
Jun 11
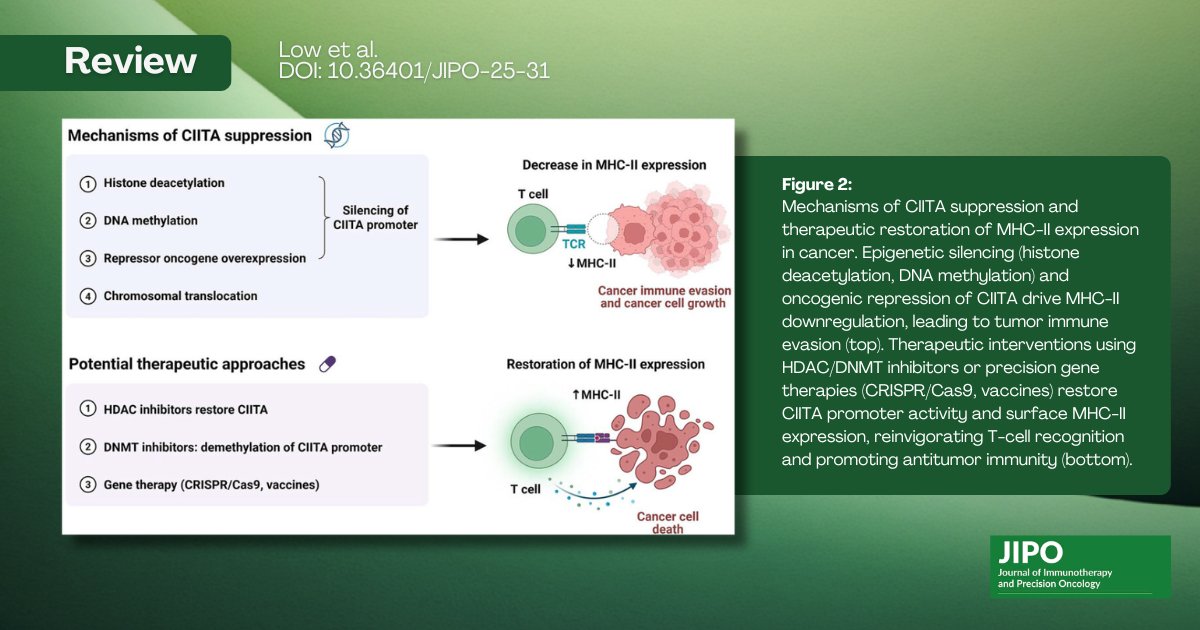
Recent #JIPO review by Low et al. explores "CIITA: A Master MHC-II Regulator Impacting Cancer and Beyond" doi.org/10.36401/JIPO-25-31 #CIITA #MHCII #immunoregulatory @OncologyNetwork #cancer #oncology #cancerawareness #cancerresearch #cancercare #oncology
31

May 30
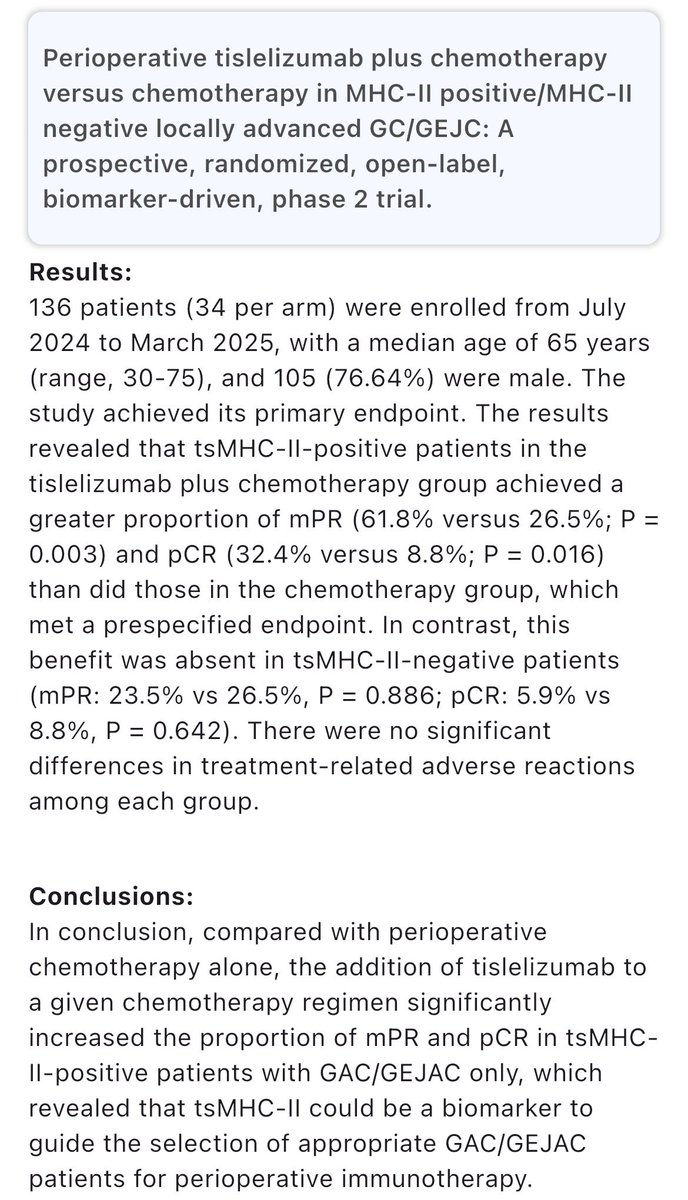
🧪Perioperative tislelizumab ChT in gastric cancer
phase II biomarker study #ASCO26
❗️Tisle benefit is only in "tumor specific MHCII positive" patients
🤔As other targets (HER2, claudin) may shift to periop in future, biomarkers other than PDL-1 may be needed for IO
#cancer #oncology #MedX #GI #gastric @OncoAlert
7
15
878

May 8
As we age, the immune system can become both weaker and more inflammatory.
Existing explanations of immune aging often look at thymic shrinkage and T-cell-intrinsic dysfunction, leaving the aged immune environment underexplained.
We funded Saad Khan @SaadKhan_Imm through @ImpetusGrants to work on this thread. He asked what happens when aged mice lose either B cells or specific B cell signals tied to insulin sensing and antigen presentation - and identified an InsR–B cell–MHCII axis linking metabolic sensing in B cells to CD4 T cell aging.
Aged mice lacking B cells kept more naive CD4 T cells and showed less inflammatory, exhausted, clonally restricted T cell aging.
When the authors disrupted B cell insulin receptor signaling or B cell MHCII, the CD4 T cell compartment again shifted toward a less immunosenescent state. B cell deficiency was also linked to better frailty/metabolic measures and a 36.3% median lifespan increase in mice.
The reusable insight is an InsR–B cell–MHCII axis that connects metabolic sensing to adaptive immune aging.
On our map of the field’s bottlenecks, this sits at immune aging/adaptive immune dysfunction, preclinical mechanism and target-validation stage.
Read it here: science.org/doi/10.1126/scii…


1
15
49
7,846

Apr 27
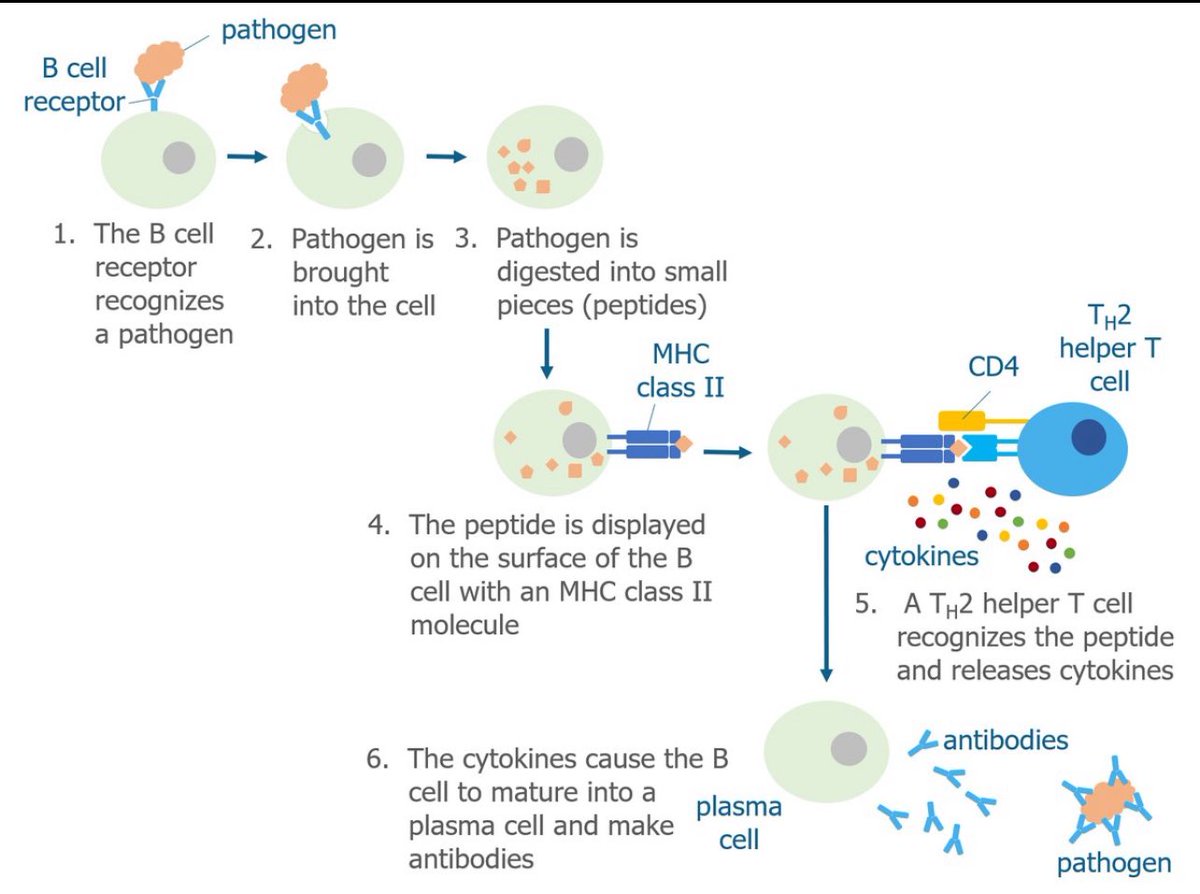
كيف تفرز خلايا (B) الأجسام المضادة⁉️
المقادير: جسم غريب,MHCII, خلايا T المساعده و TCR, B
الطريقه.
1⃣ تلتهم خلايا B الجسم الغريب وتعرضه على سطحها مع MHCII
2⃣ تجي خلايا T المساعده تتعرف عليه عن طريق TCR
3⃣ بعدهاتفرز CYTOKINES اللي تحول B الى خلايا PLASMA اللي تفرز الأجسام المضادة.
1
11
69
2,579

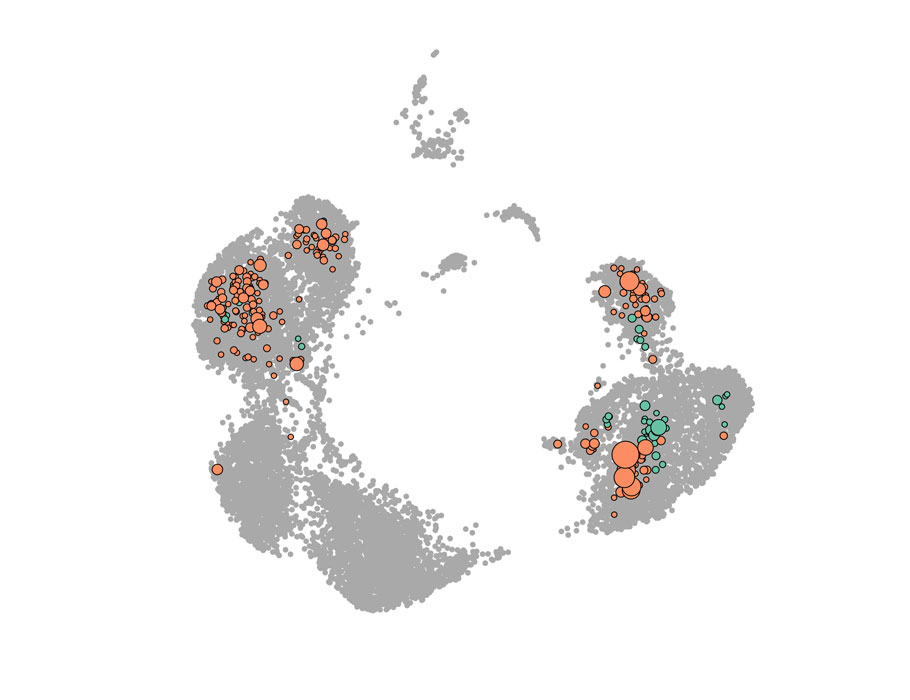
Our #singlecell of pre/post-pembro HNSCC tumors is out in @CellRepMed! An MHCII/IFN program predicts ICI response pre-tx and likely reflects engagement between malignant cells/T-cells. Congrats to Michael Mints in @TiroshLab, @ReillyAlexS, and @Asp2145! cell.com/cell-reports-medici…
7
9
37
3,665

Apr 5
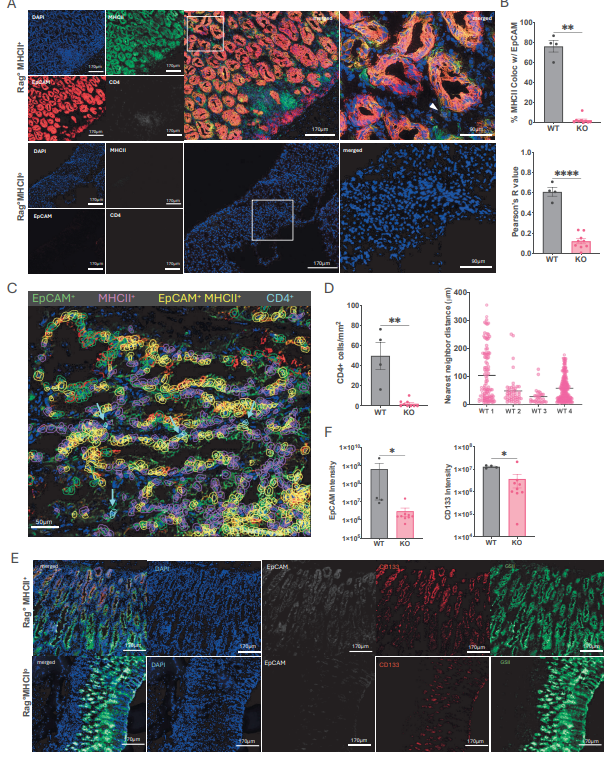
@biorxivpreprint A critical role of epithelial MHCII in initiation of autoimmune tumorigenesis and sustaining premalignancy growth in the stomach
biorxiv.org/content/10.64898…
2
15
1,129

A critical role of epithelial MHCII in initiation of autoimmune tumorigenesis and sustaining premalignancy growth in the stomach biorxiv.org/content/10.64898… #biorxiv_immuno
1
4
736

A new Science #Immunology study in mice suggests that #aging B cells can promote age-related CD4 T cell changes and functional decline via #insulin receptor signaling and #MHCII engagement. scim.ag/4rl46mf
2
13
42
2,678

31 Dec 2025
While islet amyloid harms β cells in T2D, research from @UBC and @BCCHresearch by @hDenroche @BruceVerchere reveals amyloid protects against β cell autoimmunity and diabetes in NOD mice by disrupting MHCII antigen presentation in islet macrophages link.springer.com/article/10… 🔓
2
11
879

25 Dec 2025
What, I was completely oblivious that smell may be related to MHCII, that's really cool
2
616

18 Dec 2025
IFNγ-Induced PD-L1 MHCII Macrophages and Tim-3 Tumor-Reactive CD8 T Cells Predict a Response to Anti–PD-1 Therapy in Tumor-Bearing Mice doi.org/10.1158/2326-6066.CI…
4
219

4 Nov 2025
Byrne’s group (Cancer Immunology Research) shows CD4⁺ T cells mediate rejection of MHC-deficient pancreatic tumors after anti-CD40 dual ICB.
CD4 (not CD8)T cells drive it, reprogramming MHCII⁺ stromal & endothelial cells for tumor control. aacrjournals-org.proxy.libra…
1
4
50
3,530

30 Oct 2025
Now out in @jclinicalinvest ! MHCII expression by tumor cells is critical for response to targeted therapy!!
Tweetorial incoming 👇
30 Oct 2025

Little progress has been made in the treatment of anaplastic thyroid cancer
@VeraTiedje @Gnana_Krish et al. @MSKCancerCenter now find mice with aggressive ATC respond to the inhibitor combination dabrafenib/trametinib by affecting cancer cell MHCII expression & increasing T-cell infiltration.
jci.org/articles/view/191781
The image shows multiplex immunofluorescence for immune cell populations in the tumor microenvironment of thyroid cancers.

10
4
13
3,006

30 Oct 2025
Little progress has been made in the treatment of anaplastic thyroid cancer
@VeraTiedje @Gnana_Krish et al. @MSKCancerCenter now find mice with aggressive ATC respond to the inhibitor combination dabrafenib/trametinib by affecting cancer cell MHCII expression & increasing T-cell infiltration.
jci.org/articles/view/191781
The image shows multiplex immunofluorescence for immune cell populations in the tumor microenvironment of thyroid cancers.
3
13
5,267

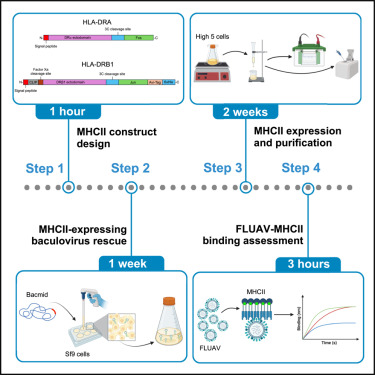
🧬 New in STAR Protocols: A step-by-step guide to measure MHC class II–Influenza A virus binding kinetics using biolayer interferometry!
🔹 Produce dimeric MHC II via baculovirus
🔹 Screen FLUAV–MHCII interactions
🔹 Quantify whole-virus affinity
👉 doi.org/10.1016/j.xpro.2025.…
6
272

11 Sep 2025
This may explain why Scott saw so many of his patients die.
He did not know the difference b/w a vax that uses extracellular injection and MHCII pathways vs. mRNA VAX that uses intracellular infection all 210 cell types and uses MHCI / Cytotoxic T-Cell cell killing.
The rules for the first type do not apply to the second.
Examples:
1) Immune Response Timeline Status Mortality:
The speed and severity of mRNA infected cell killing is dependent on the number of T-Cells present, in turn dependent on your last antigen exposure and if you are on primary or secondary immune response timelines.
Administering mRNA VAX at the wrong time (high T-Cell count times) would cause horrendous self-cell killing, particularly in the cardiovascular system where LNP/mRNA enters first,— resulting in eventual death.
How would you even know to check for this, and avoid it, if you don't know how mRNA VAX works?
2) Covid Infection / Body Mass Status
mRNA VAX mortality would mechanistically also be associated with the percentage of systemic cell killing experienced.
If you have a covid infection, you already have ACE2 cells infected, adding an mRNA infection can push that into lethal burden, particularly for lower body cell mass patients (because of the "one size fits alls" mRNA dose).
Again, if you don't know how mRNA VAX works, how would you know to avoid lethal burden ?
3) Metabolic Activity Level - Immune System Destruction
LNP internalization is dependent on the metabolic activity level of the cell (per Grok).
If you are on the upslope of a secondary immune response timeline, readily infecting B and T-cells would effectively wipe out your immune response capability (i.e. death in critical care situations).
Again, if you don't know how mRNA VAX works, how would you know to avoid this?
1
2
146
27 Jul 2025
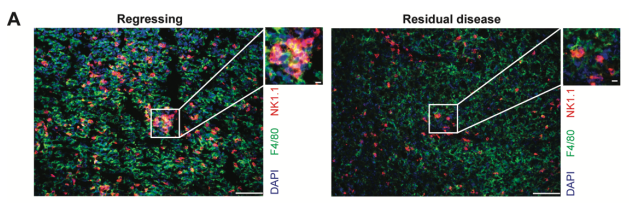
Preprint: A unique macrophage subset (F4/80hiCCL5 MHCII CD63 ) orchestrates NK cell recruitment through CCR2/5 during tumor regression, is perturbed in Ptpn22-dependent manner in resistance to therapy and residual disease @CindyChiaHsinH1 @ZhongYinZhang1
biorxiv.org/content/10.1101/…
1
5
41
2,780

27 Jul 2025
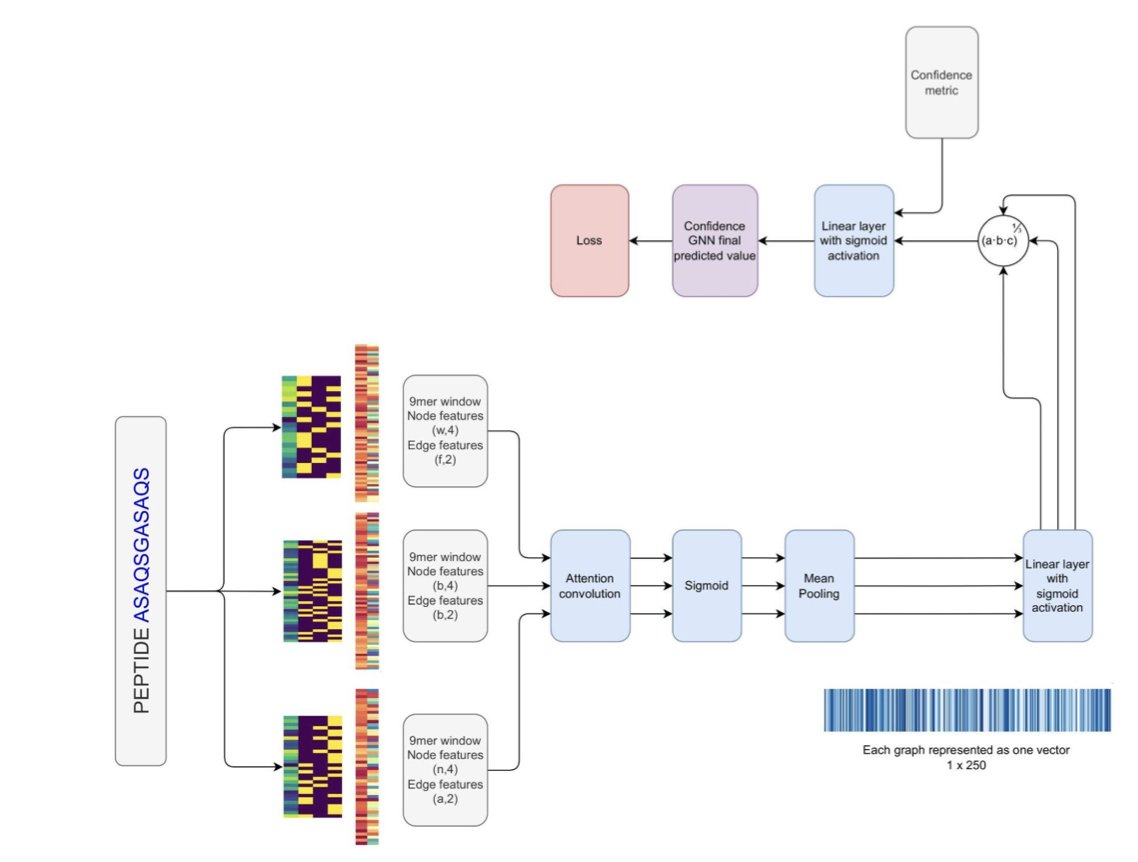
Learned Geometry, Predicted Binding: Structurally-Based Prediction of Peptide:MHC Binding Using AlphaFold 3 Enables CD4 T Cell Epitope Prediction
1. A groundbreaking study introduces MHCIIFold-GNN, a novel approach combining AlphaFold 3, a highly-multiplexed peptide:MHCII binding assay, and transfer learning with Graph Neural Networks to predict CD4 T cell epitopes with state-of-the-art accuracy.
2. The study leverages AlphaFold 3 to generate structural representations of peptide:MHCII complexes, which are then processed by a Graph Neural Network trained on in vitro binders. This method achieves comparable performance to existing non-structural models that rely on much larger datasets.
3. The researchers developed a highly-multiplexed peptide:MHCII binding assay called MHCII-PepSeq, which identifies binding peptides across diverse MHC II proteins. This assay generated a new dataset of 1,615 epitopes across 16 HLA-DR proteins.
4. The study demonstrates that combining MHCIIFold-GNN with a leading non-structural method (NetMHCIIpan 4.3) results in a significant performance boost, highlighting the orthogonal nature of the structural and non-structural approaches.
5. The zero-shot confidence metric derived from AlphaFold 3's pLDDT scores alone achieves competitive results with NetMHCIIpan 4.3, underscoring the biological relevance of structural confidence in peptide:MHC binding prediction.
6. The authors propose that using AlphaFold 3 as a foundation model to extract structural features for downstream tasks can significantly enhance prediction accuracy even with limited training data, paving the way for future advancements in precision immunology.
📜Paper: biorxiv.org/content/10.1101/…
#AlphaFold #GraphNeuralNetworks #StructuralBiology #Immunology #CD4TEpitopePrediction
17
1,915
27 Jul 2025
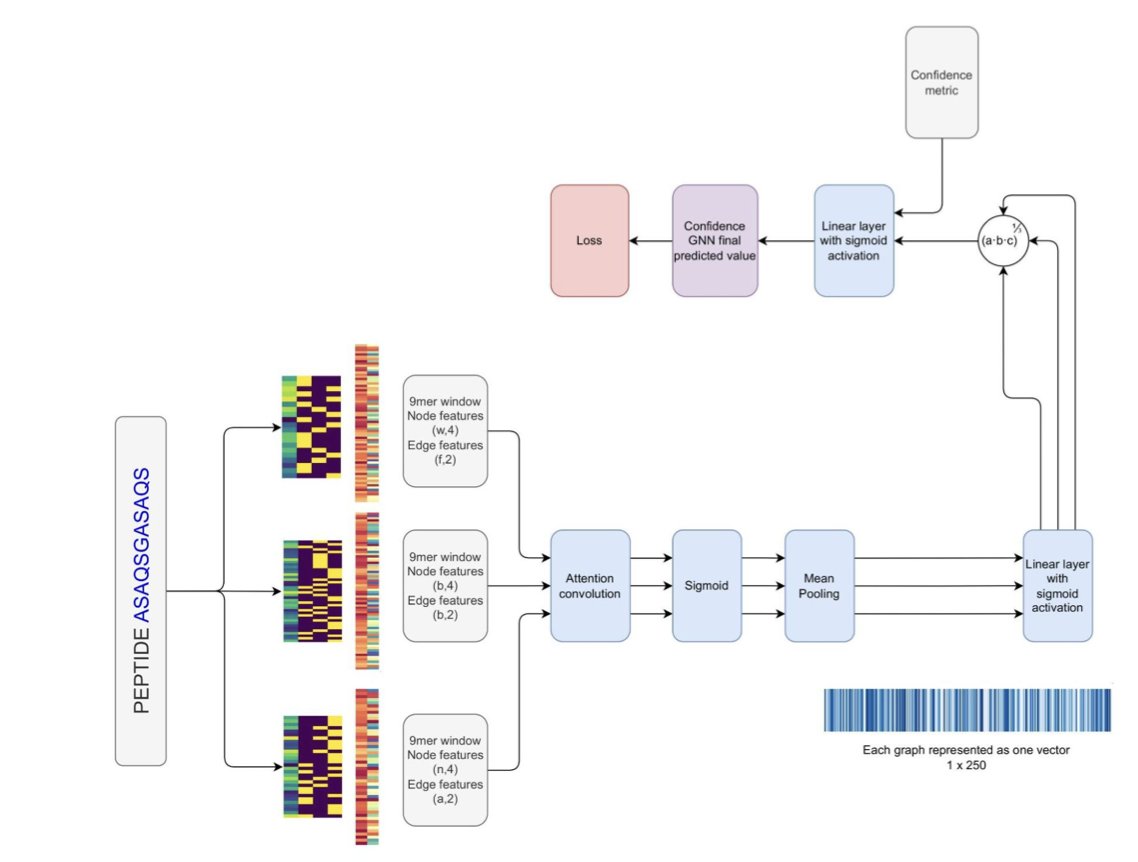
Learned Geometry, Predicted Binding: Structurally-Based Prediction of Peptide:MHC Binding Using AlphaFold 3 Enables CD4 T Cell Epitope Prediction
1. A groundbreaking study introduces MHCIIFold-GNN, a novel approach combining AlphaFold 3, a highly-multiplexed peptide:MHCII binding assay, and transfer learning with Graph Neural Networks to predict CD4 T cell epitopes with state-of-the-art accuracy.
2. The study leverages AlphaFold 3 to generate structural representations of peptide:MHCII complexes, which are then processed by a Graph Neural Network trained on in vitro binders. This method achieves comparable performance to existing non-structural models that rely on much larger datasets.
3. The researchers developed a highly-multiplexed peptide:MHCII binding assay called MHCII-PepSeq, which identifies binding peptides across diverse MHC II proteins. This assay generated a new dataset of 1,615 epitopes across 16 HLA-DR proteins.
4. The study demonstrates that combining MHCIIFold-GNN with a leading non-structural method (NetMHCIIpan 4.3) results in a significant performance boost, highlighting the orthogonal nature of the structural and non-structural approaches.
5. The zero-shot confidence metric derived from AlphaFold 3's pLDDT scores alone achieves competitive results with NetMHCIIpan 4.3, underscoring the biological relevance of structural confidence in peptide:MHC binding prediction.
6. The authors propose that using AlphaFold 3 as a foundation model to extract structural features for downstream tasks can significantly enhance prediction accuracy even with limited training data, paving the way for future advancements in precision immunology.
📜Paper: biorxiv.org/content/10.1101/…
#AlphaFold #GraphNeuralNetworks #StructuralBiology #Immunology #CD4TEpitopePrediction
1
974
20 Jul 2025
Dr. M, thanks, what a relief !
Makary will never understand the science of why mRNA VAX is a bad idea.
Any way to set new FDA Vaccine Approval Guidelines as a work around ?
Example:
1) For future vaccines, FDA will only approve biologically inactive viral protein fragments, that evoke an immune response via MHCII pathways, and without any other biological activity.
2) FDA will not approve any mRNA vaccine that:
a) codes for a protein other than as defined above,
b) uses a non-cell specific delivery system, and
c) if a cell specific delivery system is proposed, it must be proven to only internalize into one cell type, and a justification provided as to why that cell type will not be missed when it is killed via MHCI pathways of your immune system.
3) No adjuvants, other than saline, will be approved without safety data.
2
5
1,315