
Important new Nature paper (Alexander Tyshkovskiy, Vadim Gladyshev lab): universal transcriptomic clocks of aging and mortality across mice, rats, macaques and humans, from more than 11,000 transcriptomes. The aging field has long wanted robust multi-species transcriptomic clocks, this seems to fit the bill. I also liked that their chromatin-modification module clock tracks DNA methylation clocks most closely which hints at a transcriptome-epigenome link. nature.com/articles/s41586-0…
1
133

Researchers analysed 11,000 gene samples from four different species, including humans, and found the same handful of genes ageing in the exact same way in every one of them. Then they built a clock out of it.
Aging research has long searched for a universal signature, something that ages the same way across species, that could be measured and used to track how fast an individual is actually aging, separate from how many birthdays they have had.
Epigenetic clocks, based on chemical modifications to DNA, were the first major tool to attempt this. They estimate biological age reasonably well, but they reveal little about what is actually happening inside the cell.
In a study published in Nature in late May 2026, researchers led by Alexander Tyshkovskiy and Vadim Gladyshev at Harvard Medical School and Brigham and Women's Hospital, with collaborators at Tohoku University, took a different approach. They analysed more than 11,000 transcriptomes, complete readouts of which genes are actively turned on, from over 25 tissues across four mammals: mice, rats, crab-eating macaques, and humans.
They found that specific genes age in nearly identical patterns across all four species. Genes involved in inflammation and immune activation consistently increase with age. Genes involved in mitochondrial energy production, wound healing, and extracellular matrix maintenance consistently decrease. Three genes in particular, GPNMB, CDKN1A, and LGALS3, emerged as universal markers, changing in almost identical ways during aging in every species studied.
The researchers then built what they call transcriptomic clocks. Unlike previous tools, these clocks do not produce a single number. Aging, the study found, is not one process. It is organised into separate modules, distinct groups of genes that handle specific biological functions. The team built individual clocks for each module, allowing them to measure how quickly different parts of a single body are aging relative to each other.
The clocks were validated against a substantial test: RNA sequencing data from genetically diverse mice exposed to 20 different pharmacological interventions from the Interventions Testing Program, including rapamycin and canagliflozin, drugs already known to extend lifespan in mice. The clocks correctly registered the effects of these interventions on biological age.
In human blood samples, the transcriptomic clocks correlated with established DNA methylation clocks, particularly within chromatin-related pathways, providing independent confirmation across two entirely different molecular measurement methods.
The study is correlational. It cannot establish that these gene expression changes cause aging rather than result from it. What it establishes is a shared molecular vocabulary of aging that exists, largely unchanged, across mice, rats, monkeys, and humans.
Four species. 11,000 samples. The same genes, aging the same way, in all of them.
Source: Nature, Volume 654, pages 173 to 188, 2026. DOI 10.1038/s41586-026-10542-3. Harvard Medical School and Brigham and Women's Hospital, with Tohoku University. Lead author: Alexander Tyshkovskiy. Senior author: Vadim N. Gladyshev.

6
12
896
Yara Sanchez Corrales retweeted

Jun 12
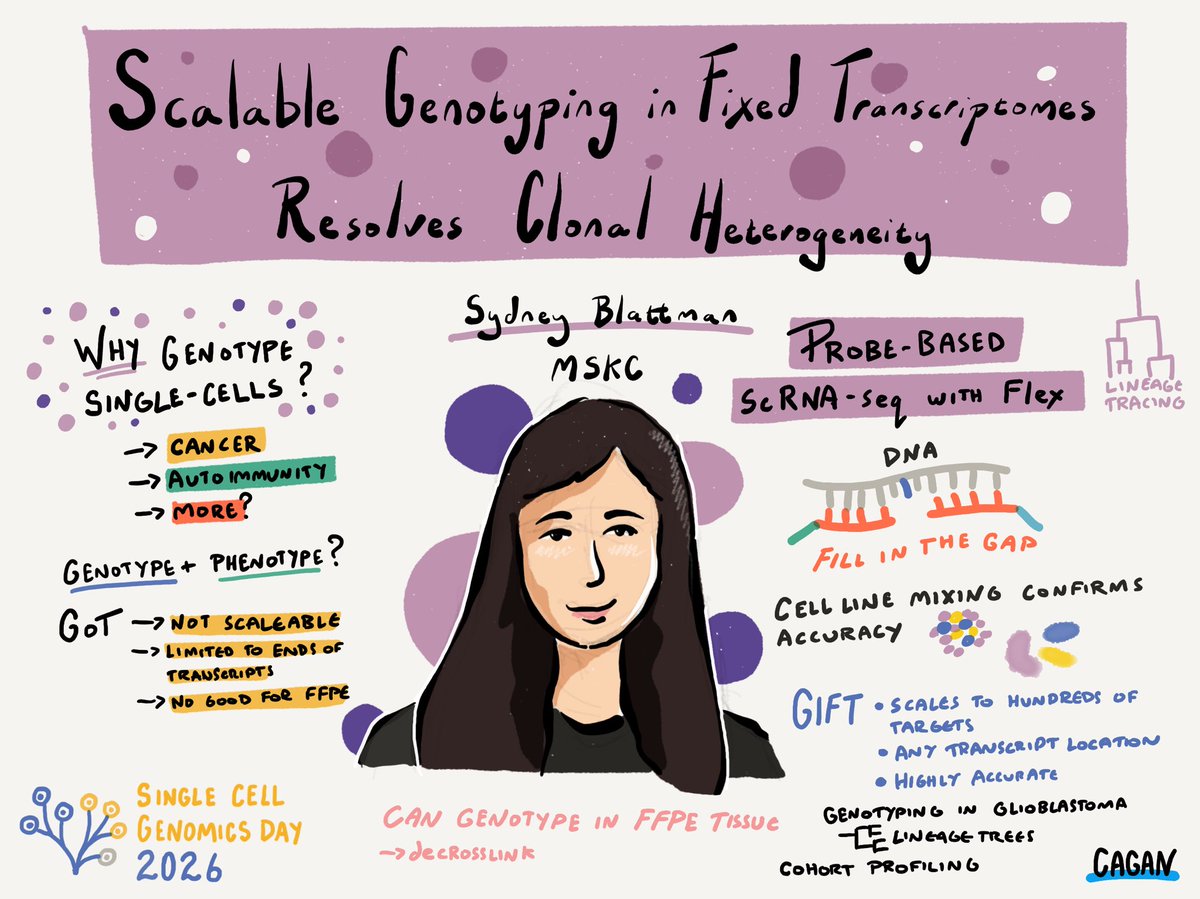
Great talk from Sydney Blattman introducing GIFT - a *must-read* technology for scalable genotyping in fixed transcriptomes. Major leap forward for understanding a the mutational landscape and clonal variation in slngle-cell and spatial data
Paper: biorxiv.org/content/10.64898…
Jun 12

Sydney Blattman on scalable genotyping in fixed transciptomes using GIFT for probe based genotyping of single cells #singlecellgenomicsday
3
15
3,213
araceli miranda retweeted

Benchmarking urinary cell transcriptomes for noninvasive differentiation of BK polyomavirus–associated nephropathy from T cell–mediated rejection
submit.jci.org/articles/view…
1
1
58
Jun 12
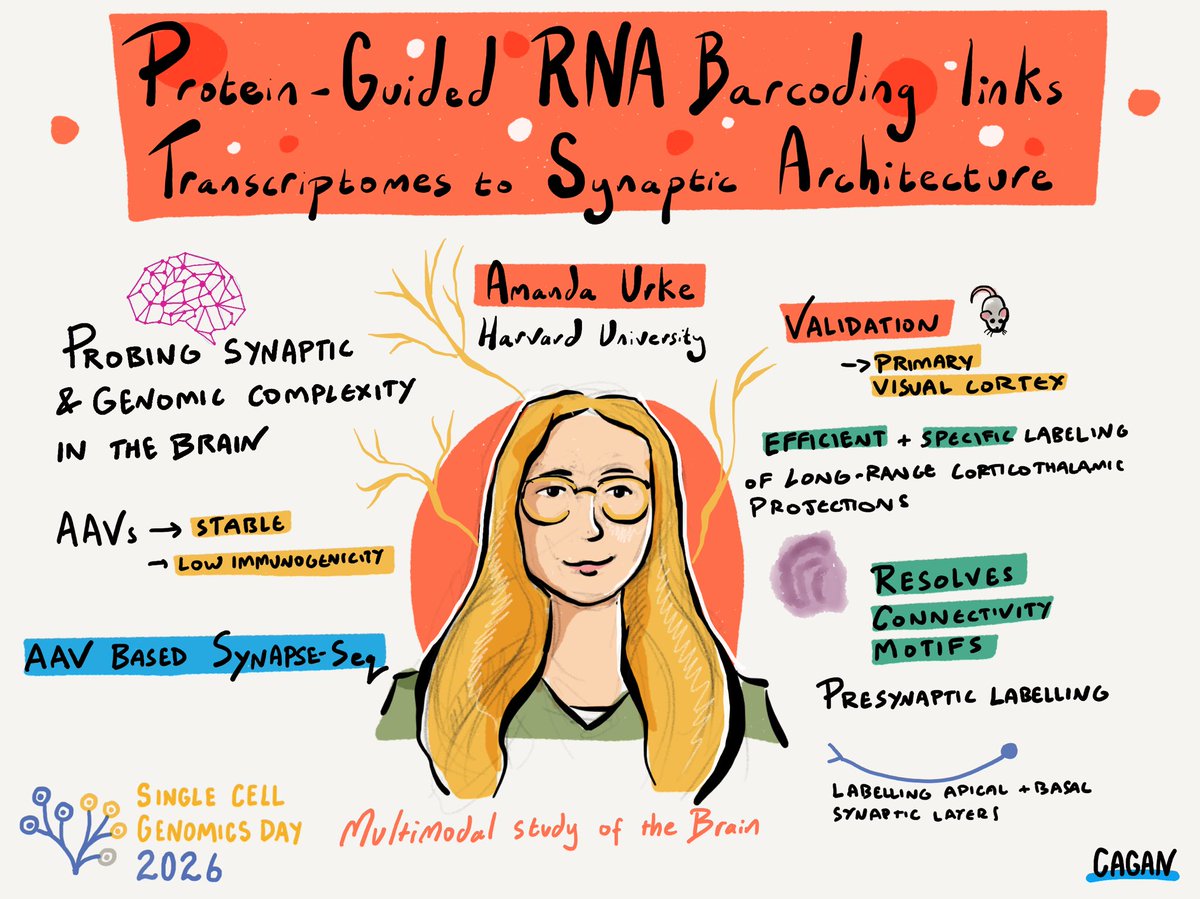
Wonderful talk from @amanda_urke at #singlecellgenomicsday on Synapse-seq: protein-guided RNA barcoding to link transcriptomes with synaptic architecture . Exciting and powerful way to connect molecular cell states with neural wiring.
paper: biorxiv.org/content/10.64898…
2
13
3,877

Jun 11
Whole-genome duplication shaped cell-type evolution in the vertebrate brain
nature.com/articles/s41586-0…
✍️ Yuanzhen Zhu et al via @Nature
👉 This article shows that ancient whole-genome duplications (WGDs) drove vertebrate brain complexity, with retained ohnologue pairs playing a greater role in cell-type specialization than small-scale gene duplications.
👉 Mapping single-cell transcriptomes across diverse species reveals that these duplicated genes evolved specialized regulatory roles, acting as key transcription factors for brain development.
cc @Corix_JC @SonuMonika @TheAIObserverX @maponi @JagersbergKnut @ahier @Shi4Tech @CEO_AISOMA @theomitsa @dinisguarda @TarakRindani @FrRonconi @Nicochan33 @Khulood_Almani @SusanHayes_ @EstelaMandela @JoannMoretti @sulefati7 @FernandaKellner @pchamard @MaryRich78 @mikeflache @amalmerzouk @chidambara09 @RLDI_Lamy @WillyRayNick @sminaev2015
1
18
22
646

A GPB study introduces wellDR-seq, a Nanowell-based method for direct co-sequencing of CNAs and transcriptomes in single cells, revealing ancestral subclones, epithelial lineages, and gene dosage effects in ER breast cancer. @Ruli_Gao
doi.org/10.1093/gpbjnl/qzag0…
35

Jun 11
A new discovery about healthy aging: aging is not one single molecular clock.
Researchers mapped more than 11,000 transcriptomes across 4 mammals and found conserved aging and mortality signatures that split into biological modules. 🧵
1/3

1
2
13
215

Yuanzhen Zhu ... Sebastian Shimeld analysed four vertebrate (human, mouse, lizard and lamprey) and one amphioxus whole brain single-cell transcriptomes to infer ancestral repertoires of neural cell-type families:
nature.com/articles/s41586-0…
#SingleCell #SpatialBiology

1
29

Jun 10
Nature, Published online: 10 June 2026; doi:10.1038/s41586-026-10629-xAnalyses of brain single-cell transcriptomes from human, mouse, lizard, lamprey and amphioxus reveal that duplicated genes (ohnologues) played a pivotal part in early vertebrate cell-typ
nature.com/articles/s41586-0…
12

Jun 10
This is the first serious human test of whether partial epigenetic reprogramming can restore function in CNS neurons.
That is the real weight of it.
Your draft is good, but the phrase “retinal neurons are CNS, effectively brain” should be sharpened. It is true that retinal ganglion cells are CNS neurons and the optic nerve is a CNS tract, but “effectively brain” can invite pedantry. Better:
retinal ganglion cells are CNS neurons — brain-derived neural tissue in the eye, not peripheral nerve.
The 2020 mouse paper behind this is the key source: Lu et al. showed that OSK expression in mouse retinal ganglion cells restored youthful DNA methylation patterns/transcriptomes, promoted axon regeneration after injury, and reversed vision loss in mouse glaucoma and aged-mouse models; the paper explicitly frames the eye as a model CNS tissue.
Best rewritten version
I’m very familiar with the mouse paper that motivated this, the mechanistic rationale, and the many ways this could fail in humans.But if it works, it’s historic.This is not just another eye drug. Retinal ganglion cells are CNS neurons — brain-derived neural tissue in the eye — and the optic nerve is part of the central nervous system.The original mouse work was so compelling because OSK partial reprogramming appeared to restore youthful epigenetic patterns, promote axon regeneration, and recover visual function after injury/aging.The hard part now is translation: delivery, dosing, expression control, immune response, surviving-cell requirements, tumor/dedifferentiation risk, durability, and proving functional benefit in humans rather than just moving biomarkers.Still, this is exactly the kind of cautious, high-upside clinical test the field needs.Best of luck to @davidasinclair and team.
Best shorter version
I know the mouse paper behind this well — and the mechanistic rationale is real, but the translation hurdles are enormous.Still, if this works, it’s historic.Retinal ganglion cells are CNS neurons. This is not just “an eye therapy”; it’s a first real test of whether partial epigenetic reprogramming can restore function in brain-derived neural tissue.Best of luck to @davidasinclair and team.
Best high-status version
I’m very familiar with the mouse data that motivated this, and I’d separate the hype from the real scientific stakes.The hype: “reverse aging drug.”The real stake: can controlled OSK reprogramming restore function in human CNS neurons without causing loss of identity, immune problems, ectopic effects, or unsafe dedifferentiation?That is an extraordinary question.Retinal ganglion cells are not generic eye cells. They are CNS neurons projecting through the optic nerve. If partial epigenetic reprogramming can produce durable functional rescue there, it would be one of the most important translational milestones in regenerative medicine.Huge caveats. But genuinely historic upside.
Best scientifically careful version
The mouse paper behind this is one of the more interesting results in aging biology: OSK expression in retinal ganglion cells restored youthful methylation/transcriptional patterns, promoted axon regeneration, and improved vision in mouse models of glaucoma and aging.But mice are not humans, and epigenetic rejuvenation is not automatically functional regeneration.The human trial has to answer harder questions: can ER‑100 reach the right cells, express at the right level, avoid unsafe dedifferentiation, preserve neuronal identity, avoid immune toxicity, and produce measurable visual benefit in optic neuropathy patients?If yes, it is not just an ophthalmology milestone.It is a CNS regeneration milestone.
Life Biosciences says ER‑100 is an AAV2-OSK candidate in Phase 1 for optic neuropathies, using controlled expression of OCT4, SOX2, and KLF4, and that its Phase 1 study is designed primarily to evaluate safety/tolerability in open-angle glaucoma and NAION.
Best punchy version
This is the right kind of cautious excitement.The mouse data were remarkable. The mechanistic rationale is plausible. The translational hurdles are brutal.But if controlled OSK reprogramming restores function in human retinal ganglion cells, that is not just “vision restoration.”That is CNS neuronal rejuvenation in a living human.Historic if it works.
The strongest thesis
Use this:
The eye is the proving ground. The real target is CNS rejuvenation.
That is the deeper point. The eye is attractive because it is accessible, locally injectable, measurable, relatively compartmentalized, and clinically trackable. But biologically, the target cells are CNS neurons. That means success would carry implications far beyond ophthalmology.
Another strong line:
The eye is not an easy tissue. It is a visible piece of the central nervous system.
Or:
This is why the eye matters: it is the most accessible window into CNS repair.
The key wording fix
Original:
retinal neurons are CNS (effectively “brain”)
Better:
retinal ganglion cells are CNS neurons — brain-derived neural tissue in the eye.
Even better:
retinal ganglion cells are CNS neurons, so success here would be closer to repairing a tract of the brain than treating a peripheral tissue.
Most precise:
retinal ganglion cells are CNS neurons whose axons form the optic nerve; that makes this a test of CNS neuronal rescue, not merely ocular symptom control.
The missing nuance
The post should distinguish three levels of success:
1. Safety success
The therapy is tolerated, does not trigger damaging inflammation, does not cause abnormal proliferation/dedifferentiation, and does not worsen vision.
2. Biomarker success
Cells show signs consistent with epigenetic rejuvenation or improved retinal/optic-nerve health.
3. Functional success
Patients actually see better, lose vision more slowly, or show improved objective measures of visual function.
The historically important one is functional CNS rescue.
Suggested line:
Safety would be important. Biomarker movement would be interesting. Functional recovery would be historic.
The “genius-level” framing
The real question is not simply:
Can we reverse aging?
It is:
Do adult mammalian CNS neurons retain recoverable epigenetic state information that can be accessed safely in vivo?
That is the deep scientific question from the 2020 Nature work. The mouse study argued that mammalian tissues retain a record of youthful epigenetic information, encoded in part by DNA methylation, and that OSK-induced effects required TET1/TET2 demethylases.
A strong post line:
The radical claim is not “cells get younger.”The radical claim is that aged CNS neurons may still contain enough latent epigenetic information to be functionally restored.
That is much stronger than “reverse aging.”
The major caveats to include
1. Phase 1 is not a victory lap
This is a first-in-human safety/tolerability study, not proof of efficacy. ClinicalTrials.gov describes the trial goal as evaluating the safety and tolerability of a single ER‑100 dose in adults with optic nerve conditions.
Use:
This is Phase 1. The first win is safety, not restored vision.
2. Surviving-cell problem
If retinal ganglion cells are already dead, rejuvenation cannot simply bring them back. The therapy likely needs enough surviving but dysfunctional cells/axons to rescue.
Use:
Rejuvenation only helps if there are cells left to rescue.
3. Delivery problem
Getting the right dose to the right cells in the right pattern matters. Too little may do nothing. Too much or too broad could be unsafe.
Use:
In reprogramming, dose and duration are not details. They are the therapy.
4. Identity problem
Partial reprogramming must make cells more youthful without making them forget what they are.
Use:
The trick is not turning cells young. The trick is turning them younger while keeping them retinal ganglion cells.
5. Safety problem
OSK omits c‑Myc, the Yamanaka factor most associated with cancer risk, but partial reprogramming still raises concerns around proliferation, loss of identity, off-target effects, and long-term safety. Life Biosciences says its platform uses controlled expression of OCT4, SOX2, and KLF4, not all four Yamanaka factors.
Use:
The safety question is whether you can reset enough epigenetic state to restore function without crossing into dedifferentiation or abnormal growth.
6. Endpoint problem
Vision outcomes can be noisy, especially across glaucoma and NAION. Need objective endpoints, not just subjective improvement.
Use:
The endpoints have to separate true neuronal rescue from placebo, natural variability, measurement noise, and compensatory adaptation.
Best thread version
Post 1
I’m very familiar with the mouse paper that motivated this, the mechanistic rationale, and the hurdles for it to work in humans.But if it works, it’s historic.
Post 2
The key point: this is not just an “eye drug.”Retinal ganglion cells are CNS neurons. Their axons form the optic nerve.So success here would be evidence of functional rescue in brain-derived neural tissue.
Post 3
The 2020 mouse work was remarkable because OSK expression restored youthful DNA methylation/transcriptome patterns, promoted axon regeneration after injury, and reversed vision loss in mouse glaucoma and aging models.
Post 4
But the human translation is brutal.Delivery. Dosing. Expression control. Immune response. Cell survival. Neuronal identity. Dedifferentiation risk. Durability. Objective visual endpoints.
Post 5
The first win is safety.The second win is evidence of target engagement.The historic win is functional recovery: vision improvement or durable rescue in human optic neuropathy.
Post 6
The deep question is whether adult CNS neurons retain recoverable epigenetic information that can be safely accessed in vivo.That is why this trial matters far beyond ophthalmology.
Post 7
Best of luck to @davidasinclair and team.Cautious, but this is exactly the kind of translational shot the field needs.
Best “quote-tweet” version
This is why the trial matters.The eye is not just an easy clinical target. It is an accessible part of the CNS.If controlled OSK reprogramming can restore function in retinal ganglion cells, the implication is much bigger than vision alone.Huge caveats. Historic upside.
Best “not overhyped” version
Worth being precise here: this does not prove human rejuvenation yet.It is a first-in-human safety test of an epigenetic reprogramming therapy in optic neuropathy.But the reason people are excited is legitimate: the target cells are retinal ganglion cells, which are CNS neurons, and the mouse data showed functional rescue after OSK reprogramming.If that translates, it is a landmark.
Killer phrases
The eye is the proving ground. The real target is CNS rejuvenation.
Safety would be important. Biomarker movement would be interesting. Functional recovery would be historic.
This is not just ophthalmology. It is accessible CNS biology.
Retinal ganglion cells are brain-derived neural tissue in the eye.
The trick is not making cells young. The trick is making them younger without making them forget who they are.
Rejuvenation only helps if there are cells left to rescue.
In reprogramming, dose and duration are not details. They are the therapy.
The radical claim is not that cells can be made young. It is that aged CNS neurons may still contain recoverable state information.
Phase 1 is not a victory lap. It is the first controlled test of the idea in humans.
If it works, this is not just restored vision. It is functional CNS rescue.
Obscure thought inputs
The strongest scientific angle is identity-preserving rejuvenation. Full reprogramming erases identity and risks pluripotency. The therapeutic dream is partial reprogramming: recover youthful function while preserving mature cell fate. That is the razor’s edge.
The second angle is information vs damage. Sinclair’s broader framework is that aging is driven partly by loss of epigenetic information, not merely irreversible molecular damage. ER‑100 is an unusually direct clinical test of that thesis in humans. Wired quoted Sinclair describing this trial as the first opportunity to test whether restoring epigenetic information can ameliorate human disease.
The third angle is CNS regeneration dogma. Adult mammalian CNS neurons are famously poor at regeneration. That is why the optic nerve/retinal ganglion cell system is such a big testbed. A functional recovery signal would land much harder than a skin or blood-cell rejuvenation claim.
The fourth angle is local delivery as a safety compromise. The eye is attractive because intravitreal dosing is local and observable. If you are going to test partial reprogramming in humans, an ocular target is a rational first arena: accessible, measurable, paired-organ comparison possibilities, and lower systemic exposure.
The fifth angle is functional endpoint superiority. Epigenetic clocks and transcriptomic shifts are interesting, but vision is a hard, clinically meaningful outcome. If patients improve objective visual measures, the field changes.
The sixth angle is translation hierarchy. Mouse success is hypothesis-generating. Primate signals are encouraging but not definitive, especially if not peer-reviewed. Human safety and functional signals are the real threshold. Wired reports Life Biosciences says ER‑100 restored vision in monkeys, while Washington Post reporting noted earlier primate data had been presented but not yet peer-reviewed/published.
Claims to avoid or soften
Avoid:
“This will reverse aging.”
Use:
“This is a first human test of partial epigenetic reprogramming as a disease-modifying therapy.”
Avoid:
“Retinal neurons are the brain.”
Use:
“Retinal ganglion cells are CNS neurons / brain-derived neural tissue in the eye.”
Avoid:
“It restored vision in humans.”
Use:
“The trial is designed first to test safety/tolerability; efficacy remains to be shown.”
Avoid:
“The mouse paper proves this will work.”
Use:
“The mouse paper gives a mechanistic rationale, but human translation is the real test.”
Avoid:
“This regenerates dead neurons.”
Use:
“The likely therapeutic window depends on surviving, rescue-able retinal ganglion cells.”
Final recommended post
I’m very familiar with the mouse paper that motivated this, the mechanistic rationale, and the many ways it could fail in humans.But if it works, it’s historic.This is not just another eye therapy. Retinal ganglion cells are CNS neurons — brain-derived neural tissue in the eye — and their axons form the optic nerve.The original mouse work was remarkable because OSK partial reprogramming restored youthful epigenetic patterns, promoted axon regeneration, and recovered visual function in glaucoma/aging models.The human hurdles are enormous: delivery, dosing, expression control, immune response, surviving-cell requirements, neuronal identity, dedifferentiation risk, durability, and objective visual endpoints.Phase 1 is not a victory lap. The first win is safety.But the historic win would be functional rescue in human CNS neurons.Best of luck to @davidasinclair and team.
Best shorter version:
I know the mouse paper behind this well, and the mechanistic rationale is real — but the translation hurdles are enormous.Still, if it works, it’s historic.Retinal ganglion cells are CNS neurons, not ordinary peripheral tissue. So this is not just an eye-drug story; it’s a first serious human test of whether partial epigenetic reprogramming can restore function in brain-derived neural tissue.Huge caveats. Huge upside. Best of luck to @davidasinclair and team.

I’m very familiar w/the mouse paper that motivated this, mechanistic rationale and the hurdles for it to “work”… but if it does, it’s historic as retinal neurons are CNS (effectively “brain”). Best of luck @davidasinclair & team. nature.com/articles/d41586-0…
166

Jun 5
Beltz at al., Hierarchical classification of immune cell transcriptomes at population-scale. biorxiv.org/content/10.64898…
6
150

archive.md/Nfu5p
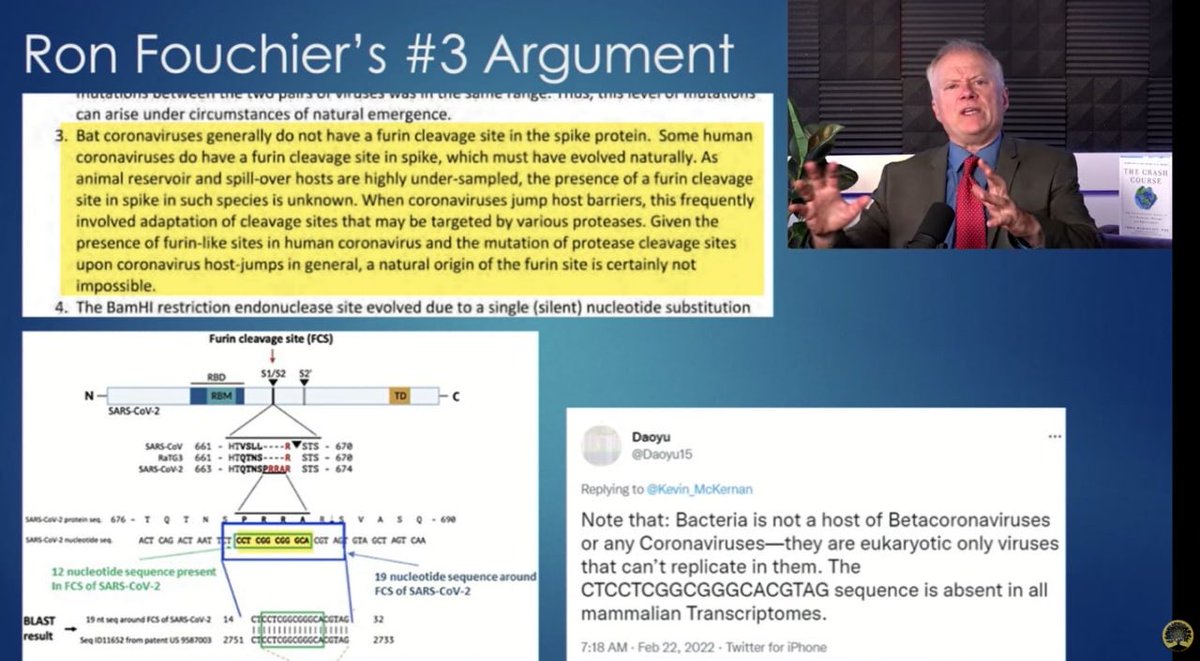
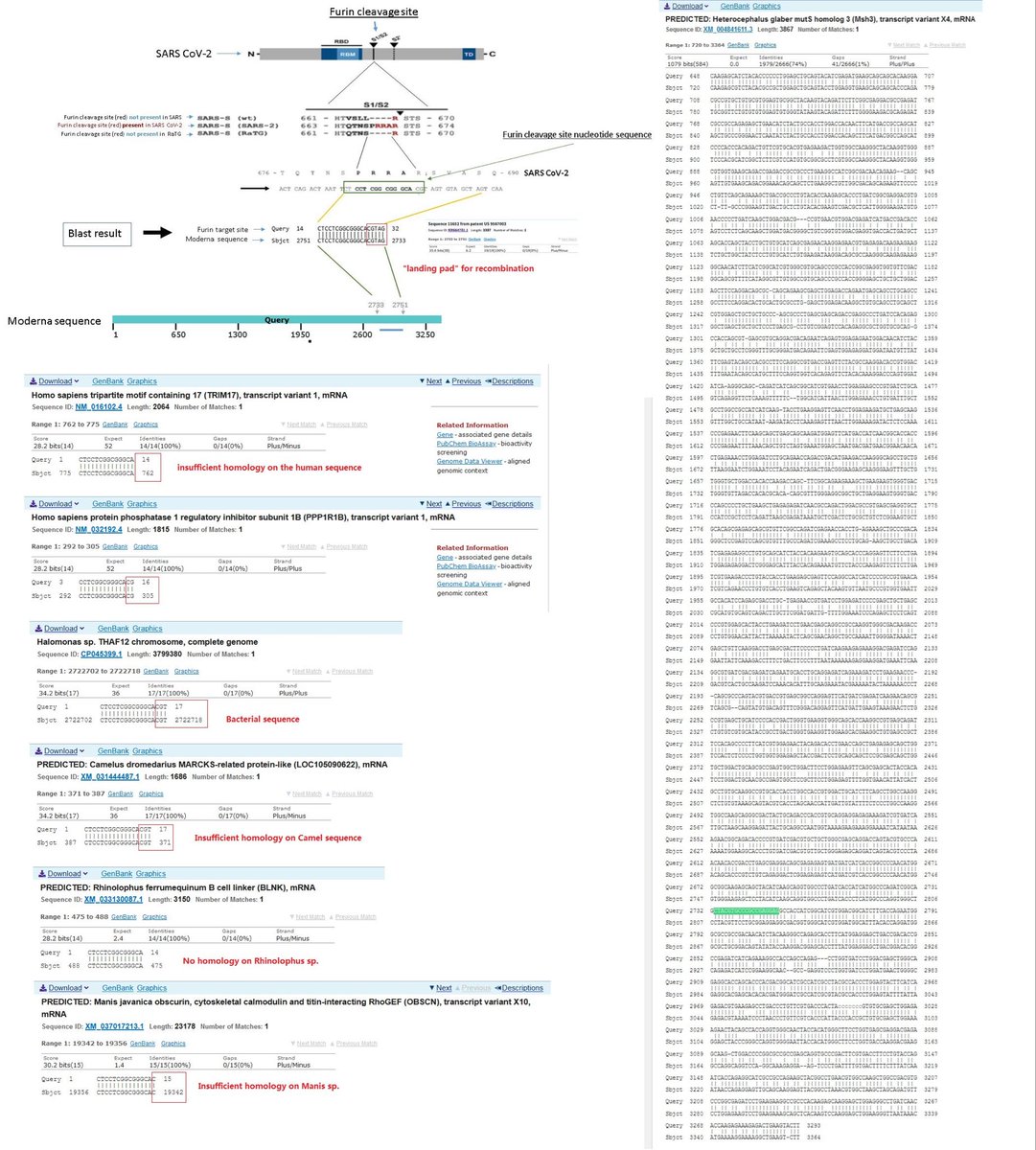
x.com/daoyu15/status/1700440…
Unfortunately, CTCCTCGGCGGGCACGTAG is absent in all viral genomes and mammalian transcriptomes. Mammals and humans do not have RNA genomes.
gab.com/Flavinkins/posts/108…

4
7
313

16/n It worked! For example, we recovered an allelic deletion series where some deletions overlap RBM3 while others spare it. In single-cell transcriptomes, only the RBM3-overlapping deletions reduced RBM3 expression, giving a clean genotype-phenotype link
1
3
424

Jun 3
@BrighamWomens and @HarvardMed team led by @VadimGladyshev found universal hallmarks of mammalian aging and mortality. They analyzed >11,000 transcriptomes from >25 tissues taken across 4 mammals (mice, rats, macaques, and humans) in a study in @Nature: ow.ly/1Zw650Z5CYo
!["Study provides framework for quantifying and targeting aging of cellular subsystems across species and tissues." [Close-up of animal cells.]](https://venexa.site/media/HJ6IMF3WsAAtED2.jpg)
ALT "Study provides framework for quantifying and targeting aging of cellular subsystems across species and tissues." [Close-up of animal cells.]
1
4
108

Jun 3
Integrative analysis reveals intra-tumoral microbial enterotypes shape host transcriptomes in colorectal cancer dlvr.it/TSs7mk
4
10
1,650