Fred Saad, CQ, MD, FRCS, FCAHS, of @cancermtl discusses data from subgroup analyses of the PSMAddition trial by disease volume and in de novo/recurrent mHSPC.
Read more here: hubs.li/Q04lyTwT0
#oncology #medtwitter #pcsm #prostatecancer #ASCO26
167
Carlos Ruiz retweeted

21h
Fred Saad, MD, CQ, FRCS, FCAHS, discusses subgroup data from the phase 3 PSMAddition study of lutetium Lu 177 vipivotide tetraxetan plus ADT and an ARPI in PSMA-positive mHSPC.
Follow all of our coverage of #ASCO26 here: hubs.li/Q04lv0gr0
#oncology #pcsm #prostatecance
2
2
567

Radiation is no longer blunt.
Targeted Radioligand Therapy is moving earlier. FDA expanded Pluvicto before chemo in PSMA mCRPC; PSMAfore showed rPFS 9.3 vs 5.6 months [1]. NETTER-2 cut progression/death risk 72% in first-line GEP-NETs [2]. PSMAddition points to hormone-sensitive prostate cancer [3] 🎯
The race is isotopes, PET access, GMP sites and trained teams ⚛️
Build capacity before demand exposes the gaps.
🤔 What will slow RLT most: evidence, isotope supply, reimbursement, or workforce?
[1] [fda.gov/drugs/resources-info…](fda.gov/drugs/resources-info…)
[2] [novartis.com/us-en/node/4217…](novartis.com/us-en/node/4217…)
[3] [novartis.com/news/media-rele…](novartis.com/news/media-rele…)
#RadioligandTherapy #Oncology #NuclearMedicine
1
1
68
Simon C retweeted

6/6
Throw PSMAddition into the frontline mix and mHSPC becomes a multidimensional puzzle. How do we sequence a patient with ATM mutation, 90%PTEN loss, and intense PSMA expression?
Balancing these overlapping phenotypes w/o compromising mCRPC options is our next great challenge
1
1
3
286

At #ASCO26, a PSMAddition analysis showed 177Lu-PSMA-617 boosts rPFS across #mHSPC subgroups, with steady safety and insights on PSMA PET selection.
🎥 Fred Saad, MD (@CRCHUM) breaks down the findings here: hubs.ly/Q04jVlGc0

2
3
191

Jun 2
The #OncoAlertTopTweet 🚨Day FOUR #ASCO26
Post by @OncoAlert Faculty @DrChoueiri 🇺🇸
PSMAddition: consistent efficacy of 177Lu-PSMA-617 across all evaluated mHSPC populations, with no differences in safety profiles. #ProstateCancer
@DrChoueiri 🇺🇸 @hoperugo 🇺🇸 @matteolambe 🇮🇹 @TiansterZhang 🇺🇸 @CathyEngMD 🇺🇸 @stolaney1 🇺🇸 @montypal 🇺🇸 @tompowles1 🇬🇧 @brian_rini 🇺🇸 @cdanicas 🇪🇸 @NiuSanford 🇺🇸 @amerseburger 🇩🇪 @GlopesMd 🇺🇸 @Icro_Meattini 🇮🇹 @PGrivasMDPhD 🇺🇸 @DrYukselUrun 🇹🇷 @nataliagandur 🇦🇷 @ElisaAgostinett 🇧🇪 @HHorinouchi 🇯🇵 @realbowtiedoc 🇺🇸 @to_be_elizabeth 🇮🇹 @UOzkerim 🇹🇷 @Erman_Akkus 🇹🇷 @yekeduz_emre 🇹🇷 @p_ciracimd 🇮🇹 @DrVilmaPBarcia 🇪🇸 @DraMartinezLago 🇪🇸 @DrMirallas 🇺🇸 @GaiaGriguolo 🇮🇹 @MarioBalsaMD 🇪🇸 @scocmem 🇬🇧 @AmandaNizamMD 🇺🇸 & @weoncologists 🇺🇸
May 31

#FreddSaad presenting important subgroup analysis from the phase 3 PSMAddition: consistent efficacy of 177Lu-PSMA-617 across all evaluated mHSPC populations, with no differences in safety profiles.
#ASCO26 #ProstateCancer #GUOnc @ASCO @OncoAlert
10
18
1,436
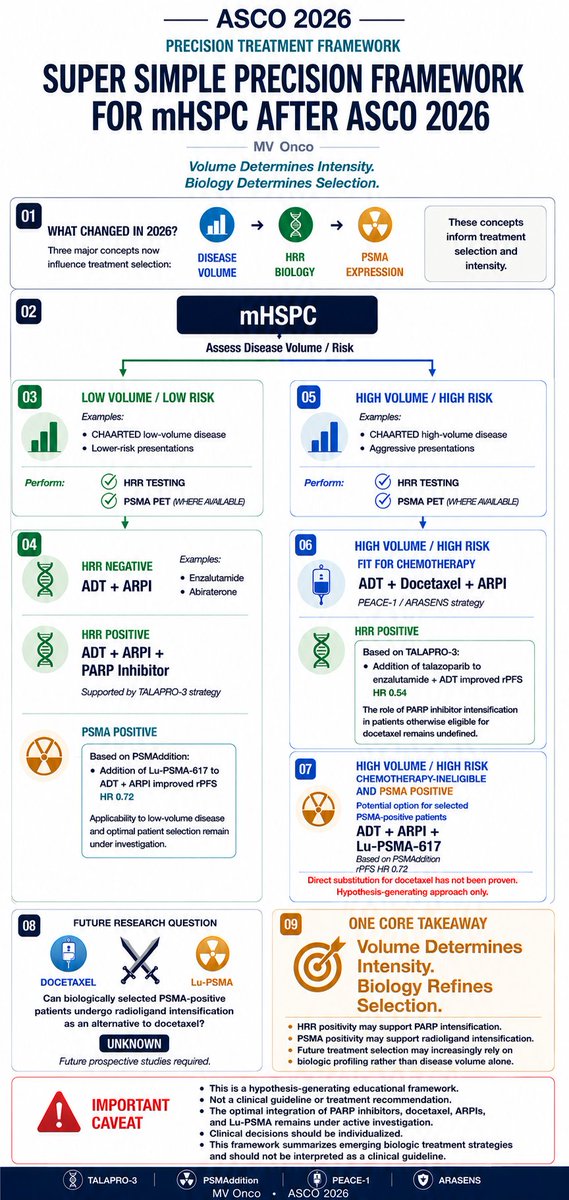
mHSPC after ASCO 2026:
Volume determines intensity. Biology refines selection.
From PEACE-1 and ARASENS to TALAPRO-3 and PSMAddition, treatment selection is becoming increasingly biology-driven.
A simple precision framework for everyday practice.
#ASCO2026 #ProstateCancer #mHSPC #MVOnco
10
14
902

Jun 1
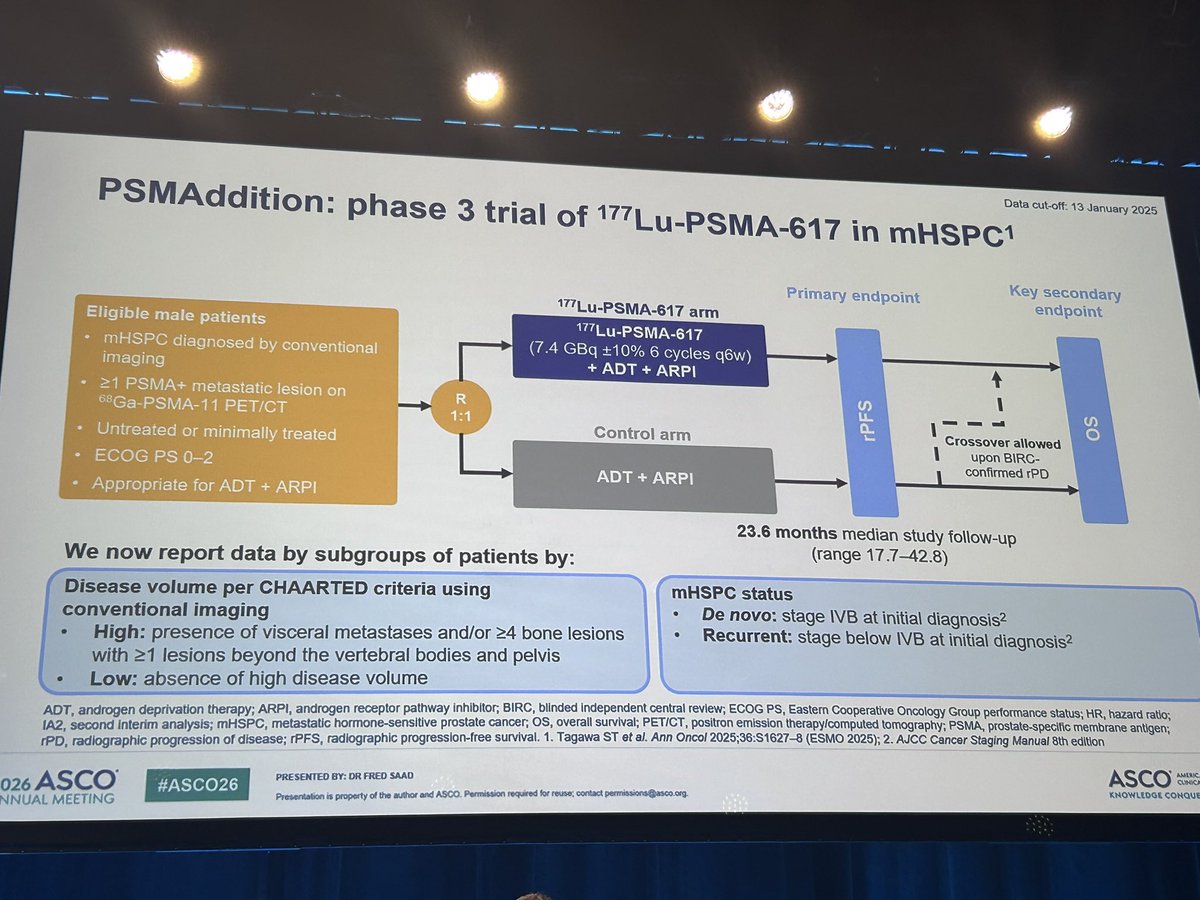
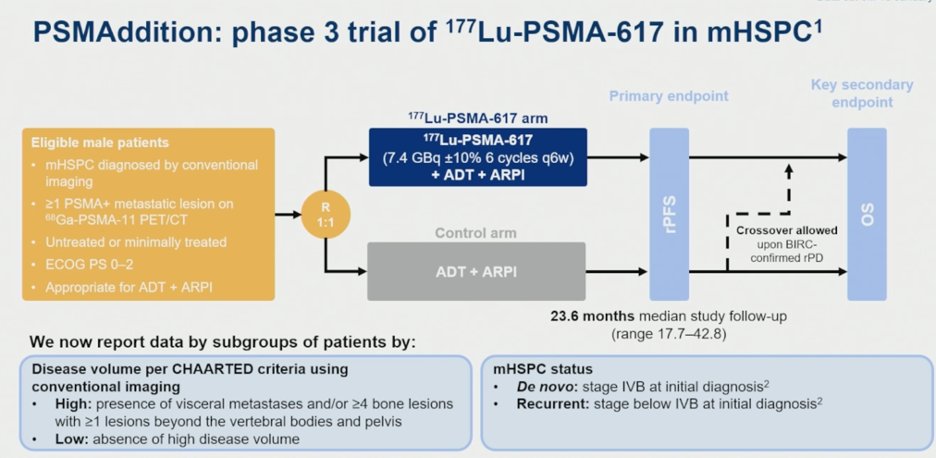
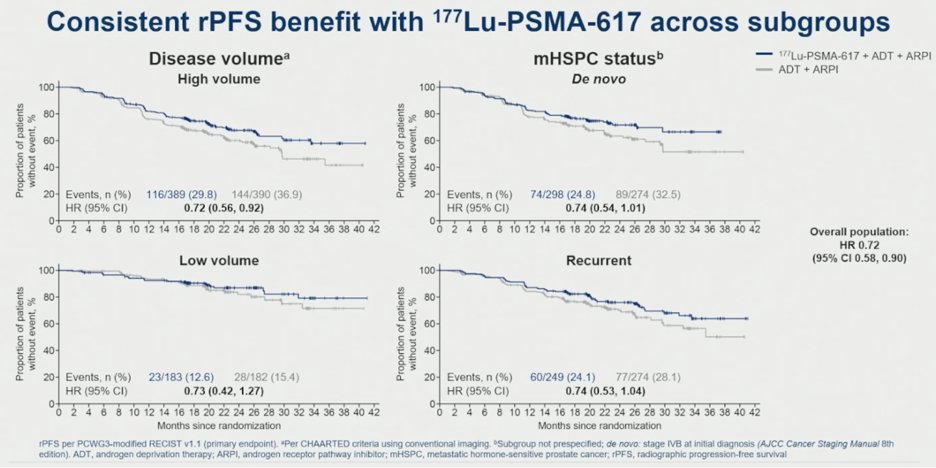
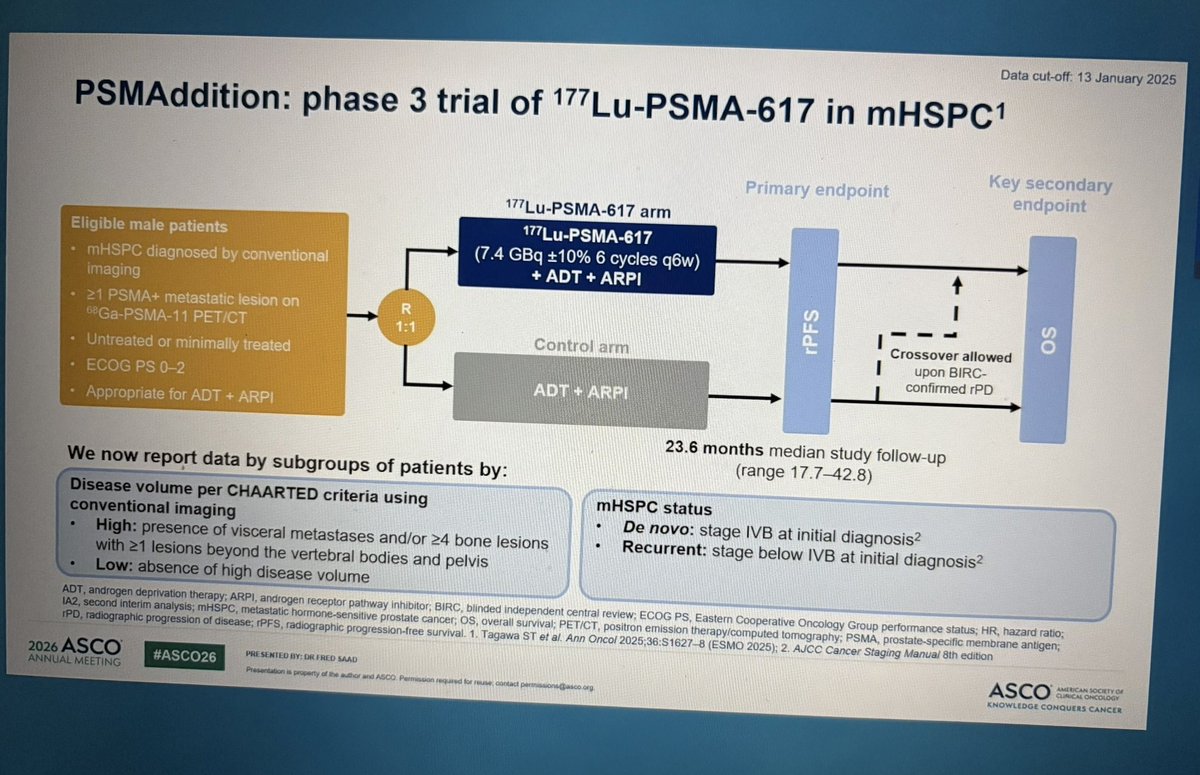
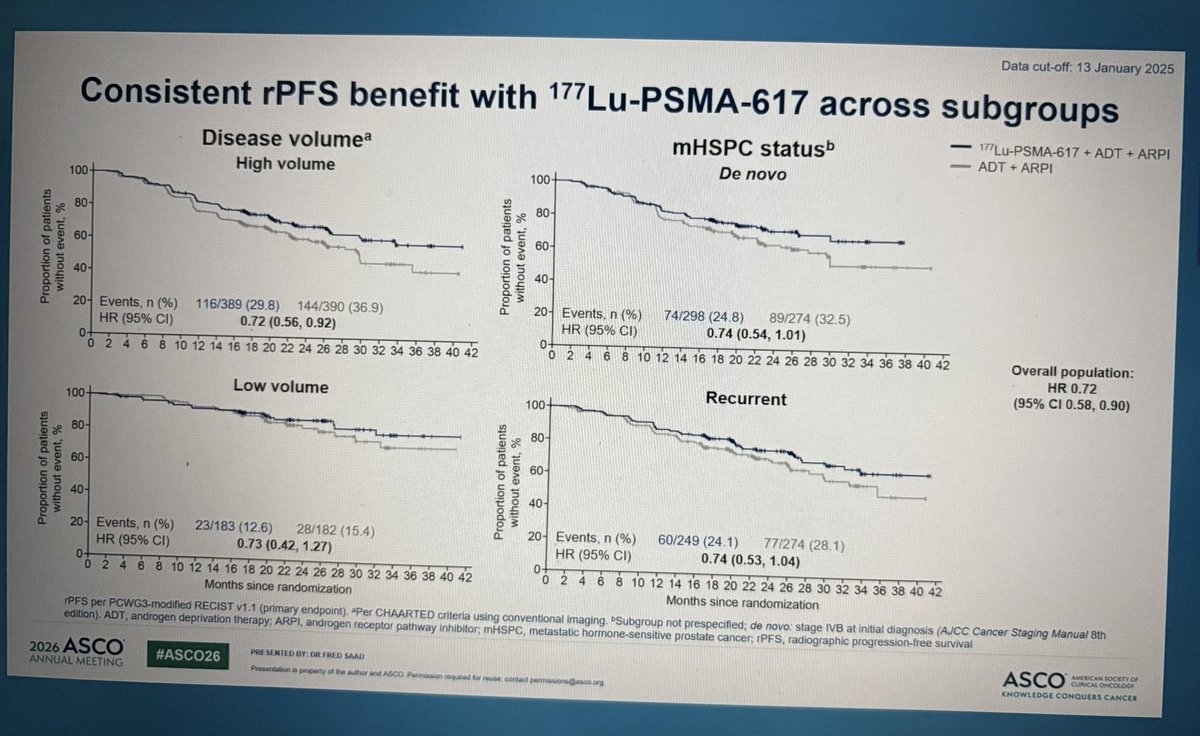
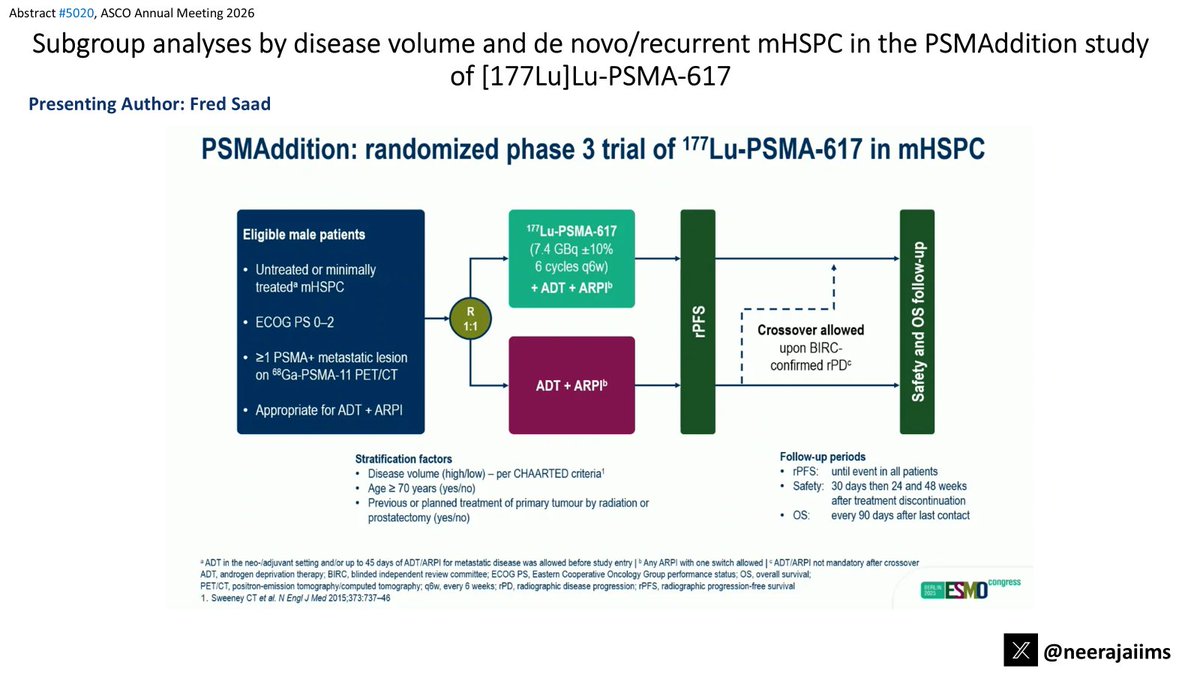
PSMAddition: Ph 3 RCT of ADT ARPI /- LuPSMA in PET mHSPC
📍Subgroup analyses by disease volume & timing
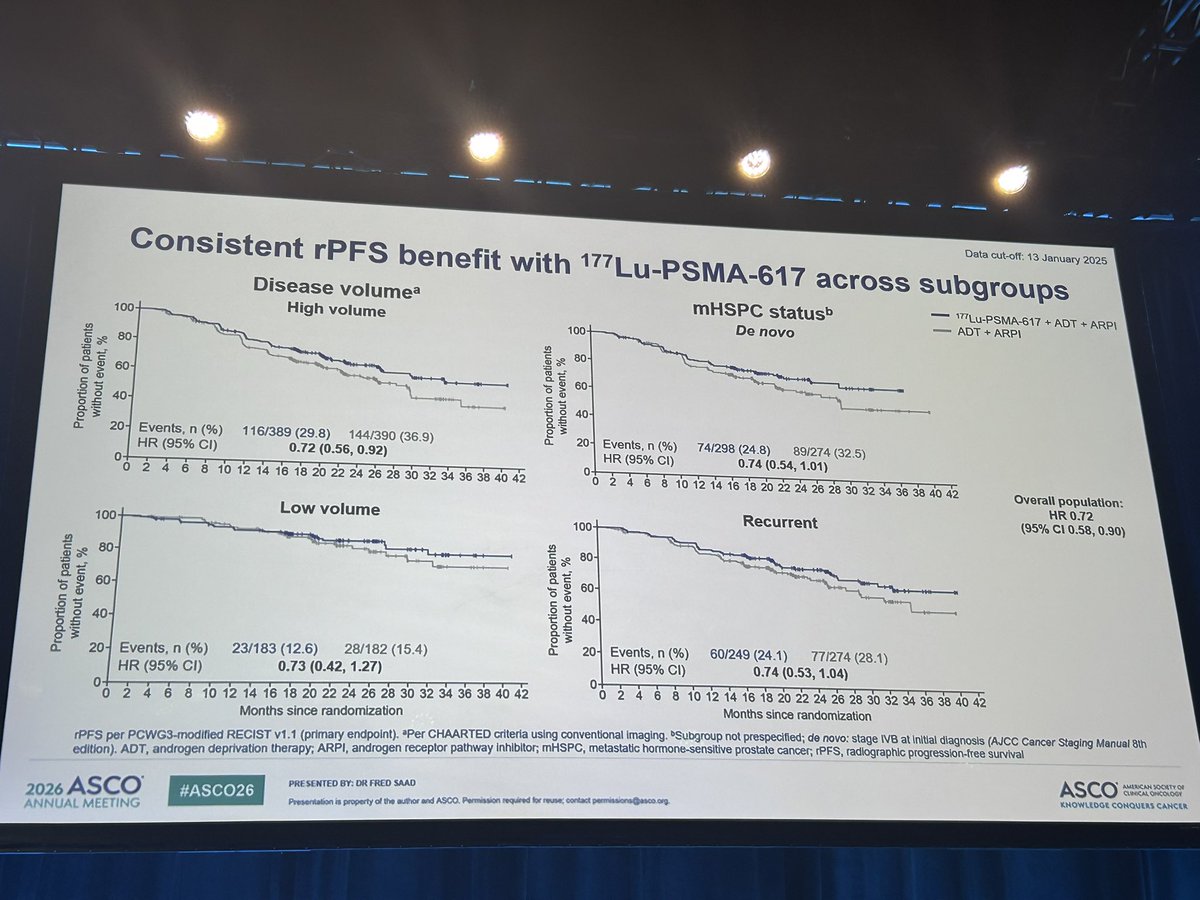
🔹Overall rPFS: HR 0.72 (95% CI 0.58-0.90; p=0.002)
🔹rPFS benefit consistent across subgroups:
•HV: HR=0.72; LV: HR=0.73
•De novo: HR=0.74; Recurrent: HR=0.74
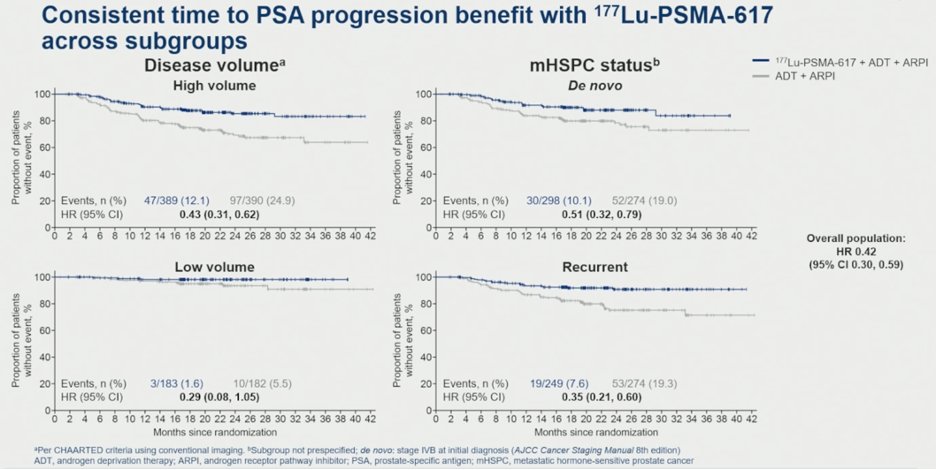
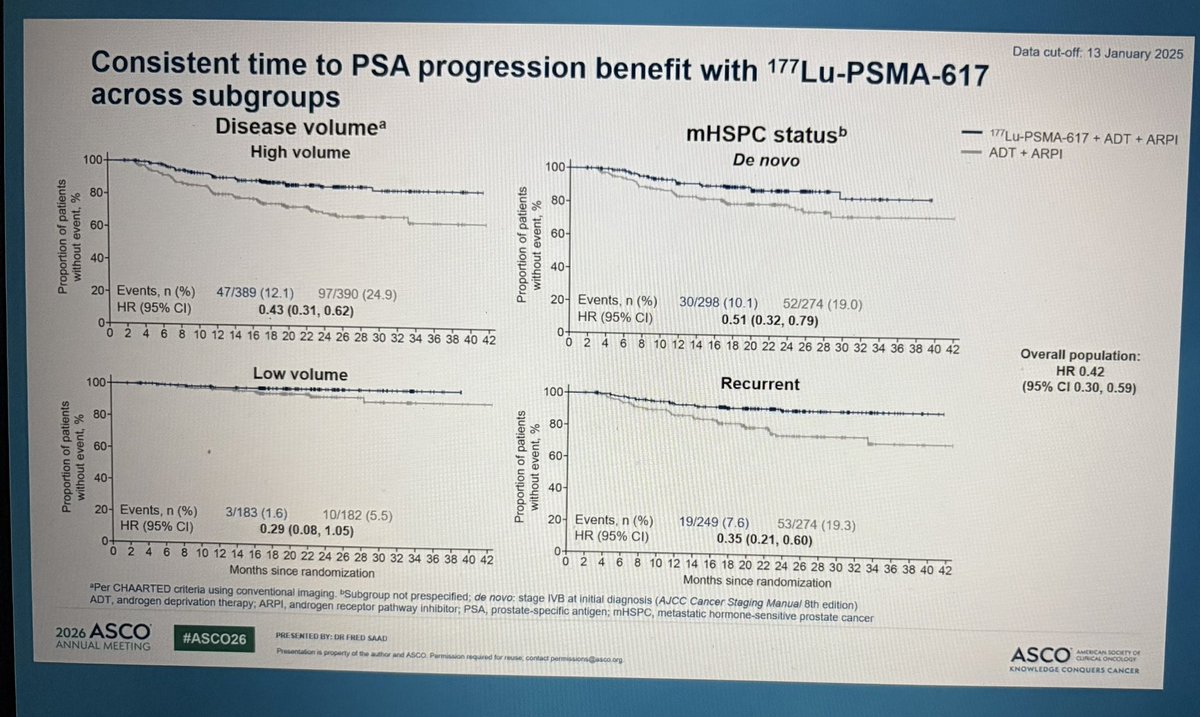
🔹Time to PSA progression improved across subgroups:
•HV: HR=0.43; LV: HR=0.29
•De novo: HR=0.51; Recurrent: HR=0.35
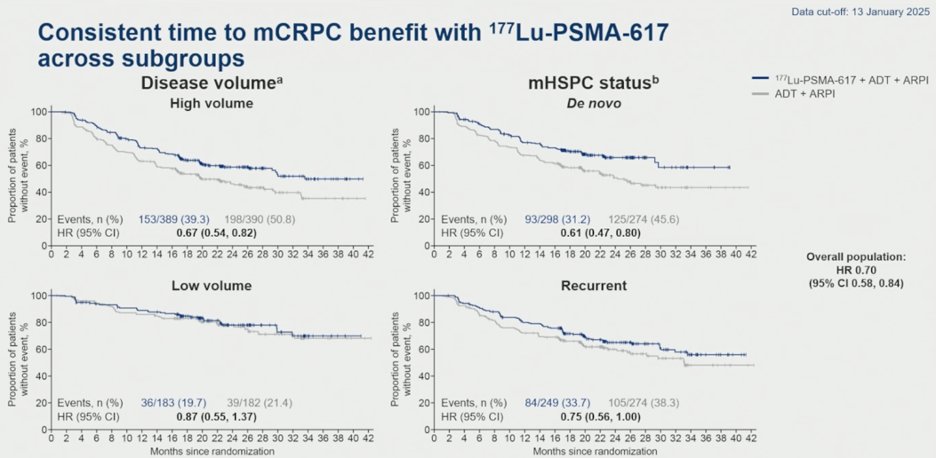
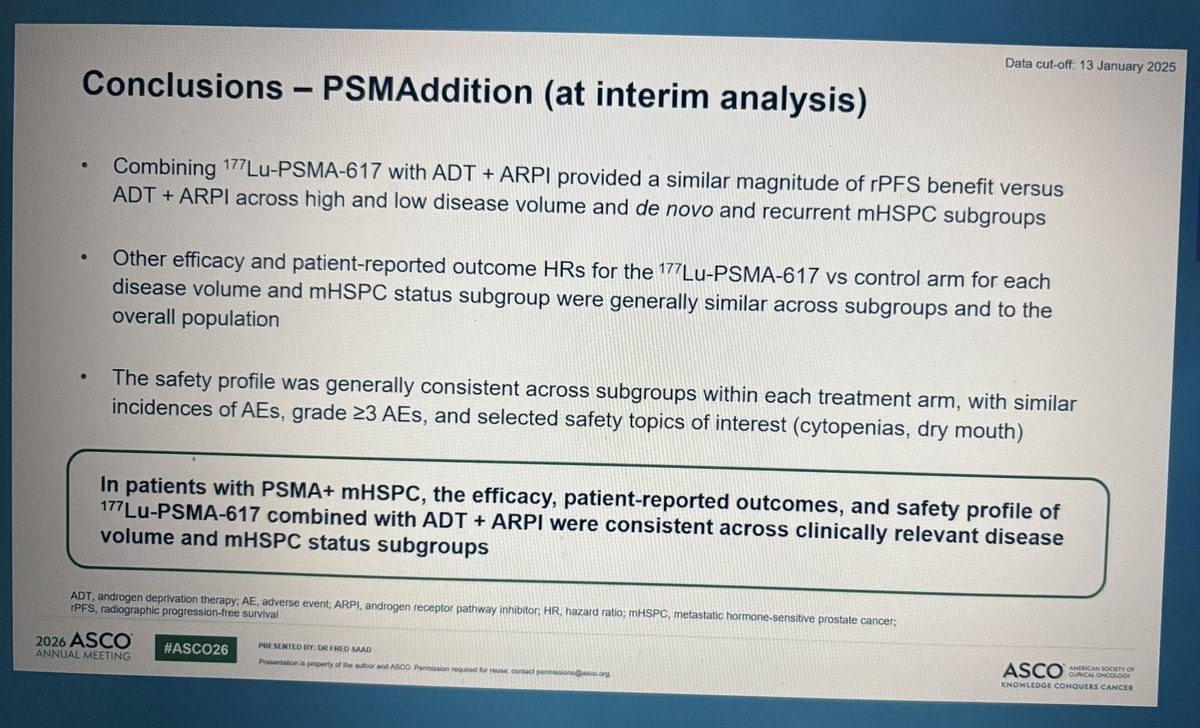
🔹Time to mCRPC similarly favored LuPSMA across all subgroups
✅ PROs and safety consistent across disease volume and disease status groups
📌The efficacy, PRO, and safety profile of LuPSMA ADT ARPI were consistent across clinically relevant mHSPC subgroups, supporting broad applicability of treatment benefit
@urotoday
#ASCO26
11
14
658


May 31
#FreddSaad presenting important subgroup analysis from the phase 3 PSMAddition: consistent efficacy of 177Lu-PSMA-617 across all evaluated mHSPC populations, with no differences in safety profiles.
#ASCO26 #ProstateCancer #GUOnc @ASCO @OncoAlert
18
21
3,345

May 29
Hi friends, it's #ProstateCancer Friday! #ASCO26 edition 🎉🎉🎉
Here are Top Posts of the Week 🧵
1/ @neerajaiims on Ab#5020 by #FredSaad on subgroup analyses in PSMAddition:

Ab#5020 @ASCO #ASCO26 by #FredSaad👉 bit.ly/3RrwTsQ👉subgroup analyses in PSMAddition #prostatecancer👉Lu-177 ADT ARPI⬆️rPFS vs ADT ARPI across high/low vol & de novo/recurrent PSMA mHSPC👇@OncoAlert @urotoday @PCF_science @DrScottTagawa @mishabeltran @OpenMedicineHQ

1
5
8
870

May 28
One core takeaway from PSMAddition:
Lu-PSMA-617 may be moving from salvage therapy into frontline triplet intensification for PSMA-positive mHSPC.
Theranostics is no longer being viewed only as late-line treatment biology — it may now be entering the hormone-sensitive disease setting.
#ASCO2026 #ProstateCancer #LuPSMA #mHSPC #Theranostics #MVOnco
3
4
483
May 28
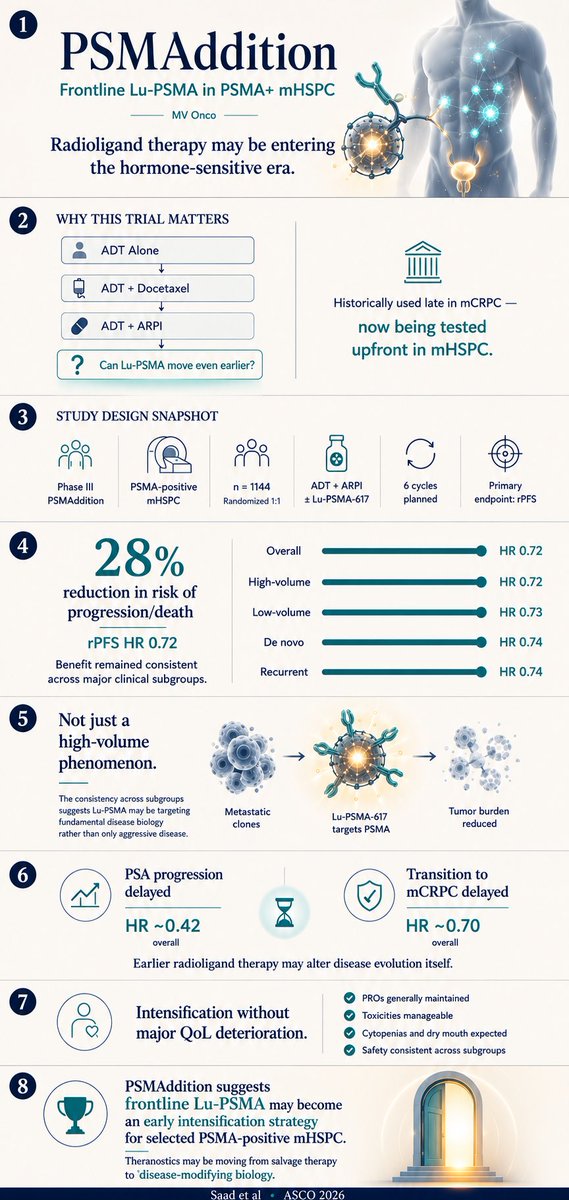
PSMAddition (Saad et al • ASCO 2026)
Lu-PSMA-617 may be moving earlier into the disease course of PSMA mHSPC.
The key signal is not just improved rPFS — but biologic consistency across disease states:
• high-volume and low-volume disease
• de novo and recurrent presentations
• delayed PSA progression
• delayed transition to mCRPC
• maintained QoL profile
Theranostics may be transitioning from salvage therapy toward frontline disease-modifying biology.
Triplet intensification may now be entering the theranostics era.
#ASCO2026 #ProstateCancer #LuPSMA #mHSPC #Theranostics #Oncology #MVOnco
1
6
490

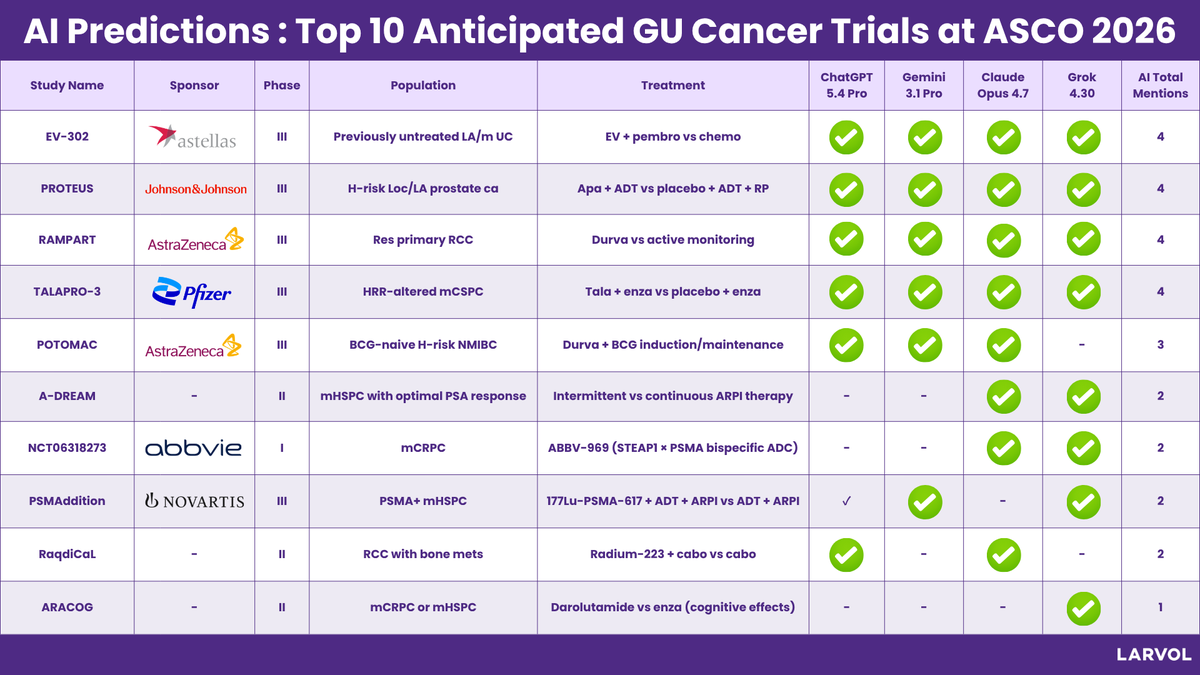
From bladder cancer to prostate and kidney cancer, several GU oncology studies are already generating strong attention ahead of @ASCO 2026.
To identify the trials most likely to shape discussions at the meeting, we asked leading AI models to rank the most anticipated GU cancer readouts.
There was particularly strong consensus around EV-302, PROTEUS, RAMPART, and TALAPRO-3 highlighting continued momentum for ADCs, radioligand therapy, immunotherapy combinations, and intensified hormonal strategies across GU cancers.
The list underscores key themes shaping the field:
▶️ Expansion of ADC and immunotherapy combinations in urothelial cancer
▶️ Continued evolution of AR-targeted and PARP-based approaches in prostate cancer
▶️ Growing momentum for radioligand and PSMA-targeted therapies
▶️ Increased focus on treatment optimization and de-escalation strategies
▶️ Novel approaches in RCC, NMIBC, and metastatic hormone-sensitive disease
Notable studies include:
• EV-302 evaluating enfortumab vedotin pembrolizumab in metastatic urothelial cancer
• PROTEUS assessing apalutamide intensification in high-risk localized prostate cancer
• TALAPRO-3 advancing talazoparib-based combinations in HRR-altered mCSPC
• PSMAddition exploring 177Lu-PSMA-617 in PSMA-positive mHSPC
• RAMPART evaluating adjuvant durvalumab strategies in renal cell carcinoma
Together, these studies reflect how GU oncology continues to move toward more biomarker-driven, targeted, and combination-focused treatment strategies heading into ASCO 2026.
Which GU cancer trial are you watching most closely?
Explore more insights and conference data from #ASCO26 👉 clin.larvol.com/conference/a…
#LARVOL #ASCO2026 #CancerResearch #CancerData #Oncology #OncologyInsights #ClinicalTrials #ClinicalOncology #GUOncology #GUCancer #GUCSM #GenitourinaryCancer | @DrChoueiri | @neerajaiims | @AndreaNecchi | @UroDocAsh | @nataliagandur
7
16
1,206

May 25
10 Must-Read Posts in GU Oncology | Third Week of May
This week’s GU oncology highlights cover:
• Prostate radiotherapy automation
• IMmotion150 in metastatic ccRCC
• Salvage RT after prostatectomy
• PSMAddition and Pluvicto
• Olaparib in BRCA-mutated mCRPC
• CheckMate 274 5-year update
• ASCO26 oncology preview, including POTOMAC
• ctDNA utDNA in bladder-sparing MIBC
• HPV evaluation in penile cancer
• EV-303 / KEYNOTE-905 in cisplatin-ineligible MIBC
@drenriquegrande @josedsh @amerseburger @LuigiFormisano_ @nancyghattas
📎oncodaily.com/genitourinary-…
#GUOncology #OncoDaily

1
7
13
419

May 24
ENZAMET Decipher analysis (#ASCO26, Abstr 5001). A practical question we deal with constantly: who actually needs docetaxel added to ADT enza in mHSPC? They ran the Decipher genomic classifier (>0.85 cutoff) on 634 pts from ENZAMET.
High-Decipher pts (>0.85) did clearly worse on ADT ENZ alone, but adding docetaxel basically erased that disadvantage (aHR 2.31 > 1.08, p-interaction 0.043). No sign of benefit from docetaxel when Decipher was low. Effect was strongest in high-volume disease.
My take: very interesting data on a highly relevant day-to-day topic. Docetaxel seems to negate the worse prognosis of Decipher >0.85 vs enza ADT alone. Makes biological sense to me, since high Decipher usually means higher Gleason, lower PSA relative to tumor burden, and less addiction to the AR pathway... so you're hitting the cancer from a different angle, which matters most in the aggressive ones.
What I keep coming back to is how this sits next to our other options. For BRCA/HRR pts we now have niraparib ARPI (AMPLITUDE), and for PSMA disease Lu-PSMA (PSMAddition). Both improved rPFS on top of ADT ARPI in their selected groups, and the PSMA benefit held up across volume. Docetaxel never showed the same, though to be fair the comparison was never made — there's no docetaxel ARPI ADT vs ARPI ADT trial — and historically its benefit has been mostly in high-volume. So when a pt qualifies for more than one, how do we prioritize??
Looking forward to seeing the presentation!
🔗 asco.org/abstracts-presentat…
#pcsm #ASCO26
@ChrisSweens1 @OncoAlert
1
8
19
3,466

Ab#5020 @ASCO #ASCO26 by #FredSaad👉 bit.ly/3RrwTsQ👉subgroup analyses in PSMAddition #prostatecancer👉Lu-177 ADT ARPI⬆️rPFS vs ADT ARPI across high/low vol & de novo/recurrent PSMA mHSPC👇@OncoAlert @urotoday @PCF_science @DrScottTagawa @mishabeltran @OpenMedicineHQ
1
15
31
4,097