
Joined March 2021
- Tweets 953
- Following 180
- Followers 566
- Likes 5,324
118 Photos and videos















Pinned Tweet

May 22
One thing I think people are massively missing in the GLP-1 / retatrutide debate:
The populations in these studies are usually:
-older
-severely overweight or obese
-metabolically unhealthy
-often sedentary
-low protein intake
-not resistance training
-on multiple cardiometabolic medications
Then people in the biohacker / fitness space who are already 12–20% body fat, resistance training 4–6x/week, eating high protein, optimized hormones, good sleep, etc try to directly apply those outcomes to themselves.
That’s where a lot of the confusion comes from.
People keep making blanket statements like:
“Look how much muscle loss happens on GLP-1s.”
But in my clinical experience, younger healthier metabolically optimized patients often preserve muscle VERY well especially when:
-protein is adequate
-resistance training is present
-weight loss is gradual
-hormones are optimized
-sleep/recovery are good
Taking a 40-year-old lifter from 20% body fat → 15% body fat is NOT the same physiological situation as taking a 72-year-old sedentary diabetic from 38% body fat → 25%.
Those are completely different humans with completely different metabolic environments.
This is why individualized medicine matters.
The real nuance isn’t:
“Tirzepatide vs Retatrutide”
or
“GLP-1s are good/bad”
The real nuance is:
-Who is the patient?
-What is their starting point?
-What are their goals?
-What are they doing with training, protein, hormones, sleep, and lifestyle while using these tools?
28
16
260
34,688
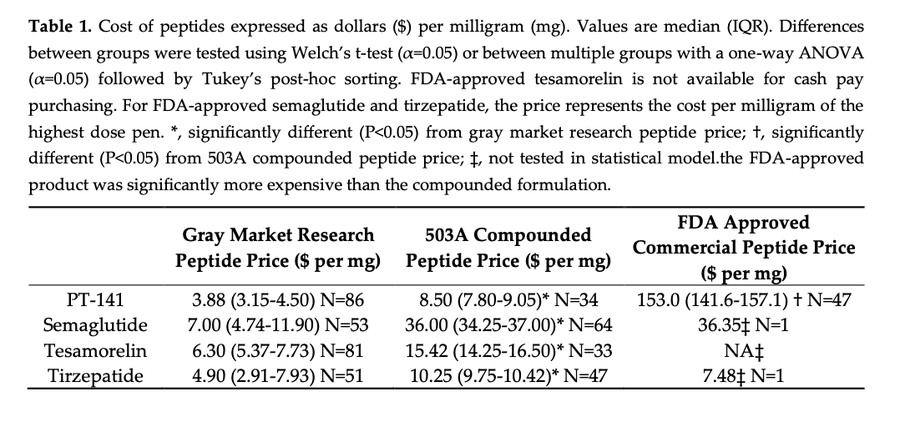
cRAZY hOW ExPensIVE cOMpOunDEd & bRAnD-NamE pEPtiDEs Are!!! tHEy OnLY cARe aBOuT mOney!
-then shills affiliate link where they get 30-50%
This is like saying:
• "Why is electricity expensive when sunlight is free?"
• "Why is bottled water more expensive than rainwater?"
• "Why is peanut butter more expensive than peanuts?"
• "Why is a meal at a restaurant more expensive than buying the same ingredients at the grocery store?"
Because you're not paying for the molecule.
You're paying for:
-Professional time & overhead (rent, payroll, utilities)
-Sterility / testing / quality control
-Regulatory compliance / documentation
-Liability / accountability
So funny for me, as an ND, to have to defend Eli Lilly and other pharma companies. Are a lot of their prices criminally high? 100%. Are they the same product when you buy them from the gray market? Absolutely not.
Of course raw peptide powder is cheaper.
The real question is whether the savings are worth the increased risk of contamination, mislabeling, dosing errors, impurities, endotoxins, and having nobody accountable when something goes wrong.
4
1
5
2,485
Jun 12
Neighbors are trying to murder you...
BUtT dA sToCK MArKEt iS At aN aLl TImE HiGh!!!!
Jun 11

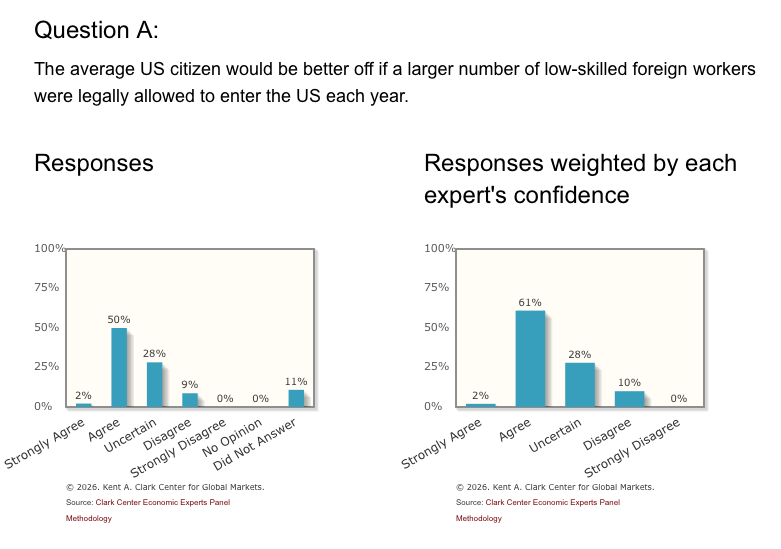
When economists were asked if Americans would be better off with more low skilled immigrants being allowed to legally enter the country, they said yes by a 6-1 ratio. On skilled immigration, it was 100%. But chuds disagree, they have their own indigenous ways of knowing.
59
Jun 11
Many things “Suppress Dopamine”
-BPC-157
-Magnesium, taurine, theanine, glycine, and other GABAergic compounds dampen excitatory tone.
-Meditation can reduce craving/reward-seeking circuitry.
-Sleep suppresses wake-promoting dopamine/catecholamine activity.
-Even caffeine, exercise, fasting, and stress all shift dopamine signaling depending on dose and context.
The question isn’t “does NAC affect dopamine?”
The question is: does NAC reliably suppress dopamine signaling enough to cause clinically meaningful anhedonia in humans?
Jun 10

you should definitely NOT use NAC daily
NAC suppresses dopamine receptor sensitivity through glutathione's effects on cystine/glutamate exchange
that means you're blunting the reward circuitry that makes life feel good.
anhedonia will creep in because you're constantly resetting dopamine signaling if you dose it daily
dose NAC at night on off-days from dopaminergic compounds. once or twice a week should be enough for most people.
if you're trying to fight depression or OCD, go weekly. but know that the goal is for you to feel less.
2
177
Dr. Michael Moeller, ND retweeted

BREAKING: Ozempic / Wegovy linked to ~30% lower breast cancer risk in 111,000 women (new Penn Medicine study at ASCO 2026).
Even bigger: Women already diagnosed with breast cancer who took GLP-1s were 50% less likely to progress to Stage 4 (Cleveland Clinic data).
Prevention slowed progression.
Here's what the studies actually show — and the caveats. 🧵
#GLP1 #Ozempic #Wegovy #BreastCancer #ASCO2026
35
86
505
106,940
Dr. Michael Moeller, ND retweeted

Jun 1
The Christian expression and heritage here is unmatched.
Unsurprisingly, they are lying to us about Russia. ✝️




4,301
5,154
46,283
3,402,508
Dr. Michael Moeller, ND retweeted

Jun 1
👀👀👀
May 31

Tomorrow's Huberman Lab episode is with Dr. @AbudBakri, MD, a physician and clinician specializing in peptide therapeutics and their applications in healing, immunity, and longevity.
Dr. Bakri and @hubermanlab discuss BPC 157, the difference between GLP-1s and the "Russian" peptide bioregulators, thymus health and immunity, and overlooked markers of longevity.


86
33
1,033
103,242
Dr. Michael Moeller, ND retweeted

May 26
Following a bit of the Protestant polemics against Orthodoxy recently, and I realize just how difficult it is to communicate the mind of the Church across these lines.
A simple example is seeing people confused about whether someone who is not baptised and participating in Orthodox communion can be "saved". Protestant are noticing that there are different answers in their estimation, and so are confused about them. The confusion comes from the belief that being "saved" or not is about "where you go after you die", when for the Orthodox "saved" means being made whole, being healed, being restored to the original purpose God had for us.
For this reason, when Protestants see declarations of how communion in the body of Christ is the only way to salvation, they immediately think this is a declaration that all the non-Orthodox are going to hell after they die. When Protestants then hear the very same person who just told them that salvation is in full participation to the body of Christ go on to intimate we have nothing to say about the eschatological finality of any specific soul, it is like a short circuit that many Protestants cannot compute. This is what I could see when @OrthodoxEthos and @Acts17David were discussing and it is what I have seen in @gavinortlund's videos.
In a similar vein, when a Protestant says he has the "assurance of his own personal salvation", this is confusing to the Orthodox. Orthodox also obviously have assurance of salvation, that assurance is Christ. He shows us what it means to be made whole and makes us participate in that wholeness. But how can I say that I am "saved" if I see that I am still a wretch, still prideful and arrogant and sinful? So the Orthodox, knowing they are are still sinning, though also knowing Christ has made them grow in the virtues will say something like: "I know that I am being saved." That is I can see that I am being healed, being made whole, being reformed to the resemblence of God. But again, this completely confuses the Protestant who just wants to know what will happen when you die. What side of the fence will you end up on?
I am not sure how to get accross these lines, and I feel that unless we can, we will perpetually be talking past each other.
194
332
1,970
113,026
May 26
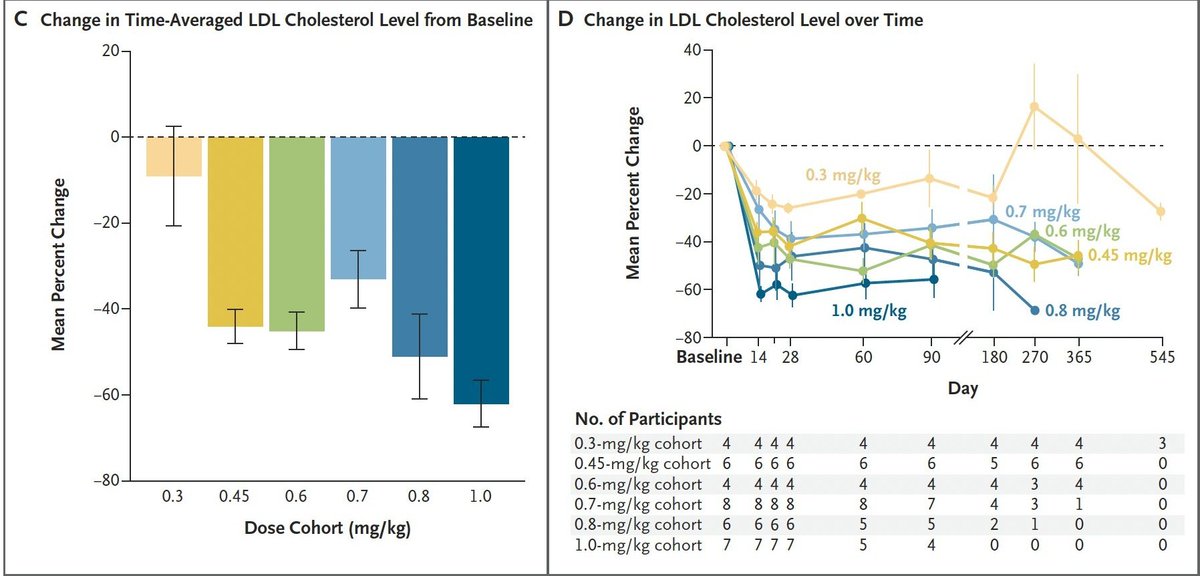
WUT!? I've seen several doctors say this!?!? Lowering LDL does NOT mean you solved heart disease!
Sure, one shot of "PCSK9 base editing" may reduce one major driver of atherosclerosis by lowering ApoB/LDL particle burden long term and that’s really cool and all, but heart disease isn’t just ‘LDL go up = heart attack.’
Existing plaque, calcification, Lp(a), endothelial dysfunction, hypertension, insulin resistance, inflammation, clotting risk, smoking history, metabolic disease, and lifestyle factors don’t magically disappear because you edited one gene.
So Reducing LDL DOES NOT curing cardiovascular disease. Cool technology? Absolutely. Potentially game changing for certain high-risk patients? Maybe.
Heck there maybe a chance it gives turbo cancer. We don't know yet.
So this whole "One shot and you’re protected from heart disease’ is just click bait.
May 26

One shot and you’re protected from heart disease. Imagine that for cancer, dementia and aging
1
87
May 25
Why eat healthy?
Why exercise?
Why even inject Repatha?
Just EDIT YOUR GENES bro 🥴😂😂🥴
Yeah I know, diet and exercise don’t always fix cholesterol because of genetics…
Permanently rewriting your DNA is definitely the move.
What could possibly go wrong?
May 25

Eli Lilly has done it.
They've gone and made what seems to be a powerful, permanent gene therapy for LDL cholesterol.
That means they'll be able to effectively prevent most heart disease with a single infusion!
1
1
5
455


May 24
The health ignorance stuff has gone massively overboard. People walking around destroying their vital signs every second of the day like they're living in toxic soup straight out of a sci-fi movie. Eating ultra-processed food like it won't kill them if they look at it. Neglecting their sleep. Never counting their steps. It's possible to live a healthy life, but you have to be intentional and work hard at it the modern world is doing everything it can to make you sick. You're gonna die either way. In a few decades you can be strong, sharp, and showing up for the people you love, or you can be on four medications, metabolically wrecked, and wondering what happened. Take this seriously and live your healthiest life while you still can.
May 24

The health consciousness stuff has gone massively overboard. People walking around with bands tracking their vital signs every second of the day like they’re astronauts on the ISS. Treating alcohol or sugar like it’ll kill them if they look at it. Tracking their sleep. Counting their steps. It’s possible to live a healthy life without being an obsessive, paranoid lunatic. You’re gonna die either way. In a few decades you’ll be just as dead as the rest of us, if not sooner. Relax a little and live your life while you still can.
5
11
4,267
May 24
7 years ago, a good friend of mine, 32 years old, working full-time while raising 2 special needs children, came to me with every symptom of low testosterone.
He told me: “Moe, I can either:
1) Work out in the morning
2) Show up great at work
3) Play with my special needs kids
4) Have energy for intimacy with my wife
Most days I can do two. Some days three. But I can never do all four.”
I told him to get tested.
His testosterone came back at 232 ng/dL.
Insurance required a second test.
It came back at 254 ng/dL.
He was told he was still in the “normal range” and denied treatment.
So he went to a cash-pay clinic. They optimized his testosterone to ~800 ng/dL.7 years later:
He’s in the best shape of his life
Thriving at work
Fully present for his children
His marriage is stronger than ever
He does all four now. Every day.
A number on a lab sheet almost robbed a family of their husband and father. Medicine should treat patients not just reference ranges.
May 24

A man with a testosterone level of 298 can qualify for TRT.
A man with a testosterone level of 312 often can't.
Same symptoms. Same risks. Completely different outcomes.
The problem isn't testosterone.
The problem is how we're diagnosing it.
In this video, I break down why current low testosterone guidelines may be failing millions of men, the ongoing decline in testosterone levels across the population, and why the future of hormone optimization could look very different than it does today.
Plus, I'm taking you inside the Enhanced Games to explore one of the most controversial questions in modern medicine:
What happens when we stop limiting human performance?
Watch the full video below 👇
#TRT #Testosterone #MensHealth #HormoneOptimization #LowTestosterone #Biohacking #EnhancedGames
2
234
May 23
It absolutely blows my mind that as a naturopathic doctor I’ve had to defend TWO things endlessly in my career:
1. Testosterone Replacement Therapy
2. Now = GLP-1 meds and other peptides
Meanwhile America keeps getting sicker. Patients stacking meds likes it out of Pez dispenser.
I’d rather see the right patient on low-dose tirzepatide or retatrutide long-term than on:
-blood pressure meds
-diabetes drugs
-pain meds
and the list goes on.
Same with TRT. The evidence is clear for properly selected patients, yet people still act shocked a naturopathic doctor would use hormones.
Do I still think diet, lifestyle, sleep, exercise, stress reduction, and root-cause medicine matter? Absolutely.
But pretending severely metabolically unhealthy patients are all going to meditate, meal prep deadlift, and colon cleanse their way out of disease is not reality.
The GLP-1 data is still evolving and I’ll change my position if the evidence changes. But right now, the benefits for many patients appear to outweigh the risks by a long shot.
Medicine should be about outcomes, nuance, and risk vs risk.
3
3
20
756
May 22
GLP-1s are dangerous!!!
You know what’s also dangerous?
Being 40 pounds overweight for 30 years.
Chronic inflammation.
Insulin resistance.
Sleep apnea.
Heart disease.
Cancer risk.
Medicine is risk vs. risk.
Not risk vs. perfection.
May 21

The world’s most popular weight-loss and diabetes drugs are linked to a powerful new possible benefit: better outcomes for cancer patients. on.wsj.com/3RBfcXO
9
7
124
10,902
May 21
Reta is crazy... may be the biggest breakthrough in obesity medicine we’ve ever seen.
Phase 3:
• 2,339 patients
• 80 weeks
• 70 lb average weight loss
• 28.3% body weight reduction
Nearly HALF of patients lost over 30% of their body weight.
A few thoughts:
-This is approaching bariatric surgery territory from a WEEKLY injection.
-The most underrated finding may actually be the LOWEST dose.
-The 4mg arm still lost ~19% body weight with fewer side effects and discontinuations.
-Most patients don’t need “maximum possible weight loss.”
They need something sustainable.
-Retatrutide isn’t just stronger Ozempic.
The glucagon agonism changes energy expenditure and fat oxidation in a very different way.
The implications for:
• obesity
• fatty liver disease
• inflammation
• cardiometabolic disease
• food addiction
• longevity medicine
…are massive.
Most people still do not understand how much medicine is about to change over the next decade.
I still really like Tirzepatide too, maybe more.
May 21

🚨 BREAKING: ELI LILLY'S RETATRUTIDE SHOWS ~30% WEIGHT LOSS IN PHASE 3 TRIAL
- Retatrutide is a GLP-3 (triple agonist)
- Helped people lose up to 85 pounds, putting it on par with bariatric surgery 🤯
- Lilly expects to file for approval later this year
$LLY $NVO $HIMS
4
4
40
12,272
May 17
One of the biggest concerns with GLP-1 medications is muscle loss, and it's a valid one.
Muscle mass is one of the strongest predictors of long-term health and longevity.
Most people optimizing through exercise and hormone balance are in a good place, but it's something to watch closely when using these compounds.
EDUCATIONAL & RESEARCH USE ONLY
This content is provided for scientific discussion and educational purposes only.
Some compounds discussed are not FDA-approved for human use and are not intended to diagnose, treat, cure, or prevent any disease.
Not Medical Advice: This does not constitute medical advice or establish a doctor–patient relationship.
Always consult a qualified healthcare professional for individualized guidance.
No Sourcing: This channel does not sell, supply, or provide links to purchase research chemicals/peptides, and nothing here is intended to encourage self-experimentation.
#MuscleMass #GLP1 #LongevityMedicine
1
1
92
May 16
Tirzepatide (Mounjaro/Zepbound) hits two receptors, GLP-1 and GIP, making it the most effective FDA-approved weight loss compound we have.
One randomized controlled trial showed 22% body weight reduction.
That's not anecdotal. That's the highest level of clinical evidence.
EDUCATIONAL & RESEARCH USE ONLY
This content is provided for scientific discussion and educational purposes only.
Some compounds discussed are not FDA-approved for human use and are not intended to diagnose, treat, cure, or prevent any disease.
Not Medical Advice: This does not constitute medical advice or establish a doctor–patient relationship.
Always consult a qualified healthcare professional for individualized guidance.
No Sourcing: This channel does not sell, supply, or provide links to purchase research chemicals/peptides, and nothing here is intended to encourage self-experimentation.
#Tirzepatide #Mounjaro #WeightLossMedication
5
783