
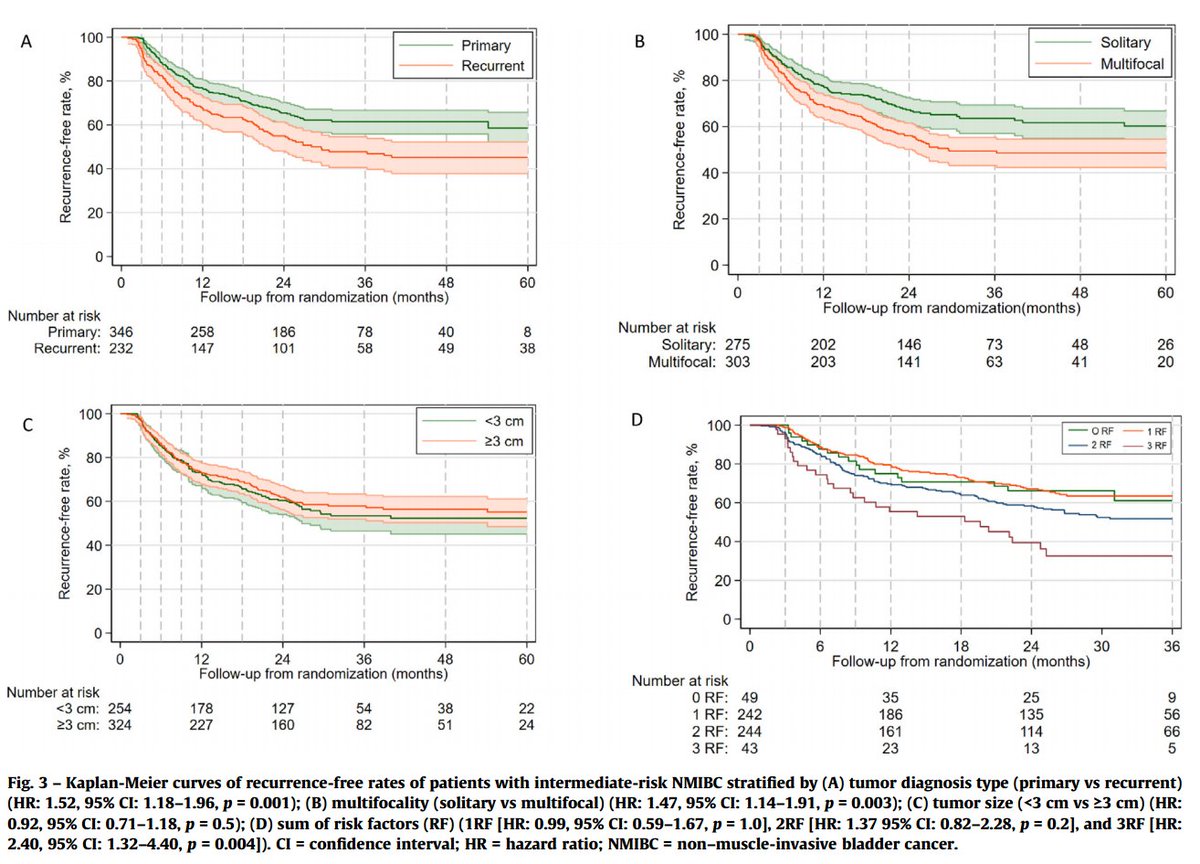
On multivariable analysis, three factors independently predicted recurrence:
-- Prior recurrence: HR 1.75 (p=0.008)
-- Multifocality: HR 1.49 (p=0.004)
-- Grade G2 vs G1: HR 1.57 (p=0.018)
One factor that did NOT predict recurrence:
-- Tumor size: HR 1.08 (p=0.6)
1
2
13
1,192

Jun 7
Atypical imaging features include hypovascularity, marked cystic degeneration, prominent calcification, tumor thrombus, and multifocality.
5
1,024
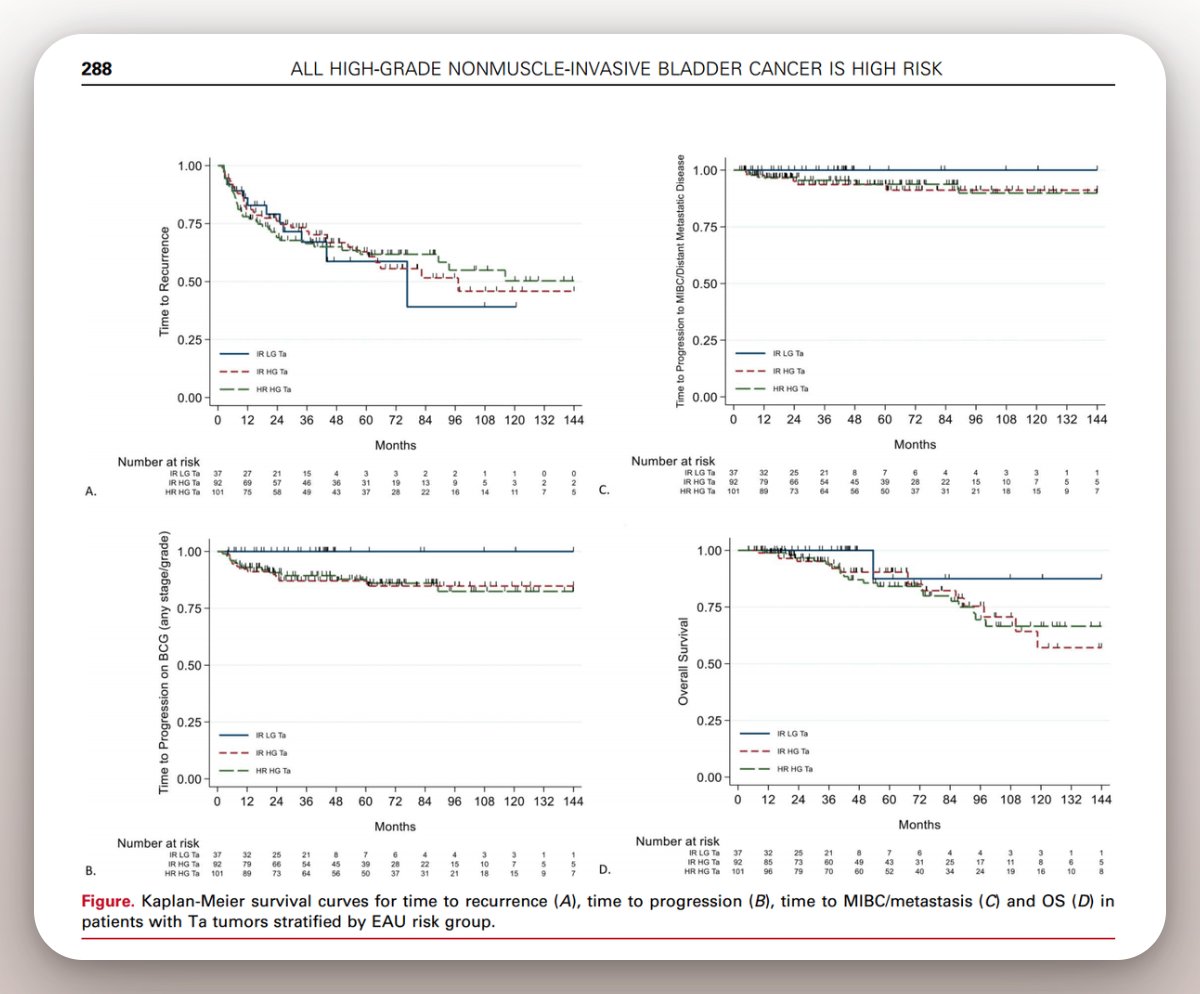
Our @JUrology paper looked at 251 patients with TaHG tumors. All treated with adequate BCG. We stratified them by risk groups - "intermediate-risk" vs "high-risk" - based on clinical factors like tumor size, age, multifocality.
All TaHG tumors behaved the same: BCG unresponsiveness: 14% vs 13%
Stage progression: 13% in both groups.
MIBC or metastasis: 6.5% vs 5.9%.
Multicenter cohorts and AI-based pathology studies have since shown the same thing: the clinical factors used to downgrade TaHG to intermediate risk do not meaningfully discriminate outcomes.
Once a Ta tumor is high grade, the biology drives the behavior. #BladderCancer #ASCO26 #OncSurgery @KKBree
3
7
27
3,449

Apr 16
the multifocality and atrophic gastritis argues for type 1 or 4 depending on PPI use and final path.. if final path does not confirm ateophic gastritis and no PPI use, I would err on getting scans for surveillance especially with G2 and nornal gastrin.
It is not completely fitting in one bucket but at that time going more into type 3 category
1
1
2
298

Apr 14
@IBCG_BladderCA Recommendations for intermediate-risk #NMIBC definitions and management. @UrogerliMD @MoffittNews joins @UroDocAsh @MDAndersonNews outlining International Bladder Cancer Group guidance that redefines intermediate-risk NMIBC as strictly low-grade disease with added risk features such as recurrence, multifocality, size >3 cm, or low-grade T1. In this framework, patients with 0–1 risk factor may be managed with active surveillance, whereas those with ≥3 risk factors warrant intravesical BCG given validated progression risks near 8%, and routine re‑staging TURBT or muscle sampling is generally unnecessary in low-grade tumors. #WatchNow > bit.ly/3Oh2b3Z
9
15
1,863

Apr 13
Metastatic Liver Carcinoma (MLC). A pathology specimen of the liver shows hepatomegaly and distortion of liver anatomy under the burden of tumor foci, indicating multifocal Metastatic Liver Carcinoma. The liver is infiltrated by cancer foci with umbilicated nodules of pale, circular masses with a dip. "Umbilication" is a hallmark sign of metastatic tumors, as they indicate rapidly growing tumors where the center outgrows the tumor's blood supply and undergoes necrosis. Umbilication occurs due to central indentation with the "navel" shape with central necrosis, fibrosis, and contraction of tumor mass. Multifocality is another pathognomic sign of metastasis, with the presence of numerous distinct nodules scattered throughout the liver, vs. primary hepatocellular carcinoma. Metastatic liver carcinoma, or secondary liver cancer places the primary cancer at Stage IV. Metastasis to the liver is mostly derived from adenocarcinoma of the body of the pancreas. Other primary malignancies that metastasize to the liver arise from the pancreas and GI tract via portal vein, colon/rectum, breasts, endometrium, ovaries, lung, kidneys, bladder, and prostate cancers. The massive blood supply in the liver and its primary role as a filtration system arriving from the digestive tract, makes the liver a common site for cancer metastasis. Small emboli are trapped in portal vein branches and metastasis occurs via detachment of cancer cells from primary tumor sites and their proliferation and transmission via hematogenous and lymphatic spread facilitated by the process of intravasation. Ddx. Hepatocellular carcinoma, multiple hepatic cysts, and hepatic hemangioma.
2
8
2,434

Mar 23
OVARIAN CANCER- We should learn from early lesions. Ovarian cancer is multifocal and multicentric.
The patient illustrated here has an early high-grade serous carcinoma with small tumors involving ovaries, fallopian tubes, and uterine serosa.The images included are from the uterine serosa. Six small foci of tumor cells are seen in the submesothelial space, mainly deep, very close to the myometrium. A clear example of multifocality. There is no lymphovascular invasion, and there is no involvement of the mesothelium. In my opinion, the best explanation is that the small groups of tumor cells developed in the stroma of the submesothelial space due to mesenchymal-epithelial transformation, as classical examples of independent primaries and multicentricity. I challenge anyone to offer a reasonable, different opinion that makes sense, and can be proven with images like these.
Better explained in the book Fere Ex Nihilo, Chapter 7
1
6
25
1,448
Mar 23
@IBCG_BladderCA Recommendations for intermediate-risk #NMIBC definitions and management. @UrogerliMD @MoffittNews joins @UroDocAsh @MDAndersonNews outlining International Bladder Cancer Group guidance that redefines intermediate-risk NMIBC as strictly low-grade disease with added risk features such as recurrence, multifocality, size >3 cm, or low-grade T1. In this framework, patients with 0–1 risk factor may be managed with active surveillance, whereas those with ≥3 risk factors warrant intravesical BCG given validated progression risks near 8%, and routine re‑staging TURBT or muscle sampling is generally unnecessary in low-grade tumors. #WatchNow > bit.ly/3Oh2b3Z
1
13
42
3,101

Mar 18
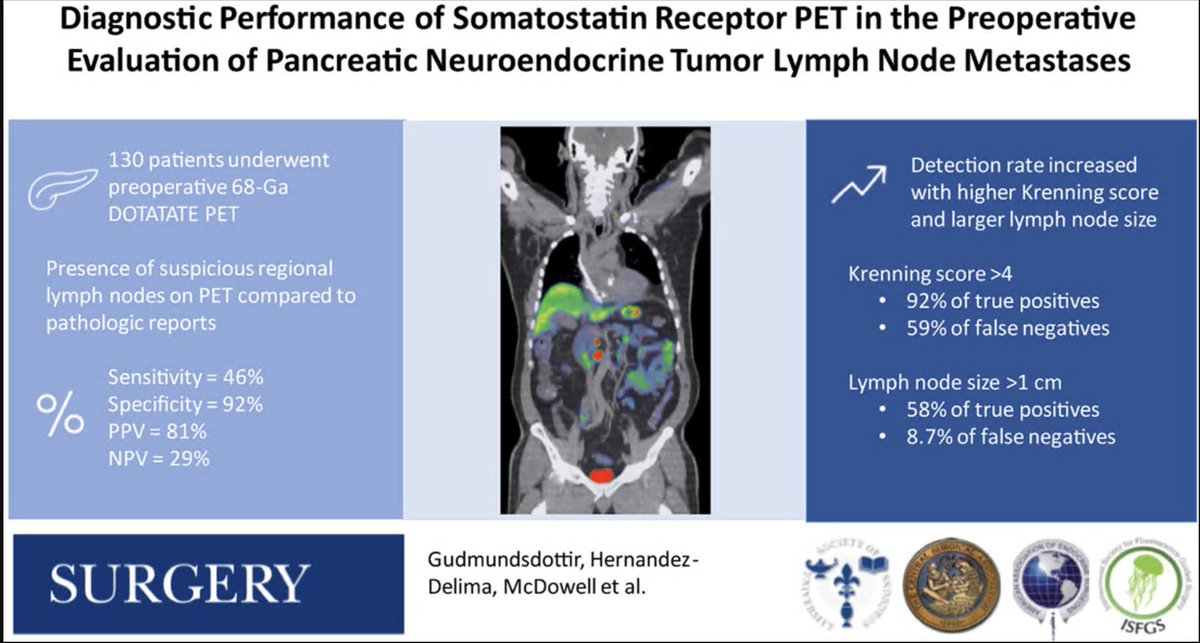
How does somatostatin PET perform in detecting nodal metastases in patients with pancreatic NETs evaluated for resection? Not so great...
130 patients w/ pNETs who all had SSTR PET followed by resection. 42% had path proven LN mets but only 24% were seen preop on PET (sensitivity 46%). Specificity much better, 92% with PPV of 81% and NPV of only 29%.
As expected, larger nodes and a higher Krenning score were more likely to be found on SSTR PET.
Be careful with multifocal pNETs such as in MEN1 as multifocality can resemble nodal mets.
@TELL_Starlinger @ThielsCA @PackardAnnie @MayoRadiology @MayoClinicSurg @MayoCancerCare @MayoHemeOnc
sciencedirect.com/science/ar…
1
12
32
2,119

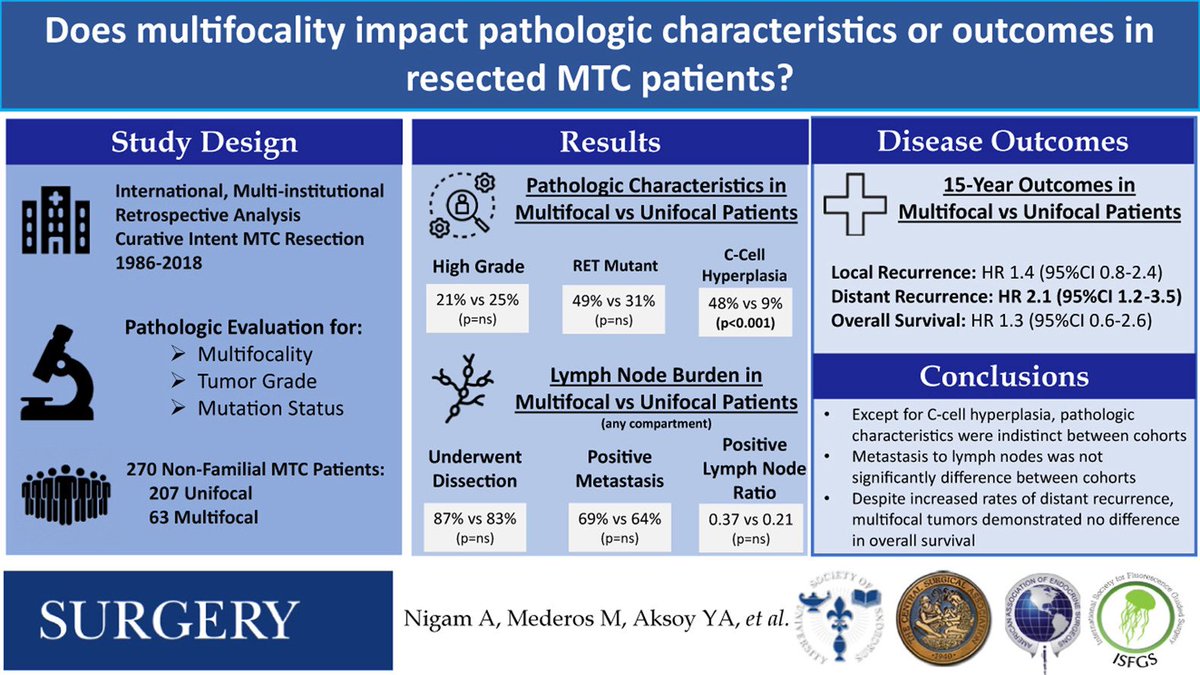
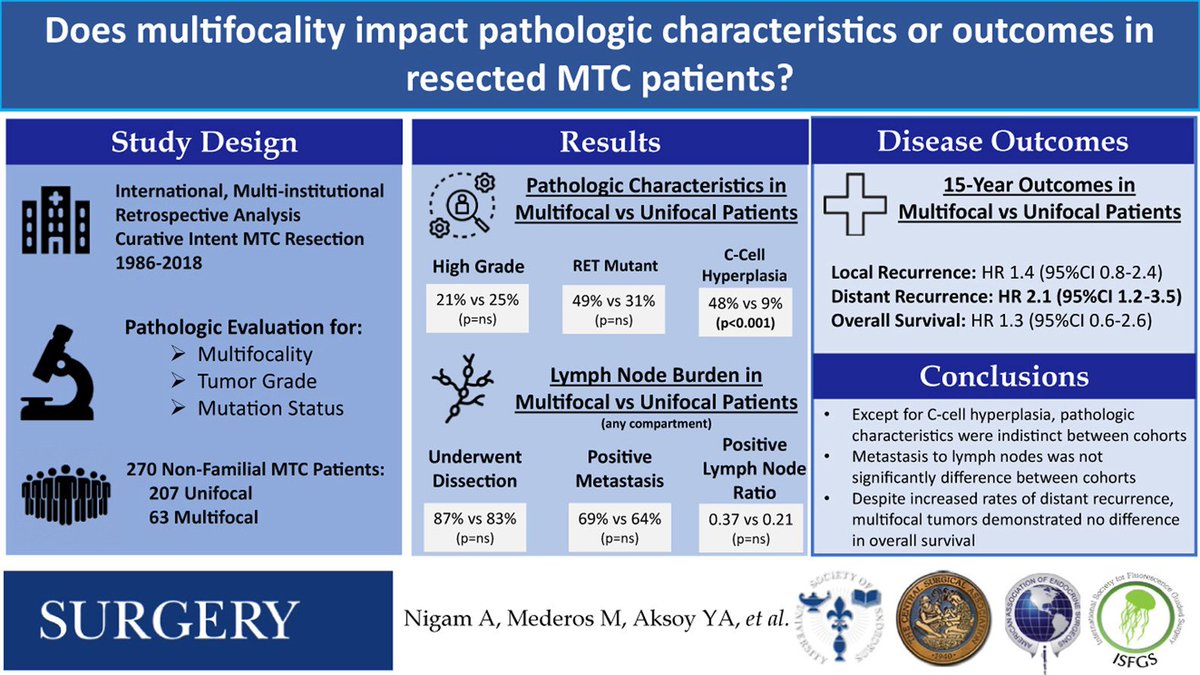
Nigam et. al. address the question, "Does multifocality impact pathologic characteristics or outcomes in resected MTC patients?" Published in January edition of @SurgJournal
buff.ly/JMipGU4

1
5
391

Feb 12
How do different types of presbyopia-correcting #IntraocularLenses (#IOLs) actually work?
Read the Alcon Medical Affairs #WhitePaper to find out: bit.ly/4rUdoXu
In the white paper, titled Refractive and Diffractive Principles in Presbyopia-Correcting IOLs — An Optical Lesson, you’ll discover:
🔹 How refractive and diffractive optical approaches achieve multifocality in IOLs
🔹 How trifocal IOLs can utilize various diffractive optical designs to create distance, intermediate and near focal points
#EyeCare #Ophthalmology #AlconScience #GlobalMedicalAffairs #MedicalAffairs
ALT AlconScience.com
5
174

29 Dec 2025
🆕️Must Read 📚 “Are we overtreating small MEN1 pNETs?”
#MEN1 & pancreatic #NETs
Key challenges in detection & management
Lancet Diabetes & Endocrinology
@TheLancet
🟡 pNETs in >80% of MEN1 pts → ~50% of disease-specific deaths
🟡 Distinct from sporadic pNETs: younger onset, multifocality, coexisting tumors
🟡 Major controversies: when to operate, how to surveil small NF-pNETs
🟡 Biomarkers limited → MRI, EUS & SSTR-PET are complementary
🟡 Management must be individualized & multidisciplinary
👥 Dr. Chris Yates Dr. Paul Newey
✍️ Prof Rajesh V Thakker (@UniofOxford)
thelancet.com/journals/landi…
1
1
3
207

15 Dec 2025
Holiday Advent Calendar🎁❄️🎄
Day 13
Multifocality in sporadic medullary thyroid carcinoma associated with low tumor grade & no difference in somatic driver mutations/overall survival compared to unifocal tumors
surgjournal.com/article/S003…
#SurgeryAdventCalendar
#SoMe4Surgery
9
15
1,867

4 Dec 2025
🆕 Important prognostic factors for #UTUC risk stratification include stage, grade, different histological subtypes, tumour size, multifocality and hydronephrosis. Use prognostic factors to risk-stratify patients for therapeutic guidance.
#EAUguidelines
uroweb.org/guidelines/upper-…
3
12
1,316

22 Oct 2025
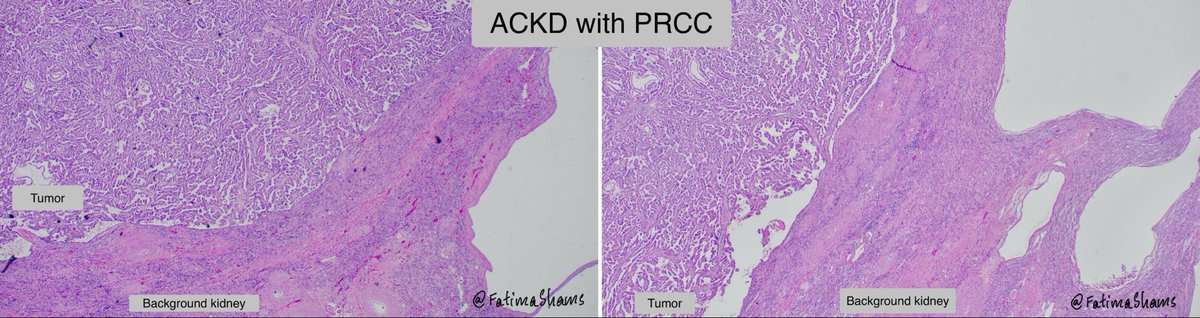
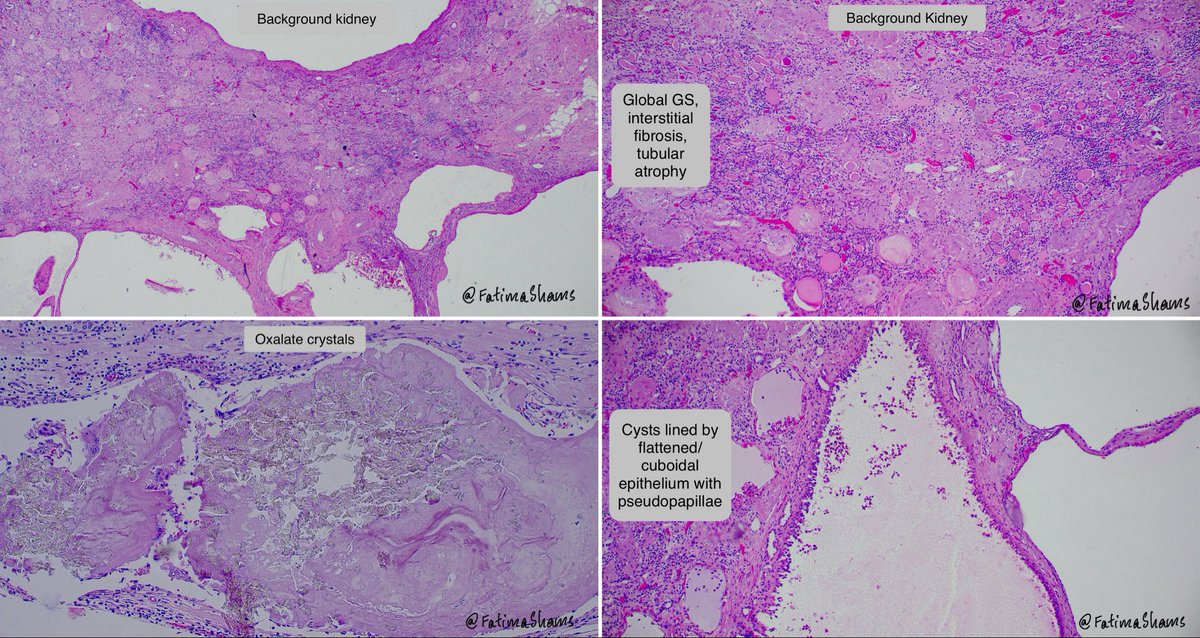
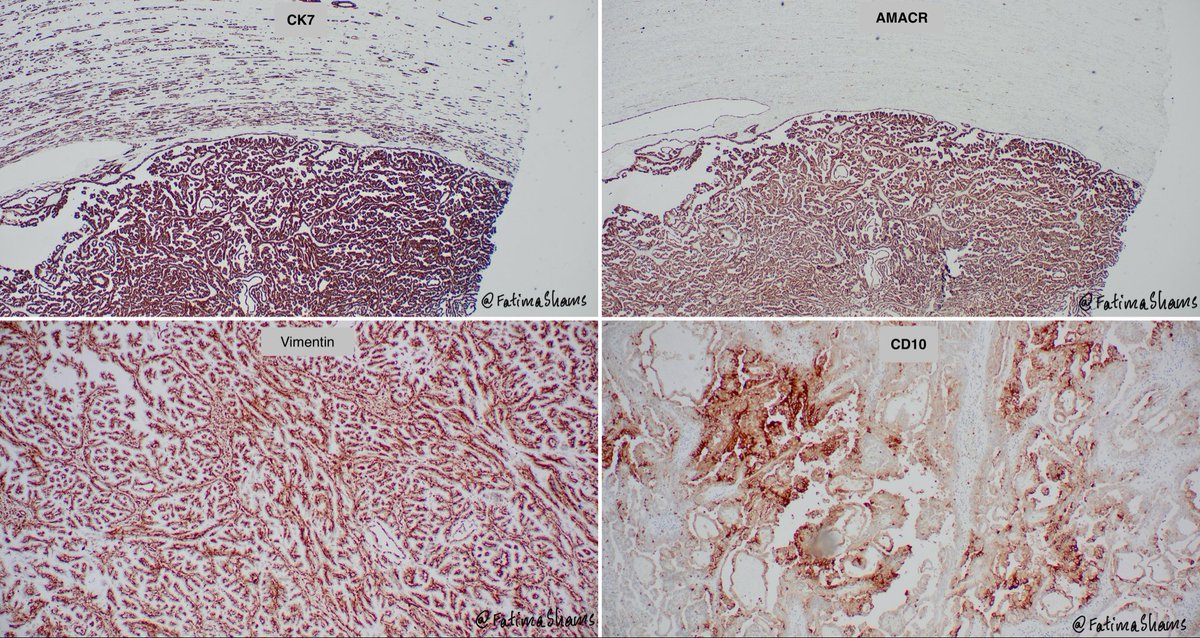
💎 Papillary Renal Cell Carcinoma (PRCC) in Acquired Cystic Kidney Disease
⚓️ Definition:
PRCC is a malignant epithelial tumour with papillary or tubulopapillary architecture — the second most common renal cell carcinoma (13–20%).
⚓️ Association:
Seen in patients with end-stage renal disease or long-term dialysis, arising in cyst walls or adjacent cortex of kidneys affected by acquired cystic disease (ACDK). Tumours may be bilateral or multifocal.
⚓️ Gross:
Well-circumscribed, yellow-tan to red-brown, sometimes friable or cystic, with areas of necrosis or hemorrhage. In ACDK, often protrudes into cyst cavity.
⚓️ Microscopy:
Papillary/tubulopapillary structures lined by cuboidal to low columnar cells, with foamy macrophages, psammoma bodies, and low-grade nuclei.
IHC: CK7 , AMACR , Vimentin , CD10±, CAIX–.
⚓️ Genetics:
Gains of chromosomes 7 & 17, loss of Y, and MET mutations (especially in low-grade tumours).
⚓️ Prognosis:
Usually low-grade and indolent, with better outcome than clear cell RCC, though multifocality is frequent in ACDK.
📚 WHO Blue Book (5ᵗʰ ed.) | Pathology Outlines – PRCC & ACDK
#pathology #surgpath #renalpath #pathologyresidents

1
15
34
2,430

21 Oct 2025
Chapter 86: Urothelial Carcinoma of the Renal Pelvis and Ureter (Transitional Cell Carcinoma of the Renal Pelvis/Urinary Tract)
第 86 章:肾盂/输尿管泌尿上皮癌(尿路上皮癌)
This chapter focuses on carcinoma arising from the urothelium of the renal pelvis, ureter, bladder, and urinary tract—commonly termed urothelial carcinoma (formerly transitional cell carcinoma, TCC). It details epidemiology, pathogenesis, clinical presentation, diagnostic evaluation, staging, treatment (surgery, chemotherapy, immunotherapy), and follow‑up considerations.
1. Epidemiology & Risk Factors
•Urothelial carcinoma of renal pelvis/ureter is less common than bladder urothelial carcinoma but clinically significant.
•Risk factors: smoking, chemical exposures (aromatic amines, phenacetin past use), chronic irritation/infection (e.g., analgesic nephropathy, urinary schistosomiasis), Lynch syndrome (hereditary non‑polyposis colorectal cancer).
•Clinical behaviour: potential for multifocality in the entire urothelial tract (so called “field change” effect).
2. Pathogenesis & Molecular Biology
•Originates in urothelial lining (transitional epithelium) of renal pelvis/ureter/bladder.
•Genetic alterations overlapping with bladder UC (FGFR3, PIK3CA, TP53, RB1, etc) may occur.
•Field defect: patients may develop synchronous or metachronous lesions throughout urinary tract.
3. Clinical Presentation
•Hematuria (gross or microscopic) is the most common presenting symptom.
•Flank pain or renal colic may occur if obstruction.
•Hydronephrosis/obstruction may lead to flank mass or declining renal function.
4. Diagnostic Evaluation & Staging
•Imaging: CT urography (abdomen/pelvis with contrast and delayed images) to detect filling defects in renal pelvis/ureter; ultrasound; chest imaging for metastasis.
•Urine cytology and ureteroscopic evaluation sometimes used.
•Staging: Depth of invasion (T stage into pyelocaliceal mucosa, muscularis, peripelvic fat), nodal (N), metastasis (M).
•Because of multifocal risk, surveillance of whole urothelial tract is important.
5. Treatment
•Localised disease: Radical nephroureterectomy (kidney entire ureter bladder cuff) is standard. Partial ureterectomy in select cases. Late‑stage/locally advanced: surgery adjuvant chemotherapy.
•Intravesical therapy (e.g., BCG) used in bladder UC but less commonly in upper tract UC.
•Systemic therapy: platinum‑based chemotherapy, immune checkpoint inhibitors (e.g., anti‑PD‑1) in metastatic disease.
•Endoscopic/laser ablation in low‑risk small tumors of renal pelvis in patients with solitary kidney or renal insufficiency.
6. Prognosis & Surveillance
•Prognostic factors: stage (depth of invasion), grade, presence of nodal/metastatic disease, multifocality.
•Recurrence is common in the bladder or contralateral urothelium—hence long‑term surveillance is essential.
•Long‑term renal function loss may occur due to nephroureterectomy.
—《Harrison’s Principles of Internal Medicine》

32
165

14 Oct 2025
🧬 PTC = most common thyroid cancer (≈ 80 %)
👩⚕️ More common in women than men
🕰️ Usually slow-growing, good prognosis
🔍 Presentation / Diagnosis
• 🗣️ Often a painless thyroid nodule, sometimes found incidentally
• 🔬 Ultrasound fine-needle aspiration (FNA) are key
• 🧪 Molecular alterations: BRAF V600E, RET/PTC fusions, others
🧩 Pathology / Behavior
• 📖 Characteristic nuclear features (Orphan Annie eyes, nuclear grooves, pseudoinclusions)
• 🌿 Propensity for lymphatic spread (neck lymph nodes) more than hematogenous
• 🔄 Multifocality is common
🏷️ Variants
• Tall-cell, columnar, diffuse-sclerosing, hobnail, etc. (some more aggressive)
• Encapsulated follicular variant → if noninvasive, now sometimes reclassified as NIFTP (noninvasive follicular thyroid neoplasm with papillary-like nuclear features)
🎯 Staging & Risk Stratification
• Uses age, tumor size, extrathyroidal extension, nodal involvement, distant metastasis
• Many small tumors (≤1 cm) are “microcarcinomas”
• Active surveillance sometimes acceptable for low-risk microcarcinomas (≤10 mm) in select patients
🛠️ Treatment
• 🧰 Mainstay = surgery (lobectomy or total thyroidectomy)
• 🎯 Radioactive iodine (RAI) when indicated (depending on risk)
• 💊 Thyroid hormone suppression therapy (to reduce TSH)
• ✅ Lifelong monitoring (e.g. thyroglobulin, imaging) for recurrence
📊 Prognosis
• 5-year survival ~ 95-98 % in many series
• Lymph node metastases often ↑ recurrence risk but do not greatly worsen survival in many patients
• Distant metastases are rare but more serious when present
🔔 Take-home points
• PTC is usually very treatable with excellent outcomes
• Many “low-risk” micro-PTCs can be managed conservatively in selected cases
• Multidisciplinary care is key (endocrinology, surgery, nuclear medicine)
1
4
521

10 Oct 2025
Multifocality in sporadic medullary thyroid carcinoma is associated with low tumor grade and no difference in somatic driver mutations or overall survival when compared with unifocal tumors - @SurgJournal surgjournal.com/article/S003… @TheAAES
1
3
10
1,127
9 Oct 2025
🧠 CNS Lymphoma — Matrix
🎯 Classification
🏠 Primary CNS Lymphoma (PCNSL) — lymphoma confined to brain, leptomeninges, spinal cord, or eyes.
🌍 Secondary CNS Lymphoma (SCNSL) — systemic lymphoma (esp. DLBCL) with CNS involvement at dx or relapse.
🔬 Pathophysiology & Markers
💥 Nearly all PCNSL are DLBCL, non-GCB type.
🧩 MYD88 L265P and CD79B mutations → NF-κB activation.
🧫 IHC: CD20⁺, MUM1⁺, BCL6⁺, high Ki-67.
🧠 Clinical Picture
⚡ Focal deficits, seizures, cognitive decline, headache, ↑ICP.
👁️ Ocular involvement (vitreous haze) → diagnostic clue.
⚠️ Avoid steroids pre-biopsy (lympholysis → false negative).
📸 Diagnosis
🔎 MRI with contrast (deep periventricular enhancing lesions).
🧬 Stereotactic biopsy = gold standard.
💧 CSF: cytology, flow cytometry, IL-10, MYD88 mutation.
🧠 PET-CT to rule out systemic disease.
💊 Treatment Strategy
💧 Backbone: High-dose Methotrexate (≥3 g/m²) ± Cytarabine ± Rituximab ± Temozolomide.
🧴 Support: Hydration Alkalinization Leucovorin rescue monitor MTX levels.
🌱 Consolidation:
- Fit → Thiotepa-based ASCT 🚀
- Others → Reduced-dose WBRT or chemo-consolidation.
♻️ Relapse: Ibrutinib, lenalidomide, CAR-T, or re-challenge with MTX-based chemo.
⚖️ Prognosis Factors
📊 Age > 60, ECOG ≥ 2, deep location, elevated LDH, multifocality, CSF/ocular disease.
⏳ Median OS ~4–5 yrs (younger ASCT).
💡 Hema Pearls
💧 MTX BBB penetration > CHOP ➜ CHOP ineffective.
⚠️ Always check renal function before MTX.
🧠 Neurotoxicity risk ↑ after WBRT; use reduced dose in elderly.
🧬 Molecular confirmation (MYD88) boosts diagnostic yield.
🧪 CNS-IPI score guides prophylaxis in systemic DLBCL.
📘 MCQs
1️⃣ A 65-yo with deep periventricular lesion, CD20⁺, MYD88⁺. Best induction?
A. R-CHOP B. HD-MTX Rituximab C. WBRT D. IT-MTX
✅ Answer: B. HD-MTX crosses BBB; CHOP doesn’t.
2️⃣ What reduces diagnostic yield?
A. Steroid use pre-biopsy B. Stereotactic biopsy C. Flow cytometry D. MYD88 testing
✅ Answer: A. Steroids lyse lymphoma cells.
3️⃣ High CNS-IPI systemic DLBCL → best prophylaxis?
A. IT-MTX B. IT-AraC C. None D. HD-MTX systemic
✅ Answer: A (± D in selected protocols).
🩺 OSCE Tips
👂 History: Duration of neuro symptoms, focal deficits, B-symptoms, immune status.
🧠 Exam: Cognitive assessment cranial nerves papilledema motor/sensory.
🧾 Investigations: MRI CSF Biopsy PET-CT.
💉 Management Plan: Hold steroids → Biopsy → HD-MTX regimen → Evaluate for ASCT.
🧍 Counseling: Discuss risk of neurotoxicity, relapse, need for MTX monitoring.
🧩 Follow-up: Cognitive testing MRI q3-6 months MTX toxicity watch.
📚 Key Sources:
•Ferreri AJ et al., Haematologica 2022;107(9):2149–2161.
•Houillier C et al., J Hematol Oncol 2022;15:94.
•Abrey LE et al., J Clin Oncol 2023;41(7):1185–1203.
•NCCN Guidelines: CNS Cancers v.2025.
#HemaPearls #CNSLymphoma #MTX #ASCT #Hematology #OSCE
5
25
1,196

9 Oct 2025
3D genomic mapping reveals multifocality of human pancreatic precancers
nature.com/articles/s41586-0…
1
2
60