
Blocking moronic assholes who just add noise not signal
Joined January 2010
- Tweets 10,996
- Following 1,380
- Followers 382
- Likes 4,626
305 Photos and videos





Jay Kusnetz 💜 retweeted

It’s funny, motocross at the White House is, like, fine with me. But here’s an example of something that is genuinely unforgivable but that a lot of people seem to have moved right past.

80
704
6,030
166,730
Jay Kusnetz 💜 retweeted

Jun 10
During the Holocaust, European Jews actually did petition for refuge in Alaska (Google the Slattery Report). They were denied and perished.
That’s exactly the point.
Jewish survival cannot depend on finding some piece of land where everyone else agrees Jews are allowed to live.

If Israel was created in Alaska, no Palestinians or Arabs would've objected!
The issue is NOT Jewish statehood, the issue is building a state on top of OUR land, stealing OUR homes, properties, assets, farms, culture, & olive trees then caging us in concentration camps!
61
239
1,901
56,377
Jay Kusnetz 💜 retweeted

Jun 7
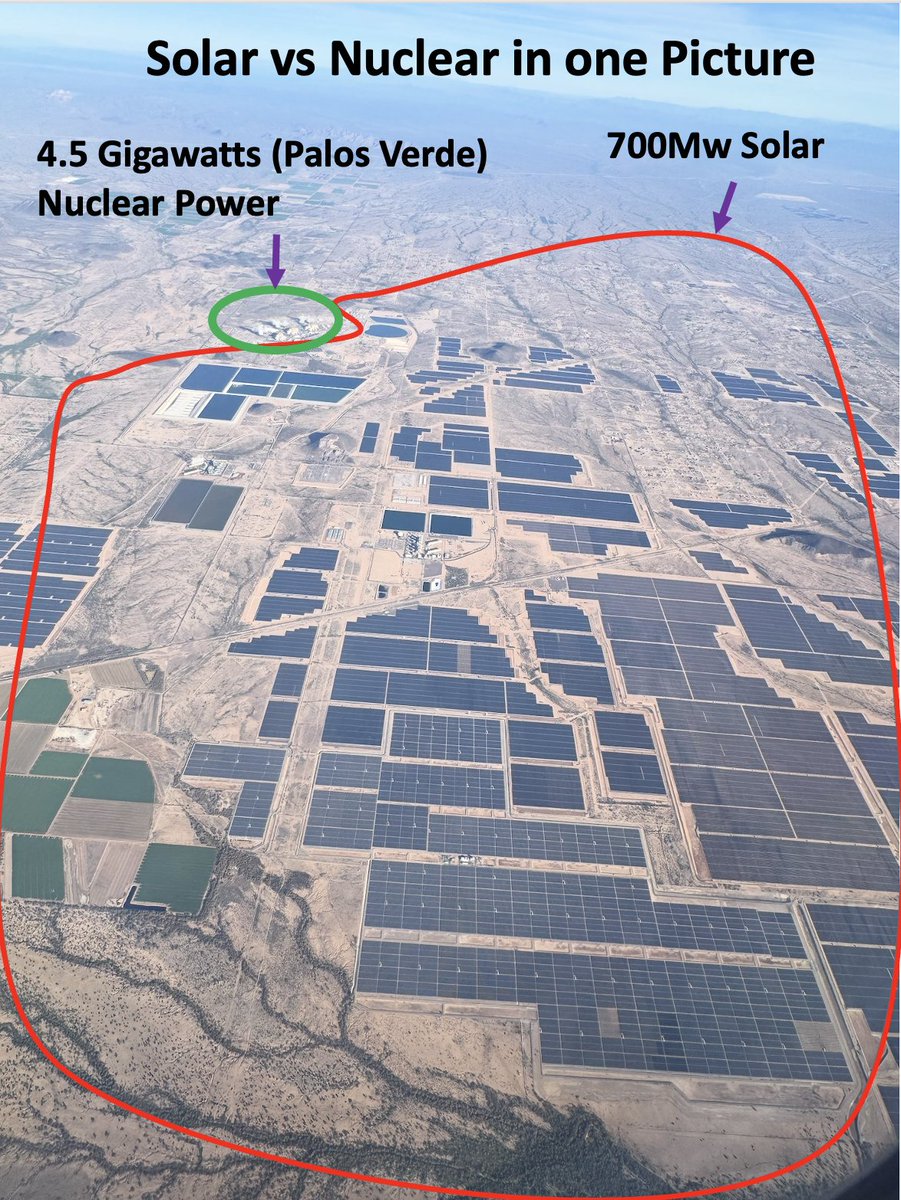
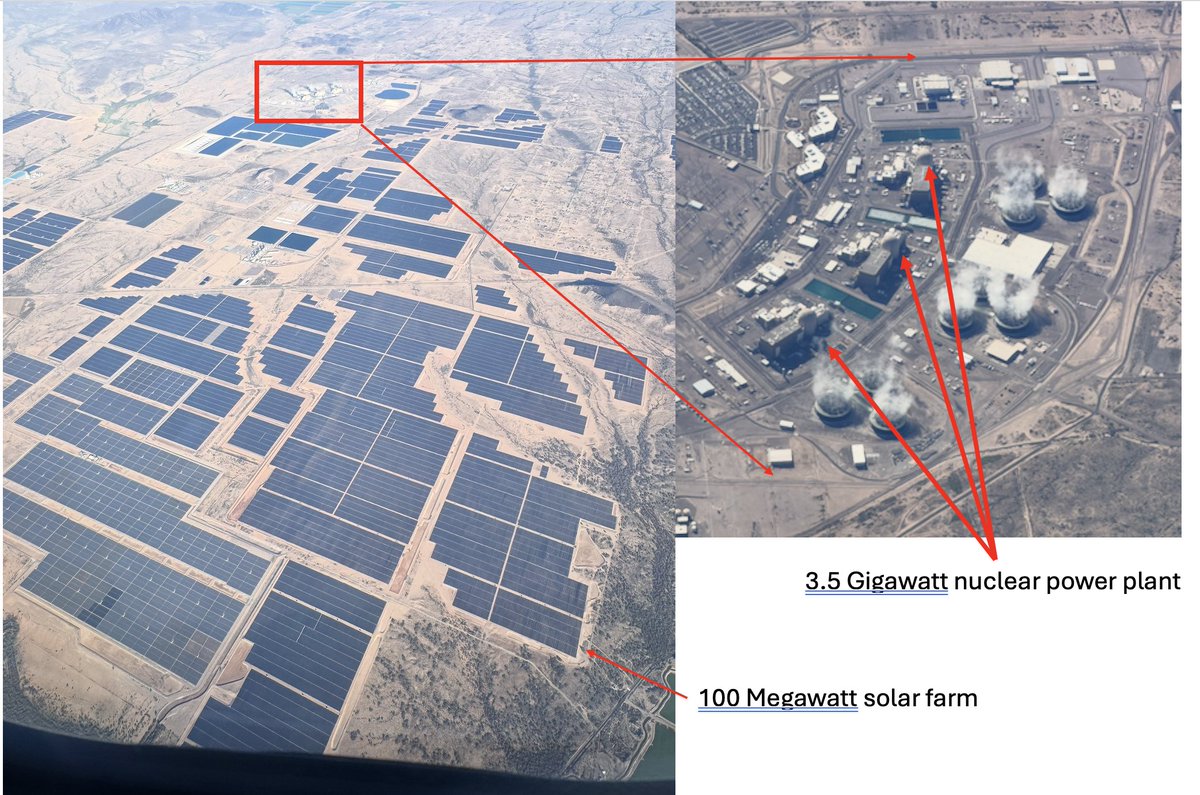
That picture shows why we can't use them to run an industrial civilization of 9 billion people.
It turns land into a desert monoculture.
18
9
66
3,640
Jay Kusnetz 💜 retweeted

May 27
🦊 🦊🦊🦊 Sake!!!
Apparently suggesting aerosol scientists, engineers, industrial hygienists, and ventilation experts should help shape infectious disease policy is controversial now.
You know… the same types of people responsible for:
clean water systems
sewage infrastructure
filtration
occupational safety
hospital ventilation
indoor air standards
Instead we’re told to “trust the experts” after years of public health agencies fumbling airborne transmission guidance, removing aerosol language from websites during outbreaks, and acting like respirators are exotic technology from the future.
Meanwhile the “random guy on the internet” they’re dismissing:
has a PhD
works in a College of Applied Health Sciences
teaches Tech-Driven Health Interventions
studies behavior, cognition, health technology, and intervention design
and understands the physics behind why respirators, ventilation, filtration, and germicidal UV work
But sure. Better to keep pretending infection control begins and ends with hand sanitizer and vibes.
7
141
483
4,435
Jay Kusnetz 💜 retweeted

May 21
The whole IPAC PRECAUTIONS paradigm used in healthcare is fundamentally wrong
It's been wrong for decades
So long in fact that it's become enshrined in stone
Fossilized
Immutable
Regarded as a Universal Truth
In reality it's a Fundamental Lie
6
57
184
5,541
Jay Kusnetz 💜 retweeted

May 21
Millions of people got sick, then got sicker — and then stopped getting better.
They came back with normal labs. Unremarkable imaging.
And the quiet suggestion that maybe the problem wasn't biological.
Long COVID didn't just introduce a new illness. It exposed how modern medicine responds when suffering can't yet be measured.
Modern healthcare systems struggle with:
- Illness without measurable biomarkers
- Symptoms that fluctuate and defy categorization
- Patients — especially women — whose suffering outpaces the science
- Chronic complexity in a system built for acute resolution
What Long COVID revealed was already there.
Patients with ME/CFS, fibromyalgia, and dysautonomia (like POTS) had been describing this reality for decades.
Long COVID just made it impossible to ignore.
In this essay, I explore:
- Why Long COVID exposed cracks in medicine that existed long before the pandemic
- How "we can't explain this" quietly became "this may not be real"
- Why chronically ill patients already knew this story
- How a system built for acute disease failed millions with chronic illness
- Why Long COVID's research funding is catastrophically misaligned with its actual harm
- And what medicine still owes the patients it dismissed
open.substack.com/pub/britta…
49
320
1,010
23,910
Jay Kusnetz 💜 retweeted

REMEMBER THIS?
This wouldn’t have happened if I didn’t fix the problem that 15 experts you paid to come from Europe said they need at least 8 to 10 months to fix the issue!
Remember that you said “FUCK! if we need to delay it until 2013 I am out of Money!
I Fixed it in 10 DAYS

3
4
31
983
Jay Kusnetz 💜 retweeted

May 17
Invisible Warfare
Headline: The MIT Study that Finally Visualizes the Brain-on-COVID
Have you ever had a medical scan come back "clear" while your brain felt like it was made of inflamed concrete? You aren't crazy. Standard medicine just wasn't looking small enough.
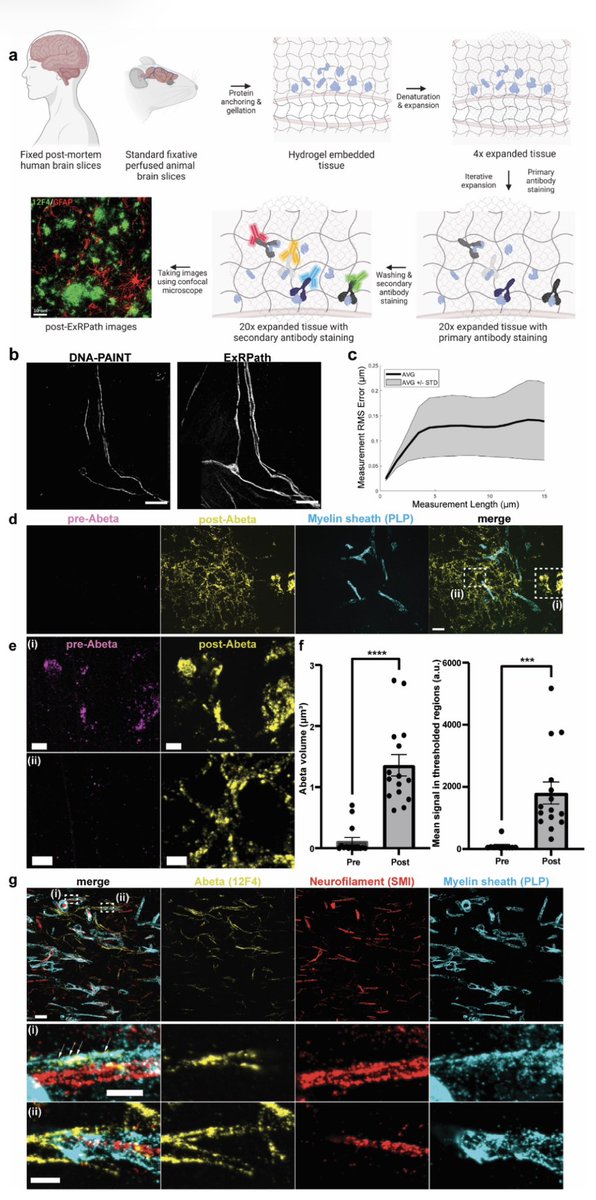
A major 2026 paper from MIT and Harvard just changed the game. They didn't just look at brain tissue; they physically expanded it 15-20x its size—like using a molecular magnifying glass—to achieve 20-nanometer resolution.
What they found changes everything:
Standard imaging looks for damage. This paper visualized defense.
Deep inside the brains of people who had SC2, they found periodic Amyloid Nanoclusters co-localizing directly with the virus.
What does that mean?
The Cargo: Your body is running on infected, hyper-activated platelets (the 'weaponized platelets' of LC). They carry viral debris and proteins into the brain's capillaries.
The Body's Defense: When the brain detects these viral invaders, it doesn't wait. Its immune system (microglia/astrocytes) triggers a protective, antimicrobial "foam" called amyloid-beta.
The Trap: This amyloid foam physically traps, cages, and neutralizes the viral proteins to stop them from causing further harm.
The Price: The paper found a 2-fold increase in activated astrocytes, the cells that manage the brain's environment. These dense, sticky amyloid traps and swollen astrocytes create a state of permanent, local, architectural neuroinflammation.
This isn't a "chemical imbalance." This is structural warfare. The brain is filled with tiny, persistent defensive knots that it cannot clear, causing the profound fatigue, cognitive impairment, and severe inflammation so common in LC.
#LongCOVID #Neuroinflammation #Microbiome #VigilanceLab
A comic showing this! Hope this helps my friends and fellow humans.
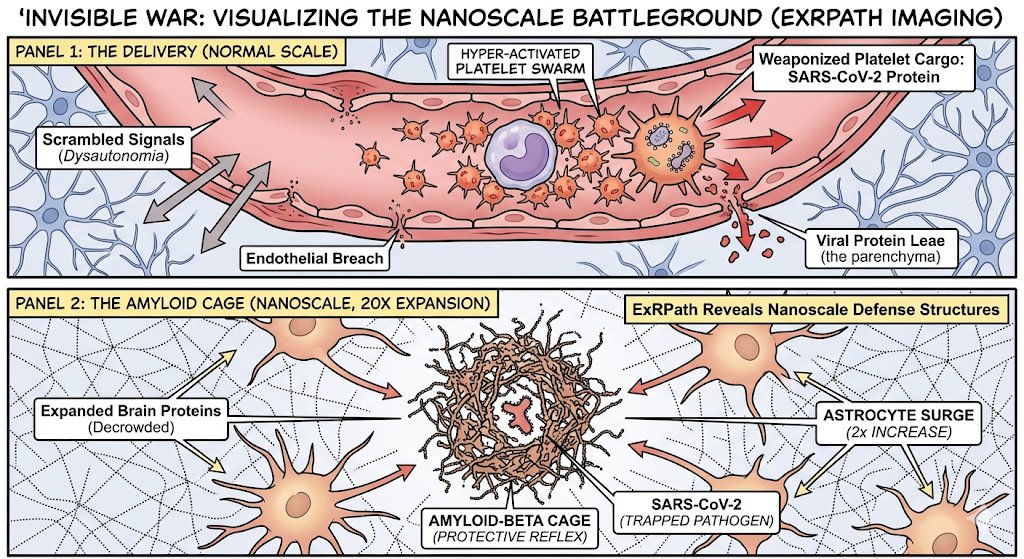
ALT Panel 1 (The Delivery): Infected, hyper-activated platelets swarm and breach the brain capillary wall, leaking viral protein cargo into the brain parenchyma and scrambling neurological signals. Panel 2 (The Amyloid Cage): 20x tissue expansion reveals the nanoscale defense. The brain sprays an "amyloid-beta cage" to trap the viral pathogen, triggering a massive, persistent astrocyte inflammatory surge.
May 17

SARS-CoV-2 spike protein may directly amplify brain inflammation.
➡️ Researchers found that spike proteins can colocalize with amyloid-β (Aβ) and trigger distinct inflammatory responses in microglia — the brain’s immune cells.
➡️ This raises important questions about potential long-term neurodegenerative consequences of COVID-19. 1/
14
249
549
19,310
Jay Kusnetz 💜 retweeted

1
1
15
Jay Kusnetz 💜 retweeted

May 16
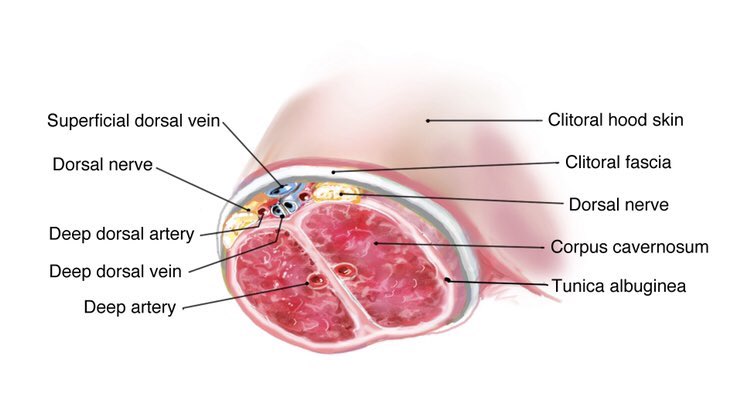
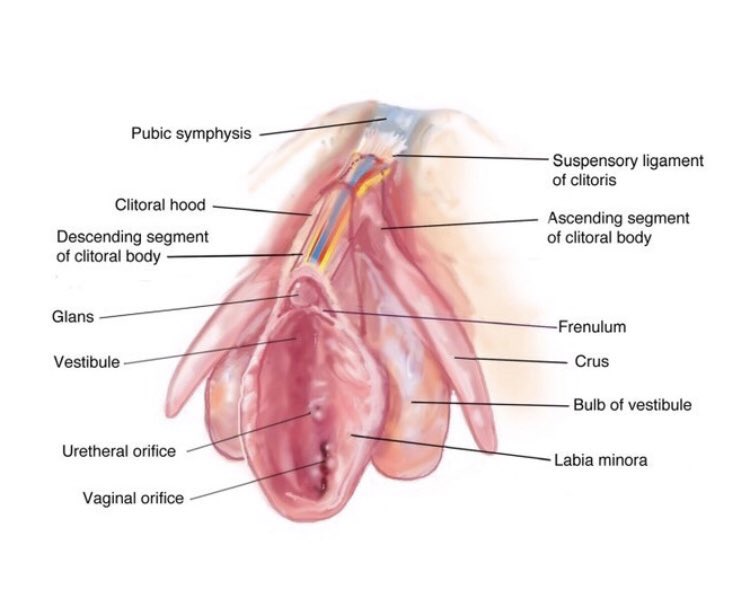
Since people apparently have missed the memo, FYI I am not just randomly obsessed with clits.
I’m an activist for prevention of medical female genital mutilation because I was mutilated when I was barely 18 years old.
My OB/GYN cut into my clitoris without my consent and damaged it permanently.
This happened because of widespread censorship of anatomy known since 1672 from medical education and institutionalized disregard for female sexual function.
This problem applies to ALL procedures involving this anatomy. It also causes there to be no help for women with damage caused by accidents or childbirth or with clitoral/vulvar causes of sexual dysfunction.
I’ve changed 20 major medical textbooks, 6 online resources, 2 top anatomy apps, virtual dissection tables, anatomy posters, consent forms, medical org websites, board exams, etc.
Here’s a poster I got updated to include clitoral anatomy. It’s still wrong.
17 Jun 2020

Hi! Whether you‘re a doctor or layperson, please share this message.
1. #Anatomy of the clitoris should be covered in the same depth as that for other organs.
2. #femalesexualmedicine should have anatomic basis.
3. Doctors who operate on vulvas should know clitoral anatomy.
6
12
68
5,248
Jay Kusnetz 💜 retweeted

The Swiss Re Institute suggests COVID will kill about 150,000 Americans this year (excess deaths), so it's more like a bad cancer than a bad flu.
I would suggest talking to scientists who do Covid research and continue to take it seriously. My wife and I lead separate PhD programs. We homeschool so that our children do not experience the brain damage and other health problems from reinfections, which continue to pose a serious burden in 2026. It remains the most common chronic health condition in kids.
A key reason why it might appear "milder" is that about 2 million Americans have died from COVlD (excess deaths). Wipe out 2 million people most vulnerable to any health problem, it will almost always appear acutely milder.
20
356
1,334
17,135
Jay Kusnetz 💜 retweeted
May 12
There are now more than half a million scientific publications related to COVID-19 and a rapidly growing body of evidence linking SARS-CoV-2 infection to immune dysregulation, microvascular injury, autonomic dysfunction, clotting abnormalities, viral persistence, and measurable cognitive changes.
And to the people constantly sick, exhausted, dizzy, forgetful, exercise intolerant, waking up to feeling like you got hit by a truck on the daily or suddenly developing strange inflammation, heart issues, GI problems, or “mystery” symptoms after repeated infections…
At some point you and society as a whole must confront the reality that repeated infection with a vascular and neurotropic virus was never as harmless as everyone wanted it to be.
I choose to live in reality.
That virus is still here. It is still spreading through the air. And it is still associated with long-term vascular, immune, and neurological consequences for many people.
Protecting yourself from that threat — through cleaner air, better ventilation, filtration, vaccination, and high-quality masks in high-risk settings — also reduces your risk from many of the other respiratory pathogens constantly circulating around us.
And if you are tired of watching people suffer while being told this is “normal,” then start demanding urgency.
Ask why Long Covid clinics are closing instead of expanding.
Ask why immunologists, virologists, neurologists, vascular scientists, and pathologists are not being funded at Manhattan Project scale to investigate viral persistence, immune dysfunction, clotting, mitochondrial damage, and cognitive impairment.
Ask why billions can appear overnight for almost anything else, but millions living with chronic illness are told to “pace themselves” and move on.
Support researchers (the ones who are still focused on Long Covid that don’t conflate the disease)
Support clean air initiatives (two strong efforts happening in Illinois right now! Help us!!).
Support disability advocacy.
Pressure institutions to improve indoor air quality.
Stop mocking people for protecting themselves.
And stop accepting “everyone is sick all the time now” as a normal feature of modern life.
51
506
1,373
28,555
Jay Kusnetz 💜 retweeted

Hey I'm off private for the first time in ages, retweet this if you want to help me get back to my friends feeds OR if you want to make anti-maskers and homophobes really mad 🤷♀️🙏🌈

ALT Lulu, with long rainbow hair, wearing a light blue k95 mask
19
132
504
6,462
Jay Kusnetz 💜 retweeted
May 10
Any questions?
The reactors are at Palos Verde nuclear power plant in Arizona.
It also produces power at night and cloudy days.
95% capacity factor.
7
8
52
1,687
Jay Kusnetz 💜 retweeted

May 5
Imagine being a scientist investigating vaccines in the U.S. After years of research and millions spent, your study is blocked from publication because your data doesn't support RFK's and the FDA's battle against vaccines. This is why people like me were forced to leave.
May 5

Breaking News: The FDA has blocked publication of research that found widely used Covid-19 and shingles vaccines were safe. nyti.ms/49dtF24
424
7,091
24,342
469,067
Jay Kusnetz 💜 retweeted
What if you could talk to your Bookmarks.
linkagogo.com/blog/prompt-ba…
1
13
Jay Kusnetz 💜 retweeted

Apr 30
Why did nobody warn you? I can tell you. Late March 2020, I was part of the COVID taskforce of the German Interior Ministry. In our first report from 27 March, we were probably the first in Western countries to warn about long-term sequelae from COVID, based on experience with SARS (2003) and data about COVID from China. We also argued against herd immunity strategy. A few days later, the German government abandoned herd immunity. But we, and I personally, were violently attacked by influential German right-wing media, followed by major mainstream media, including moderate left-wing. A massive defamatory media campaign. My university threatened to fire me (they actually did a few months ago). That's how mainstream media and the academic community silenced those who knew and warned.
56
837
2,757
77,286
Jay Kusnetz 💜 retweeted

May 1
There's a common misconception that Brutalist buildings were unpainted, but thanks to microscopic analysis of the exteriors we can now recreate what they looked like in their prime.

443
3,329
39,373
7,428,075
Jay Kusnetz 💜 retweeted

Apr 30
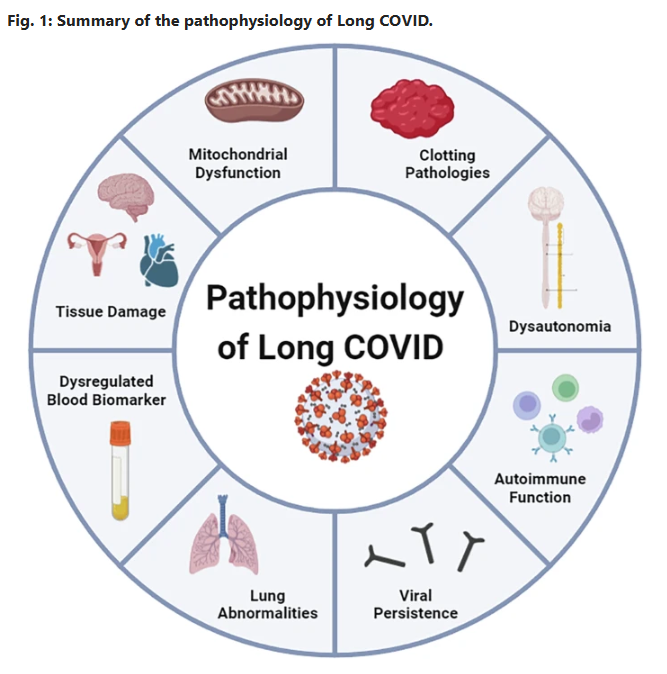
Current status and future perspectives on the mechanistic and pathophysiological understanding of long COVID
🚨JUST DROPPED YESTERDAY and rips open the black box of Long COVID:
Viral persistence up to at least 24 months. Fibrin microclots that laugh at fibrinolysis. Autoimmune storm. Mitochondrial sabotage. An up-to-date full mechanistic map is finally here!
No more guessing. This changes everything, let’s dig into this overview👇, better yet…..read it yourself!! #MustRead
➡️Global Impact & Context:
- Long COVID (PASC) affects >400 million people worldwide, incurring >$1 trillion in annual economic costs,
- Core symptoms, debilitating fatigue, cognitive dysfunction (“brain fog”), sleep disturbances, and post-exertional malaise (PEM) in 50–80% of cases, persist months to years’ post-infection, with a mechanistic overlap to ME/CFS,
➡️Core Mechanisms:
1. Immune Dysregulation:
- Persistent systemic inflammation features elevated cytokines (IL-6, TNF-α, IL-1β) detectable up to 14 months, driving T-cell exhaustion (reduced CD8 IFN-γ/TNF-α production) and monocyte activation (COX-2, IL-8Rβ, CXCR6),
- Autoantibodies (anti-GPCR, anti-PITX2, anti-FBXO2, ANA/ENA) persist 12–14 months and correlate directly with fatigue, dyspnoea, palpitations, and cognitive impairment with molecular mimicry, gut dysbiosis and latent herpesvirus reactivation (EBV, HHV-6) amplifying autoimmunity,
2. Viral Persistence & Reactivation:
- SARSCoV2 RNA, spike protein, and antigens remain detectable in brain, muscle, gut and plasma up to 14–24 months in ~60% of cases, fuelling chronic low-grade inflammation,
- EBV/CMV reactivation signatures are common with spatial transcriptomics highlighted as a possible next tool to map tissue reservoirs,
3. Endothelial/Microvascular Pathology:
- Glycocalyx shedding (elevated SDC-1), capillary rarefaction and endothelin-1 elevation create a pro-thrombotic state,
- Platelet hyperactivation releases vWF/FVIII, forming anomalous fibrin(ogen) microclots that resist fibrinolysis and these circulate and fragment during exertion, causing hypoxia, ischaemia-reperfusion injury, and PEM,
4. Autonomic Dysfunction:
- Present in ~50% of patients (POTS predominant), driven by hypovolaemia (70%), small-fibre neuropathy (20–40%), vagus-nerve damage and microclot-induced compensatory tachycardia with 4-fold norepinephrine spikes,
5. Mitochondrial Impairment & Neuroinflammation:
- Skeletal-muscle biopsies show reduced respiration, cytochrome c oxidase activity and WASF3-mediated supercomplex disruption, producing rapid lactate rise and PEM within 48 h,
- Systemic cytokines breach the blood–brain barrier, sustaining microglial activation and cognitive sequelae,
➡️Diagnostic & Therapeutic Gaps:
- No validated biomarkers or subtype-specific criteria exist.
- Graded exercise is contraindicated.
- Observational promise exists for IVIg, low-dose naltrexone and apheresis, but large RCTs are urgently required.
➡️Future Priorities:
Calls for subtype-specific research, large-scale RCTs, advanced techniques (spatial transcriptomics, proteomics), and interdisciplinary collaboration to develop precision diagnostics and therapies.
‼️This exceptional review delivers a masterful, evidence-based roadmap that not only clarifies Long COVID’s complex pathophysiology but stimulates the scientific community toward urgently needed mechanistic breakthroughs and effective, patient-centred interventions.
‼️Bottom line: Long COVID is not a single disease but a complex, multisystem condition that can impact your life seriously!
#AvoidSars2 #AvoidReinfections
A huge thanks to all authors, @DrMark_Faghy @DavidJoffe64 @PutrinoLab @DaniBeckman @resiapretorius @Sunny_Rae1 are only some of them!👏👏
nature.com/articles/s43856-0…
28
373
772
17,133
Jay Kusnetz 💜 retweeted

Apr 29
This statement is disingenuous because it deliberately abandons science, proportionality, and regulatory process in favor of fear, accusation, and moral panic.
First, it asserts causation without evidence. Claims like “pesticides are giving kids cancer” are presented as settled fact, not as hypotheses to be tested.
Regulatory science, however, does not operate on slogans. It distinguishes clearly between hazard - whether a substance can cause harm at some dose - and risk - whether real‑world exposure actually causes harm.
Glyphosate (and all pesticides) are repeatedly reviewed by the EPA and other regulators specifically on exposure and cancer risk, not on abstract hazard alone. Declaring causation while ignoring exposure data is not an argument; it is an assertion.
Second, it replaces regulatory science with jury outcomes. Civil juries decide liability, not toxicology, dose‑response relationships, or population‑level risk. They evaluate narratives under tort law, not exposure models or epidemiology.
Treating jury verdicts as scientific proof is a category error. Courts are not risk‑assessment bodies, and they were never designed to be.
Third, it misrepresents what is meant by “immunity.” EPA preemption is framed as a “get‑out‑of‑court‑free card,” when in reality it is about legal consistency. If a product meets federal safety standards, claims about harm from label‑compliant use must align with that determination.
This prevents science‑by‑lawsuit, not accountability for fraud, misuse, or negligence. Calling this “immunity” is rhetorically powerful - and factually false.
Fourth, it collapses all pesticides into a single moral category. Phrases like “every pesticide, every herbicide, every insecticide” erase critical differences in chemistry, mode of action, exposure profiles, and regulatory decisions.
This is classic motte‑and‑bailey framing: an emotional attack on one product is used to justify blanket condemnation of an entire category.
Fifth, it uses children to shut down scrutiny. Invoking “actual children are dying” is an escalatory tactic designed to pre‑empt questions, delegitimize disagreement, and replace evidentiary thresholds with moral outrage. Invoking children does not strengthen weak evidence; it substitutes for it.
Sixth, it frames fear as proof. Statements like “it’s being placed in the food supply” omit essential context - dose, exposure, and residue limits - that regulators evaluate explicitly. This omission is not accidental. Fear does the work that evidence cannot.
Finally, it accuses corruption without evidence. Rhetorical questions about who is “getting paid” or whose spouse might be “on the payroll” are insinuation masquerading as accountability: no proof, just suspicion. It is a textbook tactic when facts cannot carry the argument.
In short, this is not a safety case. It is the deliberate manufacture of fear, presented as concern, and outrage substituted for risk assessment.
11
20
148
3,351