
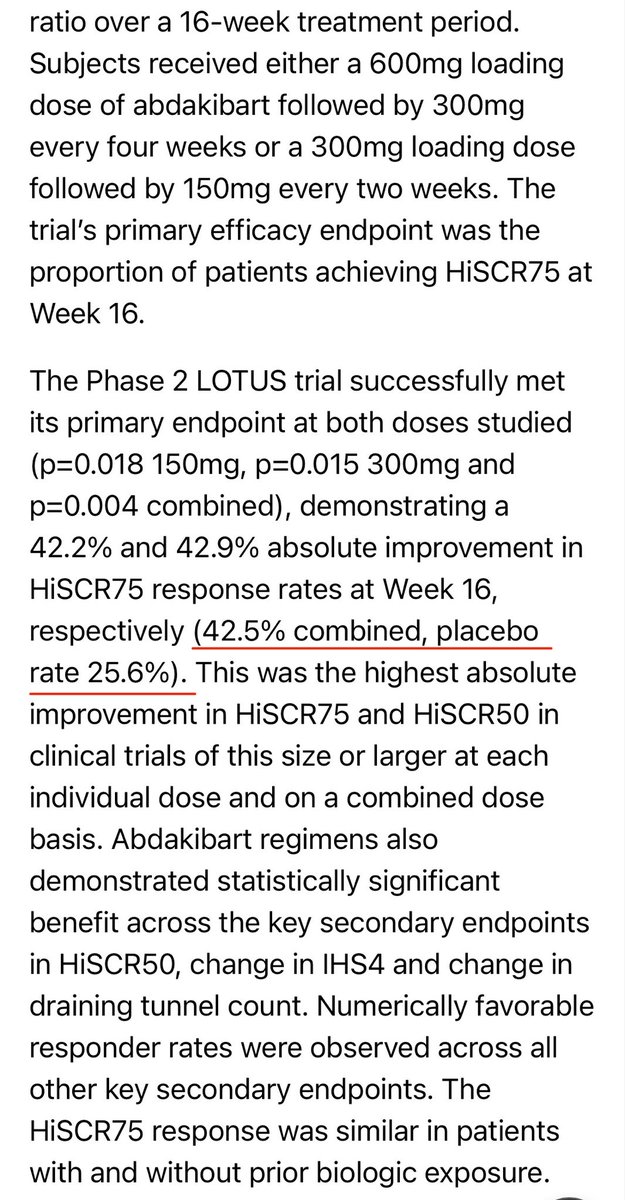
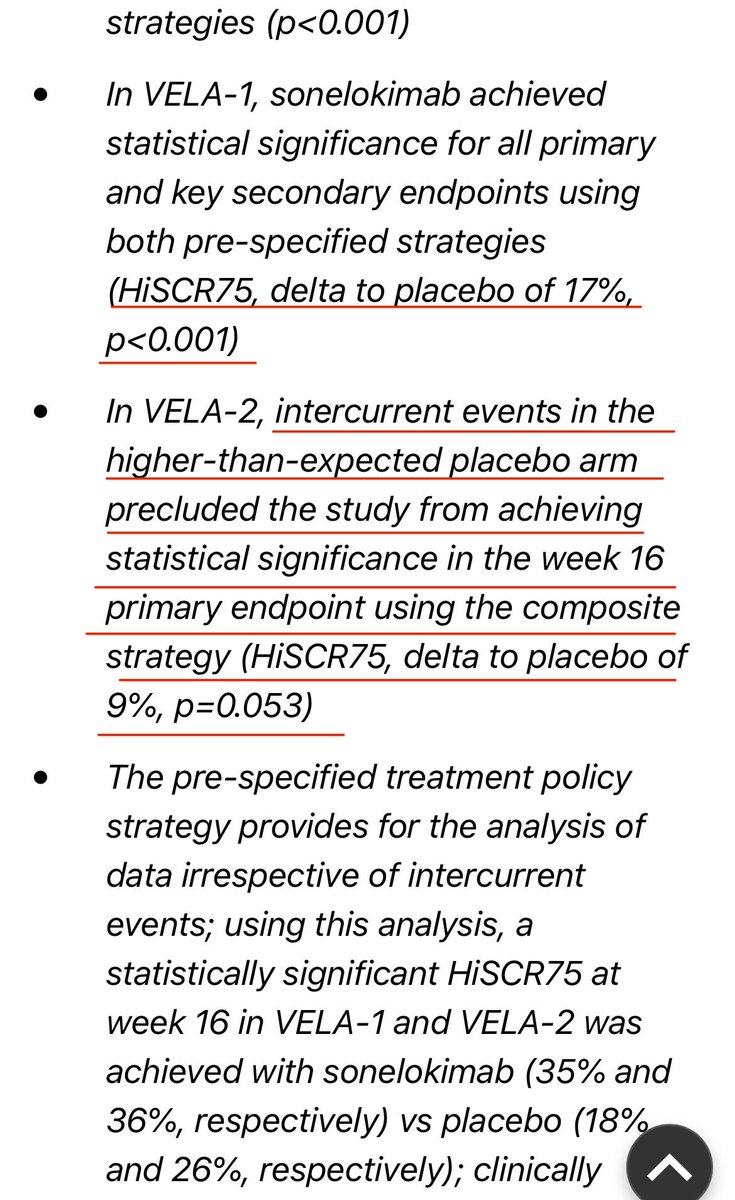
The 2 estimands seem very similar to traditional "intention to treat" analysis and "per protocol" analysis. But the language focuses on how intercurrent events such as non-adherence and use of protocol-prohibited drugs while on treatment might have affected the endpoints.
7
751

From ME Global Chronical
🩵 An extremely sad message 🩵
"Readers may remember the distressing story in 2014 of 14 yr old Mirjam Knapp of Germany. She had very severe ME and was subjected to an "Activation Regime" in hospital for 20 months, during which time her mother's parental rights were removed.
With the help of Save4Children Dr Nigel Speight was able to attend court in Germany and managed to get her freed to come home. You can read reports on this in issues 3–6 of the ME Global Chronicle (in which she was referred to as Joanne for security reasons: meglobalchronicle.wordpress.…, copy & paste)
She was much happier at home but her ME continued to be severe with her remaining bed bound and needing tube feeding.
Very sadly, possibly due to an intercurrent illness, she deteriorated and passed away recently at the age of 26. Right up until the last moment, Mirjam held onto hope that medical research would discover a way to heal her.
We are sure all readers will extend their warmest sympathy to her mother Christina and her family.”
Dr Nigel Speight
picture provided by Christina, the mother of Mirjam

6
5
40
1,492

At the Society of Clinical Trials (#SCT2026) conference last week, one of the topics being discussed was estimands & intercurrent events in cluster trials. Perfect timing for the publication of the new cRCT estimand framework 1/8
#MethodologyMonday #129
1
2
8
2,675

IMPUTATION BIAS. The protocol states that “missing data will not be imputed” but then specifies imputation in Table 9-1: “For participants with intercurrent events ‘b or c’, the participant will be assumed to have been infected with SARS-CoV-2” - withdrawals “before occurrence of the event for the primary endpoint” are treated as positive COVID-19 events. Imputing dropouts as positive may be reasonable in certain trials but does not make sense for a COVID-19 prophylaxis trial - e.g., consider if there were 5 events and 50 dropouts. Imputation could significantly alter the result. In this trial there were 22 treatment and 35 placebo dropouts (we do not know how many led to imputation).
HHC MISMATCH. The distribution of Randomized Household Contacts per Index Patient appears inconsistent. Table S1 shows that out of 1,319 Index Patients, 546 had ≥4 randomized HHCs, 275 had 3, 273 had 2, and 225 had 1. This indicates a minimum of (546*4) (275*3) (273*2) (225*1) = 3,780 randomized HHCs. However, the CONSORT diagram shows only 2,387 randomized HHCs.
HDL ADVERSE EVENT ASCERTAINMENT. Previous trials reported HDL decreases as the most common TEAE (>30% of patients). In this study, authors acknowledge a 27% median reduction in HDL on day 6 in the treatment group. The protocol specified that HDL-C results would be withheld from study sites/blinded personnel until unblinding because HDL-C decreases could reveal treatment assignment. Authors state that the changes are transient and are not a safety concern. We do not see evidence that HDL values were reported after unblinding and captured as adverse events. Therefore, the headline AE table may not fully account for treatment adverse effects.
Preliminary analysis - please report updates/corrections.
c19early.org/hayden2.html
1
4
337

2
10
3,154


Apr 15
Enhanced doubly robust estimation in clinical trials accounting for intercurrent events. Junyi Zhang, Ao Yuan, Chenguang Wang, Jing-Ou Liu, Ming T. Tan. Journal of Biopharmaceutical Statistics.tandfonline.com/doi/full/10.…
1
7
502
Mar 18
What Makes an Estimand Useful? Guidance on the Choice of Intercurrent Event Strategies. Brennan C. Kahan, Fan Li, Michael O. Harhay, Suzie Cro. Statistics in Medicine. onlinelibrary.wiley.com/doi/…
1
7
21
943
Mar 18
Commentary on Fleming et al. “A Perspective on the Appropriate Implementation of ICH E9(R1) Addendum Strategies for Handling Intercurrent Events.” Oliver Keene, David Wright, Christine Fletcher. Statistics in Medicine. onlinelibrary.wiley.com/doi/…
7
452

Children heavily infected with hookworms are likely to develop deficits in both physical and cognitive development and are more susceptible to other intercurrent infections.
Page 226 📕 Parasitic Diseases, Eighth Edition
Download a copy for free! parasiteswithoutborders.com/…

2
7
254

Mar 9
🧬 Obinutuzumab in Active Systemic Lupus Erythematosus
•Obinutuzumab is a glycoengineered type II anti-CD20 monoclonal antibody that produces potent B-cell depletion.
•It is already approved for lupus nephritis, but its role in non-renal active SLE has not been clearly established.
🧪 Study Design
•Phase 3, multicenter, double-blind, placebo-controlled trial
•303 adults with active SLE
•Excluded: proliferative or membranous lupus nephritis
•All patients continued standard background therapy
Randomization (1:1):
•Obinutuzumab 1000 mg
•Placebo
Dosing schedule
•Day 1
•Week 2
•Week 24
•Week 26
🎯 Primary Endpoint (Week 52)
SLE Responder Index-4 (SRI-4)
Defined as:
•≥ 4-point reduction in SLEDAI-2K
•No worsening in BILAG-2004
•No worsening in Physician Global Assessment
•No intercurrent events (rescue therapy, protocol violation, or early discontinuation)
📊 Results
•303 patients randomized
•151 received obinutuzumab
•152 received placebo
At week 52, an SRI-4 response occurred in 76.7% of patients receiving obinutuzumab compared with 53.5% in the placebo group.
•Adjusted difference: 23.1 percentage points
•95% CI: 12.5–33.6
•P < 0.001
In a sensitivity analysis excluding non-fatal intercurrent events, response rates were:
•85.4% with obinutuzumab
•68.5% with placebo
⭐ Key Secondary Outcomes
Obinutuzumab showed superiority for multiple clinically relevant outcomes:
•✔ BILAG-based Composite Lupus Assessment (BICLA) response
•✔ Sustained reduction in glucocorticoid dose
•✔ Sustained SRI-4 response
•✔ SRI-6 response
•✔ Longer time to first BILAG-defined flare
⚠ Safety
•Adverse events: 88.7% with obinutuzumab vs 81.5% with placebo
•Serious adverse events: 15.9% vs 11.9%
•Deaths during double-blind period: 1 with obinutuzumab and 3 with placebo
Overall, safety was consistent with the known profile of anti-CD20 therapy.
🧾 Conclusion
🧬 Obinutuzumab significantly improved disease activity in adults with active SLE without lupus nephritis, achieving higher response rates and better outcomes across all key secondary endpoints compared with placebo.
#RheumattDoc #MedTwitter #RheumTwitter #Medicine #rheumatology @DrAkhilX @IhabFathiSulima @CelestinoGutirr @DurgaPrasannaM1
1
17
56
2,597

The patient's presentations are a typically classic signs for Gilbert syndrome.
Triggers are usually fasting (reduced caloric intake), intercurrent illness, dehydration, or stress increase unconjugated bilirubin by reducing UGT1A1 activity further or increasing bilirubin load.
1
2
58

This pain is intermittent, relapsing, and intercurrent!
1
4
276

Teething can cause local gum inflammation, drooling, irritability, and sometimes a slight temperature rise (<38°C).
However, high fever (≥38.5–39°C), poor feeding, or lethargy should not be attributed to teething. These findings warrant evaluation for intercurrent infection (e.g., viral illness, otitis media, UTI).
Teething ≠ cause of significant fever.
4
915

Feb 22
Agree case balancing risks/benefits. If limited treatment options for bipolar, pts can also be v reluctant to stop. Once damage done, can be v difficult to manage even after stopped. AKI in setting of intercurrent illness & reduced oral intake - progressive CKD.
1
1
27

Before starting an SGLT-2 inhibitor, check whether the person may be at increased risk of diabetic ketoacidosis (DKA),if they:
Previous episode of DKA
Intercurrent illness
At risk of dehydration or volume depletion
Following a very low carbohydrate or ketogenic diet.
NICE 2026
1
8
24
1,486


Feb 4
Recurrent Diabetic Ketoacidosis in a 37-Year-Old Female with Insulin-Dependent Diabetes
Case By-Dr Sybal Noel Dbritto
Diabetologis,Nalasopara, Mumbai
Discussion in CME INDIA/RSSDI Group
A 37-year-old female patient was diagnosed with diabetes mellitus 2 years ago.
"No family history/ BMI - under weight. Was overweight before diagnosis. Lost weight over the period. USG- nothing significant- pancreas normal."
Analysis: Adds crucial details ruling out familial or pancreatic pathology. The weight loss supports progressive beta-cell failure, consistent with insulin-deficient states rather than typical type 2 progression.
She was initially managed with oral hypoglycemic agents (OHAs) but rapidly progressed to requiring insulin therapy due to poor glycemic control. Despite insulin treatment, her diabetes remains largely uncontrolled, with recurrent episodes of diabetic ketoacidosis (DKA), often precipitated by intercurrent illnesses such as gastrointestinal infections and urinary tract infections. These episodes have led to repeated hospitalizations with prolonged stays.
Additional history: No family history of diabetes. BMI currently underweight (was overweight before diagnosis, with subsequent weight loss over the period). USG abdomen shows nothing significant, with a normal pancreas.
Recent note: The patient has been uncontrolled for a long time, developing symptoms of hypoglycemia at blood sugars below 200 mg/dL, raising concerns about altered counter-regulatory mechanisms contributing to further hyperglycemia.
Key investigations:
Negative islet cell antibodies and negative GAD antibodies.
Markedly low C-peptide levels (0.04 ng/mL), indicating near-complete endogenous insulin deficiency.
This case was shared in the CME India AND rssdin group for discussion, highlighting challenges in classification and management of atypical diabetes phenotypes, particularly in patients presenting with ketosis proneness despite an initial type 2-like diagnosis.
Analysis of Comments
The discussion elicited diverse insights from group members, focusing on differential diagnosis, classification, and management. Below is a chronological and thematic analysis of all contributions, including an apparently unrelated initial comment on sweeteners (which may stem from a parallel thread but is included for completeness as per the query).
Dr. Abhay, Bilaspur : "History suggests type 1 but diagnosed too late hence negative GAD and islet cell antibodies."
Analysis: Highlights the possibility of late-onset type 1 diabetes, explaining negative autoantibodies due to delayed diagnosis. This aligns with considering autoimmune markers' temporal sensitivity but overlooks non-autoimmune etiologies.
Dr. N.K. Singh :
Provided a detailed summary: "This clinical picture is most consistent with severe insulin-deficient diabetes with a ketosis-prone phenotype, rather than classical type 2 diabetes mellitus. The early failure of oral hypoglycaemic agents, rapid progression to absolute insulin dependence, and recurrent diabetic ketoacidosis (DKA) strongly indicate profound β-cell dysfunction. The markedly suppressed C-peptide level (0.04 ng/mL) confirms near-complete endogenous insulin deficiency. The absence of islet cell antibodies and GAD antibodies makes classical autoimmune type 1 diabetes less likely, pointing instead toward idiopathic insulin-deficient diabetes, often referred to as ketosis-prone diabetes (KPD), A−β− subtype or type 1B diabetes. Intercurrent infections acting as frequent DKA triggers reflect extreme metabolic fragility, with minimal physiological reserve to counter stress-induced insulin resistance and counter-regulatory hormone surges. Overall, this represents a non-autoimmune, insulin-deficient diabetes with high DKA risk, requiring lifelong intensive insulin therapy, meticulous sick-day management, and aggressive infection prevention rather than treatment escalation typical of type 2 diabetes."
Next Post ...✍️

1
5
12
700
Jan 20
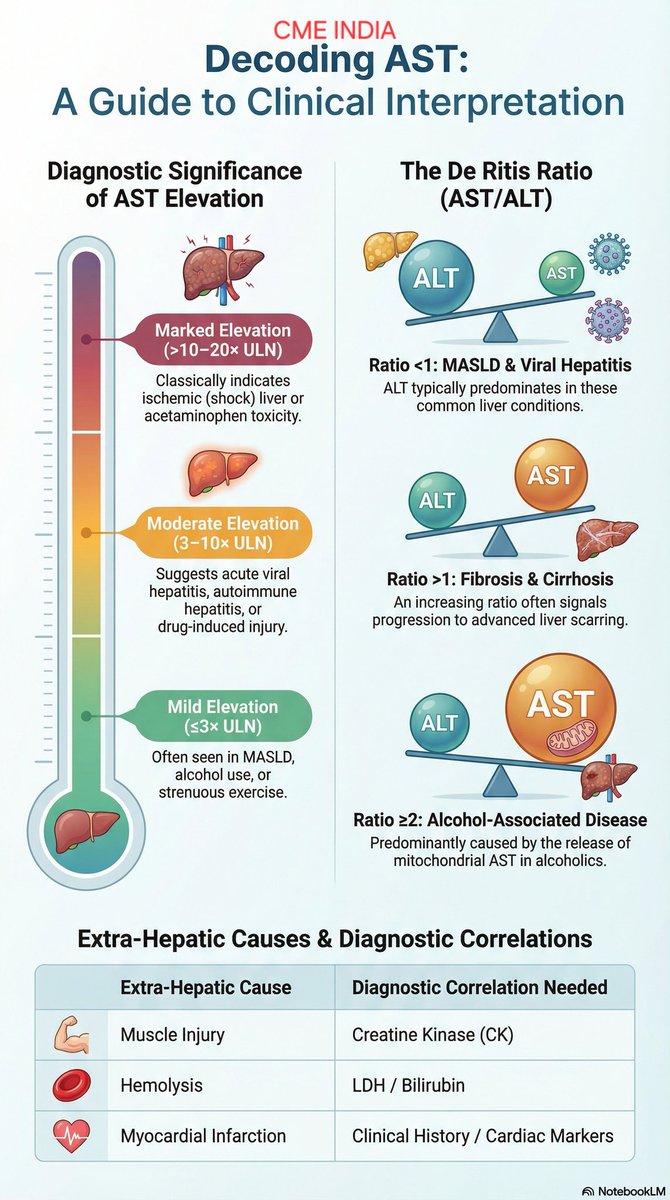
SGOT (AST) in Liver Function Tests: Clinical Significance
(CME INDIA)
Serum glutamic-oxaloacetic transaminase (SGOT), now termed aminotransferase (AST), is a transaminase enzyme present in both the cytosol and mitochondria of hepatocytes and in high concentrations in cardiac muscle, skeletal muscle, kidney, brain, and red blood cells. Hence, AST is a sensitive but relatively non-specific marker of hepatocellular injury.
AST elevation reflects cellular necrosis or membrane leakage but does not exclusively indicate hepatic origin.
Degree of Elevation – Diagnostic Implications
• Mild elevation (≤2–3 × ULN)
Seen in MASLD, alcohol use, chronic viral hepatitis, hypothyroidism, statin therapy, strenuous exercise, and muscle disorders.
• Moderate elevation (3–10 × ULN)
Suggests acute viral hepatitis, autoimmune hepatitis, evolving ischemic hepatitis, or significant drug-induced liver injury.
• Marked elevation (>10–20 × ULN)
Classically seen in ischemic (shock) liver, acetaminophen toxicity, acute viral hepatitis, severe autoimmune hepatitis, and massive hepatic necrosis.
AST vs ALT – De Ritis Ratio (AST/ALT)
This ratio provides crucial etiologic clues:
• AST/ALT <1 → MASLD, viral hepatitis (ALT predominant)
• AST/ALT >1 → Advanced fibrosis or cirrhosis
• AST/ALT ≥2 → Strongly suggestive of alcohol-associated liver disease (mitochondrial AST release)
• Very high AST with modest ALT → Ischemic injury, muscle breakdown, or hemolysis
Extra-Hepatic Causes of Raised AST (Key Pitfall)
Because AST is widely distributed:
• Myocardial infarction
• Myositis, rhabdomyolysis, strenuous exercise
• Hemolysis
• Hypothyroidism
• Macro-AST (benign persistent elevation)
Always correlate with:
ALT
CK / LDH
Clinical context
Important Clinical Pearls
• AST is less liver-specific than ALT and should never be interpreted in isolation.
• Mitochondrial AST predominance explains high AST in alcoholic liver disease.
• Rising AST with falling ALT may indicate progression to advanced fibrosis or cirrhosis.
• Normal AST does not exclude chronic liver disease.
• Disproportionately high AST with normal bilirubin may point to muscle or cardiac pathology rather than liver disease.
Interpretation in the Present LFT Context
Reported SGOT (AST): 51.6 U/L (mild elevation)
With:
Normal ALT (29.5 U/L)
Predominantly indirect hyperbilirubinaemia
Normal ALP
This pattern suggests: • Mild hepatocellular stress, or
• Non-hepatic AST source, or
• Early/resolving hepatic injury
Alcohol use, muscle injury, hemolysis, or Gilbert’s syndrome with intercurrent stress should be considered.
Take-Home Message
AST is a sensitive but non-specific marker of hepatocellular injury. Its greatest diagnostic value lies in interpretation alongside ALT and the AST/ALT ratio, which provides powerful clues to alcohol-related disease, fibrosis, and ischemic injury.
2
67
220
8,832

Jan 17
Also we should understand that
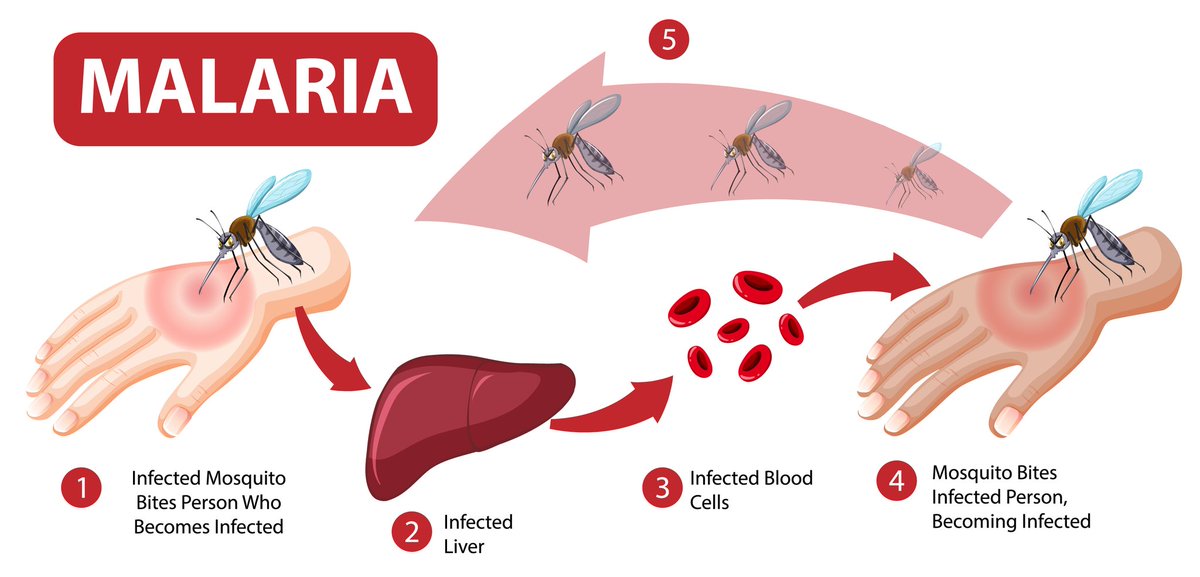
After a person is infected with Plasmodium parasites through the bite of an infected mosquito, the parasites first migrate to the liver, where they undergo an incubation period (typically 7–14 days, depending on the species). During this hepatic phase, the parasites multiply and develop into tissue schizonts, which later rupture to release merozoites into the bloodstream.
These merozoites are the infective blood-stage forms that invade red blood cells, digest haemoglobin (globin), multiply further, and cause the classical symptoms of malaria such as fever, headache, malaise, chills, and body pain.
In some malaria species, most notably Plasmodium vivax and Plasmodium ovale a proportion of liver-stage parasites do not immediately mature. Instead, they remain dormant in the liver as hypnozoites (often mistakenly referred to as “dormant schizonts”). These dormant forms can reactivate weeks or even months later, causing relapse, even in the absence of a new mosquito bite.
Most conventional antimalarial treatments, including many artemisinin-based combination therapies (ACTs), primarily target the blood-stage parasites (merozoites). This is logical because these forms are responsible for the symptoms that bring patients to the clinic. However, standard ACTs do not eliminate dormant liver forms (hypnozoites).
This explains why some individuals experience recurrent malaria episodes after apparently successful treatment. Factors such as stress, reduced immunity, intercurrent illness, or alcohol consumption may coincide with relapse, leading people to believe these factors “caused” the malaria, when in reality they triggered the reactivation of dormant parasites.
ACTs combine a fast-acting artemisinin derivative (artemether, artesunate, dihydroartemisinin, etc.) with a longer-acting partner drug. These partner drugs remain in the bloodstream after the artemisinin component has been cleared and help eliminate residual blood-stage parasites.
However, most ACT partner drugs do not effectively target liver hypnozoites.
It is important to clarify that hypnozoites are not formed by Plasmodium falciparum. Dormant liver-stage hypnozoites are a defining feature of P. vivax and P. ovale infections.
However, Plasmodium falciparum may persist at very low levels in the blood, sometimes described as drug-tolerant or persister ring-stage parasites, which can lead to recrudescence (not true relapse), particularly if blood-stage clearance is incomplete after treatment.
Crucially, only the 8-aminoquinoline class of antimalarials, notably primaquine and tafenoquine has proven activity against dormant liver hypnozoites. These drugs are essential for achieving radical cure and preventing relapse in P. vivax and P. ovale infections.
Because of persistent or recurrent infections, some clinicians use adjunct antimalarial agents, such as:
Sulfadoxine–pyrimethamine (Fansidar)
Doxycycline
Clindamycin
Atovaquone–proguanil
These agents help suppress or clear blood-stage parasites and improve treatment efficacy, but they do not reliably eliminate dormant liver hypnozoites, further underscoring the importance of 8-aminoquinolines for true relapse prevention.
Key points to note:-
Relapse—hypnozoites (P. vivax, P. ovale)
Recrudescence—persistent blood-stage parasites (P. falciparum)
Jan 15

WHY YOUR MALARIA TREATMENT ISN'T WORKING
If you treat malaria every 1-2 months and the symptoms keep coming back, there's a problem.
It could be a wrong diagnosis, incomplete treatment, or reinfection.
Let's talk about them👇
15
35
2,542