Mar 31
Las guías no se ponen de acuerdo sobre cuándo usar el calcio coronario en asintomáticos, y esa discrepancia tiene consecuencias directas en la consulta diaria.
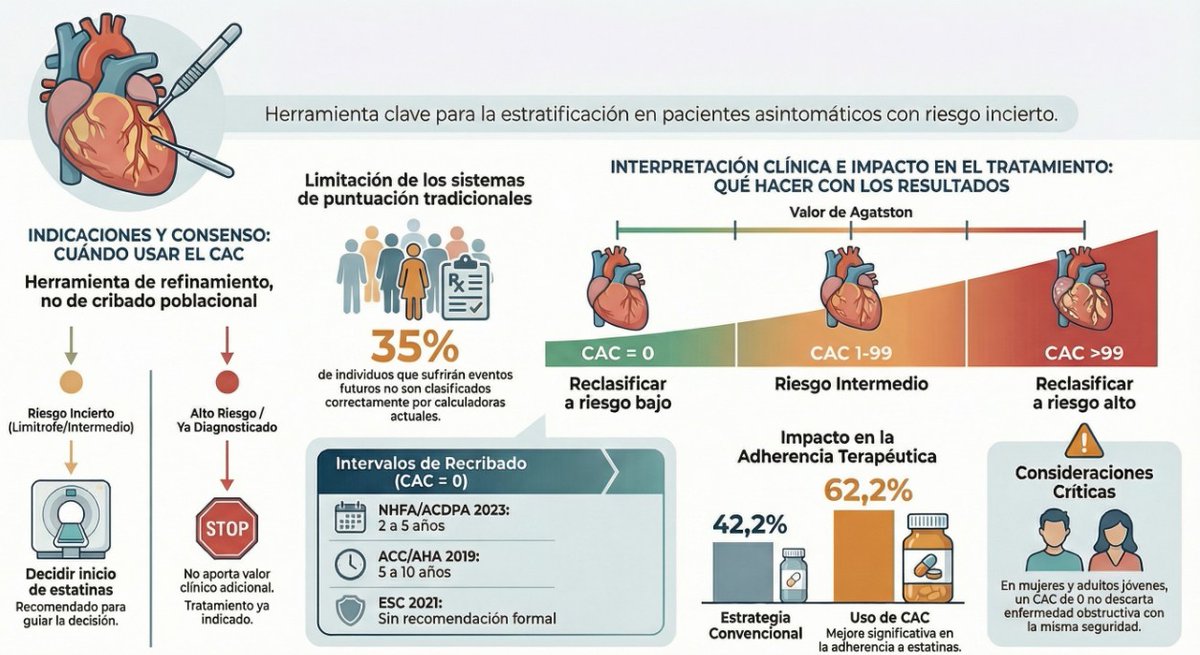
🫀 Puntuación de calcio coronario: cuándo usarla y cuándo no según ACC/AHA, ESC y Australia.
📋 Consenso en tres puntos clave: modificador del riesgo, toma de decisiones compartida y no indicada en alto riesgo.
⚠️ Discrepancias en fuerza de recomendación, categorías de riesgo diana e intervalos de recribado.
👥 Particularidades importantes en mujeres, adultos jóvenes y minorías étnicas.
🔬 Ensayos ROBINSCA y CorCal, próximos a concluir, podrían cambiar las guías futuras.
🤖 La inteligencia artificial ya permite calcular la puntuación de forma oportunista desde TC torácicos rutinarios.
📖 Descubre el análisis completo en CardioTeca. cardioteca.com/imagen/8020-q…
46
108
5,444

There is one underpowered trial ( EISNER) suggesting harm and 2 RCTs nearing completion ( Corcal and ROBINSCA). Why not wait before changing the guidelines? Perhaps, fear of those results?
1
1
7
1,015
It’s going to be very embarrassing to have to downgrade the recommendations after Corcal and ROBINSCA.
1
7
696

Jan 12
Progress in Risk Assessment and Lipid Management: Anticipated Updates in International Cholesterol Guidelines
Clinical Context:
Atherosclerotic cardiovascular disease (ASCVD) remains the leading cause of morbidity and mortality worldwide. Contemporary cholesterol guidelines in the United States and Europe are increasingly shaped by emerging trial data, refined risk prediction tools, and expanding lipid-lowering therapeutic options. The recently published State-of-the-Art Review highlights key evidence that is likely to influence forthcoming guideline updates.
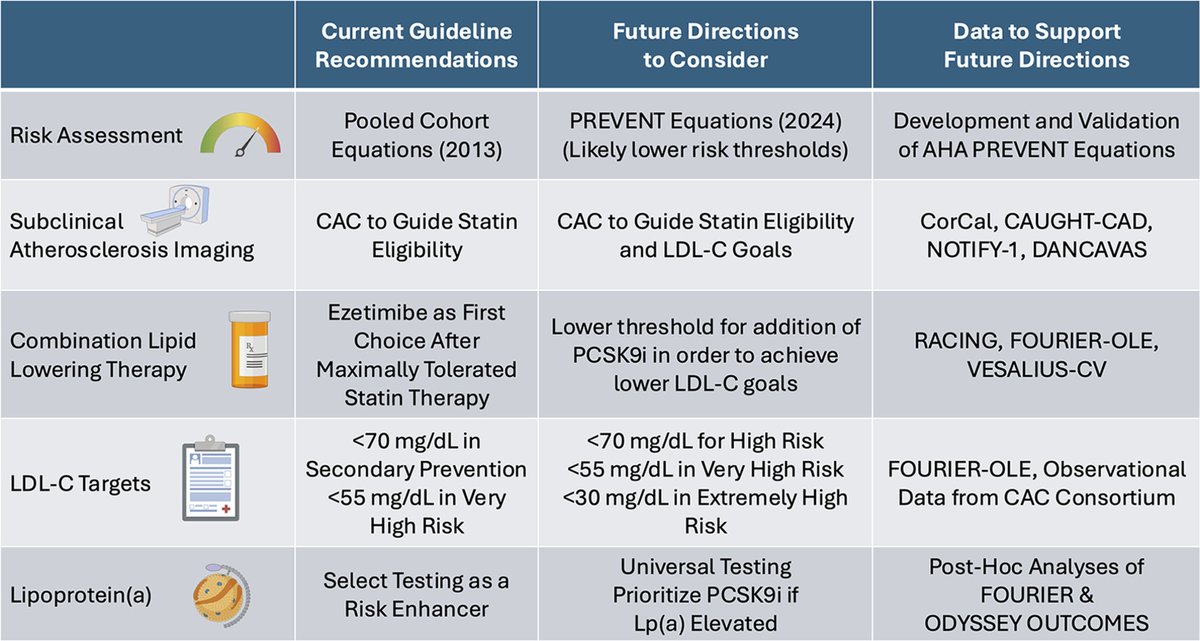
Risk Assessment: From Pooled Cohort Equations to PREVENT
ASCVD risk estimation continues to be the cornerstone of lipid management. Traditional guidelines have relied on the Pooled Cohort Equations (PCE, 2013) to stratify risk in primary prevention. However, accumulating evidence suggests that newer models, particularly the AHA PREVENT equations (2024), offer improved calibration and may define lower risk thresholds for intervention. This is expected to expand the pool of individuals eligible for earlier preventive therapy.
The incorporation of more contemporary population data and better representation of cardiometabolic risk makes PREVENT a likely foundation for future guideline algorithms in both the US and Europe.
Role of Coronary Artery Calcium in Risk Refinement
Coronary artery calcium (CAC) imaging has evolved from a risk modifier to a central decision-making tool. Current practice uses CAC scoring to guide statin eligibility in intermediate-risk individuals. Emerging evidence suggests that CAC will be increasingly used not only to initiate therapy, but also to define LDL-C targets and determine the need for more intensive lipid-lowering strategies.
Large population studies such as CorCal, CAUGHT-CAD, NOTIFY-1, and DANCAVAS demonstrate that CAC burden strongly predicts ASCVD risk and identifies patients who benefit most from aggressive LDL-C lowering beyond traditional risk factor assessment.
Combination Lipid-Lowering Therapy: A Paradigm Shift
Guidelines have traditionally recommended maximally tolerated statin therapy, followed by ezetimibe if LDL-C goals are not achieved. However, contemporary trials now support earlier and more routine use of combination therapy.
Evidence from RACING, FOURIER-OLE, and VESALIUS-CV suggests that many high-risk individuals require two or more agents to achieve contemporary LDL-C targets. For selected patients, low-to-moderate intensity statins combined with ezetimibe or bempedoic acid may offer effective LDL-C reduction with improved tolerability.
Furthermore, thresholds for introducing PCSK9 inhibitors are likely to be lowered, particularly in individuals with established ASCVD or high CAC burden, to facilitate achievement of more stringent LDL-C goals.
LDL-C Targets: “Lower Is Better” Reaffirmed
Current secondary prevention targets of <70 mg/dL for high risk and <55 mg/dL for very-high risk are increasingly being challenged by newer evidence. Data from FOURIER-OLE and large observational cohorts demonstrate continued ASCVD risk reduction at LDL-C levels as low as <30 mg/dL in extremely high-risk individuals, without significant safety concerns.
This reinforces the principle that intensive LDL-C lowering is both effective and safe, and supports guideline movement toward more aggressive target-based strategies in very-high and extremely-high risk populations.
Lipoprotein(a): From Risk Enhancer to Therapeutic Priority
Lipoprotein(a) [Lp(a)] testing is currently recommended selectively as a “risk enhancer.” However, post-hoc analyses of FOURIER and ODYSSEY OUTCOMES demonstrate that patients with elevated Lp(a) derive greater absolute ASCVD risk reduction from PCSK9 inhibitor therapy.
NEXT....
sciencedirect.com/science/ar…
Next...
1
2
12
600

11 Nov 2025
251111 🦁🫧
🦁 i miss you y/n *cutely*
🦁 *sends 9 ppeppero coupons for fans to get 🥹*
🦁 this time i wasnt kidding i really brought it hehehe
🦁 i want to give it to all of you but
🦁 who is gonna be todays luckyyy🍀
🦁 go run quicklyyyy
👥 woah! im in japan so i cant eat it ㅠㅠ
ㄴ🦁ㅠㅠ how good would it be if i could send it all the way to japan too🥺
🦁 instead, i will use them one by one (* implying that one fan should only use one coupon)
👥what ppeppero does hiyyih like the most?
ㄴ 🦁 for me its totally nude ppeppero
🦁 i can eat 3 boxes a day
🦁 what does y/n like the most?
👥 I’m you are favorite (eng)
ㄴ 🦁 I like u
👥 the corcal corn flavour and jyoseba (strawberry and orange) flavour was yummyy
ㄴ🦁eeehhh really ..??. is it april fools
🦁 they make those..
🦁 is it yummy~??
👥 i ran fast and got the ppeppero!! thank you hiyyih
ㄴ 🦁 Lucky girl🍀(eng) eat it well~
🦁 i have to go get my makeup done now!!

1
5
50
3,475

 Shailenzo.sun.and.moon 💚🧬🤍
Shailenzo.sun.and.moon 💚🧬🤍

1 Jul 2025
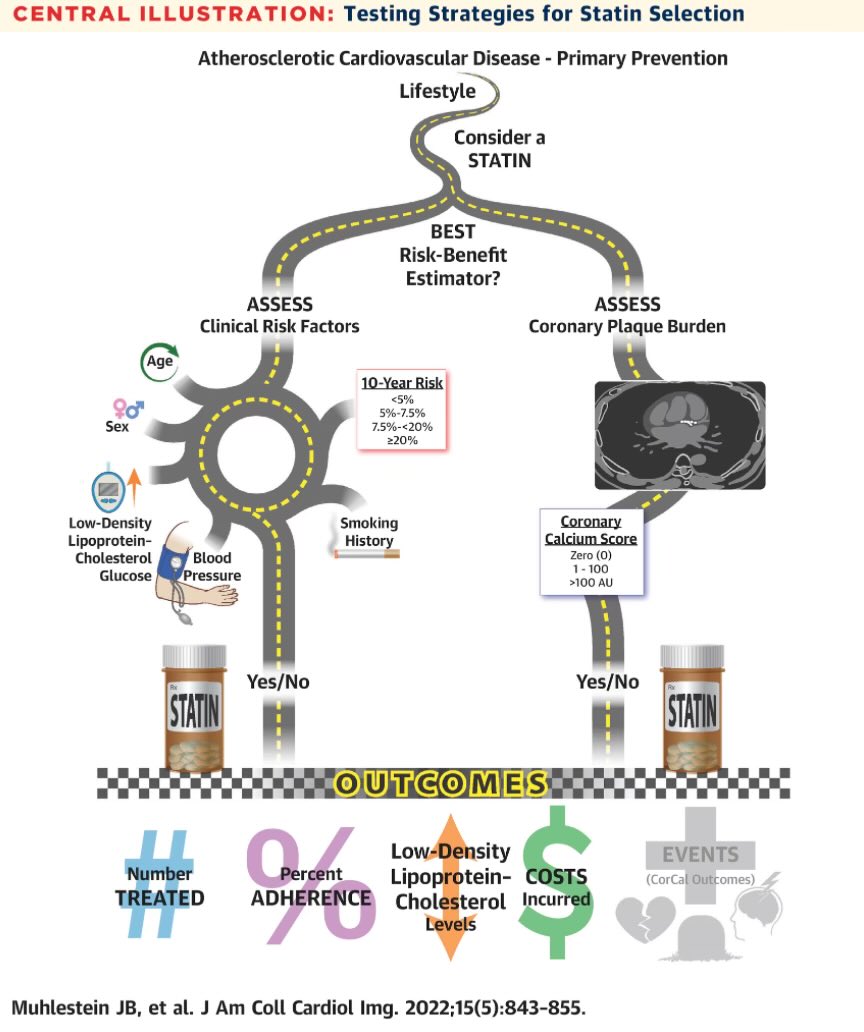
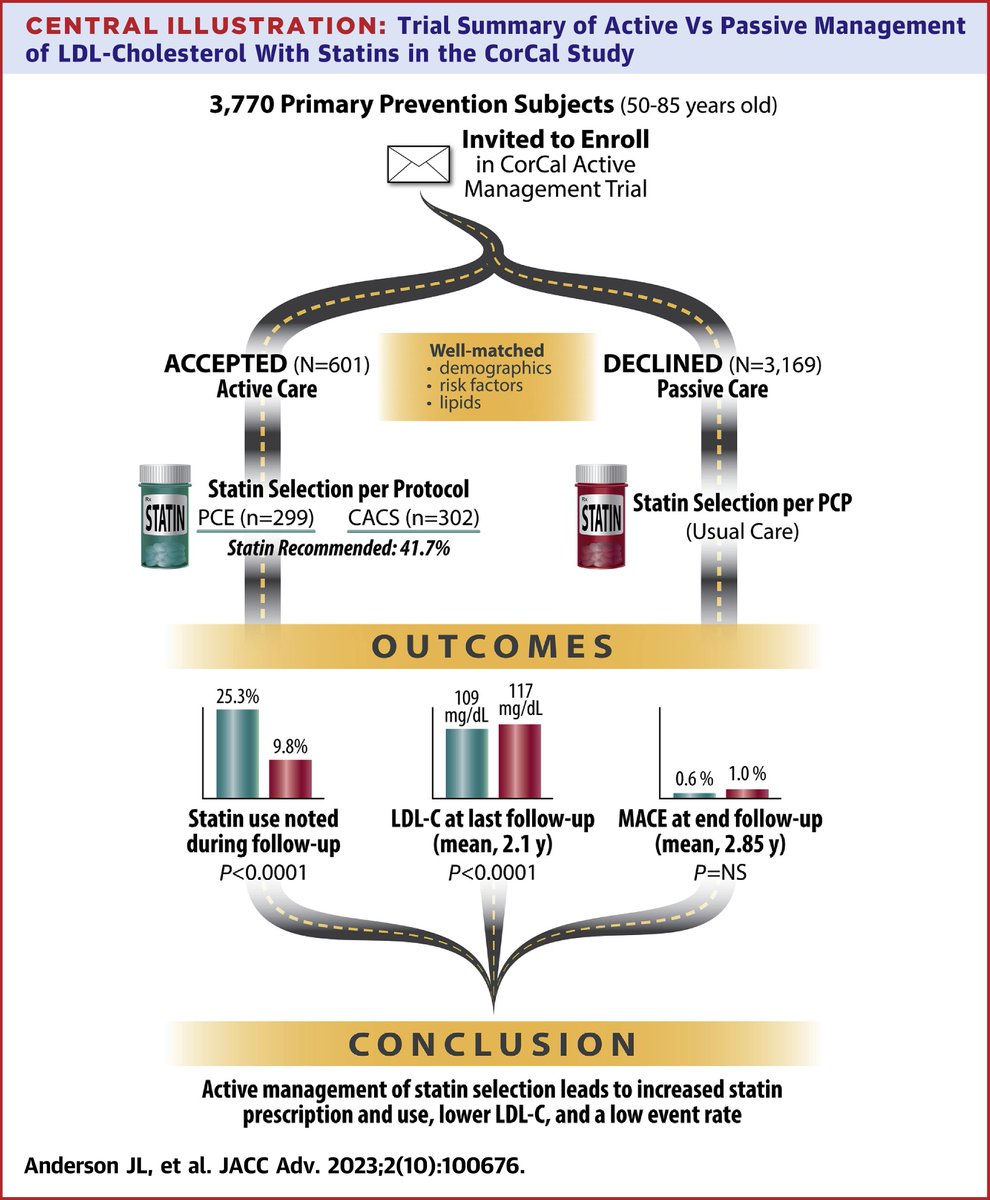
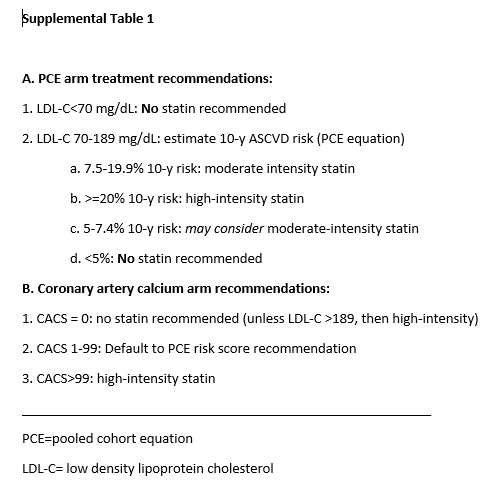
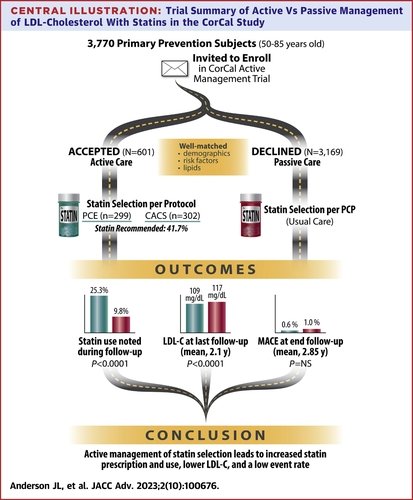
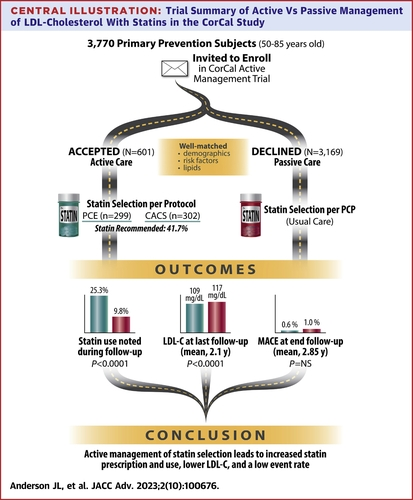
“The primary objective of CorCal was to compare 2 proactive ASCVD primary prevention strategies: CAC- (investigational) versus PCE {pooled cholesterol equation} - (standard) guided statin therapy.”
1
3
381


Effectiveness of a Proactive Cardiovascular Primary Prevention Strategy, With or Without the Use of Coronary Calcium Screening, in Preventing Future Major Adverse Cardiac Events (CorCal)

2
624

5 May 2024
🔴 Statin Selection for Primary Prevention (Active vs Passive): The CorCal Vanguard Trial
🔴Primary ASCVD Prevention: Optimally Active, Agile, and Accountable #editorial
#OpenAccess @JACCJournals
✅jacc.org/doi/10.1016/j.jacad…
✅jacc.org/doi/10.1016/j.jacad…
#CardioEd #Cardiology
1
30
71
5,086

29 Feb 2024
☝️We don’t need more LDLc/statin trials to evaluate outcomes, but with CAC
👇👇👇
Ongoing randomized trials in Europe, United States, and Australia studying CAC versus no CAC to evaluate for outcomes will answer any lingering questions about the utility of the test, and these are due out in the next few years. One such ongoing European trial is the DANCAVAS (Danish Cardiovascular Screening) trial, investigating whether multifaceted advanced CV screening will prevent CV events and whether possible health benefits are cost-effective.63 The ROBINSCA (Risk or Benefit IN Screening for CArdiovascular Disease) trial is awaiting final outcome results, after comparing traditional risk scores versus CAC.64 American trials are also extensive, including the CorCal (Effectiveness of a Proactive Cardiovascular Primary Prevention Strategy, With or Without the Use of Coronary Calcium Screening, in Preventing Future Major Adverse Cardiac Events) trial.65 The ongoing CorCal trial tests effectiveness of a proactive CV primary prevention strategy with or without CAC, compared with current standard care in preventing major adverse cardiac events.65 Also ongoing is the ACCURATE (Assessment of Patients With suspeCted Coronary Artery Disease by Coronary calciUm fiRst strATegy vErsus Usual Care Approach) trial, examining whether a CAC-first strategy may be used as a gatekeeper for progression to the cardiac positron emission tomography stress test. Australian CAUGHT-CAD (Coronary Artery calcium score: Use to Guide management of Hereditary Coronary Artery Disease) trial examines coronary calcium for risk evaluation and prevention in patients with a family history of CAD
2
5
103

Posada Del Corcal en Tama, el lugar perfecto para descansar y recuperar fuerzas, después d recorrer Picos de Europa. Tranquilo, acogedor, encantador en sus detalles, fantástico trato d sus propietarios y d Lili en la Posada y d Fernando en Casa Fofi, su restaurante fantástico.




2
100

6 Nov 2023
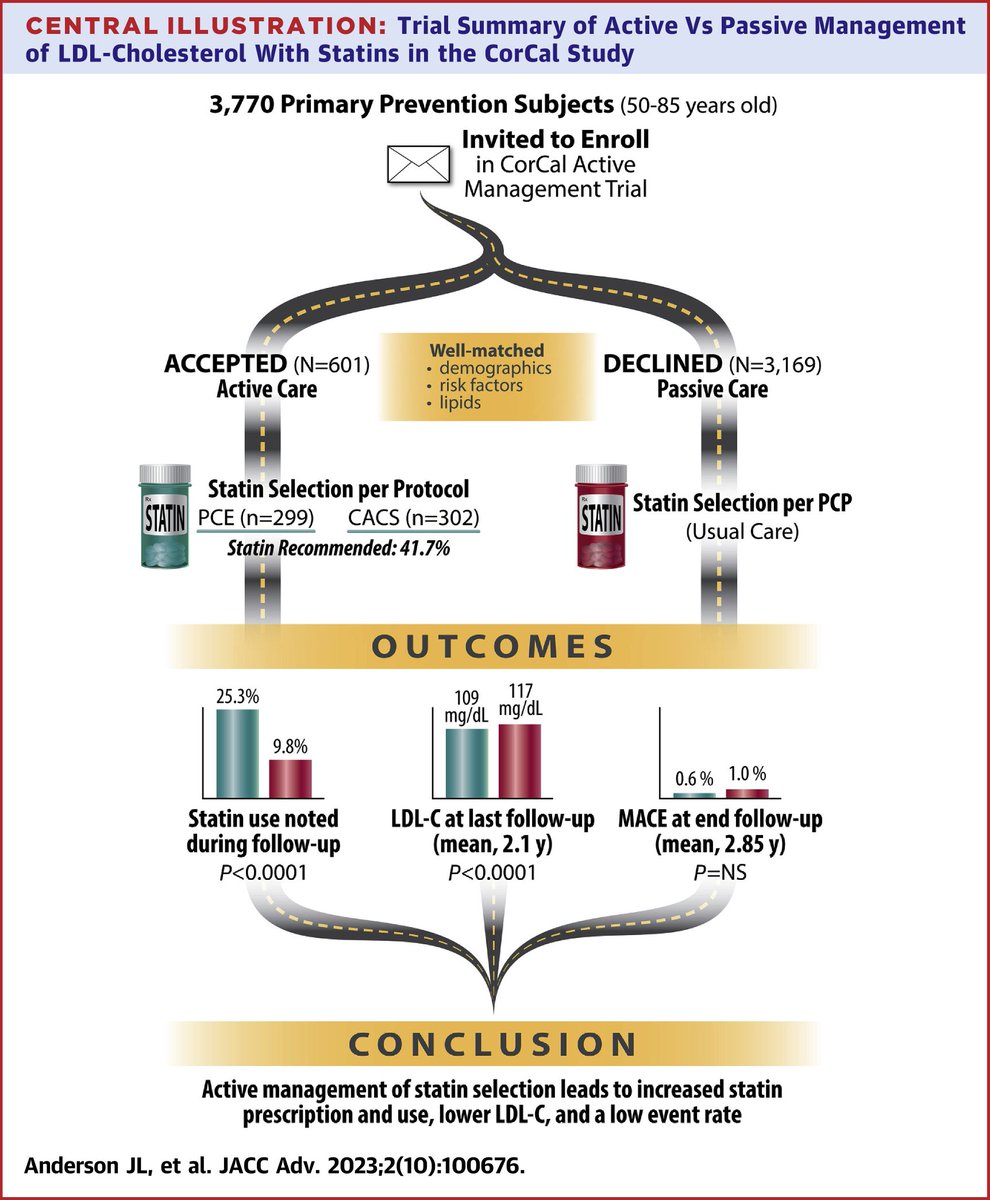
An active approach to statin selection for primary #ASCVD prevention identified a large treatment opportunity and led to over twice as many patients on statins compared to passive (usual care) management. bit.ly/3SoWlNW
#JACCAdvances #cvPrev #CorCal #CardioTwitter
1
11
27
9,173

3 Nov 2023
Dear Dr @VietHeartPA: congratulations for your brilliant work!
By the way, would you have an intention to capture long-term outcomes data without assisted-intervention?
Maybe we could note some differences between groups in The CorCal Vanguard Trial - Extended.
1
3
65

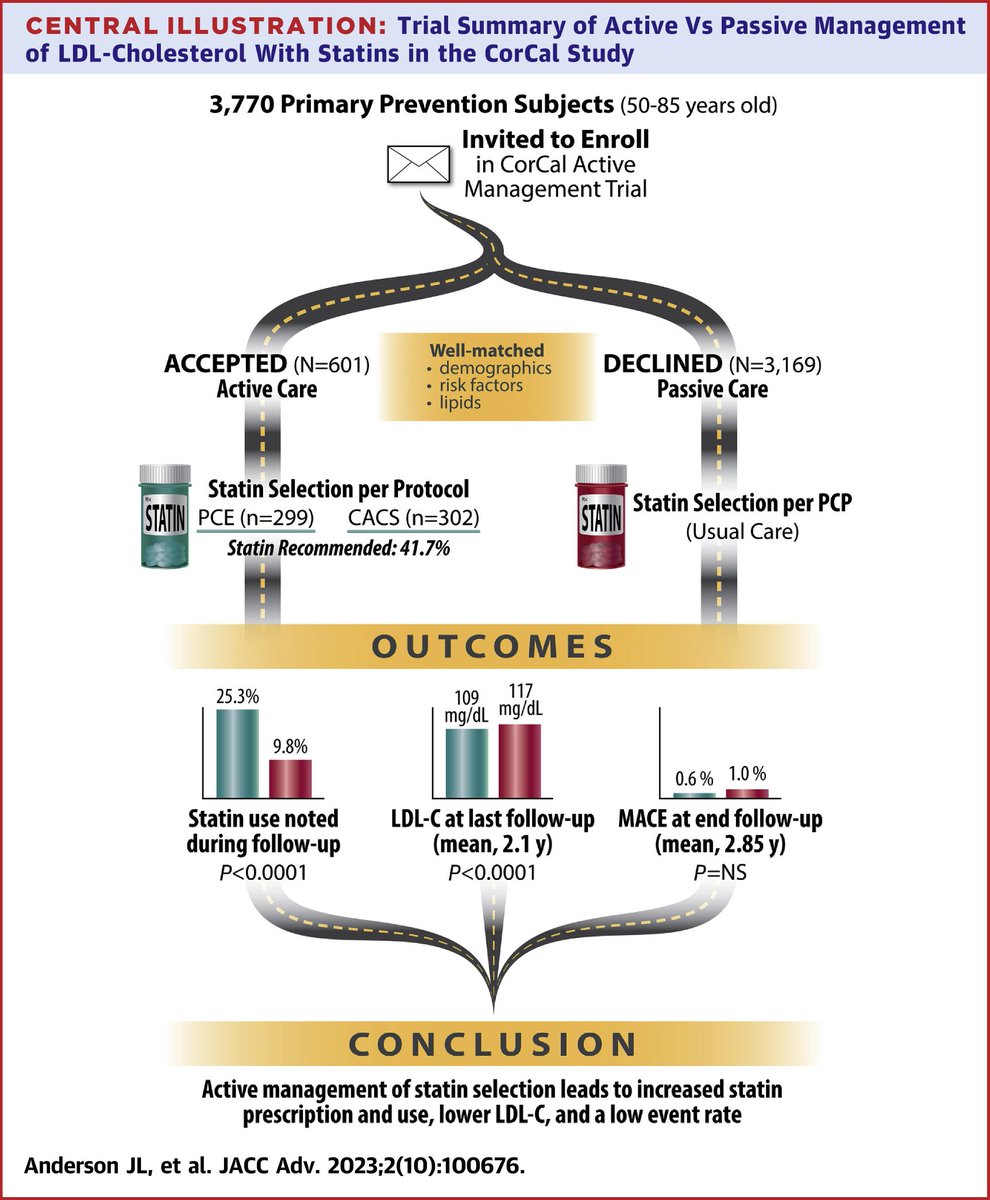
Thank you my friend. Agree. Not a large difference in LDL-C level attained 109 vs 117.
Here were the recommendations we used for Corcal Vanguard.
The Corcal main study implemented nuance in CAC too (75th percentile, when CAC 1-99).
1
2
286
2 Nov 2023
🫀Impact of Active vs Passive Statin Selection for Primary Prevention: The CorCal Vanguard Trial
👉 Active Mx (#PCE risk score #CAC) = Higher statin use than passive
👉Trend to lower MACE
jacc.org/doi/10.1016/j.jacad…
#CardioTwitter #Cardiology #cardioEd
3
4
399
Impact of Active vs Passive Statin Selection for Primary Prevention: The CorCal Vanguard Trial jacc.org/doi/10.1016/j.jacad… via @JBMuhlesteinMD et al. Not sure how the die-hard CAC enthusiasts are reacting now @DavidLBrownMD @drjohnm @andrewfoy @kaulcsmc @mmamas1973 @cpgale3
2
1
3
1,126
The #CorCal vanguard
1. Active management (risk score OR #CAC) = ^statin use than passive in primary prevention cohort
2. Trend to lower MACE
Impact of Active vs Passive Statin Selection for Primary Prevention: The CorCal Vanguard Trial jacc.org/doi/10.1016/j.jacad…
5
9
34
51,088

10 May 2023
Représentation hypothétique de Lautréamont issu de "La chambre de Lautréamont" de Corcal & Edith
3
76