
America orders billions of medical tests each year.
In Hypochondria, Hal Rosenbluth explores how fear, uncertainty, and overtesting contribute to rising healthcare costs; and why empowering patients matters. 🌊
newoceanhealth.com

3

Jun 12
Abolish the Federal Department of Education.
As a relative of John Adams and 30 year veteran public school teacher, I watched as the profession deteriorated, becoming more and more burdened by micromanagement, recertification requirements, mandated curriculums, useless data collection, overtesting, the list could go on and on …
Abolish Dept. of Education, I say.
2
16


May 30
No. All tests have false positives and false negatives. Overtesting (e.g. getting a test when not indicated) drastically ⬆️ false positives which leads to more testing and can lead to harm.
That's why there's been a project called @ChooseWiselyCA, to prevent overtesting
5
99

May 28
Longevity medicine has a major bottleneck.
And it's not even the science.
It's care delivery.
Because most health decisions don’t happen in a doctor’s office.
Spent the last two days at the Aging Code Summit in Cambridge with scientists, founders, investors, and clinicians working across biomarkers, therapeutics, AI, neurodegeneration, inflammation, regenerative medicine, and clinical trials.
The discovery engine is real.
But as a practicing longevity clinician, I kept thinking about the layer after discovery:
How does any of this actually reach people?
Not just the patient with time, money, and medical literacy.
Not just the person who can find the right concierge doctor.
And not just once a year, during a visit.
People make health decisions every day: in grocery stores, gyms, group chats, supplement aisles, lab portals, algorithm feeds, and anxious 11pm searches.
Most of those moments do not involve a physician.
So if the future of longevity is “clone more doctors,” we’re going to fail.
There will never be enough of us. And that’s not how people live.
The real opportunity is to build better surfaces for healthcare:
- tools that translate evidence into action
- systems that support follow-through
- guardrails against overtesting, overtreatment, and false certainty
- care models that meet patients where they already are
That’s the part I care most about building.
Longevity needs great science.
It also needs delivery models that make the science usable. @gocarecore
Thanks so much to @LongevityGL for another amazing meeting, and fellow speakers, organizers, and attendees: @Mindvyne @3cubedAi @DrGlorioso @justinqtaylor @NeuroAgeTX @agingdoc1 @usnehal @CoreViva @agelessrx_ @kpfortney @bioagelabs @lifebiosciences @JamieHeywood @microbeminded2 @polybioRF @mahdi_moqri @agingbiomarkers @manoliskellis @MIT_Picower @DrDorisDay @VincereBio @InSilicoMeds @hevolution_f @CellinoBio @MariZazzer

1
3
7
797

Sometimes medicine becomes difficult not because we do not know what to do, but because we know how easily disease can hide behind normal appearances.
A slim body, a flat stomach, good stamina, regular running, no diabetes, no family history. On paper, everything looks reassuring.
Then one day the patient develops “gastric discomfort”, mild chest heaviness, or unexplained acidity for months. Nothing dramatic. Nothing that clearly screams heart disease.
How do you advise a CT coronary angiography to a 30-year-old runner with no obvious risk factors?
Most cardiologists would hesitate. And reasonably so.
Because medicine is always balancing two fears:
the fear of overtesting healthy people,
and the fear of missing silent disease.
But reality keeps humbling us.
Two days back, a 50-year-old with minimal symptoms was found to have a 100% block.
Yesterday, a 30-year-old had two arteries completely blocked.
Both looked healthier than many people.
Coronary disease does not always arrive wearing the face of obesity, diabetes, or old age.
Sometimes it hides behind fitness, routine, and years of silent adaptation.
That is why symptoms matter.
Even vague symptoms.
Especially when they persist, change, or do not fit the usual pattern.
Not every acidity is cardiac.
But not every cardiac symptom looks like chest pain either.
1
3
55
2,937

May 15
Nonsense.
Overtesting led to overdiagnosis and overtreatment killed more than the damn disease, and that's before we get on to the shocking, lasting, lethal effects of the "vaccinations".
You are a sick man.
Excess deaths were only reliably high after the jabs came out.
16
138

May 10
If you mean Marty Makary, many people actually respect him a great deal — especially for being willing to challenge healthcare orthodoxy and speak in plain language. He built a strong reputation through patient safety work, transparency advocacy, and books like The Price We Pay.
The criticism tends to come from a few areas:
•During COVID, he became a very visible commentator and sometimes took positions earlier or more skeptically than mainstream public health leaders. Supporters saw him as independent-minded; critics thought he occasionally overstated confidence or undermined consensus.
•He criticizes parts of the healthcare establishment — hospitals, pricing, incentives, overtesting, bureaucracy. People inside institutions sometimes resist that style.
•He communicates very directly and publicly. Physicians who go heavily into media often attract stronger reactions than quieter academic leaders.
•Some people view him as too media-oriented or politically adjacent because he appears frequently on national television and writes opinion pieces.
But a lot of healthcare leaders and physicians appreciate him because:
•he focuses on waste, transparency, and incentives,
•he is generally understandable to non-physicians,
•he pushes for accountability,
•and he often frames issues around patients rather than institutions.
He’s also different stylistically from more traditional academic physicians. He tends to simplify complex issues into clear narratives, which is powerful for communication but can frustrate people who prefer more nuance or caution.
In terms of broad public reputation, he is probably viewed more favorably by the general public and business community than by some segments of academic/public-health circles.
3
2
157
May 10
Here is what ChatGPT says.
If you mean Marty Makary, many people actually respect him a great deal — especially for being willing to challenge healthcare orthodoxy and speak in plain language. He built a strong reputation through patient safety work, transparency advocacy, and books like The Price We Pay.
The criticism tends to come from a few areas:
•During COVID, he became a very visible commentator and sometimes took positions earlier or more skeptically than mainstream public health leaders. Supporters saw him as independent-minded; critics thought he occasionally overstated confidence or undermined consensus.
•He criticizes parts of the healthcare establishment — hospitals, pricing, incentives, overtesting, bureaucracy. People inside institutions sometimes resist that style.
•He communicates very directly and publicly. Physicians who go heavily into media often attract stronger reactions than quieter academic leaders.
•Some people view him as too media-oriented or politically adjacent because he appears frequently on national television and writes opinion pieces.
But a lot of healthcare leaders and physicians appreciate him because:
•he focuses on waste, transparency, and incentives,
•he is generally understandable to non-physicians,
•he pushes for accountability,
•and he often frames issues around patients rather than institutions.
He’s also different stylistically from more traditional academic physicians. He tends to simplify complex issues into clear narratives, which is powerful for communication but can frustrate people who prefer more nuance or caution.
In terms of broad public reputation, he is probably viewed more favorably by the general public and business community than by some segments of academic/public-health circles.
5
2
11
1,201

May 4
I concur
AI benchmarking is important
but we should be clear eyed the problem it is solving, which is the real benchmark:
HUMAN SLOP
I've trained and worked at the best medical centers in the world
the ceiling of care delivered is mediocre at best
the Bay area is pretty strong but it is much worse in the wild outside the ivory tower generally from my experience
massive overtesting and overtreatment, rampant misdiagnoses (20-30%), and underuse of best evidence

4
1
9
5,641

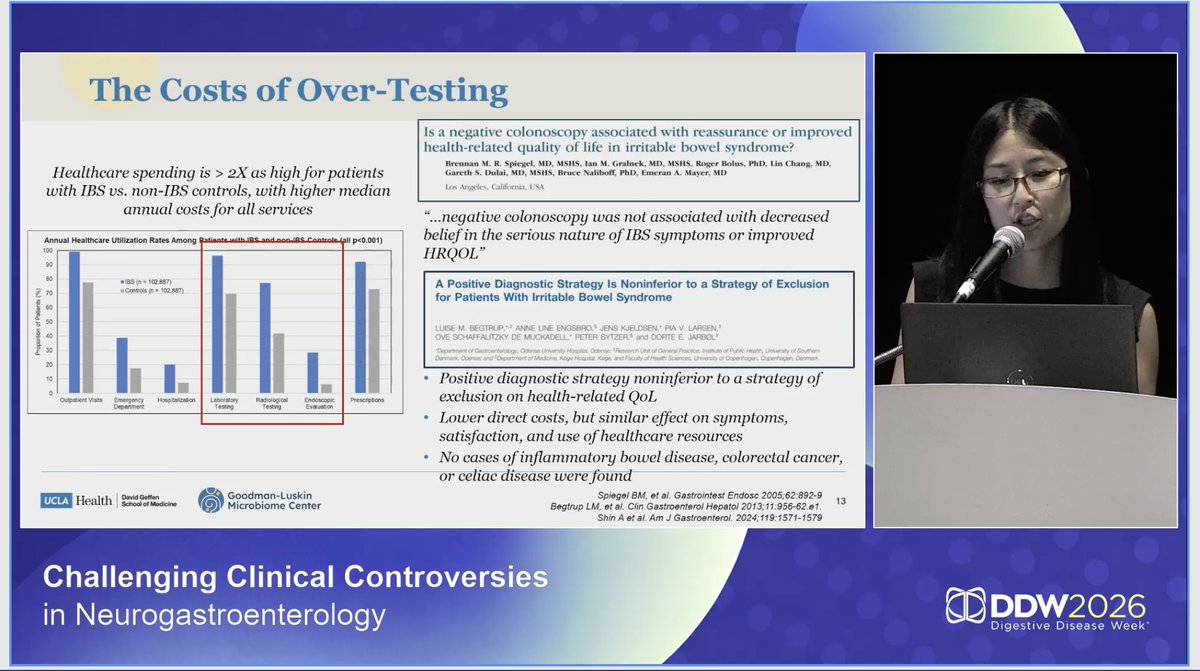
Minimal work-up or aggressive approach for #IBS?
Andrea Shin highlights the costs of overtesting - we need the right test for the right patient!
#DDW2026 @DDWMeeting
2
255

Bad fertility advice can harm. Overtesting, needless surgery, and delays can reduce your odds. Medicine should not become a maze. #IVF drmalpani.com/knowledge-cent…
2
164
Wrong fertility advice can reduce fertility. Patients need protection from overtesting, overtreatment, and blind obedience. #IVF drmalpani.com/knowledge-cent…
4
317

partial list of pathologies that all contribute to high cost and worse overall performance:
* supply bottlenecks for providers
* incredibly high cost of labor
* explosion of administrative bloat
* Certificate of Need laws
* The entire 'non-profit' hospital deception
* Hospital chain consolidation/market power
* Opaque pricing/billing practices
* Overtreatment/overtesting
* Obese/unhealthy population
* the entire structural mess that is drug pricing
* Imbalance towards specialty care
* Deficiencies in rural healthcare
Insurance companies belong in that list too, but they're not the single unique villain that some people want them to be.
10
16
201
3,996

Diagnosing shoulder pathology?
Clusters > single tests.
This Deep Dive explains how to improve diagnostic accuracy without overtesting:
🎥 youtube.com/watch?v=0vNc1GB1…
🌐 deepdiveortho.com
2
9
882

Open Access:
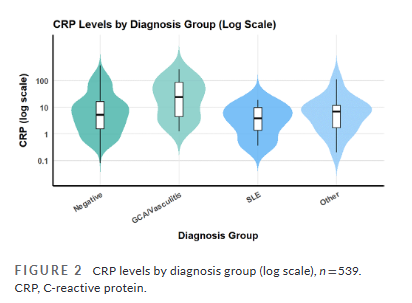
Myth: Headache → order ANA test
Fact: Most positive ANA results aren’t linked to autoimmune disease
A new study highlights the risks of overtesting.
Manuscript link: headachejournal.onlinelibrar…
@nicmaggio et al
#Headache #Neurology
2
6
3,814

Well said and illustrated. We normalize overtesting, overtreating, and overbuilding systems that reward volume rather than outcomes. Every extra scan, specialist hop, or “just in case” prescription feeds a machine designed to bill, not heal It's indefensible!
2
2
101

u For young, healthy people without symptoms, excessive medical testing-
overtesting—can lead to a "diagnostic cascade" where one unnecessary test triggers increasingly invasive procedures, higher costs, and psychological stress with no actual health benefit.
📷MS Kettering
1
1
2
45

Mar 30
Interesting. With widespread overtesting, overdiagnosis, and overtreatment, almost every Indian now seems to be labelled vitamin D deficient. Prescribing vitamin D has become a knee-jerk response for anyone who walks into a hospital with aches and pains.
7
193

هلا بروف خالد
بقول له بعد اذنه
“أتفهم فكرة إن الواحد ما يبي يقلق نفسه،
لكن الاطمئنان الحقيقي هو إنك تعرف وضعك بدري وتتحكم فيه،
مو إنك تتفاجأ بالمشكلة بعد ما تتأخر.”
الوقايه خير من العلاج وهنا سوف اشرح اهم الفحوصات للوقايه حسب التوصيات العالميه والمقدمه مجانا من وزاره الصحه السعودية ، اعز الله حكومتنا الرشيده
تمام 👌 هذا ملخص أهم الفحوصات الوقائية للرجال والنساء البالغين حسب التوصيات العالميه 2026 بصيغة عملية وسريعة 👇
⸻
🧠 أولاً: فحوصات أساسية للجميع (رجال نساء)
🩺 ضغط الدم
•من عمر 18 سنة
•كل سنة أو حسب الحالة
✔️ أهم فحص على الإطلاق
⸻
🩸 السكري (Type 2)
•من عمر 35–70 (إذا زيادة وزن)
•كل 3 سنوات
✔️ مهم جدًا بسبب الانتشار العالي
⸻
🧬 الدهون (الكوليسترول) سبق كتبت بالتفصيل عنها حسب اخر توصيات 2026
•من عمر 40–75
•كل 5 سنوات (أو حسب الخطورة)
⸻
⚖️ السمنة (BMI)
•تقييم دوري
✔️ مرتبط بكل الأمراض المزمنة
⸻
🚬 التدخين
•سؤال روتيني عرض علاج للإقلاع
⸻
🧠 الاكتئاب
•فحص دوري عند البالغين
⸻
🦠 فيروس B
•للفئات عالية الخطورة
⸻
👨🦱 فحوصات خاصة بالرجال
🧫 سرطان القولون
•من عمر 45–75
•خيارات:
•منظار كل 10 سنوات
•تحليل براز سنوي
⸻
❤️ تمدد الشريان الأبهر (AAA)
•رجال 65–75 المدخنين
•فحص بالموجات فوق الصوتية مرة واحدة
⸻
⚠️ PSA (سرطان البروستاتا)
•قرار مشترك (55–69)
•ليس فحص روتيني للجميع
⸻
👩🦰 فحوصات خاصة بالنساء
🌸 سرطان الثدي (Mammogram)
•من عمر 40–74
•كل سنتين
⸻
🧫 سرطان عنق الرحم
•21–29: Pap smear كل 3 سنوات
•30–65:
•HPV كل 5 سنوات
أو
•Pap كل 3 سنوات
⸻
🦴 هشاشة العظام
•من عمر 65
•أو أصغر إذا عندها عوامل خطورة
⸻
⚠️ فحوصات “ليست روتينية للجميع”
حسب USPSTF:
•❌ فحوصات شاملة سنوية بدون سبب
•❌ تصوير عشوائي (CT / MRI)
•❌ تحاليل بدون داعي
👉 الهدف: تقليل الإفراط الطبي (Overtesting)
⸻
🧠 خلاصة ذكية (مهم جدًا)
•✔️ الفحص = وقاية وليس وسوسة
•✔️ الفحوصات محددة حسب العمر والخطورة
•✔️ كل شخص له خطة مختلفة
⸻
🎯 خلاصة مختصرة جدًا
•ضغط – سكر – دهون = أساس
•قولون من 45
•ثدي وعنق رحم للنساء
•فحوصات حسب الخطورة وليس عشوائي
وفق الله الجميع وشكر دكتور على الطرح
4
12
9,756