Wafik S. El-Deiry, MD, PhD, FACP retweeted

Thanks very much for having me and the interest in Australia’s pancancer IO access.
A real time experiment to see if broadened eligibility improves equity of access whilst retaining responsibility to ensure efficacy, toxicity and real world outcomes are responsibility tracked

WIN rare cancers committee meets to discuss impacting patients with rare cancers across the globe. Jenny Liu presents Australia’s universal immunotherapy access initiative. Jim Palma discusses rare cancer position statements for the USA and for the globe. 🌎 🌏🌎
2
5
488
Jan Vincent Beltran, Ph.D. retweeted

30 Jun 2025
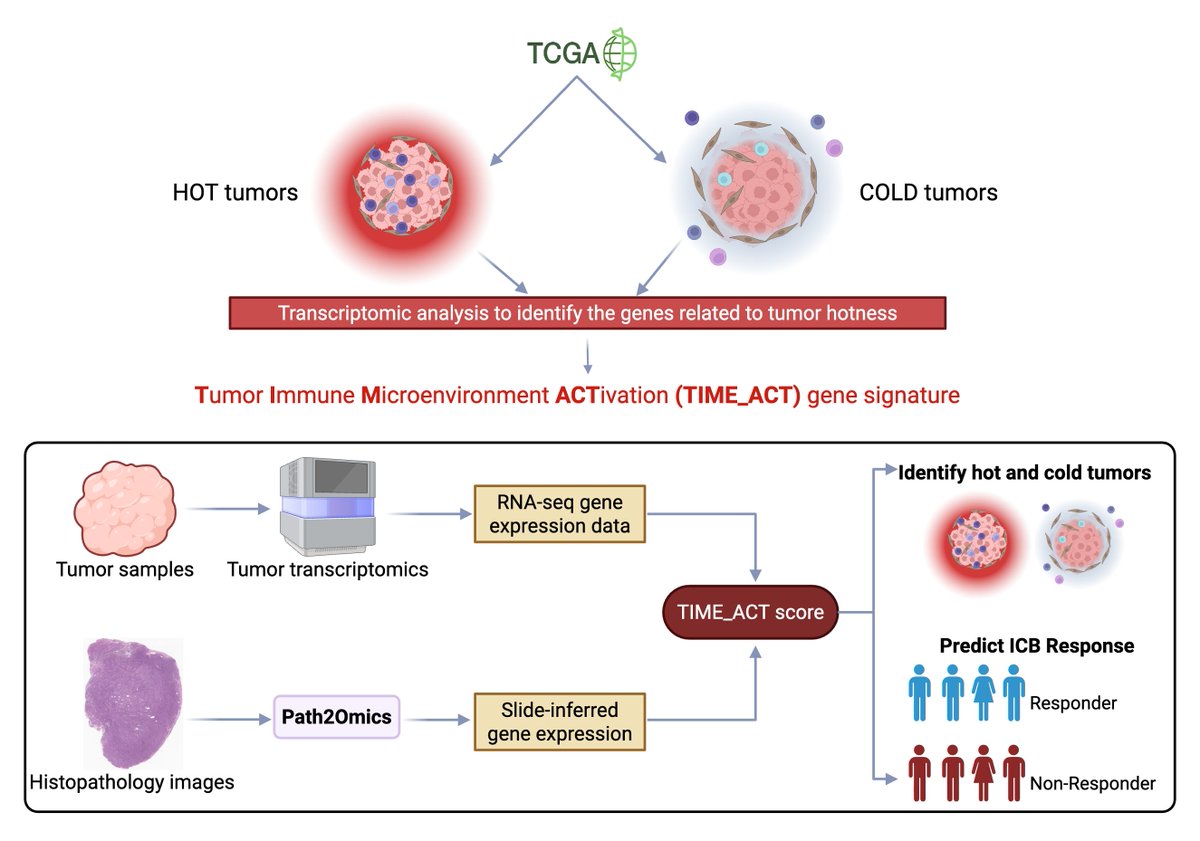
Proud to introduce TIME_ACT: an unsupervised, #pancancer signature, which accurately identifies hot tumors and predicts response to #ICB across #Cancer from tumor transcriptomics and histopathology. 🧵 (1/6)
📄 doi.org/10.1101/2025.06.27.6…
3
40
127
11,520

Jun 4
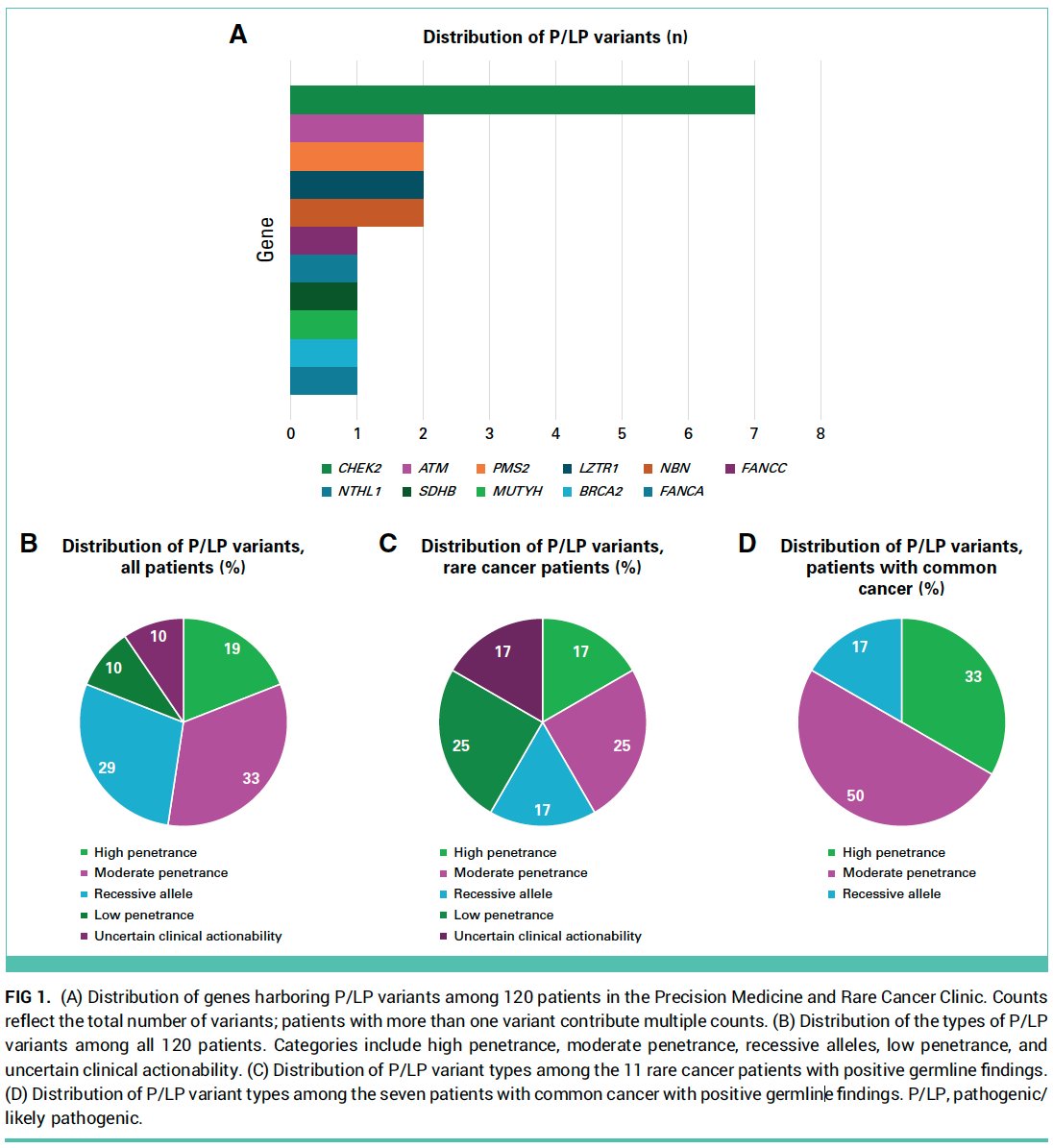
50% of #patients [w/ #cancer] positive for #germline variants did not meet @NCCN testing criteria, in a #PrecisionMedicine clinic providing #universal #germlinetesting to all #patients w/ common & rare #cancers
15% of all #patients had #pathogenic #germline #variants (PGVs)
13% of #patients w/ common #cancers (inc #breastcancer #lungcancer #CRC #pancreaticcancer #prostatecancer)
17% of #patients w/ rare #cancers (inc #sarcoma #braincancer #cholangiocarcinoma)
c/w
jamanetwork.com/journals/jam… #PiperNicolosi et al. @JAMAOnc
ascopubs.org/doi/full/10.120… @beitsch et al. @JCO_ASCO
ascopubs.org/doi/full/10.120… #NealShore et al. @JCOOP_ASCO
jamanetwork.com/journals/jam… @WhitworthMD et al. @JAMANetworkOpen
jamanetwork.com/journals/jam… @J_Samadder et al. @JAMAOnc
mdpi.com/1422-0067/26/7/2839 #IsaacAilts et al. @MDPIOpenAccess
ascopubs.org/doi/10.1200/JCO… @VivekSubbiah @Dr_R_Kurzrock @JCO_ASCO
Overall, our data support #universal [#pancancer] #germlinetesting as a strategy to uncover clinically valuable information...including...#medical management, #targeted #treatment...
#access #reducedisparities #genetictesting #precisionmedicine #precisiontherapy #clinicaltrials #precisionprevention
ascopubs.org/doi/pdf/10.1200… #PhebeLemert @Dr_R_Kurzrock et al. @MedicalCollege @JCOOA_ASCO @ASCO
10
14
1,567

How is AACR Project GENIE® shaping cancer research? At #AACR26, multiple sessions will explore how this pancancer registry continues to drive discoveries. Learn more in AACR Annual Meeting News: brnw.ch/21x1IOu
3
2
893
Through 2025, more than 21,000 users have accessed AACR Project GENIE®, the open-source, international, pancancer registry with more than 250,000 sequenced tumors from more than 211,000 patients. Learn more in the AACR Annual Impact Report:
brnw.ch/21x1blt

2
2
845

Feb 19
🌟New Resource article
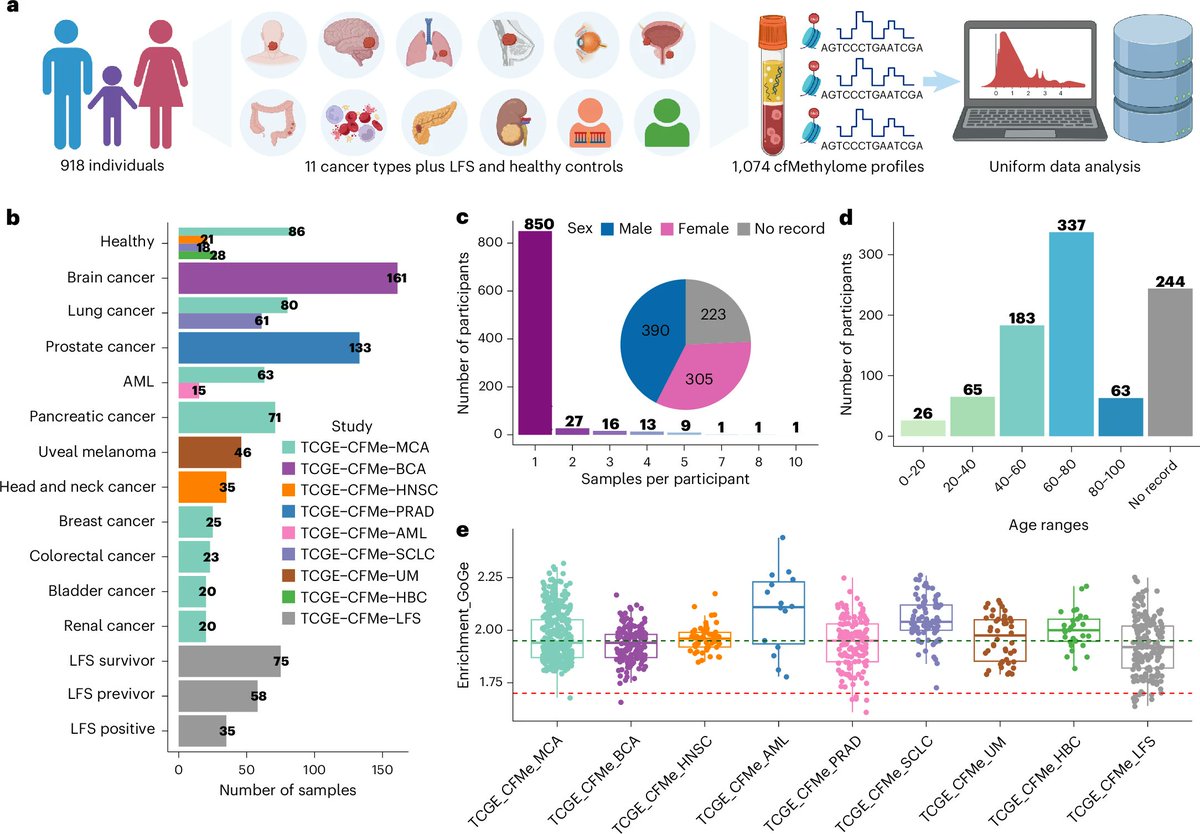
Read about the pancancer landscape of cancer-specific cell-free DNA methylation and fragmentomic features from plasma samples from 1,294 patients
✒️Yong Zeng, @MatLupien, @PughLab, Housheng Hansen He & colleagues
nature.com/articles/s43018-0…
1
18
58
4,319

9 Dec 2025
Cancer diagnosis is going digital faster than hospitals are planning for.🧬
Digital pathology is $1.15B today and expected to more than triple this decade.[1] Roche now has FDA clearance for primary diagnosis on whole-slide images.[2] Paige’s PanCancer Detect has FDA Breakthrough status for AI cancer detection.[3]
With staff shortages, this is infrastructure: faster turnaround, remote reads, richer data — or worsening backlogs.
🤔 What holds back digital pathology in cancer care: tech, rules, money or culture?
[1] [fortunebusinessinsights.com/…](fortunebusinessinsights.com/…)
[2] [marketwatch.com/story/roche-…](marketwatch.com/story/roche-…)
[3] [firstwordhealthtech.com/stor…](firstwordhealthtech.com/stor…)
#DigitalPathology #Cancer #HealthTech
Sciqst: AI-powered literature reviews in minutes.
Generate comprehensive, up-to-date scientific reviews from the latest papers with one click.
sciqst.com
1
5
233

@CFerroneMD of @MassGeneral leads Alliance A021806 studying whether chemotherapy before and after surgery is better than just after surgery for pancreas cancer. Learn more: bit.ly/Alliance-A021806 #NCI #NCTN #pcam #PanCancer #PancSM #PancreaticCancerAwarenessMonth
2
133
17 Nov 2025
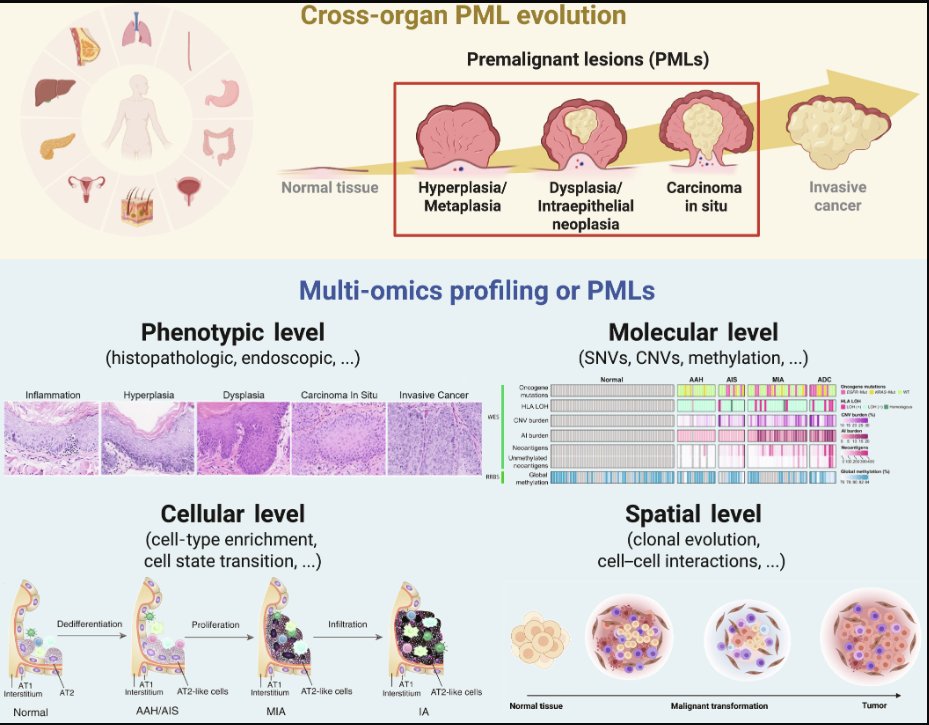
"...the convergence of high-resolution #multiomics with sophisticated #AI is poised to redefine #premalignant lesion research, enabling #pancancer exceedingly-#early risk stratification and pharmacological #prevention."
For example, #multiomics analysis of #colorectal #polyps from #patients w/ #familialadenomatouspolyposis/#FAP found that the #arachidonicacid pathway was up-regulated early in hyperplasia, which was targeted by #aspirin, giving a potential explanation of the preventative #treatment mechanism. @EdEsplin et al. nature.com/articles/s43018-0… @NatureCancer
#genetics #genomics #RNASeq #proteomics #metabolomics #lipidomics #CRC #colorectalcancer #precisionmedicine #precisiontherapy #clinicaltrials #precisionprevention @CGAIGC
spj.science.org/doi/10.34133… #FeiranZhang et al. #Research @ScienceMagazine
1
3
8
498
4 Nov 2025
$TEM 🔥🔥🔥Shareholder letter: "While others have been largely focused on bringing assays to market, our main focus over the past 10 years has been investing in technology and AI. If you look at the lines of code we have written, the number of software engineers we employ, or the amount of money we invest in cloud and compute, there is no comparable in diagnostics.
Those investments have allowed us to build an agentic platform that brings the benefits of AI to the over 5,000 providers that are now connected to Tempus. Not only has this allowed us to amass over 400 petabytes of multimodal data, but those investments also serve as the cornerstone of our long-term strategy to use AI to contextualize all diagnostics, helping physicians make data-driven decisions in real time.
As a result, what we can now do is pretty amazing, such as recommend alternative therapies based on prior drug regimens, match patients to clinical trials based on inclusion and exclusion criteria, close care gaps and ensure guideline adherence, run multimodal algorithms that are both predictive and prognostic, analyze time on therapy and progression-free survival for patients like the one being treated, predict IO response beyond conventional markers such as TMB and MSI status, deliver real-time insights across disease areas to better understand comorbidity, and run diagnostic algorithms at scale in adjacent medical practices, such as radiology and pathology, to further refine treatment.
Focusing on the last of those, we have long invested in digital pathology given its clinical importance. We have built hundreds of algorithms from the library of ~1 million H&E images we have digitized over the years, as we believe generating insights faster and more efficiently is important for care.
When Paige became available, we decided it was too strategic to pass up. Paige is a unique asset. Not only does it have the largest pathology library of cancer patients we know of, with ~7 million digitized slides, it was formed through a unique partnership with Memorial Sloan Kettering, who over the past decade has worked hand in hand with the Paige team to assemble millions of patients’ worth of connected clinical and pathology data."
On top of its proprietary library of slides, Paige has a state-of-the-art pathology viewer, an FDA-approved algorithm for prostate cancer with a pancancer application in flight, and the industry-leading AI foundation model. Integrating the Paige offering within the Tempus platform will allow us to provide additional actionable insights to the physicians and patients we serve."
2
2
23
5,109

9 Oct 2025
Es que sois unos pringados haciendo mamografias cada no se cuantos años en lugar de ina biopsia liquida pancancer una vez al mes.
1
2
341

25 Sep 2025
New generation of cancer-preventing vaccines could wipe out tumors before they form (Jocelyn Kaiser, Science, 7 Apr 2022).
🧬 Cancer-Preventive Vaccines – Entering a New Era
🔹 Background
Current vaccines prevent virus-linked cancers (HBV → liver cancer, HPV → cervical cancer).
Most cancers are non-viral and historically beyond the reach of vaccines.
New antigen-based preventive vaccines are now in early clinical trials for high-risk populations.
🔹 Core Concept
Vaccines deliver tumor-associated antigens or neoantigens (exclusive to tumors).
Goal: prime B & T cells before cancer arises.
Works best in healthy but high-risk individuals (e.g., Lynch syndrome, BRCA mutations).
🔹 Strategies on Trial
Neoantigen-based vaccines (Lynch syndrome, pancreatic KRAS).
DNA / RNA vaccines (e.g., hTERT DNA vaccine at Penn).
Protein / peptide vaccines (MUC1, alpha-lactalbumin).
Multipronged vaccines with multiple antigens (Mayo Clinic breast cancer trial).
mRNA vaccines modeled on COVID-19 success—safer, scalable, strong immune activation.
🔹 Clinical Trial Highlights
Lynch Syndrome Vaccine – 209 frameshift neoantigens (Nouscom, Italy).
Pancreatic Cancer Vaccine – KRAS mutant peptides (Johns Hopkins).
BRCA-related cancers – DNA vaccine with hTERT, PMSA, WNT1 (Penn, Mayo).
MUC1 Vaccine – Prevents recurrence of polyps, reduces progression risk.
Triple-Negative Breast Cancer – Alpha-lactalbumin protein vaccine (Cleveland Clinic).
🔹 Early Evidence
Trials show strong immune responses and hints of reduced recurrence.
In pancreatic cancer survivors: vaccine extended recurrence-free interval (41% cancer-free at 18 months vs avg 12 months).
MUC1 responders: markedly fewer polyps within 1 year vs placebo.
🔹 Challenges
Immune suppression from tumor microenvironment.
Risk of autoimmunity if antigens overlap with normal tissues.
Identifying reliable biomarkers of protection (to avoid decades-long follow-up).
Genetic diversity in immune responses complicates universal vaccine design.
🔹 Future Directions
Stepwise approach: start with single high-risk syndromes (Lynch, BRCA, KRAS-driven cancers).
White House’s Cancer Moonshot supports pancancer mRNA vaccine research.
Comparative oncology: dog cancer vaccine trial (400 dogs, 31 antigens) may guide human efforts.
Long-term vision: universal cancer-prevention vaccine covering common driver mutations.
🔹 CME INDIA Clinical Pearls
Cancer vaccines are shifting from treatment to prevention.
Best candidates: high genetic risk carriers (Lynch, BRCA, KRAS).
Neoantigens are key: tumor-exclusive, highly immunogenic, predictable in some syndromes.
mRNA platform is the likely workhorse—proven safety, rapid development.
Early results are promising, but long-term randomized data are awaited.
A preventive vaccine reducing cancer risk by even 30–50% in high-risk groups would be transformative.
For now, vaccines complement—not replace—screening & surveillance.
science.org/content/article/…

2
5
621

3 Sep 2025
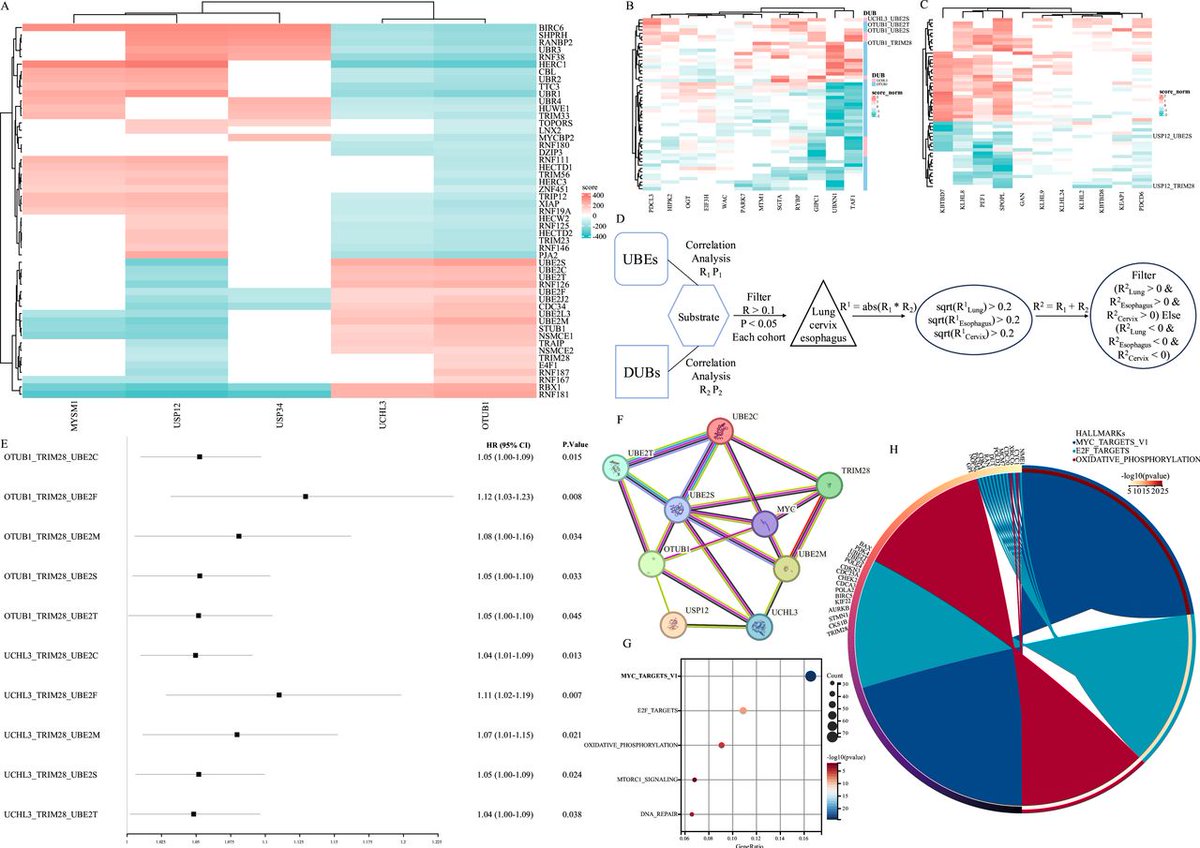
New #JITC article: Constructing a pancancer ubiquitination regulatory network to determine tumor characteristics, immunotherapy response, and prognosis bit.ly/45Z16TG
6
9
776

3 Sep 2025
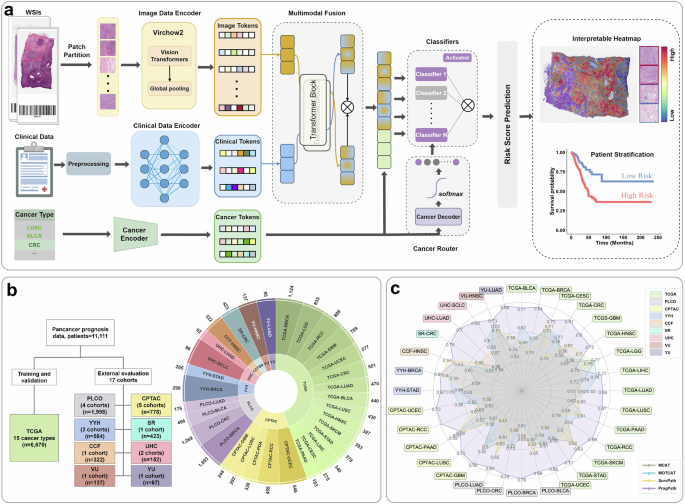
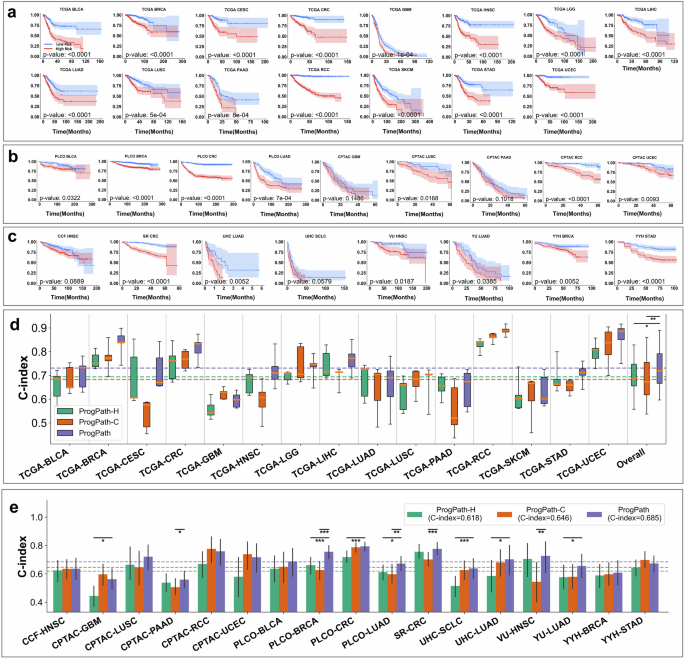
🚨 New paper out in Nature’s Signal Transduction and Targeted Therapy!
We introduce PROGPATH — a unified AI model for pancancer outcome prediction using histopathology images clinical data.
👉 nature.com/articles/s41392-0…
#AI #Oncology #DigitalPathology
3
3
14
987
29 Aug 2025
El nuevo protocolo: a toda persona que pise urgencias, CT de cuerpo completo, una biopsia liquida pancancer, marcadores de daño miocardico, colo y gastroscopia, y un holter durante una semana.
1
8
476
22 Aug 2025
Oye, si de verdad es tan demandado, yo estoy dispuesto a montar una empresa que haga un panel pancancer en biopsia liquida a quente sana que lo quiera pagar. Luego lo de saber de donde viene un 0.01% de KRAS mutado ya problema vuestro :)
1
2
12
1,198

20 Jun 2025
I was always pro-assisted dying, ever since I saw my grandparents die of cancer.
I went into nursing bc I couldn't look after my nana end-stage PanCancer when I was 10.
I couldn't finish my 3rd year of training due to various personal reasons, inc a few marriages to abusive men
1
2
74