the permission. IL-12 is the speech. Now the headline makes sense. Treat one tumor, and the teacher inside it learns that tumor, gets permission, and broadcasts IL-12. The killers it arms travel everywhere and strike tumors the needle never touched. The body files the lesson as memory, so the response lasts. Doctors call it in-situ vaccination. One site teaches the whole system. Here is what the post leaves out. All of it depends on the teacher being able to speak, and cancer silences the teacher at the level of the genes. A master switch called IRF8 makes the cell a teacher in the first place. The disease pins a chemical tag on it and locks it off, and bolts the IL-12 message shut besides, from more than one direction. The teacher is still there. It has gone mute. This is where the drug in the study hits its first ceiling. A CD40 agonist is a manufactured permission signal. It walks up to the teacher and grants the go-ahead to speak, standing in for the worn-out helper cells. Clever, and it solves exactly one piece of the problem. But permission is worthless if the teacher has lost its voice. Hand a permission slip to a cell whose IL-12 message is locked shut, and nothing comes out. Worse: give that permission to a patient whose teacher is already gone, and the body trains suppressor cells that tell the immune system to stand down (Burrack). The few patients who responded still had a working teacher. The drug found a voice that could speak. It did not rebuild a silent one. So the honest line is narrow: the drug works where the teacher still has a voice, and cannot help the patients whose teacher has gone silent, who are the ones who need it most. The drug has a second ceiling, and it is poison. CD40, the permission switch, is not only on the teacher. It sits on immune cells, blood vessels, and the platelets that clot your blood. Push it everywhere at once, which is what a drug in the bloodstream does, and the body overreacts: a body-wide inflammatory storm, liver damage, a dangerous drop in platelets. That toxicity is the wall that has capped CD40 agonists given in the blood, and it is why this one had to be re-engineered and injected straight into a tumor to stay safe. But injecting into one tumor lands you back at the start. Now you need that tumor’s teacher to carry the response body-wide, and in a sick patient that teacher is the silenced one. The safety fix recreates the problem. The αDC1 carries neither ceiling, because it does not push a button on a broken cell. It is a brand-new teacher, built outside the body in a dish the disease cannot reach. You grow it already able to speak, at full volume. A recipe of immune signals, IFN-γ, IL-1β, TNF, and a few more, delivers in the dish the permission an aged helper cell can no longer deliver in the body. It broadcasts IL-12 at about forty times the volume of the older dendritic cell vaccines (Mailliard 2004). And it speaks up close, one teacher to one killer, not flooded through the blood. That matters, because IL-12 given into the blood as a raw drug was so toxic it killed patients in a 1995 trial. Same molecule, whispered at the right address instead of shouted through the whole body. It does one more thing. The army it raises gives the patient’s own silenced teachers the permission their worn-out helpers stopped giving, and lifts them back into the conversation. The injected cell is the spark. The patient’s own restarted conversation is the fire. This is the technology Northwest Biotherapeutics licensed from Kalinski through Roswell Park, and DCVax is already that cell, a dendritic cell grown to speak IL-12. The αDC1 is the same cell turned up louder. DCVax-Direct injects it straight into the tumor, the literal one tumor this post is marveling at. And in the human trial of that cell, across forty patients and thirteen cancers, one thing predicted who survived: how much IL-12 the injected cells produced (Subbiah, p=0.028). The variable the science calls the bottleneck was the variable that mattered in patients. So read the headline for what it is. A small injection driving a whole-body response is not a someday result. It is the documented mechanism of the αDC1. The drug version flips a permission switch on a cell that may already be silent, and floods the body to do it. The cell version brings its own voice and speaks at the right address. One depends on a teacher the disease has taken away. The other is the teacher. The mechanism is textbook. The cell that carries it is Kalinski’s. The company carrying it forward is $NWBO. #DCVaxForBraelyn
2
15
653
Andy Blidy retweeted
🏀 The case for $NWBO starts with a claim that sounds wrong until you watch LeBron play at 41.
He is Athlete of the Century with more mileage on his body than anyone alive, and knees that outlasted players half his age. If joints simply wore out, that is impossible.
They do not wear out. They stop being cleared, once the cell that issues the order goes silent. He kept his issuing it.
$NWBO builds the cell that carries that order back.
X Article: x.com/andrewcaravello/status…
The Biological Reboot: a.co/d/0bgObRNK
#DCVaxForBraelyn #GBM @KingJames

LeBron James wrote the blueprint for exceeding expectations.
Here’s how our first-ever TIME100 Sports cover star redefined the modern athlete: time.com/collection/time100-…
4
22
1,441
Jun 13
RT @brkthroughprize: INTO THE LIGHT: Jean Bennett, Katherine A. High and Albert Maguire shared the 2026 Breakthrough Prize in Life Sciences…
2
Andy Blidy retweeted

Jun 12
$NWBO @MHRAgovuk @NBTStweets @AlMusella @braintumourrsch
MHRA, you need to do better based on your standard timelines you shoot for. You have exceeded your own set timelines by a factor of 4. GBM patients such as shown here has to raise funds to extend or sometimes even cure the Brain Cancer.
Jun 12

1
17
72
2,447
Andy Blidy retweeted

Jun 13
Scientists removed the extra chromosome that causes Down syndrome from human cells using CRISPR gene-editing.
Led by Dr. Ryotaro Hashizume, the research team achieved "trisomy rescue" by targeting the surplus copy of chromosome 21, which is responsible for the condition's developmental and cognitive challenges.
By deploying precise molecular guides, the team successfully excised the extra chromosome and restored typical cellular functions in over 30% of the treated human cells. This breakthrough represents the first time an entire extra chromosome has been cleared from patient-derived cells, resulting in healthier, faster-growing cells with restored gene expression.
Although the research is in its early stages and currently confined to lab-grown cells, it represents a bold leap forward for precision medicine.
Instead of targeting individual genes, this approach addresses the genetic root of the condition, offering a revolutionary glimpse into future chromosomal therapies. Researchers caution that translating this laboratory success into real-world patient treatments will require extensive safety trials, refined delivery systems, and careful ethical considerations.
Nevertheless, this proof of concept marks a promising step toward potentially altering the trajectory of Down syndrome and other complex genetic conditions.
source: Hashizume, R., Wakita, S., Sawada, H., Takebayashi, S., Kitabatake, Y., Miyagawa, Y., Hirokawa, Y. S., Imai, H., & Kurahashi, H. Trisomic rescue via allele-specific multiple chromosome cleavage using CRISPR-Cas9 in trisomy 21 cells. PNAS Nexus.

8
59
169
12,287
Andy Blidy retweeted
Steve, I am sorry for what Daniel and Lauren are facing. There is a real treatment option for Lauren that is reachable in the UK right now, and I want to make it simple to act on. I am a physician, and I am glad to help. Please get this to Daniel.
DCVax-L is a personalized immunotherapy for glioblastoma. It has been available in the UK for several years on a compassionate use, private pay basis under the “Specials” route, manufactured near Cambridge. Patients from the US, Germany and Canada have been treated, so being outside the UK is not a bar.
To start, Lauren’s neuro-oncologist or neurosurgeon submits a request to the maker, Northwest Bio, through the new patient inquiry form: nwbio.com/patients-informati…. There is a wait list, so the sooner her team reaches out, the better. You or Daniel can message me directly, and I will help walk her medical team through it.
One instruction matters more than any other, and most hospitals do the opposite by default. The vaccine is made from Lauren’s own tumor tissue, and that tissue must be kept fresh, unfixed, and frozen. Standard pathology drops tumor into formalin and paraffin wax, which destroys the proteins the vaccine needs. Formalin fixed tissue cannot be used. So before any surgery or biopsy, tell the surgeon to set aside a fresh, unfixed piece of tumor and freeze it. That one step often decides whether she is eligible.
Why it can work: dendritic cells are the immune system’s master cells. DCVax-L loads them with the full set of markers from a patient’s own tumor and gives them back as a simple injection in the arm, so the immune system learns to hunt many targets at once rather than one, which the cancer cannot easily escape. It has been notably safe across more than a decade of use, with no serious treatment-related toxicities.
The survival data are not a someday promise. In the Phase 3 trial of 331 glioblastoma patients across four countries, published in JAMA Oncology, adding DCVax-L to standard care extended overall survival. At recurrence, median survival was 13.2 months versus 7.8 (hazard ratio 0.58), with a meaningful tail of patients alive years later.
Daniel and Lauren make the call, but this is a real door, open now. Reach out anytime.
To see what the path looks like, follow #DCVaxForBraelyn, where Braelyn’s mom Amanda (@HollensbeAmanda) is documenting her 18-year-old’s DCVax journey.
2
6
45
908
Andy Blidy retweeted
$NWBO #DCVaxForBraelyn @SecKennedy @MHRAgovuk #GBM @AlMusella @glioblastf @glioblastomaorg @GBCancerStudy #DCVax x.com/HollensbeAmanda/status…
2
19
71
1,299
Andy Blidy retweeted
Jun 12
MIT settles quantum debate, proving Einstein wrong
MIT physicists have just delivered the most precise version yet of the iconic double-slit experiment — and in doing so, they’ve effectively proven Albert Einstein wrong about one of quantum physics’ greatest mysteries.
Using ultracold atoms and single photons, the team recreated the experiment at a level Einstein and his rival Niels Bohr could have only imagined.
The result?
Bohr was right: a photon can act like a wave or a particle—but never both at once. Their work demonstrates that when information about a photon's path is gained—even indirectly—its wave-like interference disappears, affirming the uncertainty principle at the heart of quantum mechanics.
The breakthrough came from a novel method that used isolated atoms as “slits” and tuned their “fuzziness,” or spatial uncertainty, to control whether light acted like a wave or particle. In doing so, the MIT team stripped away classical components like springs or screens and showed that Einstein’s proposed workaround for observing both aspects of light simultaneously doesn't hold up. This experiment not only clarifies a century-old debate but also marks a milestone in quantum research during what the UN has declared the International Year of Quantum Science. The findings shine new light on the strange, fundamental rules that govern the quantum world.
source
“Coherent and Incoherent Light Scattering by Single-Atom Wave Packets” by Vitaly Fedoseev, Hanzhen Lin, Yu-Kun Lu, Yoo Kyung Lee, Jiahao Lyu and Wolfgang Ketterle, 22 July 2025, Physical Review Letters.
29
53
168
7,315
Andy Blidy retweeted

Jun 12
So, you are suggesting the method you are commercializing can cure the patient before treatments?
or even prevent the disease?
1
1
1
85
Andy Blidy retweeted

On 4 June, The New York Times posted an online story with a dramatic headline: “In a First, Scientists Precisely Edit Human Embryo Genes.” Others quickly echoed the claim, reigniting a simmering debate over whether it’s safe, ethical, and worthwhile to create gene-edited babies. But the reality of the reported advance, an effort to improve the use in embryos of an approach called base editing, is more subtle than many stories suggested. (The New York Times changed its online headline by the next day to eliminate the “first” claim.)
Even the stem cell scientist who led the new work acknowledges the tool still has major limitations and says it shouldn’t yet be used to make a baby. “I think it [our findings] will shift the conversation but it won’t change the landscape of use anytime soon,” he says.
Science delves behind the headlines to look closer at his group’s research, posted as a preprint on 1 June: scim.ag/4urOwGR

ALT An embryo editing ‘first’ is more complicated than headlines suggest Scientists may have a better way to make gene-edited babies, but it’s still far from safe
2
1
12
2,874
Andy Blidy retweeted
1
5
18
73,786

**Simple implications:**
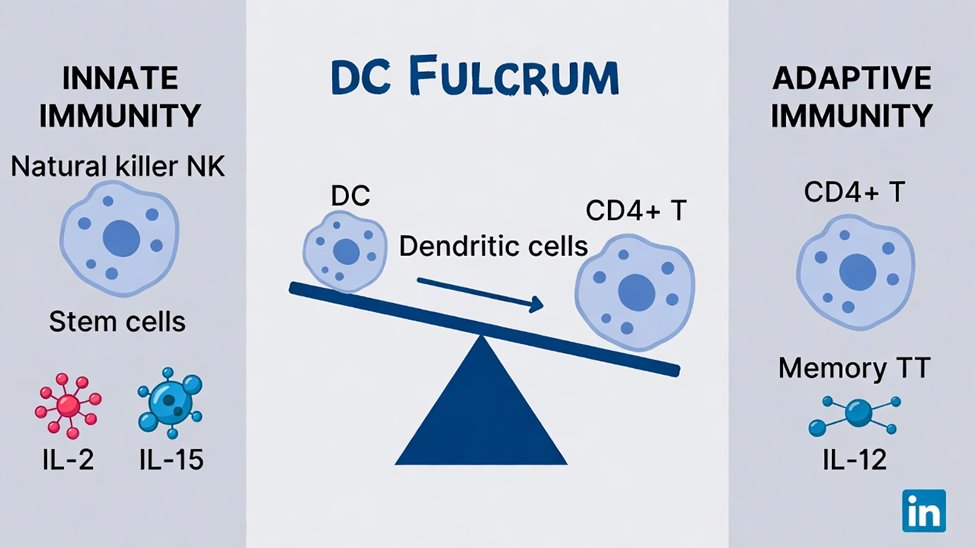
Osteoarthritis isn't inevitable "wear and tear." It's a biological failure: damaged/senescent joint cells build up because key immune instructor cells (cDC1 dendritic cells) get silenced and stop ordering their clearance via IL-12.
Heavy use triggers damage, but whether it becomes disease depends on whether the joint can still clean it up. Good lifestyle (exercise, sleep, recovery, diet) keeps the system working — which is why some high-load athletes stay healthy longer.
This shifts OA from "manage until replacement" to potentially preventable or modifiable by restoring immune surveillance (e.g., targeted cell therapies), not just mechanics or anti-inflammatories. It ties OA into broader aging/immune-clearance biology.
The theory predicts new tests and interventions focused on that silenced instructor cell.
1
2
49
Andy Blidy retweeted

Jun 11
Dixit is one of the 2,705 active members of the National Academy of Sciences
He joins fellow NAS members in cancer researcher Ira Mellman and immunologist Shannon Turley as recent departures from Genentech.
Mellman was laid off in a 2024 restructuring that hit cancer immunology
2
1
15
4,833