
FYI those are the uncharted waters that many of us face due to iatrogenic disease , guidelines free zone, sadly very avoidable if you #IVUSfirst as preached by so many like @GreggWStone and @mmamas1973

@mmamas1973
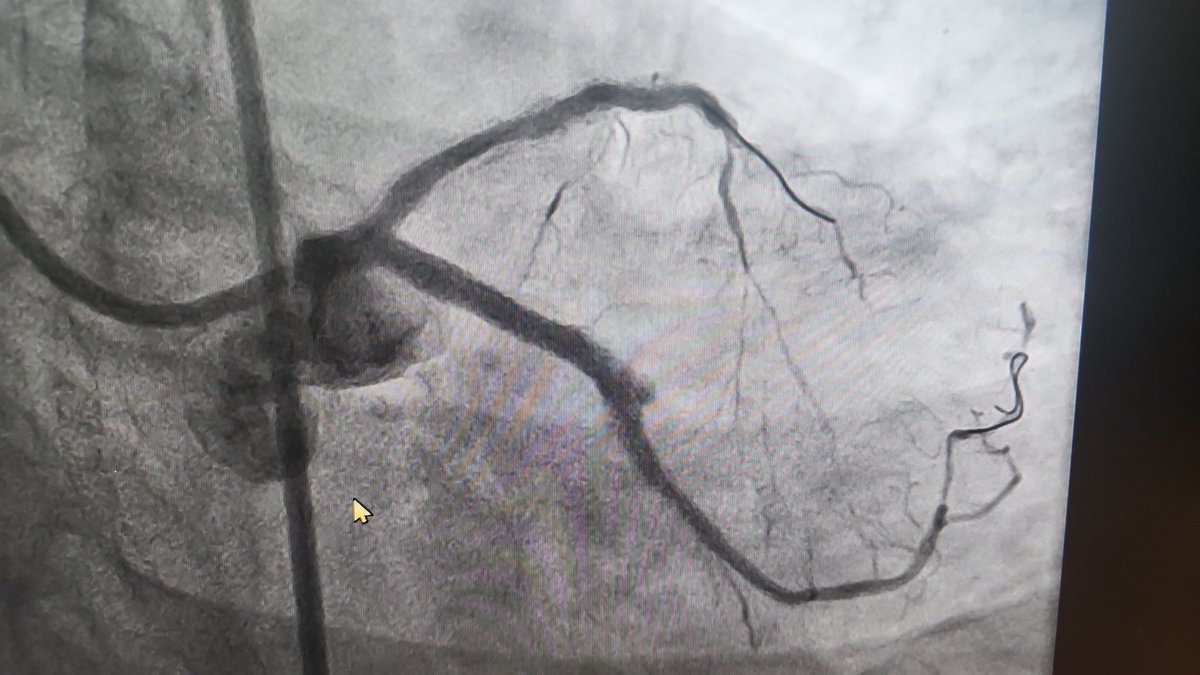
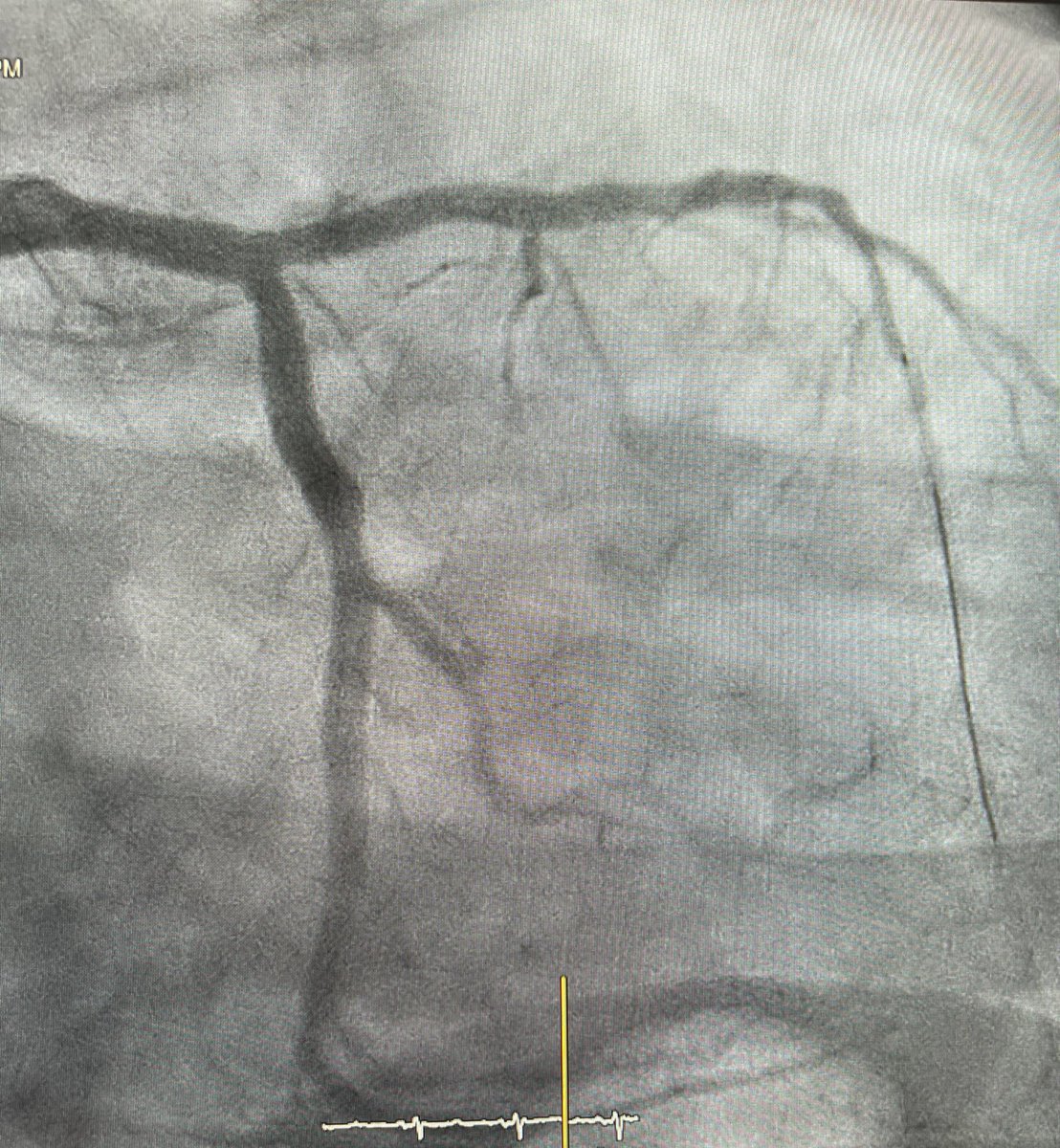
We have a floating 3.5 mm stent in a 5.5 mm proximal LAD, that has been there since 2021, in a patient with severe effort angina since then, MLA 8.7 mmsq, 3.1x3.4 MLD artery diameter 5.5mm
2
3
1,019

19 Apr 2025
1
7
3,362

13 Dec 2024
👴🏽 79y, COPD, CKD, AS, Ostial LAD disease #Radialfirst #IVUsfirst #Rotablator🎈🔪 #Wolverine Rota-Cut, Real-time intravascular ultrasound guidance, #IVUs 👀 Done 👌🏾🔥🔥🔥🙋🏾♂️🇲🇽 @jedicath @SarahFairley7 @AllanaSalman
@mirvatalasnag @mmamas1973 @AdrianMercadoMD @DrNataliaP
2
6
33
2,281
28 Mar 2024
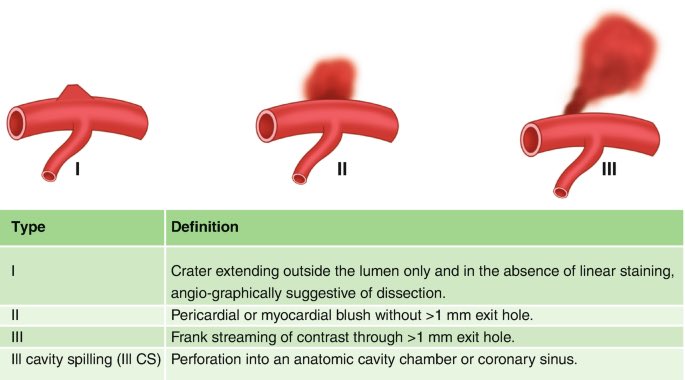
Coronary Perforation. Ellis Classification. Wich type is this? #IvusFirst #coronary #CardioTwitter @mirvatalasnag @agtruesdell @IvanRendonm @LAzzaliniMD @jorgeachv @DrNataliaP @KPujdak @RameshDaggubati @SCAI @CTOcomplication @UjjwalRastogiMD @TWilsonMD @MPAOSS @OjedaOjeda18
4
20
73
5,657

11 Feb 2023
4
509

#ZeroContrastPCI #CKD #ContrastShortage #IVUSfirst #Gadolinium
#NSF risk <0.07%
@mirvatalasnag @RhianEDavies1 @DrJayMohan @adityadoc1 @AnkurKalraMD @chadialraies @kerrigjl @DocSavageTJU @mmamas1973 @BagaiJayant @SripalBangalore @SrihariNaiduMD @aayshacader #Cardiotwitter

Introducing the JIC Podcast!
First up, @DLBHATTMD interviews @HadyLichaaMD about his article appearing in the June issue (using gadolinium-based contrast agents) #cardiotwitter #Cardiology bit.ly/3mqxBDR

4
8
36
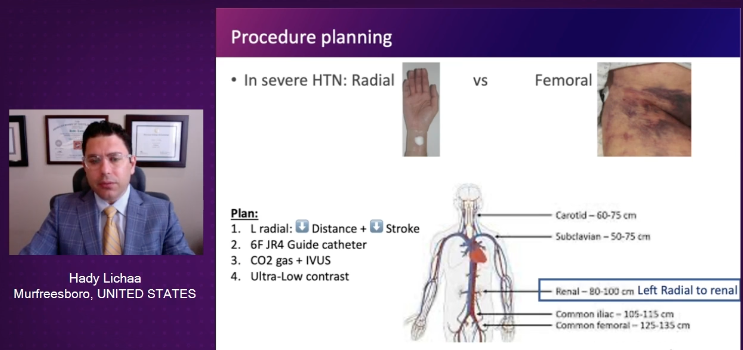
#R2R: #Radial2Renal presented @ #EuroPCR2022
Novel term & particularly favorable #RadialFirst access
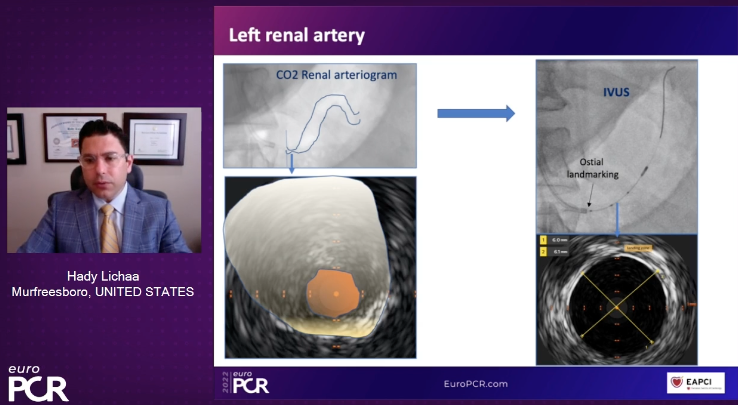
#IVUSfirst #CO2angio -> ⬇️dye
@EricSecemskyMD @mirvatalasnag @prkothapalli @jcgeorgemd @agtruesdell @kerrigjl @adityadoc1 @RajTayalMD @mcbunte @sealtin1 @AkramWIbrahim
4
19
59

If surgery declined and opted for high risk PCI then would go with #IVUSfirst.
Heavily calcified and ectatic ostial trifurcation > would go with MCS then try IVL to LAD followed by provisional stenting LM/LAD /- bailout TAP technique to LCX and leave RI for Med Rx
2
22 Mar 2022
#IVUSfirst is essential in #LM and #Calfication PCI for me!!!! #PleaseShowUs
Looks like an @ShockwaveIVL case to me but depends on LVEF, IVUS-calcium score (type of calcification) and patient characteristics! #PrecisionPCI
5
25 Feb 2022
Great and real conclusión at most time "When a stent faills, it is not the stent's fault" #IVUSFirst #OCTFirst @DrNataliaP @jorgeachv @foroepic @MauroEchavPinto @AlcantaraCardio @joaoeduardotp @rickytiago @LCathlab @LAzzaliniMD @hect2701 @drgianma
25 Feb 2022

#CTO2022 Jennifer A. Tremmel stent failures
Imaging is essential to know the mechanism to treat
Right tool for the right problem.

2
2
14
16 Nov 2021
No options of #ELCA (Laser) or #Shockwave @ShockwaveIVL in México yet, of course #Radialfirst #IvusFirst #Glidesheatslender #CardioTwitter #interventionalcardiology #Complex #ComplexPCI @LAzzaliniMD @rotamonster @jorgeachv @foroepic @LCathlab @mirvatalasnag @AJuradoRoman
1
1
6

11 Aug 2021
Thoughts on IC imaging first (#IVUSfirst) to look for high risk features as the better approach when dealing with NCLs? #CardsJC #cardiotwitter
1
2
6

23 Jul 2021
These are the post PCI MSA BEFORE post dilating both LAD/CX ostium with 4.5mm NC @20atm and final 5.0mm POT… excellent final results… its always better to be lucky 🍀 than good… #IVUSfirst de-escalated complexity for initial strategy… CTO morphology helped… 💔😷❤️🏝
3


3 Apr 2021
Diabetic patient with ACS. LAD treated with 3.0 mm stent and postdilated with. 3.0 NC balloon. Good result? Looks good?

10
10 Feb 2021
👴🏽79y, MVD, inferior STEMI, PCI to RCA and LAD, by other operator, 2T PCI LCx #Bifurcation #RadialFirst without palpable pulse no US, #rdTRa difficulty advancing the guidewire #IvusFirst big haematoma #6Fr #Nanocrushtechnique #XienceSierra Final Result. Mexico🇲🇽😎 @ferdikiem
1
5
19
9 Feb 2021
1
3
14 Jan 2021
Although total extraction of the stent is possible, it is a very long stent, with thrombosis ... non-selective cannulation dilate struts, posdilate, RCA #ivusfirst
1
5