
Thriller award nominated author and anthropologist. Suspense thrillers CAGED, BURIED, and CUT TO THE BONE available now. #TreatLongCovid Agent: @aftannenbaum
Joined May 2017
- Tweets 5,065
- Following 989
- Followers 4,569
- Likes 43,161
199 Photos and videos








Pinned Tweet

19 May 2020
I hate self promotion, especially right now, but I just have to link my starred review over @PublishersWkly because I am so damn honored. This is one of those dreams that you don't ever expect to actually happen. Never stop writing, my friends. bit.ly/3e1rZcY
15
28
146
Ellison Cooper PhD retweeted

Jun 2
‼️⚠️Please read this until the end.
A widely shared article has presented a deeply misleading view of Long COVID, suggesting once again that cognitive behavioral therapy, exercise, and “mind-body” approaches may be the uncomfortable truth patients refuse to accept.
This needs to be challenged.
Not because the nervous system does not matter.
Not because psychological support cannot help.
But because confusing support with cure, physiology with psychology, and heterogeneity with “it might be in your head” is exactly how medicine has harmed post-infectious patients for decades.
There are articles about Long COVID that look like science journalism, but in reality they repackage, in modern language, a very old idea: if we do not fully understand a disease, maybe the problem is in the patient’s mind.
And that is not science. That is repeating history.
The article begins with a striking sentence:
“There isn’t a single approved pharmaceutical treatment, not even a test to verify the presence of the illness.”
This may sound forceful, but it is a very misleading way of presenting the problem.
The fact that there is still no drug specifically approved for Long COVID, or a single diagnostic test, does not mean that “nothing has been found.” It means that we are dealing with a heterogeneous disease, probably with several biological subgroups, and that medicine has not yet converted those findings into validated clinical tools.
“No single diagnostic biomarker” is not the same as “no biology.”
In just a few years, immunological, vascular, neurological, endocrine, and metabolic abnormalities have been described in subgroups of Long COVID patients: autonomic dysfunction, herpesvirus reactivations such as EBV/HHV-6, alterations in the cortisol axis, autoantibodies against GPCR receptors — including adrenergic and muscarinic receptors — persistent viral antigens, endothelial damage, muscle abnormalities after exertion, mitochondrial dysfunction, persistent inflammation, and differential immune changes.
Is everything settled? No.
Does that mean it is psychological? Also no.
Science does not work like that. Multiple sclerosis did not stop existing before we had MRI. Many autoimmune diseases do not show up in routine blood tests. If a complete blood count, a basic biochemistry panel, or an X-ray comes back “normal, normal, normal,” that does not prove the absence of disease. It only proves that you are looking with inadequate tools.
One of the article’s most serious mistakes is this: it confuses the absence of a simple clinical test with the absence of organic disease.
And that mistake has caused harm for decades.
The article also says:
“Almost $2 billion and half a decade of international effort have yielded little more than hypotheses about micro blood clots and spike proteins and mitochondrial dysfunction.”
No. That is not correct.
A hypothesis is a provisional explanation. But when you compare patients and controls and find significant differences in muscle tissue, metabolism, response to exertion, immune biomarkers, viral antigens, autoantibodies, or vascular dysfunction, you are no longer talking about “little more than hypotheses.” You are talking about lines of biomedical evidence that still need to be organized, replicated, stratified, and translated into treatments.
That is not scientific failure. That is research into a complex and new disease.
🔵Continued in the next post.👇🏻
(1/6)

Six years since the height of the pandemic, the scientific community remains baffled by long Covid. But there might finally be a way forward for long Covid treatment—if only you were allowed to talk about it.
wired.com/story/the-painful-…
35
215
686
32,924
This is amazing research at the forefront of untangling the biomedical roots of Long Covid. Maybe @WIRED could report on this instead of platforming anti-science quacks.

Check out these talk summaries from our recent PolyBio Symposium👇
Highlights include that four groups — Tim Henrich (UCSF), Marcus Buggert (Karolinska), Nicolas Huot (Institut Pasteur), and Esen Sefik (Yale) — presented different lines of evidence (human gut biopsies, non-human primate models, humanized mice) all pointing to the same conclusion: SARS-CoV-2 persists in #LongCovid gut tissue and adjacent lymphoid structures, and that persistence drives ongoing immune dysregulation.
3
671
Ellison Cooper PhD retweeted

Jun 3
Ok.
I've read "The Painful Truth About Long Covid" six times through, and I'm ready.
Here are ten clues in the article that point to the writer's bad faith.
27
273
1,104
65,549
Ellison Cooper PhD retweeted

Mar 24
Excited to get this out in preprint: triple-blind, placebo-controlled microtesla magnetic therapy (MMT) is safe, feasible and effective in reducing cognitive impairment in people with #LongCOVID. I get excited about interventions for cognitive symptoms
medrxiv.org/content/10.64898…
1/
29
136
486
44,875
Ellison Cooper PhD retweeted

1/ If I hear one more public official call indoor air filters a "band-aid," I'm going to explode! It's so logical, yet so readily dismissed. Filtering indoor air should be as standard as filtering water. Full stop. 🧵
53
814
2,684
89,826
Ellison Cooper PhD retweeted

Feb 23
"Tirzepatide has given me an 85% improvement after 15 years of moderate to severe #MECFS and trialing 20 other meds that either didn't work or only gave me a 1-3% improvement." reddit.com/r/cfs/comments/1r…
27
55
406
18,816
Ellison Cooper PhD retweeted

4 Dec 2025
Yale scientists reviewed 100 years of records and found that Long COVID is part of a larger pattern.
Viruses like polio, SARS, and EBV have long caused lasting illness in some people, often through immune dysfunction
cell.com/trends/immunology/f…
33
558
1,761
111,933
2 Dec 2025
My new favorite game: after reading any post that mentions the words long covid, I like to try and guess how many replies it will be until the first “it’s the jab” shows up. Apparently if you say the magic words they appear as if conjured by the magical troll fairy.
4
66
29 Oct 2025
Been a long while since I posted. Mestinon has recently moved the needle for me a bit but I’m still mostly housebound (and always masking when I go out.) In good news I’m almost done with my next book. Fingers crossed it sells!!!!
ALT A middle aged white woman is wearing a 3m aura mask in front of a UC Davis medical sign.
1
4
132

After a long wait, our longitudinal long COVID study is finally published in @NatureComms: nature.com/articles/s41467-0…. We find a skeletal muscle alterations in patients with #longcovid, which worsen with exercise. 1/n
304
2,397
5,561
1,334,191
Ellison Cooper PhD retweeted

16 Oct 2025
Long Covid Is Real — And It’s Changing an Entire Generation
Hundreds of thousands of kids in America are struggling with an illness that many doctors and schools refuse to recognize.e
Feature: rollingstone.com/culture/cul…

259
3,481
7,643
1,667,710
Ellison Cooper PhD retweeted

3 Oct 2025
Therapy helps but let’s be clear. You can’t CBT your way out of capitalism. You can’t mindfulness your way out of racism. You can’t self care your way out of oppression. You can’t journal your way out of ableism. This isn’t about coping, it’s about deconstructing the systems.
105
5,524
20,627
297,049
Ellison Cooper PhD retweeted

1 Oct 2025
🧠 Thread: A molecular clue to Long COVID “brain fog”
1/ New study from Yokohama City Univ used PET imaging of AMPA receptors. Long COVID patients showed elevated AMPAR levels, linked to both cognitive impairment and inflammation. A molecular biomarker emerges.
3
33
91
11,474
Ellison Cooper PhD retweeted
27 Sep 2025
A few days out from #UNGA80, I wanted to reflect on the session we took part in and the media responses since. Mount Sinai was one of the 150 organizations that signed the global pledge to advocate for healthy indoor air. The event itself featured four panels of speakers who
1/
32
248
676
62,927
Ellison Cooper PhD retweeted

21 Sep 2025
I do still think this article is a turning point.
bmj.com/content/390/bmj.r173…
9
68
275
9,399
Ellison Cooper PhD retweeted

3 Sep 2025
New from @PutrinoLab & Dr. Pridgen:
A combo of 120 days of celecoxib & valacyclovir with 15 days of Paxlovid is significantly more effective than celecoxib & valacyclovir alone!
The combo had vastly greater response rates for brain fog, dysautonomia, & fatigue. #LongCovid 1/
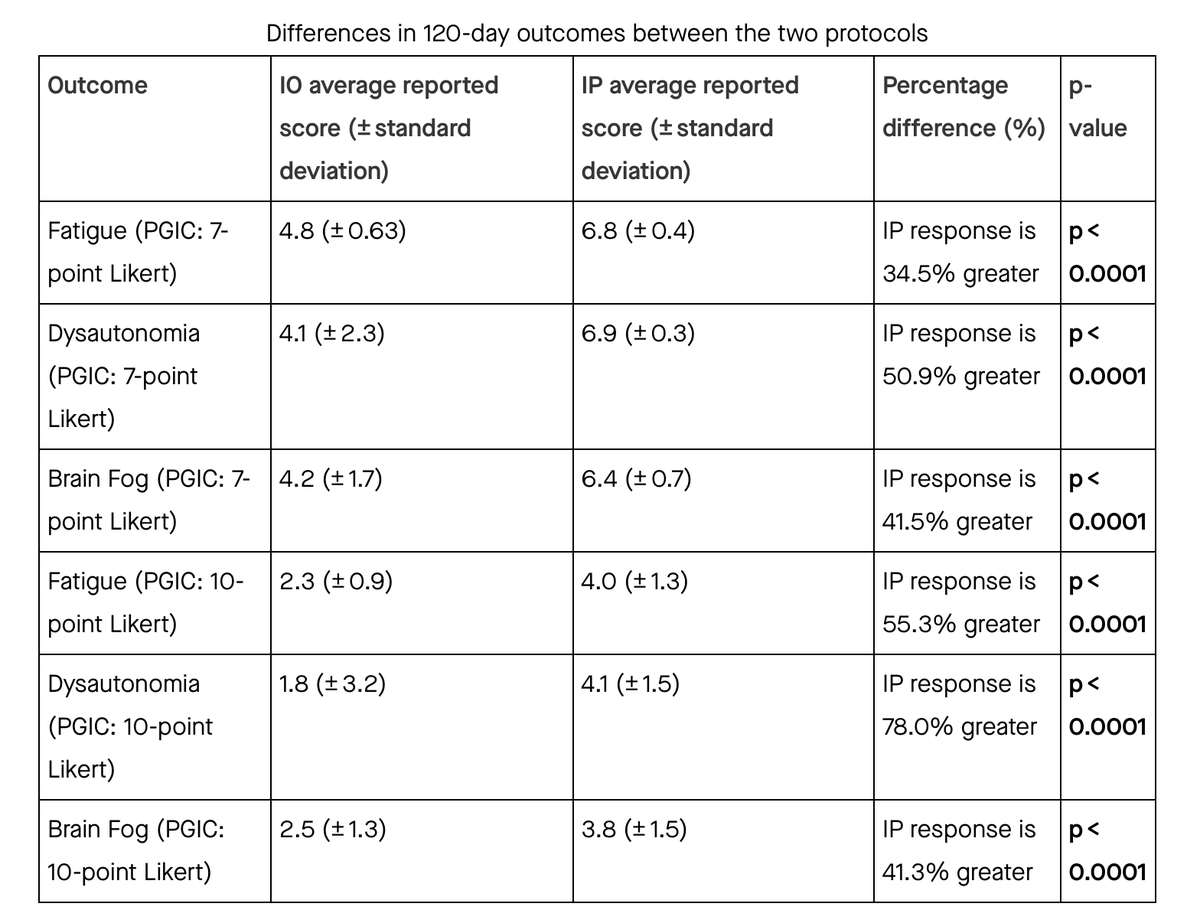
ALT differences in improvements between the two protocols show 41% better response for brain fog, 51-78% better response for dysautonomia, and 35-55% for fatigue
24
200
730
56,232
Ellison Cooper PhD retweeted

Traveling? The U.S. is experiencing a summer COVID-19 surge. Lower your chance of catching COVID-19 by masking in indoor public places like airports and planes. Wear a high-quality mask like an N95, KN95 or KF94 to stay protected. Learn more: cdph.ca.gov/Programs/CID/DCD…

ALT Promotional image by CDPH featuring a person wearing a mask, walking through an indoor public space, holding a smartphone and a bag, with text urging 'Consider Masking in Indoor Public Places' to slow the spread.
96
563
1,400
208,139
Ellison Cooper PhD retweeted
14 Aug 2025
Incredibly exciting diagnostic tool potential — @ImmunoFever MIT team is doing nailfold capillaroscopies on #LongCovid patients before and after a NASA lean test, and said the results have been incredibly striking compared to controls.
My results were very abnormal !
36
264
1,328
100,428
Ellison Cooper PhD retweeted
11 Aug 2025
Kicking off #KeystoneSympsoia with a room full of masks led by @VirusesImmunity & @MichaelPelusoMD🙏 #LongCovid

ALT Room full of people wearing masks in conference room !
131
416
2,258
456,729
Ellison Cooper PhD retweeted

7 Aug 2025
He died from Long COVID today. His words: “I’ve experienced more discrimination and stigma for being openly disabled by #LongCovid than I ever did for being openly gay” When will the gaslighting stop? How many more need to die?
7 Aug 2025

New York designer Derrick Kardos, known for Black Swan and The Departed, has died at 53 from complications of Long COVID.
He was a fierce creative force and advocate for Long COVID recognition.
hollywoodreporter.com/movies…
58
1,522
4,642
183,150