
General surgery resident - Colorectal @IstTumori @LaStatale. Research Collaborator - Colorectal @MayoClinicSurg.
Joined June 2022
- Tweets 88
- Following 316
- Followers 82
- Likes 641
Photos and videos
Davide Ferrari retweeted

Pleased to share our new model to guide decision-making after total neoadjuvant therapy in locally advanced rectal cancer, now pub'd in @AnnalsofSurgery! ⚡️
Paper 📝: journals.lww.com/annalsofsur…
Online calculator 💻: chrisvarghese-pccr-estimator…

1
9
20
2,976
Davide Ferrari retweeted

Cheers, chills, and a standing ovation when RASolute 302 showed unprecedented survival on daraxonrasib for patients with progressive pancreatic cancer
Seldom do you sense you’re witnessing a historic moment in cancer care but this feels like ras targeting has arrived
#ASCO26
92
1,273
6,506
1,148,807
Davide Ferrari retweeted

Apr 23
In my opinion OpenEvidence has basically ended the need for UpToDate, however, some disagree.
Can we at least all agree that there is virtually no role now for medical book chapters, reviews etc… that are obsolete the second they are finally published.
80
28
522
71,870
Davide Ferrari retweeted

Jan 25
I’m going to halve my publication output. You should consider slow science, too nature.com/articles/d41586-0…
1
3
21
7,544
Davide Ferrari retweeted

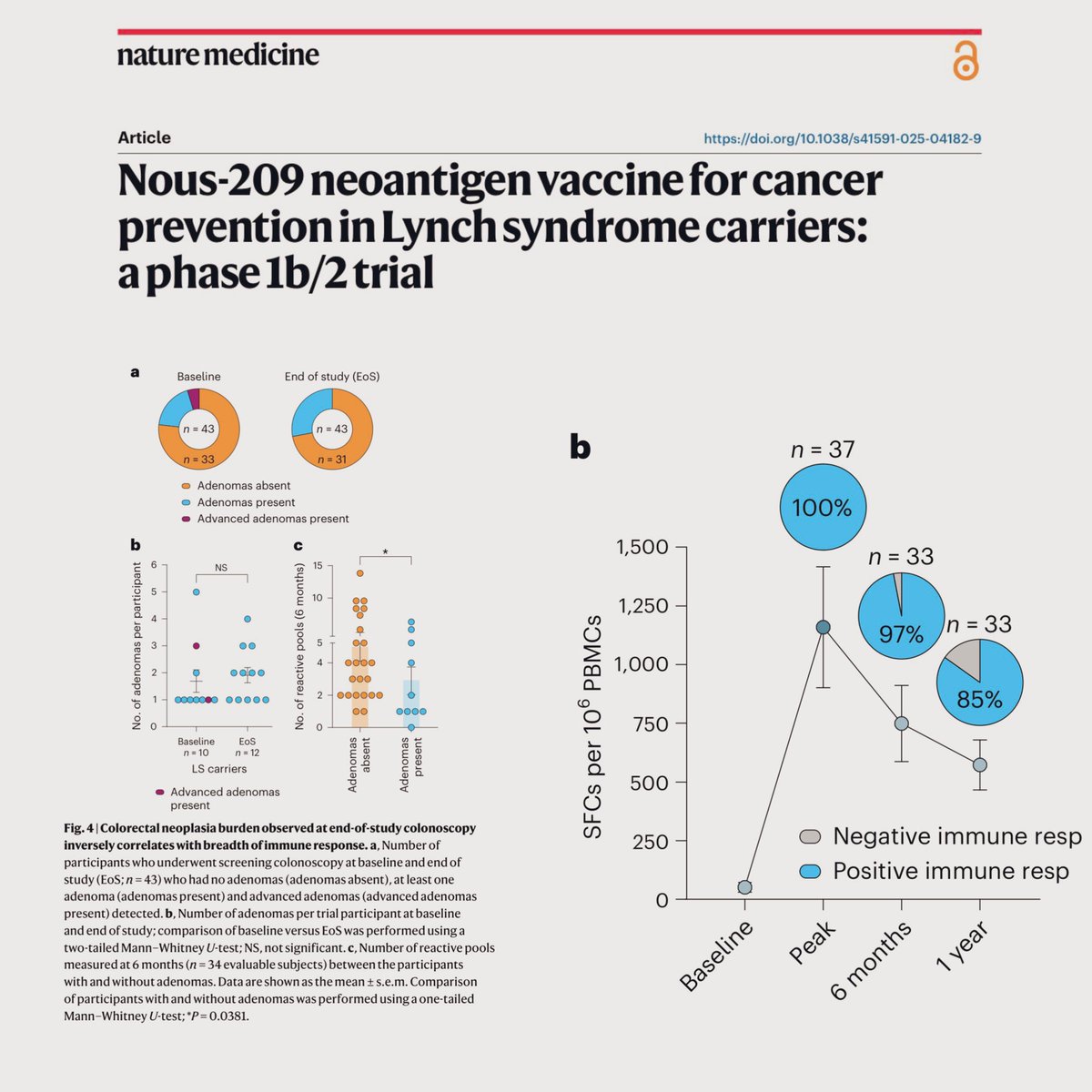
🆕🗞️ A Vaccine💉for cancer🦀interception.
A preventative approach aiming to reduce cancer incidence by targeting precancers and early-stage cancers. For patients with Lynch syndrome. Out @NatureMedicine📰
Paradigm↩️intervene early✅
#Cancer @OncoAlert
nature.com/articles/s41591-0…
7
19
37
9,053
Davide Ferrari retweeted

Jan 10
Is it sexy? No.
Is it incredibly important for how we treat patients? Absolutely 🧠🧬
For over 20 years, 6 months of oxaliplatin plus a fluoropyrimidine has been the default for stage III colon cancer, and often high-risk stage II and rectal cancer. The cost has always been cumulative neuropathy that can follow patients for life ⚡️🖐️
The SCOT trial, the largest study in the IDEA collaboration, gives us long-term clarity with nearly 6,100 patients and more than 6 years of follow-up:
📊 5-yr DFS identical with 3 vs 6 months: 72.9% vs 72.9%
📈 5-yr OS identical: 82.4% vs 82.4%
✅ Noninferiority for OS formally met for 3 months
Where this really matters clinically:
🟢 CAPOX clearly supports 3 months
🟢 Low-risk stage III shows no OS penalty
🟡 Even high-risk disease sees only tiny absolute OS differences
⚠️ Meanwhile, neuropathy nearly doubles when oxaliplatin is extended to 6 months. Many patients pay a lifelong price for minimal benefit.
SCOT also uniquely included rectal cancer patients treated with upfront surgery, and here too, 3 months held up. This fits perfectly with modern TNT strategies 🧩
Takeaway:
This isn’t flashy, but it’s foundational. For most patients with localized colon or rectal cancer, 3 months of adjuvant CAPOX is enough. Six months should be the exception, not the rule, and always a shared decision 🤝
Sometimes the most important advance is knowing when to stop.
@OncoAlert @TheGutOncLab
#GI26
ascopubs.org/doi/pdf/10.1200…

14
137
371
57,253
Davide Ferrari retweeted

1 Dec 2025
Does organ preservation after cCR with TNT🧨
affect distant metasases rate in rectal ca?
Results of NO-CUT🚫🔪trial @TheLancetOncol
show 26% of pMMR/MSS pts achieve cCR and
distant RFS 95% in nonop group vs 74% SOC
@OHSUKnight @tsikitis @HKennecke
sciencedirect.com/science/ar…
4
51
128
28,183
Davide Ferrari retweeted

13 Nov 2025
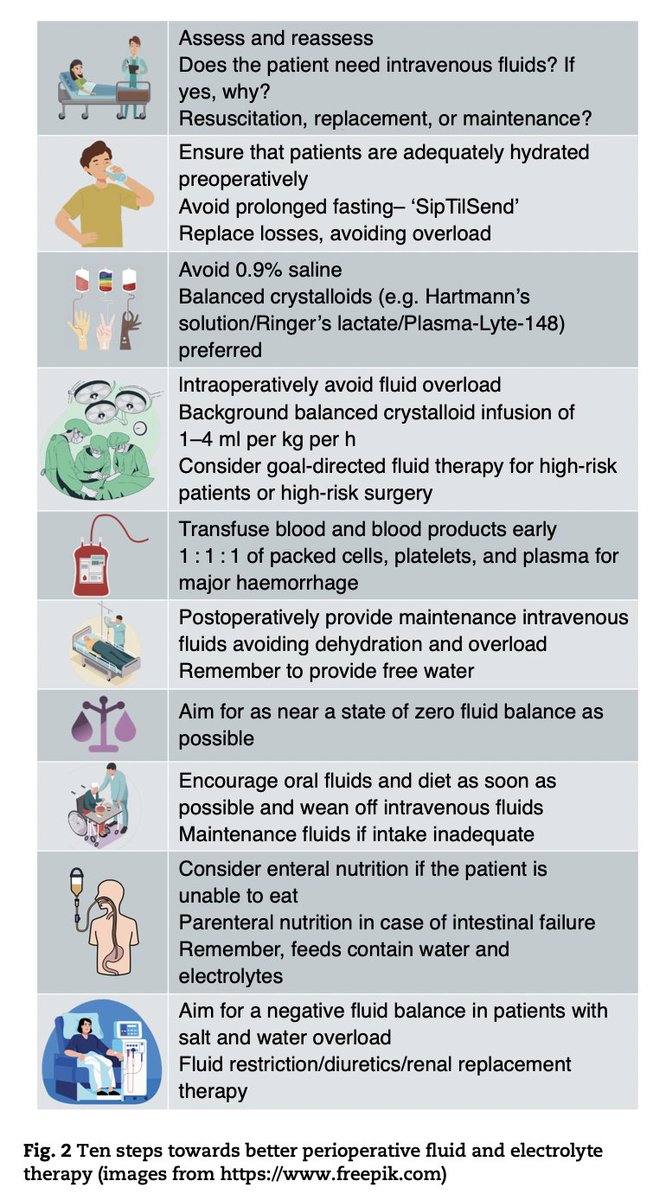
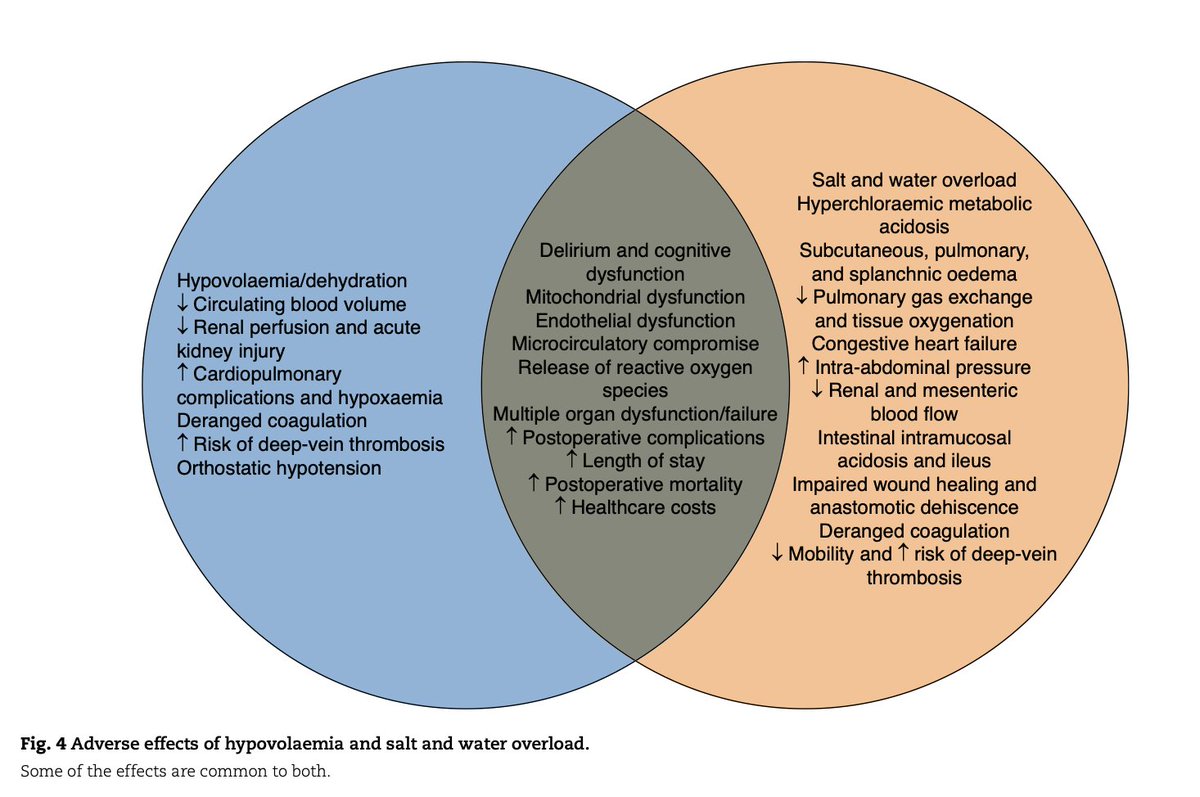
Ten steps towards better perioperative intravenous fluid therapy
➡️ doi.org/10.1093/bjs/znaf179
💧 IV fluids are drugs — both deficit and overload worsen outcomes, yet perioperative prescribing is often overlooked and delegated to juniors
🩺 The paper stresses ABCDE assessment and clear indication (resuscitation, replacement, maintenance), plus better pre-op hydration with “SipTilSend”
⚖️ Intraoperatively, it advocates balanced crystalloids over 0.9% saline, low-rate background infusions, and goal-directed boluses to avoid salt–water overload
🩸 For bleeding, early 1:1:1 blood product transfusion is advised
🥤 Post-op care focuses on tailored maintenance (≤2–2.5 L/day), early oral intake, and aiming for near-zero or negative fluid balance to reduce complications
Work by Michael Ess, Dileep N Lobo @DL08OMD
#SoMe4Surgery #MedTwitter #SurgEd #Surgery @RCPSGTrainees @aecirujanos @SEIQuirurgica @iss_sic #MedicalTechniques @BJSAcademy @young_bjs @BJSOpen @des_winter @evanscolorectal @robhinchliffe1 @bplwijn @MalinASund @nfmkok @TejedorPat @paulo_sutt @PVaughanShaw @JJEarnshaw @juliomayol @ksoreide #some4hpb #some4tpl @DPCG_official @pancreatitis_nl @PancreasClub #PancreasClub2023 #PancreaticCancer #Pancreatitis #HCC @PanCAN#PanCANawareness @EurPancClub @P_C_E_ @dice_europe #PancreaticCancer#cholangiocarcinoma #colorectalsurgery #StepUp4CRC @FightCRC @ACPGBI #ERAS @dice_europe #Crohn #proctology @Dukes_Club @ACPGBI_EduTrain @AECP_FAECP @PelvExGroup @escp_tweets @YouESCP #TeachMeColoproctology
#Some4COLoprocto
56
151
12,087
Davide Ferrari retweeted

12 Oct 2025
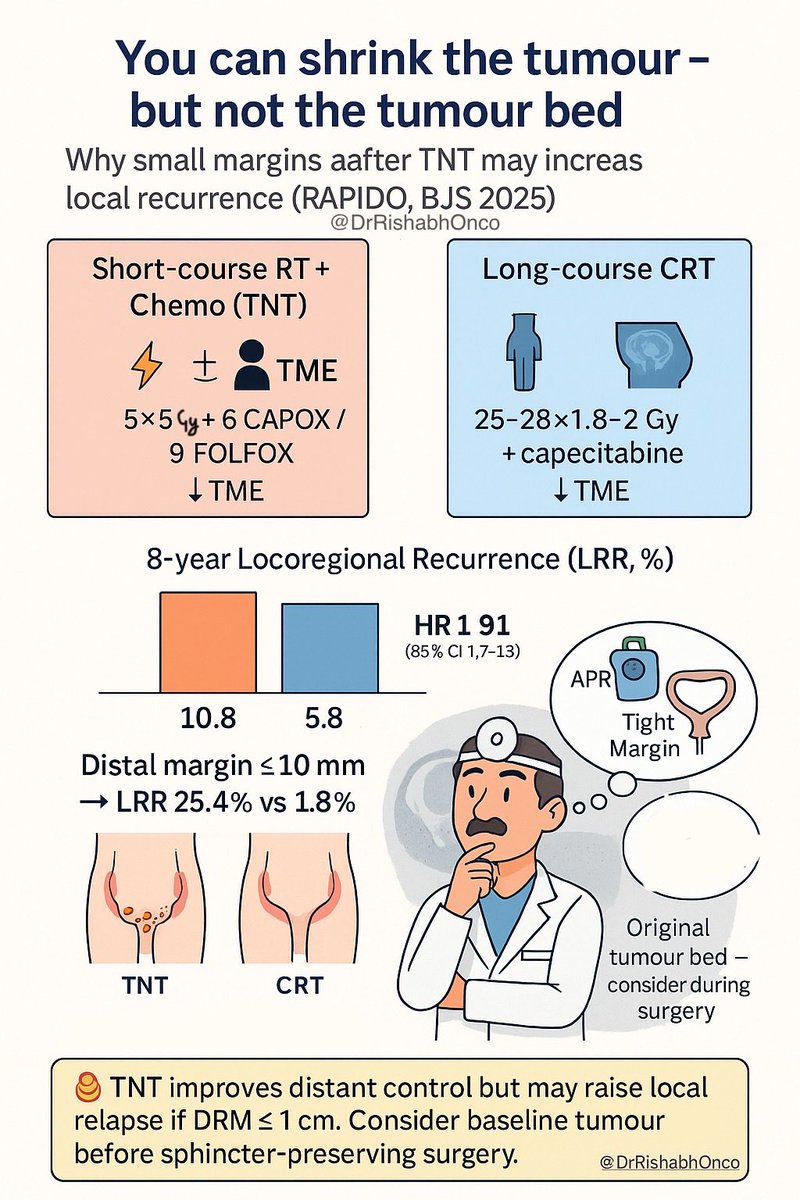
🧠 You can shrink the tumour—but not the tumour bed.
New RAPIDO analysis in BJS 2025 shows why small margins after TNT can turn dangerous 👇
💡 Trial: RAPIDO (n = 920, LARC)
🎯 TNT = 5×5 Gy 6 CAPOX / 9 FOLFOX → TME
vs CRT = 25–28×1.8–2 Gy capecitabine → TME
📊 8-year results:
• LRR 10.8% (TNT) vs 5.8% (CRT) → HR 1.91
• Spike seen only after sphincter-preserving surgery (SPS)
→ 12.1% (TNT) vs 4.8% (CRT) (HR 2.6)
• 🚨 If distal margin ≤ 10 mm → 25.4% (TNT) vs 1.8% (CRT) 💥 (HR 15.5)
🔍 Why?
TNT causes tumour shrinkage but leaves scattered viable cells in the original tumour bed.
✂️ Cutting “too close” (<1 cm) may slice through microscopic disease → higher local recurrence.
🇸🇪🇳🇱 Geography tells the story:
Sweden = more APR → no difference
Netherlands = more SPS & tight margins → higher TNT LRR
🩻 Takeaway:
TNT reduces distant mets ✅ but may raise local relapse if DRM ≤ 1 cm ⚠️
➡️ Surgeons must factor in baseline tumour bed, not just post-TNT shrinkage.
📖 Prata I et al. Br J Surg 2025
🔗 doi.org/10.1093/bjs/znaf190
#OncoTwitter #ColorectalCancer #RectalCancer #RadOnc #Surgery
@OncoAlert @esmo_open @BJSurgery
@myESMO
2
93
185
10,787
Davide Ferrari retweeted

2 Oct 2025
Is Minimally Invasive Surgery at an Inflection Point? facs.org/for-medical-profess…
1
5
19
1,727
Davide Ferrari retweeted

19 Sep 2025
#Rise of the #Robots 🦾 in the Netherlands 🇳🇱 GI surgery @AnnalsofSurgery
😳 How does this compare to your country? Data?
Nationwide use 🦾 per organ among 77,361 resections (2014-2023):
✅ pancreas 1% to 33%
✅ thoracic 3% to 11%
✅ colon 6% to 14%
✅ rectum 19% to 45%
✅ liver 10% to 25%
✅ esophageal 33% to 40%
↔️ gastric 19% to 19%
⏩️ journals.lww.com/annalsofsur…

11
40
4,119
Davide Ferrari retweeted

5 Sep 2025
Interesting paper questioning the need for routine type and screen by @KhanSidrah786 from her year at @MayoClinicSurg colorectal surgery fellowship
3 Sep 2025

Which pts undergoing elective colorectal resections need a preop type & screen? Find out exclusively in #DCRJournal: bit.ly/4fZIeIX
1
1
181
Davide Ferrari retweeted

3 Sep 2025
Which pts undergoing elective colorectal resections need a preop type & screen? Find out exclusively in #DCRJournal: bit.ly/4fZIeIX
4
2
889
Davide Ferrari retweeted

29 Aug 2025
RA-CUSUM charts offer a powerful tool to track surgeon performance in rectal cancer cases—spotting trends in complications, operative time, and outcomes in real time.
journals.lww.com/annalsofsur…
1
2
1,273
Davide Ferrari retweeted
18 Aug 2025
This study shows how RA-CUSUM can identify high and low outliers in robotic rectal surgery—offering a data-driven path to continuous surgical improvement.
journals.lww.com/annalsofsur…
1
6
1,687
Davide Ferrari retweeted

29 Jul 2025
For the 36th consecutive year since U.S. News & World Report launched its "Best Hospitals" rankings, Mayo Clinic again ranks at the top of the 2025–2026 list.
Read more: mayocl.in/4716aJm

474
120
317
97,585
Davide Ferrari retweeted

28 Jun 2025
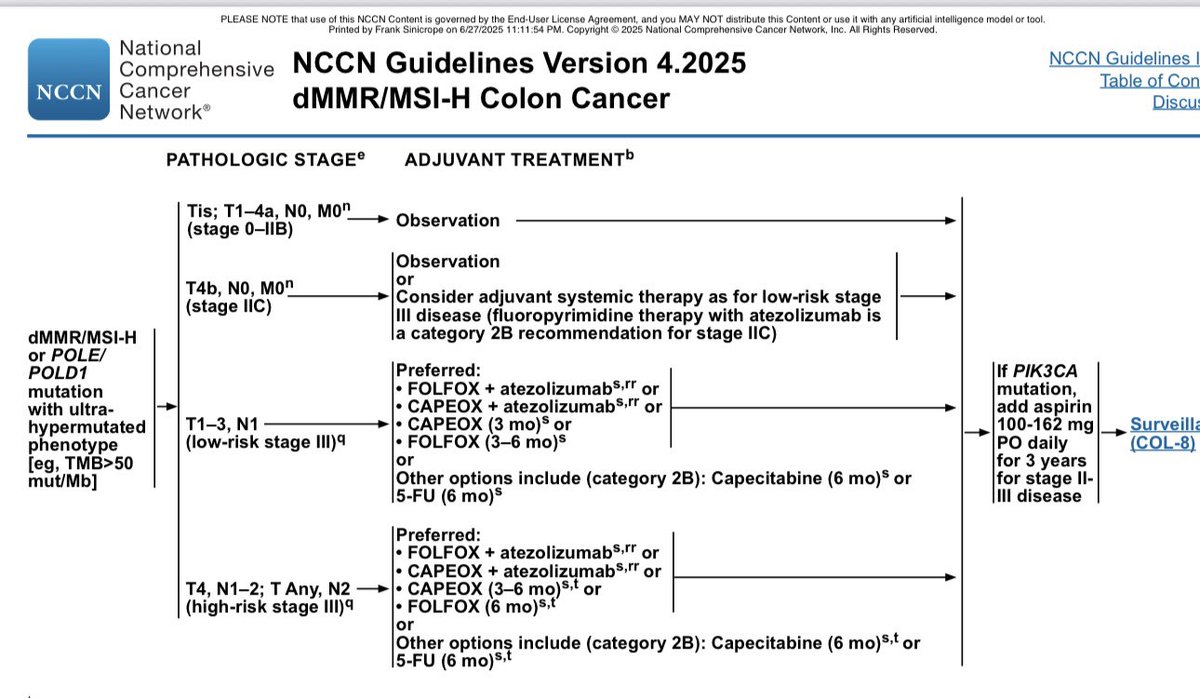
For dMMR colon cancer, FOLFOX atezolizumab per ATOMIC is now incorporated into the NCCN Guidelines.
@MayoCancerCare @ALLIANCE_org @ASCOPost @CCAlliance @RueschCenter @FightCRC
6
76
230
19,814
Davide Ferrari retweeted
18 Jun 2025
Great work team
@JyiChengNg @RichardSassun @AnnaclaraS65
@MayoClinic @MayoCancerCare @MayoClinicSurg
18 Jun 2025

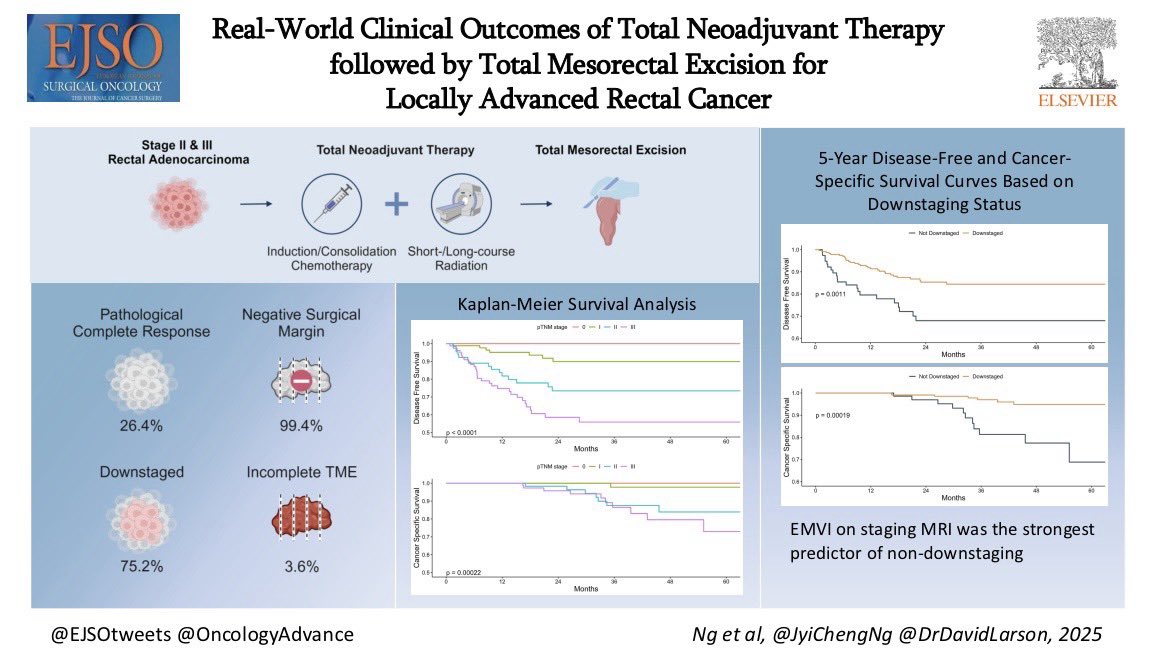
🔥 Hot off the press in @ejsotweets!
Real-world surgical & oncological outcomes of rectal cancer patients treated with TNT followed by TME at @MayoClinicSurg.
🔗: lnkd.in/gmkTV-XK
Huge thanks to 🧢 @DrDavidLarson and coauthors @RichardSassun @AnnaclaraS65 @tommyv1992

2
10
911
Davide Ferrari retweeted
14 Jun 2025
Vacation: #sailing with Capt Marco in #Sardinia fantastic water, beaches, mountains, food and Friends. @DFerrariMD @RichardSassun @tommyv1992 @EricaCento
4
20
657
Davide Ferrari retweeted

Safe Same-Day and Short-Stay Stoma Closures Revolutionize Care
by Ferrari D, Violante T (...) Larson DW et 7 al. in J Gastrointest Surg
🪡 read our summary 👉 stitches.today/2025/06/10/sa…
📖 read the article: sciencedirect.com/science/ar…
2
4
382