
Joined October 2016
- Tweets 3,311
- Following 680
- Followers 638
- Likes 20,087
220 Photos and videos







𝐑𝐚𝐥𝐩𝐡 𝐌𝐨𝐡𝐭𝐲 𝐌𝐃 𝐌𝐏𝐇 retweeted

Imagine if every passenger on an airplane had a direct line to the pilot.
That’s what medicine has become.
We have embraced frictionless communication and that not a good thing.
With things like Epic Chat, every member of the healthcare team has immediate access to the physician.
Now there’s a constant stream of minor questions. It’s discouraged people from thinking critically. “Just ask the doctor,” has replaced any sort of clinical reasoning.
When I was a resident, we had an answering service. Anyone who wanted to reach the doctor needed to go through a third party. This provided triage and accountability. If we were getting called in the middle of the night for stool softener orders, there was a record of that.
A little friction in communication is a good thing.
76
61
622
57,959
𝐑𝐚𝐥𝐩𝐡 𝐌𝐨𝐡𝐭𝐲 𝐌𝐃 𝐌𝐏𝐇 retweeted

Now open access in @NDTsocial
Bleeding risk after kidney biopsy with platelet inhibition
🧐Platelet inhibition is not associated with increased risk of serious complications after kidney biopsy.
▶️academic.oup.com/ndt/article…

1
15
45
1,948
𝐑𝐚𝐥𝐩𝐡 𝐌𝐨𝐡𝐭𝐲 𝐌𝐃 𝐌𝐏𝐇 retweeted

Jun 13
No. Check for tolerance first. Responsiveness does not equal need, nor benefit. Maximizing output was shown decades ago to not be a viable strategy. Optimize tissue perfusion. Learners, please reconsider a forward-flow-centric approach. Focus on tissue perfusion, and the two do NOT have a linear relationship. Understand hemodynamic interfaces. Ping @icmteaching @khaycock2 @EMNerd_ @edu_kattan @ross_prager

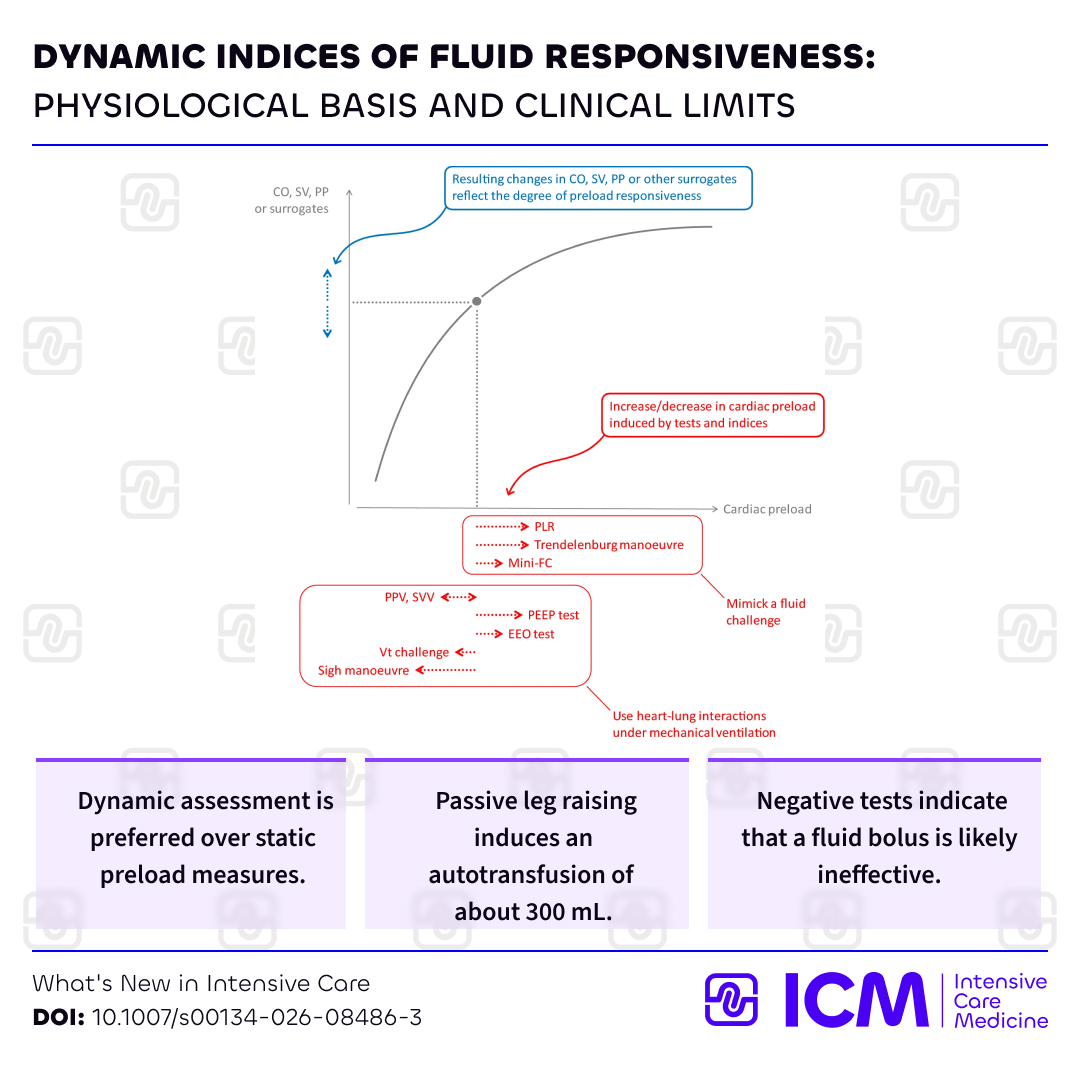
Dynamic indices of fluid responsiveness in @ICM
w/ @Prof_XMonnet @MichelleChew
💧Physiology of fluid responsiveness
📈Tests to predict fluid responsiveness
⚠️Clinical limits of these tests
Check for potential benefits before giving #fluids!
🔗rdcu.be/fnlTm #FOAM
4
23
81
7,315
𝐑𝐚𝐥𝐩𝐡 𝐌𝐨𝐡𝐭𝐲 𝐌𝐃 𝐌𝐏𝐇 retweeted

Jun 13
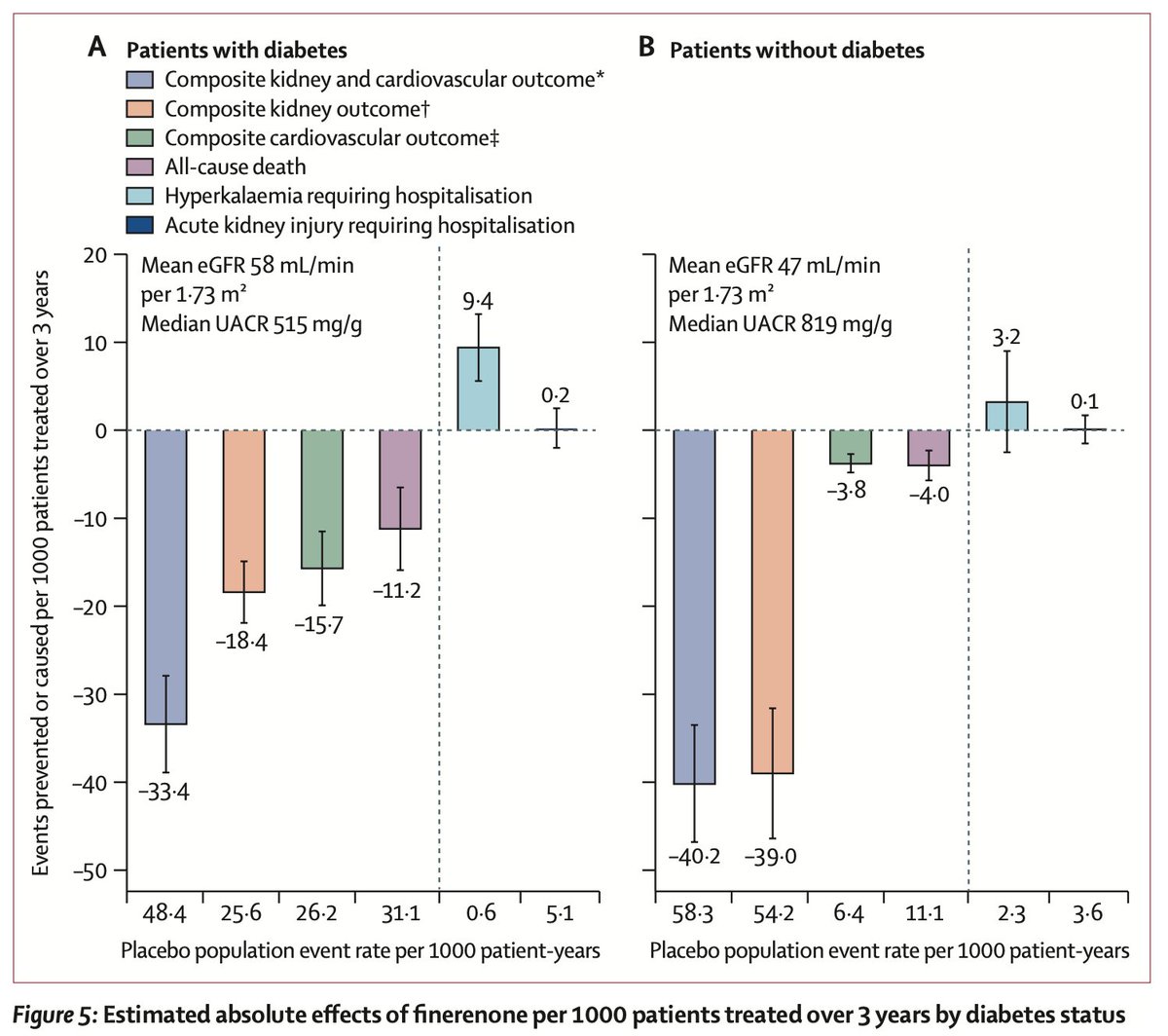
Finerenone in CKD - an IPD-meta-analysis of FIND-CKD, FIDELIO-DKD and FIGARO-DKD (INFINITY)
Free open access link to the INFINITY analysis in the Lancet (link expires July 25) authors.elsevier.com/a/1nDWe…
1
19
48
1,483
𝐑𝐚𝐥𝐩𝐡 𝐌𝐨𝐡𝐭𝐲 𝐌𝐃 𝐌𝐏𝐇 retweeted

Congratulations to this years class of @StanfordNeph fellowship graduates!

5
20
2,233
𝐑𝐚𝐥𝐩𝐡 𝐌𝐨𝐡𝐭𝐲 𝐌𝐃 𝐌𝐏𝐇 retweeted

Jun 11
“Well sir, you are very sick. Let’s engage in a shared decision making process to determine how to proceed”
Plan A: save your life
Plan B: the same as plan A except that I might randomly dump a bag of saline into your lungs for no reason because mommy (surviving sepsis campaign) says that’s what good boys are supposed to do
“I know this is a very difficult decision sir. Unfortunately the Best Available Evidence™️ simply doesn’t say which is better”
Jun 11

Fluid enjoyers won’t tell you this but this was a positive trial
A therapy with identical efficacy and fewer adverse events is, in fact, superior

1
1
3
406

Our reaction to any new study is either “I don’t believe it” or “I knew it”...
A NEJM trial in ICU pts w acute resp failure found that mucolytics (carbocisteine & hypertonic saline) don’t help. My ICU rounds line “mucolytics are useless” may need an update: “and possibly harmful”

9
55
255
21,426
𝐑𝐚𝐥𝐩𝐡 𝐌𝐨𝐡𝐭𝐲 𝐌𝐃 𝐌𝐏𝐇 retweeted
Jun 11
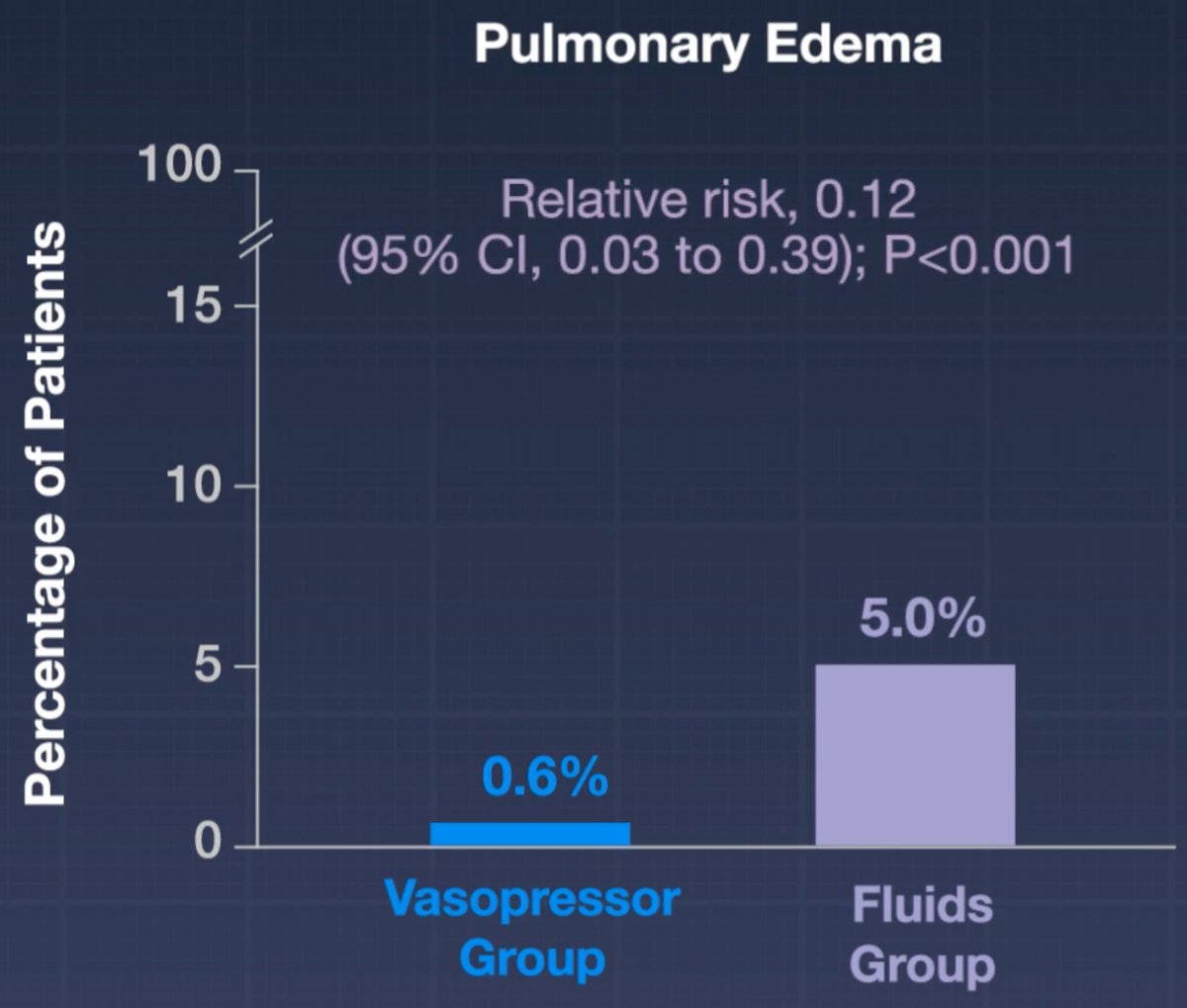
Fluid enjoyers won’t tell you this but this was a positive trial
A therapy with identical efficacy and fewer adverse events is, in fact, superior

Presented at #CCR26:
Among adults with septic shock, the use of restricted fluids and early vasopressors did not result in more days alive and out of the hospital through day 90 than the use of liberal fluids and later vasopressors. Full ARISE FLUIDS trial results: nej.md/3PVdwIp
@CritCareReviews
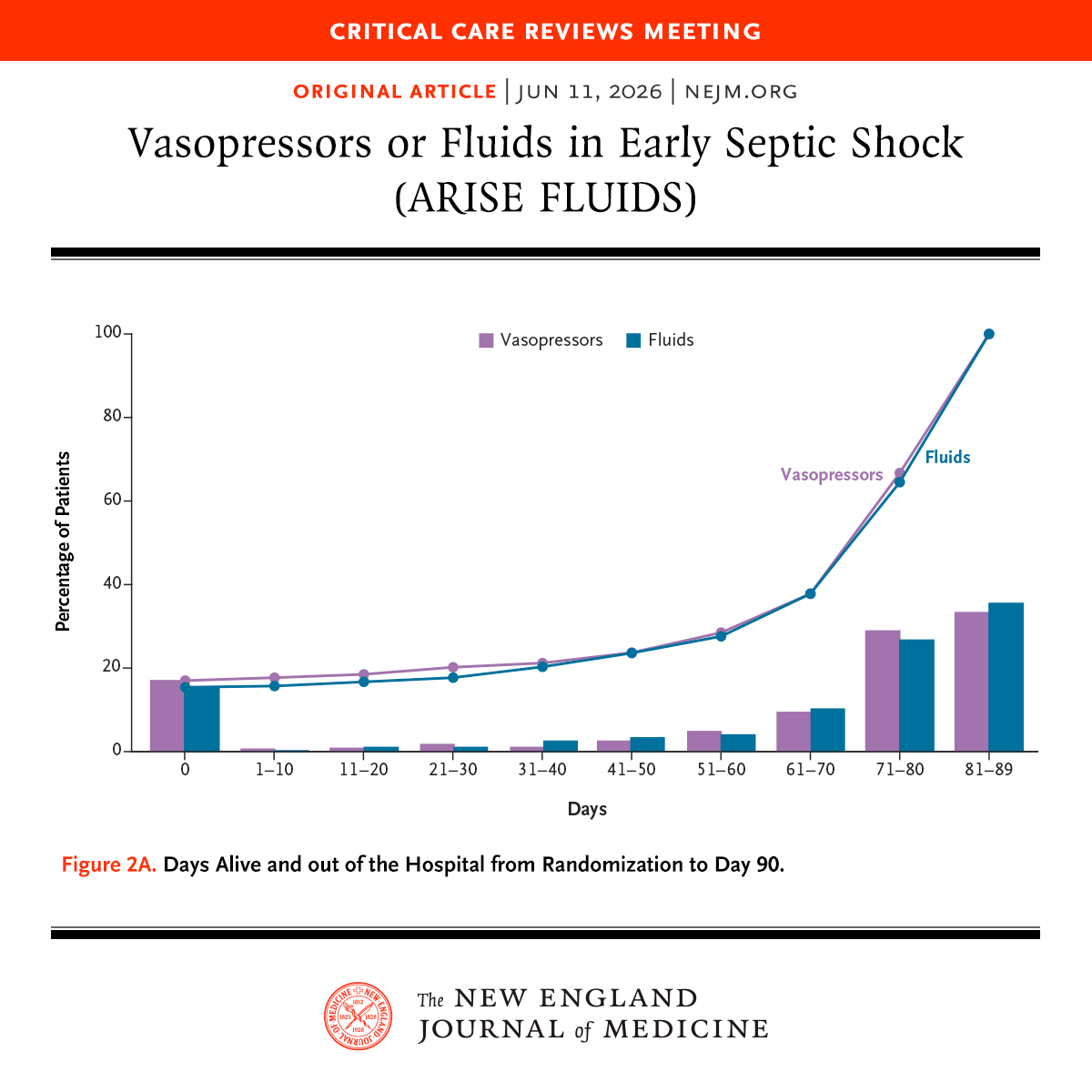
ALT A graph from an article titled "Vasopressors or Fluids in Early Septic Shock," which was presented at the Critical Care Reviews Meeting. The trial name "ARISE FLUIDS" appears in parentheses with the title. The x-axis shows days 0 to 90, and the y-axis represents the percentage of patients. Two lines indicate the percentage for vasopressors and fluids.
1
2
1,714
𝐑𝐚𝐥𝐩𝐡 𝐌𝐨𝐡𝐭𝐲 𝐌𝐃 𝐌𝐏𝐇 retweeted

Jun 11
ARISE-FLUIDS has arrived and it's awesome 🥳
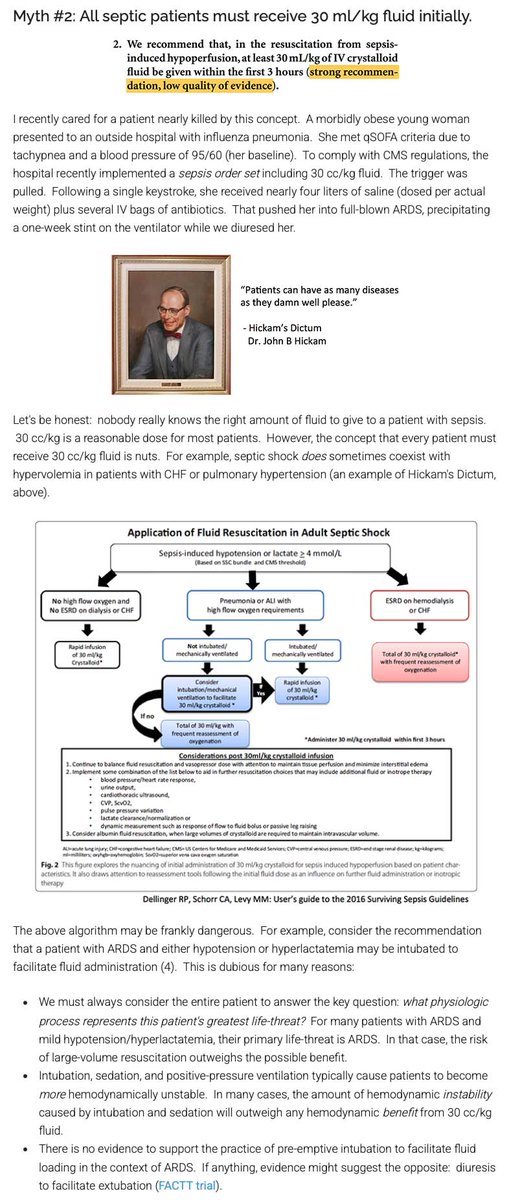
For over a decade, the Surviving Sepsis Guidelines recommended that septic patients get at least 30 cc/kg fluid. In the United States, these guidelines were weaponized into performance metrics, pressuring clinicians to prescribe arbitrary volumes to every patient.
Evidence-based clinicians have LONG known that this guideline lacked evidentiary support. For example, I've attached a picture of a blog I wrote about this back in 2017. Despite the lack of evidentiary support and some evidence of harm, the Surviving Sepsis Guidelines INSISTED on perpetually recommending 30 cc/kg fluid resuscitation.
We finally have a prospective RCT demonstrating that mandating early administration of 30 cc/kg fluid (as compared to early vasopressors) doesn't help and may actually cause harm.
It's important to note that all of the hard endpoints in this trial were neutral (e.g., mortality, days free of organ support).
I still think that 30 cc/kg fluid is a pretty reasonable volume of fluid for *most* patients. But the study does suggest that giving too much fluid may promote edema - so we should be *thoughtful* about this intervention rather than mandating it for every septic patient.
Based on the subgroup analysis, the fluid-conservative strategy may have helped the subgroup of pneumonia patients the most. This is statistically nonsignificant but aligns with my expectation. ARDSy patients often don't respond well to fluid. (In contrast, I really doubt that a liter of fluids in either direction matters for most urosepsis patients.)
This is a great example of the over-reach of guidelines and protocoled medicine. People get all upset about practice variation, so sometimes they try to stomp it out using guidelines and protocols. But these guidelines are highly fallible, so what may occur is that you standardize care in a way that harms everyone equally. 🤦♂️


17
146
461
58,408
𝐑𝐚𝐥𝐩𝐡 𝐌𝐨𝐡𝐭𝐲 𝐌𝐃 𝐌𝐏𝐇 retweeted

Jun 11
30 mL/kg has never been supported by evidence and physiologically it is nonsensical to think a weight-based prescription would be beneficial. Assess the hemodynamics in front of you and treat accordingly
1
7
40
12,296
𝐑𝐚𝐥𝐩𝐡 𝐌𝐨𝐡𝐭𝐲 𝐌𝐃 𝐌𝐏𝐇 retweeted

Jun 10
When I was an intern 3 pieces of paper went from the ER up to the floor: the doctor’s note, the nurse’s note and the registration information.
By the time I finished my fellowship (6 years later) it had metastasized into over 50 pages of worthless information…
With the occasional nugget of critical detail usually buried on page 32, which occurred during shift change and invariably got lost….
1
1
4
181
𝐑𝐚𝐥𝐩𝐡 𝐌𝐨𝐡𝐭𝐲 𝐌𝐃 𝐌𝐏𝐇 retweeted

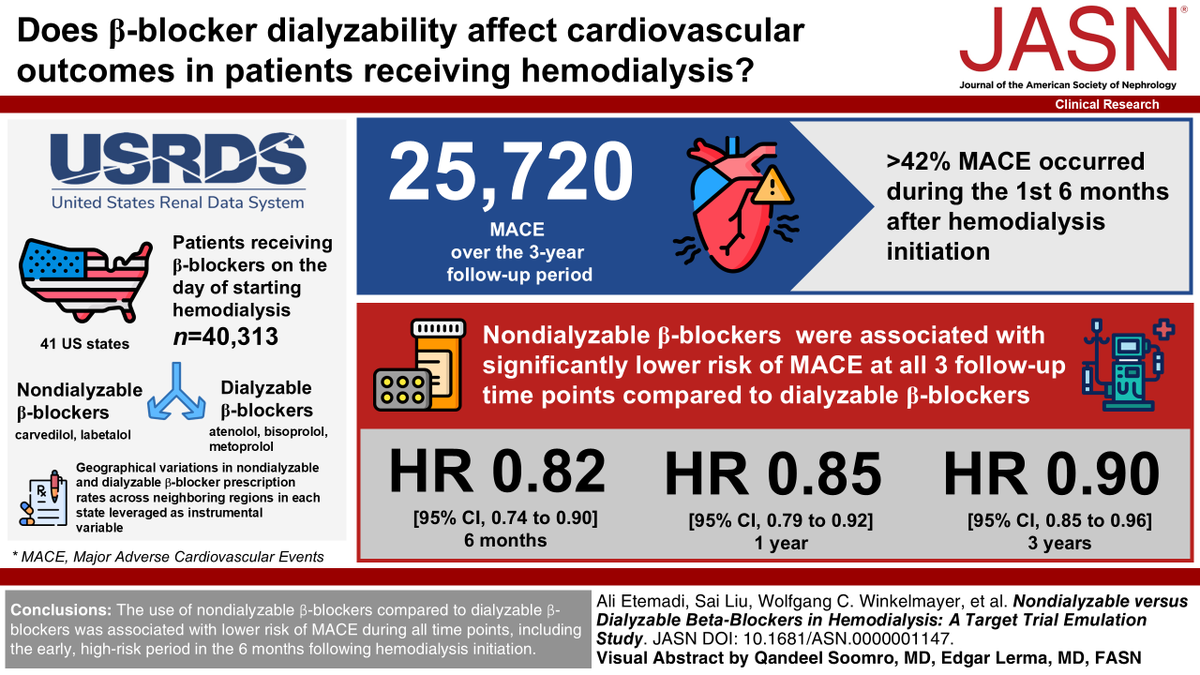
Is the use of nondialyzable vs dialyzable beta-blockers associated with different cardiovascular outcomes among patients initiating hemodialysis? Find out in #ASNJASN twp.ai/4hqlUo
17
33
4,585
𝐑𝐚𝐥𝐩𝐡 𝐌𝐨𝐡𝐭𝐲 𝐌𝐃 𝐌𝐏𝐇 retweeted

"Hipertensión Intradialítica: Cómo abordar la activación simpática y el volumen sin caer en la polifarmacia".
📈🫀
¿Qué haces cuando tu paciente de hemodiálisis sufre un aumento paradójico de la presión arterial durante la sesión?
La hipertensión intradialítica (aumento de la PA sistólica >10 mmHg post-diálisis) es un predictor independiente de mortalidad cardiovascular cruda.
Lejos de ser un fenómeno aislado, refleja sobrecarga de volumen oculta, activación simpática y disfunción endotelial.
Aplicación clínica: Antes de añadir más fármacos al tratamiento, optimiza la tasa de ultrafiltration (<10 ml/min/kg) y ajusta el sodio del dializado.
Si requieres fármacos, los betbloqueantes son la primera línea para frenar la hiperactividad simpática.
Bibliografía:
Chinnappa S, et al. Ten tips to control blood pressure in haemodialysis patients. Clinical Kidney Journal, 2026. doi:10.1093/ckj/sfag128. @CKJsocial
#Nefrología #MedicinaBasadaEnEvidencia #TrasplanteRenal #Hemodiálisis #NefroTwitter #hipertension #hypertension
1
19
45
1,940

𝐑𝐚𝐥𝐩𝐡 𝐌𝐨𝐡𝐭𝐲 𝐌𝐃 𝐌𝐏𝐇 retweeted

🧠 Are We Missing Half of the Brain's Circulation?
For decades, neurocritical care has focused primarily on arterial flow.
We monitor cerebral perfusion, vasospasm, autoregulation, pulsatility indices, and intracranial pressure. Yet one critical component of intracranial hemodynamics remains largely overlooked:
Cerebral venous outflow.
A recent review in Diagnostics argues that Transcranial Color Doppler (TCCD) should evolve beyond being merely the "stethoscope of the brain" for arterial circulation and begin incorporating systematic assessment of cerebral venous drainage.
The authors highlight a simple but important physiological concept:
🩸 Intracranial hypertension is not only a problem of arterial inflow.
It may also be a problem of impaired venous outflow.
Mechanical ventilation, elevated PEEP, hypercapnia, increased intra-abdominal pressure, Trendelenburg positioning, cardiac tamponade, pulmonary hypertension, large-bore jugular catheters, and venous obstruction can all impair cerebral venous drainage and contribute to cerebral congestion.
Using venous TCCD combined with internal jugular vein ultrasound, clinicians may be able to detect cerebral venous congestion before conventional markers such as optic nerve sheath diameter (ONSD) enlargement or arterial Doppler changes become evident.
Particularly interesting for intensivists and anesthesiologists, the review presents clinical examples where:
🔹 Mechanical ventilation reduced Rosenthal vein flow despite stable arterial Doppler findings.
🔹 Large-bore central venous catheters further impaired cerebral venous drainage.
🔹 Hemodynamically significant pericardial effusion produced profound venous congestion detectable by ultrasound before definitive diagnosis.
🔹 Pneumoperitoneum and Trendelenburg positioning increased jugular venous congestion during surgery.
The key message is not that venous TCCD replaces current neuromonitoring tools.
Rather, it may provide an additional physiological layer that helps explain why some patients develop intracranial hypertension despite apparently acceptable arterial parameters.
As critical care increasingly moves toward physiology-guided management, perhaps the next frontier is understanding not only how blood enters the brain, but also how it leaves it.
Question for the neurocritical care and perioperative community:
Do you routinely consider cerebral venous drainage when adjusting PEEP, patient positioning, pneumoperitoneum pressures, or central venous access strategies?
Reference📚
Bianchini A, Vitale G, Melegari G, et al. Transcranial Color Doppler for Assessing Cerebral Venous Outflow in Critically Ill and Surgical Patients. Diagnostics. 2026;16:289.
doi.org/10.3390/diagnostics1…
#NeurocriticalCare #POCUS #TCD #TCCD #CriticalCare #IntensiveCare #Anesthesiology #NeuroMonitoring #Ultrasound #MechanicalVentilation #ICP #BrainInjury #CriticalCareMedicine #FOAMed #MedEd

ALT
1
20
56
3,190
𝐑𝐚𝐥𝐩𝐡 𝐌𝐨𝐡𝐭𝐲 𝐌𝐃 𝐌𝐏𝐇 retweeted

Jun 7
True x 1000. This is the disconnect b/w GDMT evangelists and every day HF care. Never forget: trials enroll the best pts. Table 1 tells an important story
Jun 7

I ran a heart failure clinic years ago with the goal of maximizing GDMT therapy for systolic HF patients. Most patients sent to the clinic were over 80 with frailty and high fall risk. It was hard for them to even ambulate into clinic in some cases. Increasing GDMT meds lowered their blood pressure and made some dizzy. There were a few falls after meds were increased. I wondered if we were doing some of the patients any good. This showed me the problem with clinical care aimed at a treatment outcome measure (GDMT) rather the patient’s overall health.
10
6
102
39,261
𝐑𝐚𝐥𝐩𝐡 𝐌𝐨𝐡𝐭𝐲 𝐌𝐃 𝐌𝐏𝐇 retweeted

Far worse: seems the ADA called the police - on their own journal EiC and other well respected academics
See NYT coverage; nytimes.com/2026/06/05/well/…
#ADA2026
1
7
26
14,808
𝐑𝐚𝐥𝐩𝐡 𝐌𝐨𝐡𝐭𝐲 𝐌𝐃 𝐌𝐏𝐇 retweeted

Well the good news @hswapnil is that the lecture hall on extracorporeal treatments is pretty empty (so I’m guessing not many are buying it.) #ERA26
@CristinaDeReins already 🗑️ it:
nephjc.com/news/2026/short/t…
1
4
7
584
𝐑𝐚𝐥𝐩𝐡 𝐌𝐨𝐡𝐭𝐲 𝐌𝐃 𝐌𝐏𝐇 retweeted

Jun 6
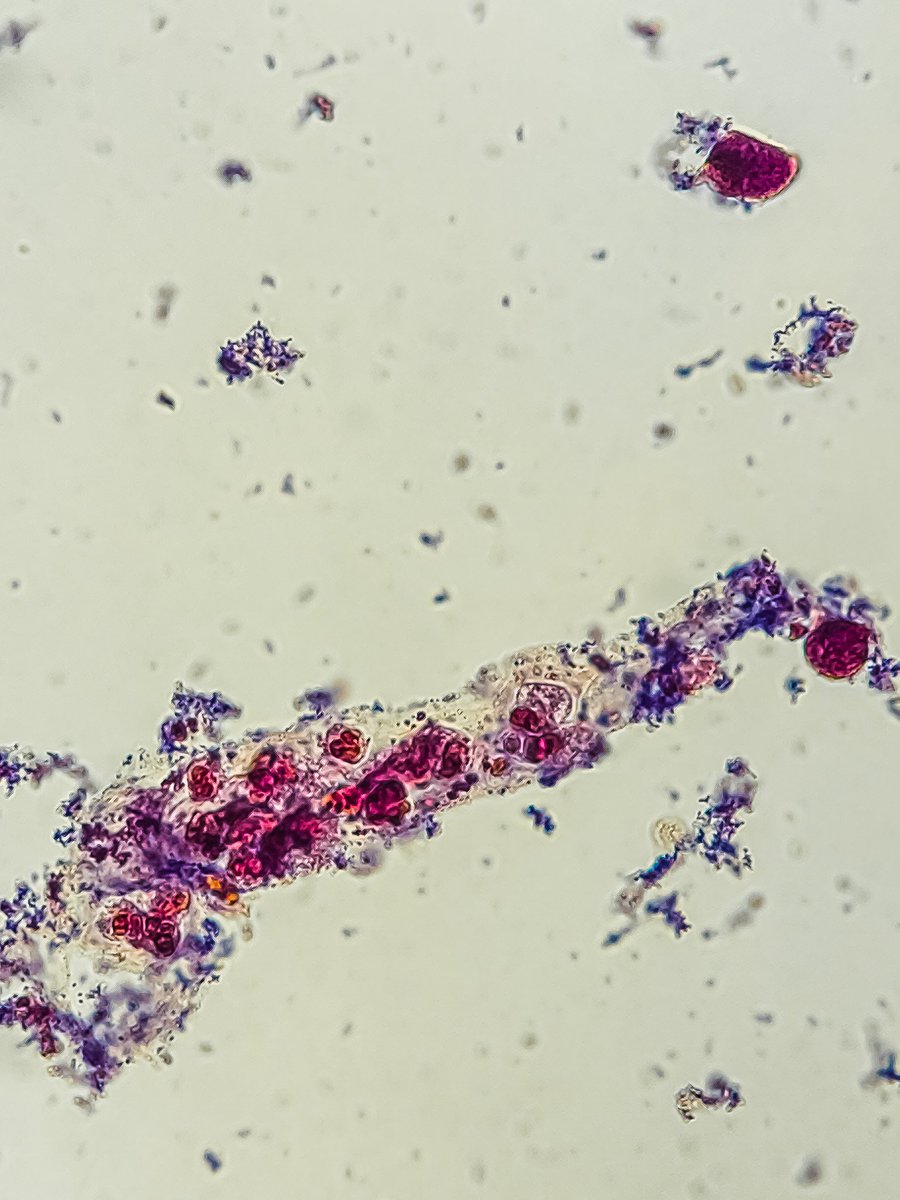
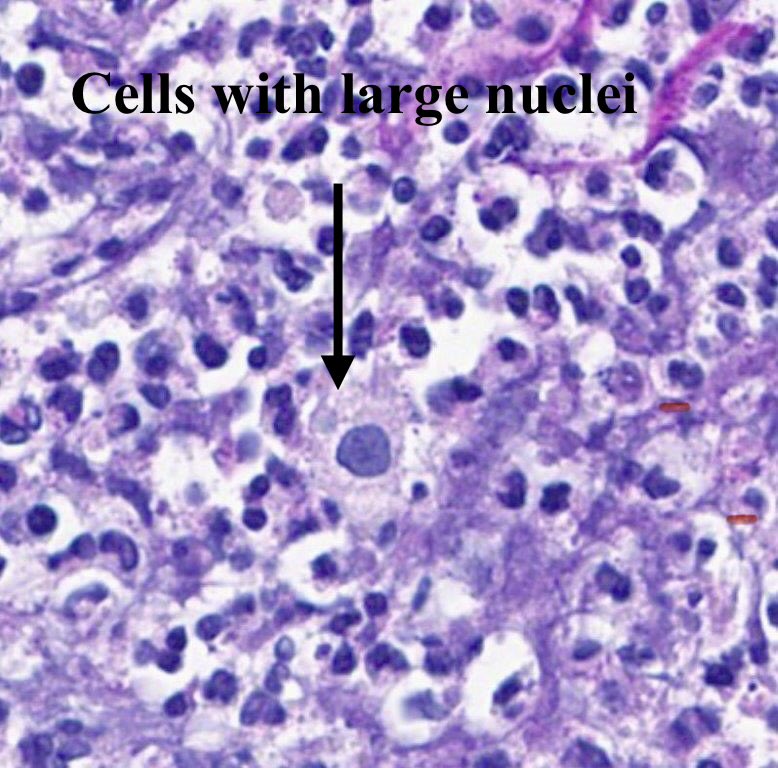
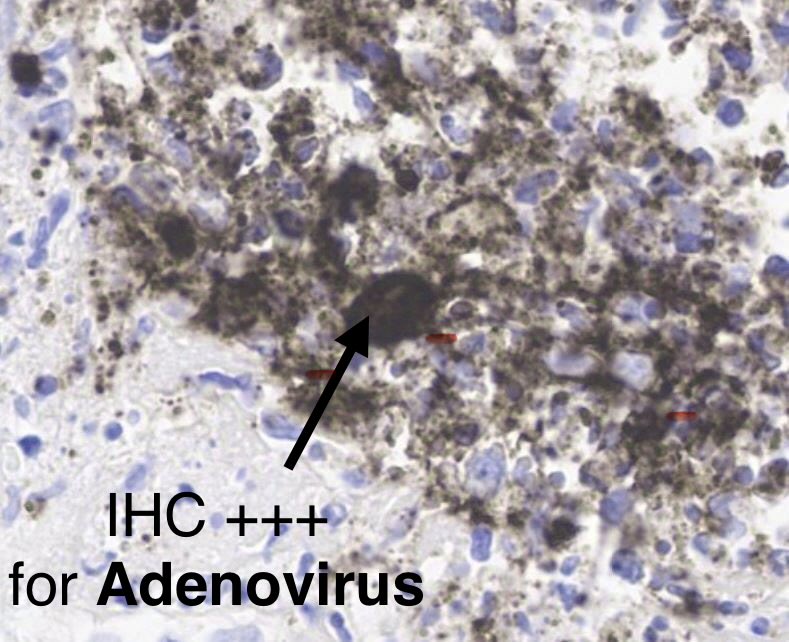
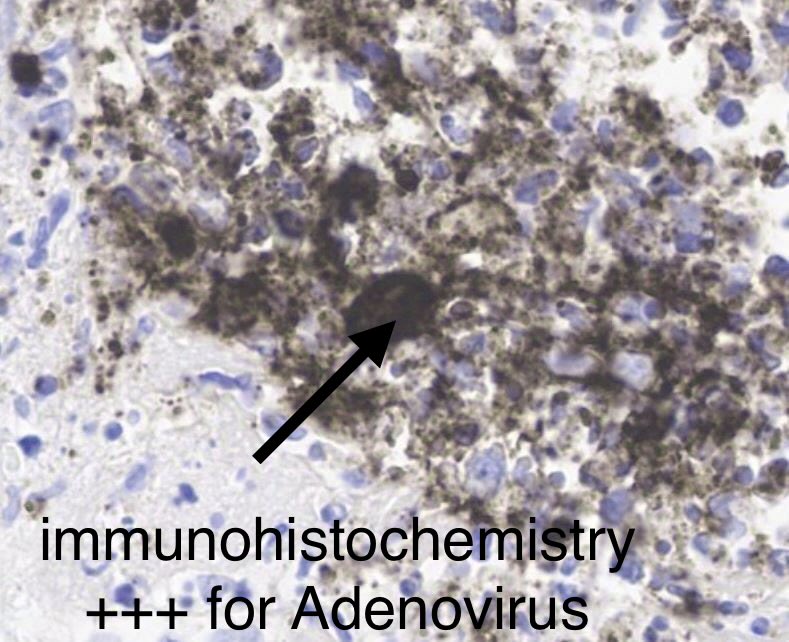
Kidney biopsy: Great teaching case
Severe inflammation and necrosis with abscess formation.
Look carefully=you see cells with large nuclei in the mix of inflammatory cells.
IHC= Positive staining for ADENOVIRUS.
DX: Adenovirus-associated interstitial nephritis.
55-yr old with kidney &
heart transplant, fevers, rise in serum creatinine.

2
42
127
6,246
𝐑𝐚𝐥𝐩𝐡 𝐌𝐨𝐡𝐭𝐲 𝐌𝐃 𝐌𝐏𝐇 retweeted
Jun 5
SOHO trial in NEJM:
🏙️ Multicenter RCT comparing high-flow nasal cannula vs. low-flow oxygen among patients with acute hypoxemic respiratory failure (mostly pneumonia)
🏙️ Inclusion criteria required a respiratory rate >25 and substantial hypoxemia (P/F <200)
🏙️ No difference in the primary endpoint of mortality (not surprising, the mortality endpoint is nearly always neutral in modern RCTs evaluating the nuances of supportive care).
🏙️ HFNC reduced the rate of intubation and increased the number of ventilator-free days.
🏙️ No significant signals of harm from HFNC.
This is similar to the FLORALI trial (by the same group of investigators). However, FLORALI showed *improvement* in mortality, whereas the current study didn't.
Why do these studies disagree about mortality?
The FLORALI trial found no mortality difference between HFNC versus conventional oxygen among ALL PATIENTS. However, it DID find a mortality difference in the *subgroup* of patients with P/F <200.
So this is a classic tale in critical care - a subgroup analysis from one trial subsequently fails to replicate. (At least, in terms of the mortality benefit.)
But chasing mortality in these trials is a fool's errand. Overall, the SOHO trial still supports the use of HFNC in acute hypoxemic respiratory failure (in terms of reduced intubation and improved ventilator-free days).
Using HFNC for sick pneumonia patients is already standard care, so I don't see this changing practice very much. Keep calm and HFNC on. 🌬️
For patients with acute hypoxemic respiratory failure, whether high-flow oxygen is superior to standard oxygen in reducing mortality is unclear. Research findings from the SOHO trial are summarized in a new Quick Take video. nej.md/4x706JY
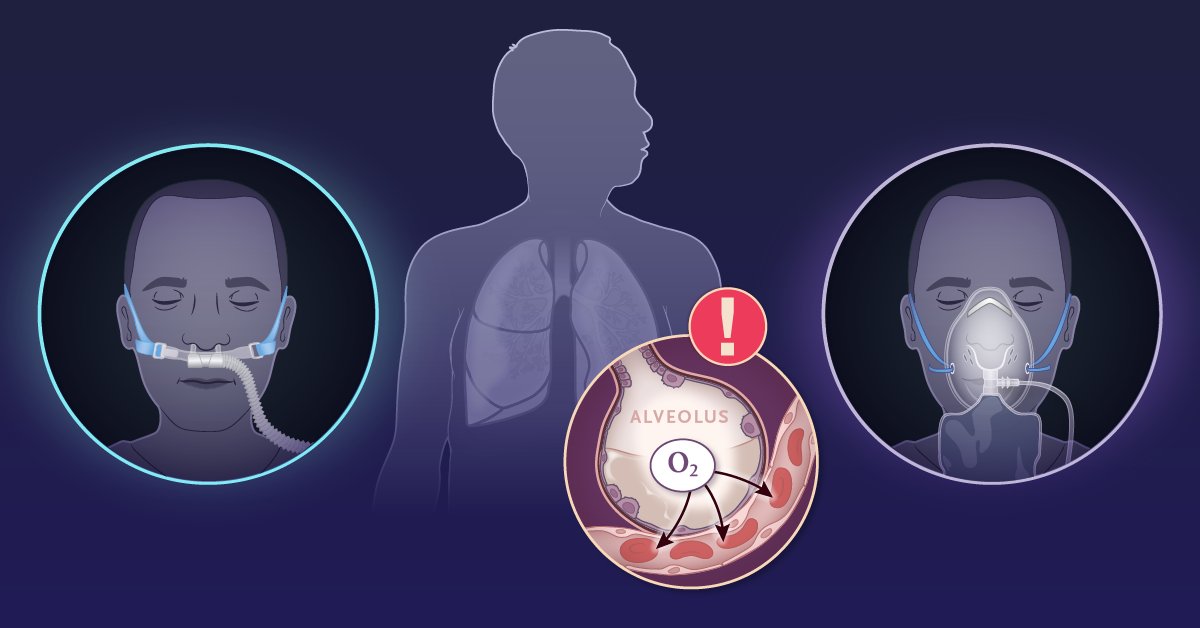
ALT An illustration showing a patient receiving oxygen through nasal cannula on the left and standard oxygen on the right. In the center, there is a diagram highlighting acute hypoxemic respiratory failure with an oxygen (O2) symbol and an exclamation mark, positioned against a silhouette of lungs.
4
39
149
33,773