
Jun 16
the only adult accounts you can follow now are obviously bpd or hypermanic ppl, bc if you only post nudes without any personality outside toasted bread i cant tell you apart from the 10 000 bot accounts that does your niche but with better clothes, dressing and lightning you can never afford
43

we're supposed to get storms again later.
i need to have Ivy's syringe filled with gaba and ready to go.
aaaaaaand i just cleaned half the kitchen and i'm still awake from yesterday. this better not be the annual pre-solstice hypomanic or hypermanic episode starting already.
1
5
39

Jun 9
The way you swallow Palestinianist Islamist terrorist propaganda bullshit and regurgitate it here like a hypermanic moron says everything we need to know about you. May Allah in His infinite mercy purge you of Islamist terrorist lies and lying, ameen.
10
79

Different leadership styles exist:
1. Warren Buffett, the rational thinker who analyzes businesses;
2. Steve Jobs, the creative visionary; and
3. Elon Musk, the hypermanic operator juggling multiple ventures.
Associate these figures with their strengths:
Buffett for his patience and reasoning, Steve Jobs for product development and growth, and Elon Musk for exceptional operating performance.
7
1,300

Apr 23
You forgot loomer is now lewinskymaxxing...
She is on some hypermanic episode
2
12


I think he would be closer to being HYPERmanic. Excessively manic is closer.
This can certainly be the result of abuse of amphetamines in different forms.
5
161

Apr 11
I’d rather tweet coherent thoughts right through a hypermanic episode. I’d be punching my opps in the throat right now.
1
3
156

Apr 11
Did his nurse's training cover professional help for hypermanic TDS & ICE-DS? How about for viral dickitis? This twat seriously needs it.
3
44
Bipolar disorder is a debilitating condition that when untreated, can cause hypermanic episodes that MAKE you do erratic things you wouldn’t do in a controlled mental state. BUT being bipolar does not mean you escape the responsibility of the result of your actions during your manic episode.
Yes Matshidiso, bipolar disorder can be a lethal threat to you and the patient themselves. Bipolar disorder CAN make you kill people. Does that mean you can’t be charged with murder because you are bipolar? No.
Oh my goodness. The ableism towards and gross defense of Kanye is equally jarring.
6
8
217

stream ideas ive been throwing around:
- hypermanic streams like tadothon where i stream for 24 hours
- hypomanic stream where i act like a husk and can barely talk but im just watching youtube
- breaking a long fast with a bottle of vodka, a personal pizza, and leafy cosplay
LMK
1
18
390

any iteration of this song is awesome. the bubblegum aura reminds me a lot of you open.spotify.com/track/5O4hm… (i only chose this one bc this remix is the fastest i think but she has a "hypermanic" version which is just a sped up version of the original which is already fast lol)
1
2
55

Tbh ive had hypomanic moments while adjusting to meds and idk if I'd say I ever experienced a proper hypermanic episode
3
15

Mar 23
Me waking up and I'm still a short working class Italian-American (At least I'm hypermanic now)

3
120

Mar 10
I find that most days I can channel my general unceasing rage at the world in a way that lets me get a pretty good if hypermanic vibe going. Probably long term bad for my like heart or something but it's working for now
1
10
398

Mar 9
There is a point to be made here about how coming from a biological low state (high neuroinflammation, endotoxity, stress, and allostatoc load) to a high state feels like hypermania.
Every time I've taken a ride on this roller coaster, like from my burnout to single % bodyfat and razor sharp focus with clarity of reality that gives it high def natural psychedlic tinge, it was like a hypermanic state.
Not that I started doing crazy stuff, but it is clear that whenever I touched those states my writing would reflect that state, because the lucidity affords profundity of realizations that had to be shared.
It only took me a few rides to realize that there is very little value in that because those posts lacked a process and a practice for others to experience it, and my propositions alone don't mean anything.
In fact, once I had learned my lesson, I once told an acquitance who was not as familair with the rollercoaster that total darkness and total brightness are equally blinding, which to this day is perfectly suited metaphor for not just what one experiences in states on either side of the spectrum, but is equally a good lens to have for what people post or say since everthing is beholden by those states.
In general, I'm strongly oriented towards the invariant, for several reasons. And ultimately I found that the most valuable for others, and my own learning, to write about process, practice, and mechanism that foster deeper understanding and lead to experiences regardless of my state, since those aspects are indeed the invariant. It's been a good move.
Instead of writing out of state, and let that color the writing and admittedly its fleeting meaning, since it is bound by that state, I attempt to write with my soul and the convergence of my knowledge and experience. The latter feels far more timeless and prudent. Since writing from this point feels generative, whereas the other are more reactive.

The hypomanic edge is not discussed enough because almost every successful entrepreneur (in a traditional sense) has it, so it's taken for granted.
Being a little crazy is required for you to improve your life's situation but it's a double-edged sword.
It's like having access to fire.
Not everyone with hypomanic traits succeeds, most simply flame out.
It's better to approach it as a mild form of bipolar (BD-II) no matter what some crazy person (besides me) on the internet will tell you.
Here are some basic concepts in case any of you are interested.
First and foremost, BD-II involves disrupted connectivity and activity in certain neural circuits.
In the prefrontal cortex (PFC), which encompasses the ventromedial PFC (vmPFC) and dorsolateral PFC (dlPFC) (the vmPFC modulates amygdala activity, while the dlPFC supports planning and decision-making), dlPFC hypoactivity is noticed during depression and also reduced vmPFC-amygdala connectivity which leads to the person having a hard time controlling negative emotions.
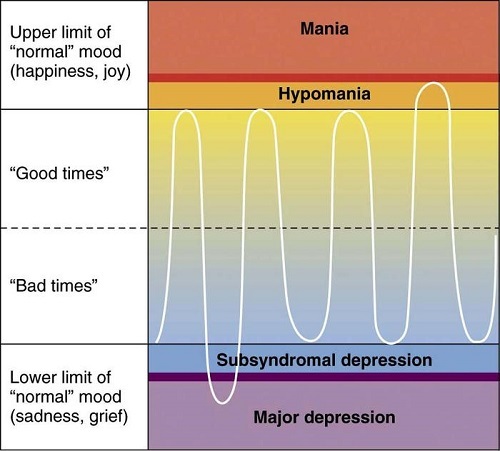
In hypomania, dlPFC hyperactivity drives impulsivity, and vmPFC overactivation enhances reward sensitivity.
Neuroimaging also shows reduced PFC gray matter volume and altered functional connectivity in BD-II.
Key note: Glutamate dysregulation (excessive NMDA receptor activity), reduced GABAergic inhibition, dopamine surges impair PFC function while neuroinflammation reduces PFC plasticity.
Another trait is increased amygdala excitability (the amygdala processes emotions such as fear, pleasure and reward modulating emotional reactivity).
During depression, amygdala hyperactivity amplifies negative emotions, contributing to sadness, anxiety, and rumination.
In hypomania, excessive amygdala activation drives reward-seeking, impulsivity and so on.
The role of the hippocampus is also interesting, where reduced hippocampal volume and impaired neurogenesis, driven by low BDNF and chronic stress, impair memory and emotional regulation.
There are also dysfunctions noted in the DMN (medial PFC, posterior cingulate cortex, precuneus) that mediates self-referential thinking and rumination and the salience network (ACC, insula) that processes emotional and reward-related stimuli.
In depression, DMN hyperactivity promotes rumination and negative self-focus, while the salience network is hyperresponsive to negative stimuli, amplifying distress.
In hypomania, the salience network overactivates in response to rewards and reduced DMN-dlPFC connectivity impairs emotional regulation.
Now let's talk about neurotransmitters.
In BD-II there's altered receptor sensitivity so focusing just on "balancing" neurotransmitters can be a mistake.
For example during depressive episodes, diminished 5-HT1A receptor binding in the PFC and hippocampus impairs emotional regulation, contributing to symptoms like sadness, anhedonia (loss of pleasure), and suicidal ideation.
Low dopamine and norepinephrine levels in the PFC also contribute to apathy and fatigue with norepinephrine dysregulation in the locus coeruleus disrupting arousal as well.
GABA-A receptor dysfunction is also noted during depression and lead to excessive neural excitability, manifesting as anxiety, irritability, and poor emotional regulation.
In hypomania, increased serotonin turnover may lead to overstimulation of 5-HT2A receptors, driving elevated mood, impulsivity, and risk-taking behaviors.
Dopamine also surges in the striatum and nucleus accumbens increasing reward-seeking behavior, impulsivity, euphoria and so on.
Excessive glutamate release and NMDA receptor hyperactivity in the PFC, hippocampus and amygdala also increase neuronal excitability, contributing to racing thoughts, impulsivity etc.
And on top of these, impaired GABAergic inhibition fails to counterbalance excitatory neurotransmitters like glutamate, amplifying impulsivity even more.
Finally excess muscarinic receptor activity is linked to depression and mania, with heightened cholinergic activity contributing to agitation in hypomania.
We also need to talk about ion channel dysregulation ( CACNA1C variants, such as rs1006737, are a major risk factor for bipolar disorder (they enhance L-type VGCC activity, increasing calcium influx and glutamate release) and SCN1A/SCN2A variants increase VGSC activity, correlating with hypomania).
Voltage-gated calcium channels (VGCCs) and sodium channels (VGSCs) are integral membrane proteins that regulate neuronal excitability, action potential generation and neurotransmitter release.
VGCCs (L-type, N-type, P/Q-type, T-type, encoded by CACNA1C, CACNA1D) control calcium influx, modulating glutamate, dopamine and serotonin release in the PFC, amygdala, hippocampus, and striatum.
In hypomania, excessive calcium influx via L-type VGCCs amplifies glutamate and dopamine release, increasing neuronal excitability and contributing to racing thoughts, impulsivity and reward-seeking behavior.
In depression, impaired calcium signaling disrupts PFC function, reducing excitatory drive and causing cognitive deficits and anhedonia.
Excessive calcium in the amygdala amplifies negative emotions as well.
Then, VGSCs (Nav1.1, Nav1.2, Nav1.6, encoded by SCN1A, SCN2A, SCN8A) regulate action potential generation and excitatory signaling in the PFC, amygdala, and striatum.
In hypomania, overactive VGSCs increase firing rates, amplifying glutamate and dopamine release, leading to racing thoughts and impulsivity.
In depression, reduced VGSC activity in the PFC impairs excitatory signaling, contributing to cognitive deficits (2016 study).
Mitochondrial dysfunction is also a central feature of BD-II and a very interesting one.
First, impaired pyruvate dehydrogenase (PDH) is noted.
PDH basically converts pyruvate to acetyl-CoA for the TCA cycle, producing ATP with thiamine pyrophosphate (TPP), derived from vitamin B1 being a critical coenzyme.
Impaired function leads to pyruvate accumulation and reliance on glycolysis, elevating lactate levels and causing energy deficits.
Magnetic resonance spectroscopy (MRS) studies show elevated lactate in the cortex of BD-II patients.
And finally let's talk about the hormonal influences.
First low testosterone in men and high testosterone in women with BD-II is noted.
BUT, in men with low testosterone, TRT can trigger mania so try to increase your testosterone levels through more "gentle" so to speak lifestyle interventions first.
Then, elevated cortisol is often noted and it disrupts PFC and hippocampal function, increasing glutamate excitotoxicity.
There's also some evidence that low DHEA and pregnenolone are noted, but these can just be a byproduct of high cortisol.
Do they play a role? Of course and low levels will impair inhibitory control.
Hypothyroidism or subclinical thyroid dysfunction is also common in BD-II, particularly during depression.
Elevated adrenaline in hypomania, driven by norepinephrine surges, also amplifies arousal and impulsivity, disrupting PFC regulation.
Now here are some steps/interventions/tests you can consider none of which should be used as a substitute for medical advice.
Number 1: Go camping for a weekend if you can.
This might sound weird, but just 1 weekend of camping is shown to shift melatonin onset 1.4 hours earlier which is perfect for people with BD-II.
Number 2: Bright light first thing in the morning for 15-20 minutes (go outside).
Number 3: IR-Sauna during depressive episodes (it's even more effective than working out).
Number 4: Avoid stimulants (nicotine included), sugar, gluten, MSG and A1 dairy.
Nicotine for example amplifies VGCC/VGSC activity.
This also includes supplements that can have quite strong dopaminergic effects.
Number 5: Reduces pyruvate/lactate levels by going lower on carbs and using small doses of B1 or going keto.
Number 6: Magnesium (500 mg/day) acts as a natural L-type VGCC blocker by binding to the channel’s pore, reducing calcium influx and glutamate excitotoxicity in the PFC, amygdala and hippocampus. It also enhances GABA-A receptor function.
Number 7: Taurine (500–1000 mg/day (start with this amount and you can go up to 3 grams)): Modulates VGCCs/VGSCs and GABA.
Number 8: Lithium orotate (start with just 2.5mg and go to 5mg if you don't notice anything after 10 days) inhibits inositol monophosphatase and glycogen synthase kinase-3 (GSK-3), reducing IP3-mediated calcium release from ER stores.
It also downregulates L-type VGCCs, decreasing calcium influx and glutamate release in the PFC and amygdala.
Number 9: Go measure your vitamin D levels.
Vitamin D regulates CACNA1C expression and calcium signaling (vitamin D deficiency is linked to increased VGCC activity and mood instability in bipolar disorder).
Number 10: NAC (mitigates glutamate excitotoxicity).
Number 11: L-Theanine/lemon balm/valerian/chamomile (enhance GABA).
Number 12: Check your ferritin.
Number 13: Check for vanadium.
Number 14: Ignore social media if you don't use them for anything serious.
Number 15: Consider using 10mg of PLP and go up to 20mg.
Number 16: Blackseed oil.
Number 17: Whole food vitamin C.
Number 18: Managing exposure to nnEMFs.
Number 19: Eat breakfast (to prevent any excessive and pointless cortisol spike) and don't fast.
That's all, these were the absolute basics.
But: DO NOT use any strong serotonergic supplement/tool when depressed if you have BD-II because you might induce hypomania.
Point being: Self-made success and craziness are close siblings.
Study it, understand it and control it.
2
162



Jan 26
The penguin's not depressed, it is hypermanic. The euphoria it feels makes it ignorant of death.
4
1,047

Jan 18
I feel so empty numb depressed for the past couple days i cba to do anything hopefully a brief wave of hypermanic delusion hits me to balance my emotions so I can get back to normal
1
3
190