
Professor @TuftsMedSchool, Co-Founder @Naveris_inc. Dedicated to understanding the biological, molecular, and genetic underpinnings of cancer & prevention.
Joined August 2015
- Tweets 744
- Following 208
- Followers 1,646
- Likes 357
132 Photos and videos





Charlotte Kuperwasser, PhD retweeted

Jun 5
TRAILER:
New documentary from @WSJ on Great Barrington Declaration, Twitter Files, and Covid dissent!
Full doc dropping next week.
70
685
2,269
111,825
The most widely used herbicide in US farming…Atrazine is an endocrine disruptor. It cause mammary tumors in animals: Cancer Sci. 2005 Jan 13;96(1):19–25.
atsdr.cdc.gov/toxprofiles/tp…
According to CDC/ATSDR....
“ Any atrazine that is washed from the soil into streams and other bodies of water will stay there for a long time, because breakdown of the chemical is slow in rivers and lakes. It will also persist for a long time in groundwater.”
AND
“ One of the primary ways that atrazine can affect your health is by altering the way that the reproductive system works. …An increased risk of developing mammary tumors was observed in female rats.”

A scientist was hired by a chemical company to study its weedkiller. He found it was castrating and feminizing frogs. So the company stopped studying the chemical and started studying him. This is the documented story of atrazine. 🧵
3
411
Charlotte Kuperwasser, PhD retweeted

I’m intrigued by the numbers for hem-malignancies as we noticed that from the case reports (oncotarget.com/article/28824…) but this is a very strong signal at the population level that needs to be verified and investigated with some urgency.
@SenRonJohnson @KUPERWASSERLAB @Kevin_McKernan @DJSpeicher @RetsefL
@NIHDirector_Jay @NCIDirector @RandPaul
@HHSGov @US_FDA @kharaguchi @MaryanneDemasi
@RWMaloneMD @JanciToxDoc @danaparish
@xazalbert @JesslovesMJK @efenigson @Arightside
@Fynnderella1 @Jikkyleaks @AaronSiriSG @RobertKennedyJr @TracyBethHoeg @statnews
@TheCancerLetter

Jun 2

x.com/i/broadcasts/1dJrPPlNg…
@Shawnbuckleylaw @brownstoneinst @Kevin_McKernan @KUPERWASSERLAB @weldeiry

10
54
119
14,925
Charlotte Kuperwasser, PhD retweeted
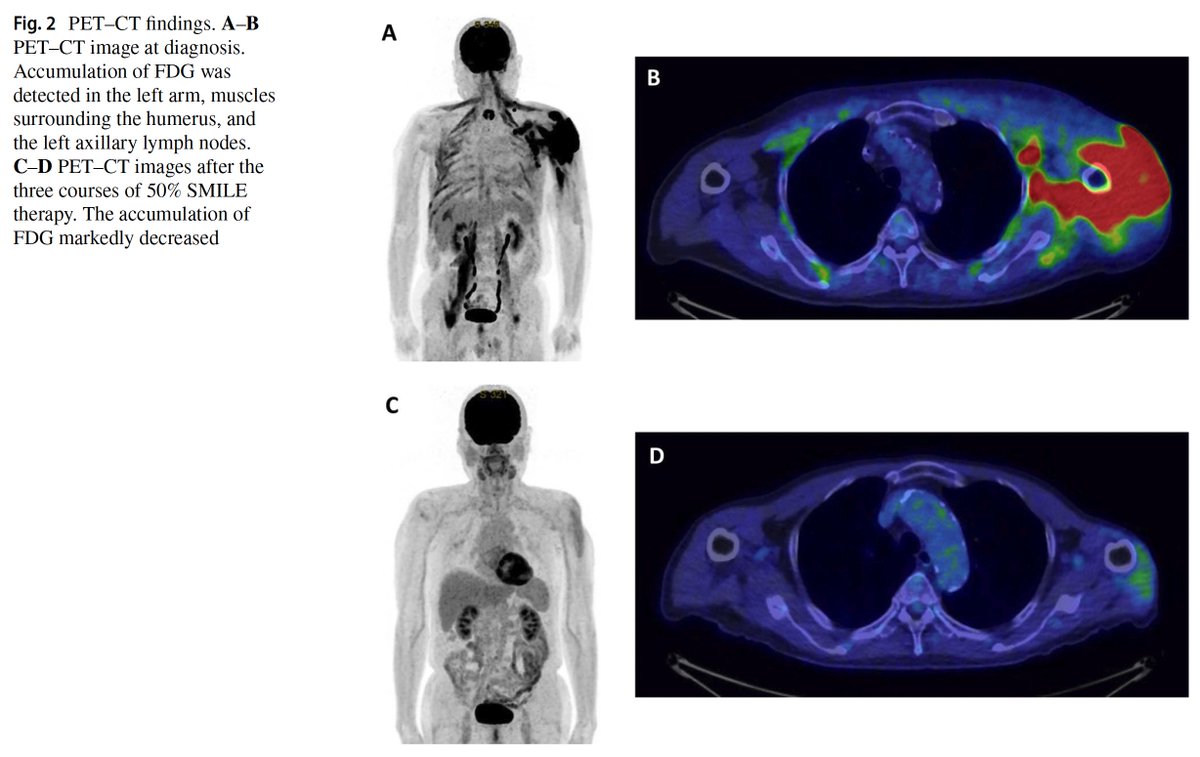
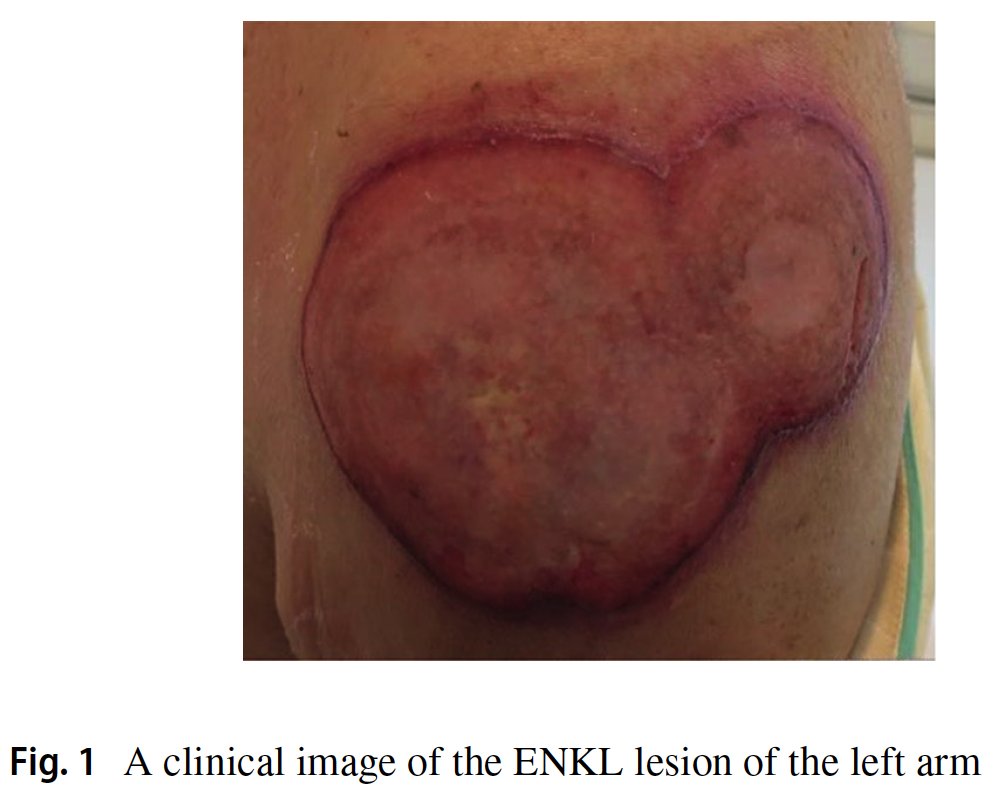
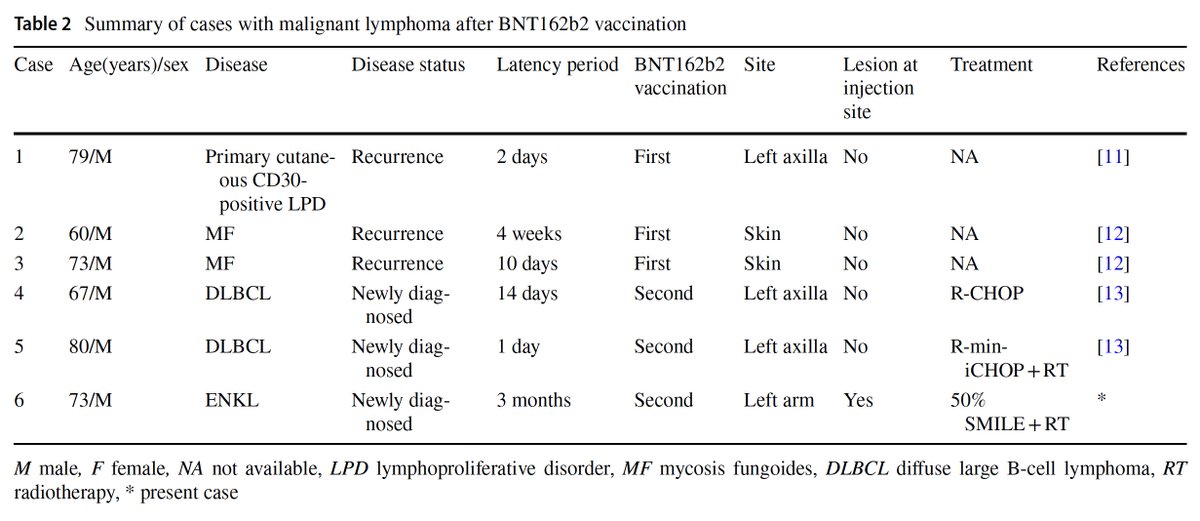
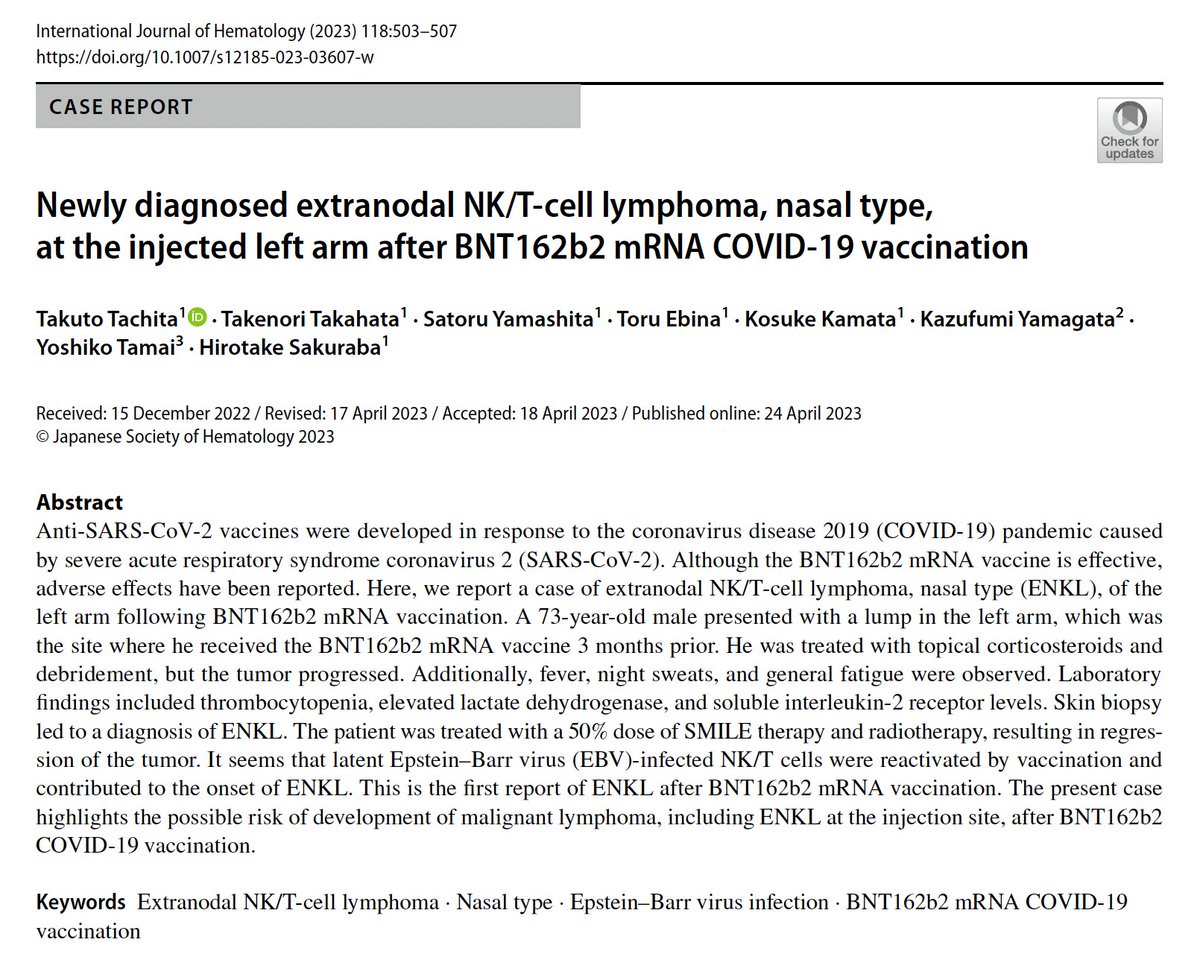
Important case of a 73 year old man with extranodal NK/T cell lymphoma at the injected left arm after BNT162b2 mRNA COVID-19 vaccination 3 months earlier. The authors described 5 other cases with recurrence of T-cell lymphoma or newly diagnosed diffuse large B-cell lymphoma (DLBCL) shortly after BNT162b2 mRNA vaccination.
link.springer.com/article/10…
8 Sep 2025

There's lots of cases reported in the literature. Causation not confirmed but the case reports haven't dug that deep. Further investigation needed.
Here's a NK/T-cell lymphoma at the injection site.
pubmed.ncbi.nlm.nih.gov/3709…

4
64
121
12,105
Charlotte Kuperwasser, PhD retweeted
Thank you @MaryanneDemasi
"It's academic terrorism," says top cancer researcher
blog.maryannedemasi.com/p/it…
@SenRonJohnson @KUPERWASSERLAB @Kevin_McKernan @DJSpeicher @RetsefL @NIHDirector_Jay @NCIDirector @RandPaul
@HHSGov @US_FDA @kharaguchi @MaryanneDemasi
@RWMaloneMD @JanciToxDoc @danaparish
@xazalbert @JesslovesMJK @efenigson @Arightside
@Fynnderella1 @Jikkyleaks @AaronSiriSG @RobertKennedyJr @TracyBethHoeg @statnews @TheCancerLetter
10
58
141
14,004
Charlotte Kuperwasser, PhD retweeted

I’m holding a hearing tomorrow at 2:30pm ET: “Plausible Mechanisms of COVID-19 Injections Causing Cancer and Attacks on Scientific Publications and Research.”
We’ll hear from 6 doctors and a cancer survivor:
- Angus Dalgleish, M.D.
- @weldeiry
- @SabinehazanMD,
- Saskia Mostert, M.D., PH.D.
- @DrAseemMalhotra
- @jrgralow
- Tamika Felder
Tune in on my X account and find more information at the link below⬇️
495
3,554
9,188
387,663
Charlotte Kuperwasser, PhD retweeted

🚨Senate hearing Wednesday, June 3, investigating link between COVID shots and cancer! 2:30PM
Led by @SenRonJohnson 🙏
67
1,039
2,536
36,639
I’m excited to participate in the #PresCancerPanel meeting on June 8–9.
This meeting will focus on modifiable risk factors for cancer & potential approaches to reduce cancer risk in the United States.
Check it out: prescancerpanel.cancer.gov/r….
1
4
892
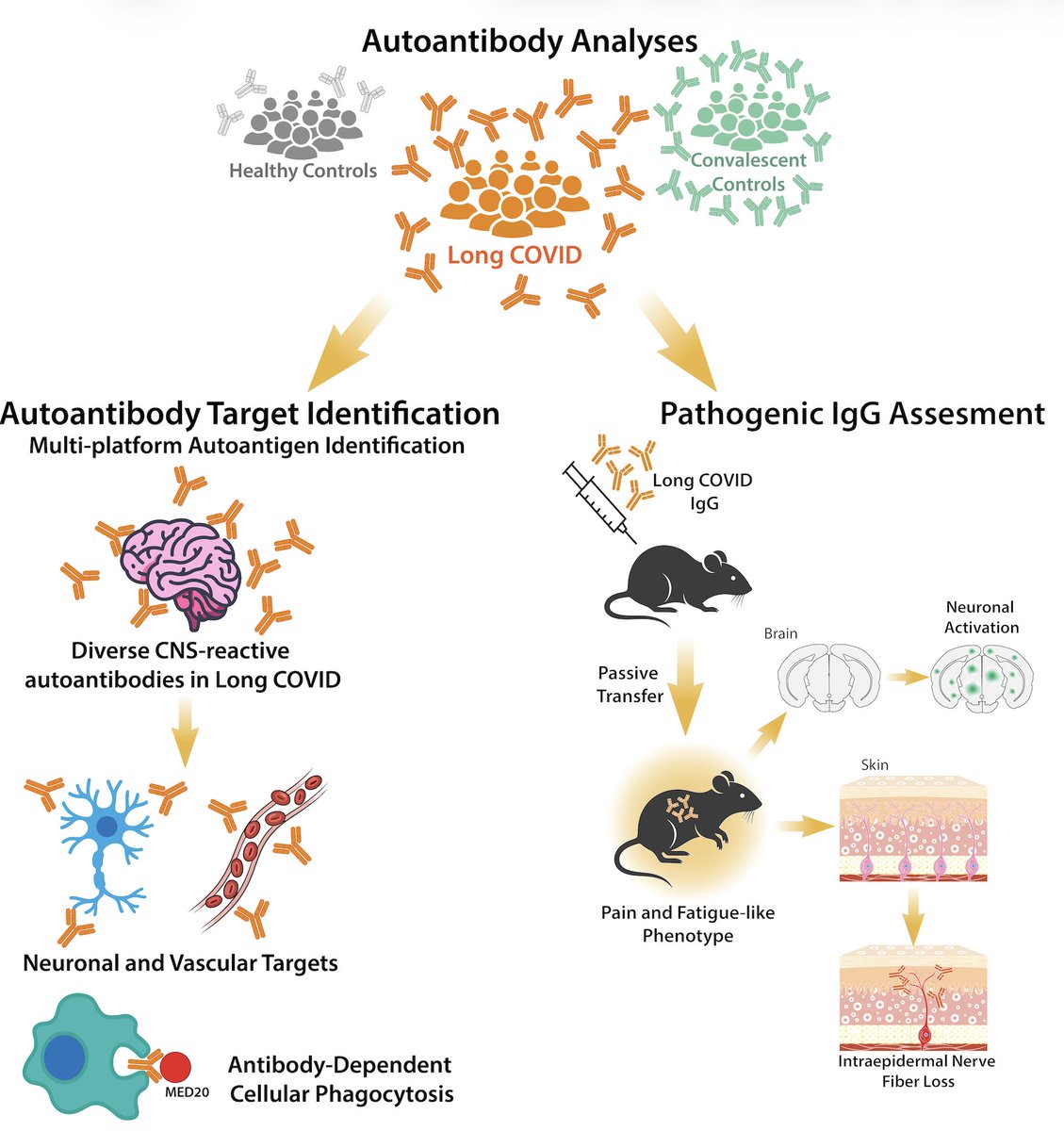
A terrific study that sheds important insights into Long Covid

Excited to share our study by @keylas3 et al. on pathological autoantibodies in people with Long COVID. We asked whether IgG in patients with Long COVID bind to human tissues/antigens and cause pathologies when transferred into mice. With @PutrinoLab
doi.org/10.1016/j.cell.2026.…
4
10
50
8,350
Charlotte Kuperwasser, PhD retweeted

🚨SPECIAL INVESTIGATION: Inside the FDA’s ‘cover-up’ over child deaths linked to Covid vaccines
Insider accounts, leaked memos and Congressional scrutiny reveal what happened behind closed doors at the FDA blog.maryannedemasi.com/p/sp…
@SenRonJohnson @SecKennedy @MartyMakary
@Kevin_McKernan @VPrasadMDMPH @TracyBethHoeg

13
120
219
24,490
Seems like an important and relevant finding….
facs.org/media-center/press-…
Primary paper here: journals.lww.com/journalacs/…
3
5
16
1,447
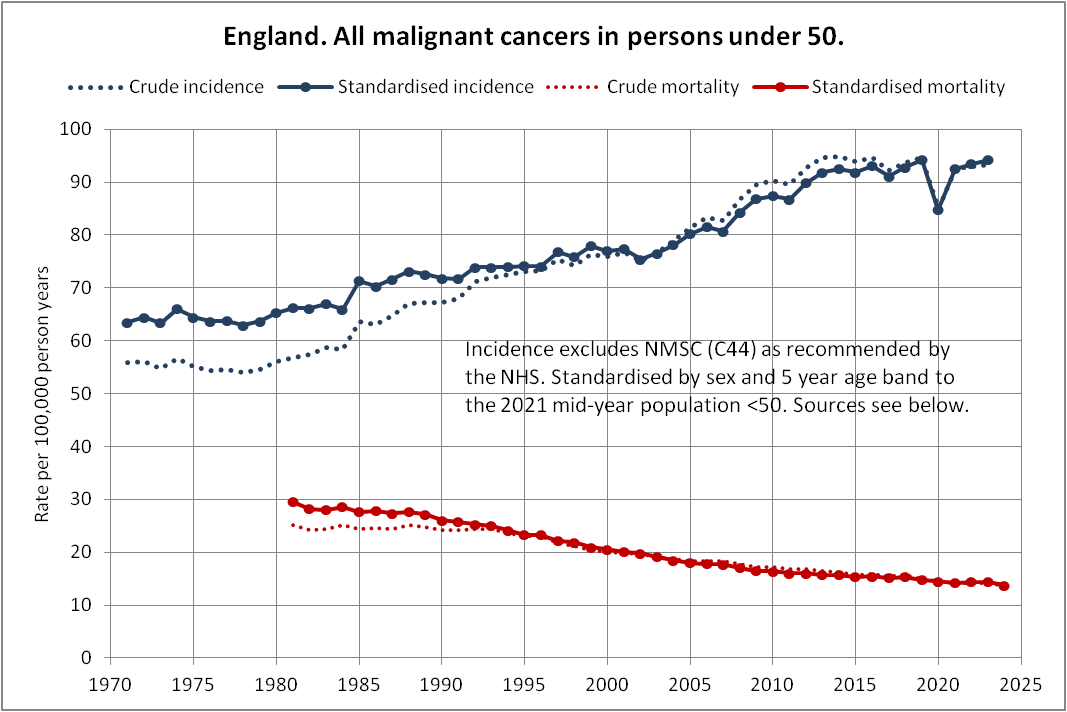
I get your point- I'm just pointing out that it is overly simplistic to keep pointing to crude population-level incidence trends which can obscure relationships because cancer is heterogeneous, latency is variable, exposures are uneven, and screening/diagnosis changes confound the signal.
Some glaring examples of this include DES and clear-cell adenocarcinoma, asbestos and mesothelioma, radon and lung cancer.
This last one is particularly relevant here because radon is known to cause lung cancer, but this signal is masked in population-level data since smoking is such a dominant risk factor and radon exposure varies dramatically by geography and by household...
May 21

My reply here:
1
2
12
1,802
That’s not my argument.
I’m not saying every cancer trend since 2020 should be attributed to COVID or COVID vaccination. I’m saying the absence of a clean, population-wide “hockey stick” across all cancers is not evidence that there is no biologically meaningful signal.
Cancer is not one disease. It is hundreds of diseases with different etiologies, latency periods, tissue susceptibilities, immune dependencies, exposure histories, and host vulnerabilities. If a signal exists, it would likely appear unevenly — in particular cancer types, in particular populations, and against already-moving background trends.
The right question is not: “Did every cancer rise everywhere after 2020?” It is are there biologically plausible, cancer-type-specific, age-specific, sex-specific, or immune-related patterns that warrant closer investigation?
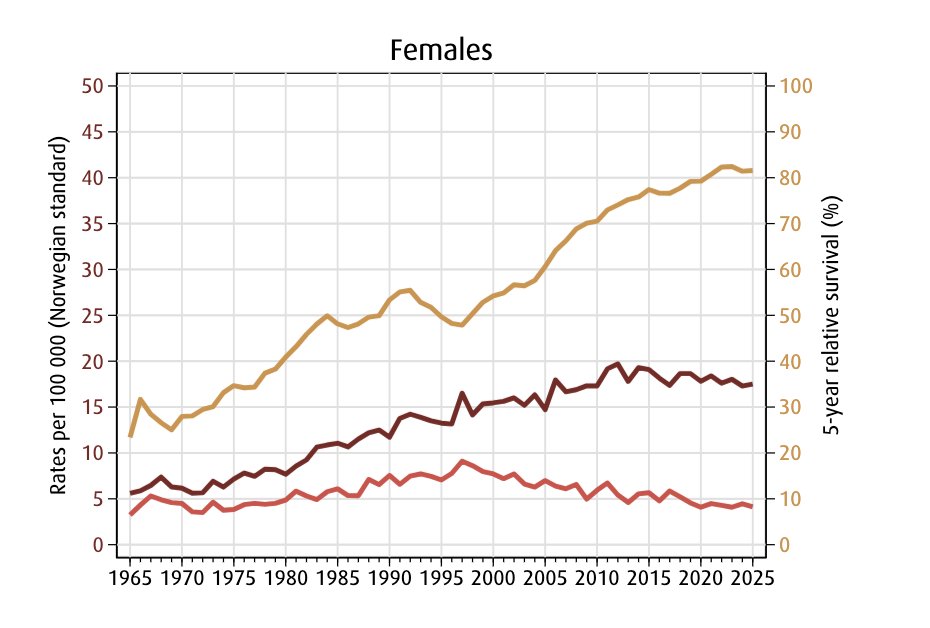
And in the Norway data for several cancers — including pancreatic, stomach, NHL, and leukemia in women — I don’t think the trends look reassuring. Some predate COVID, which makes them no less important. It may point to broader environmental, infectious exposures or immune-related pressures that we should be studying more carefully, not dismissing as “good news.”
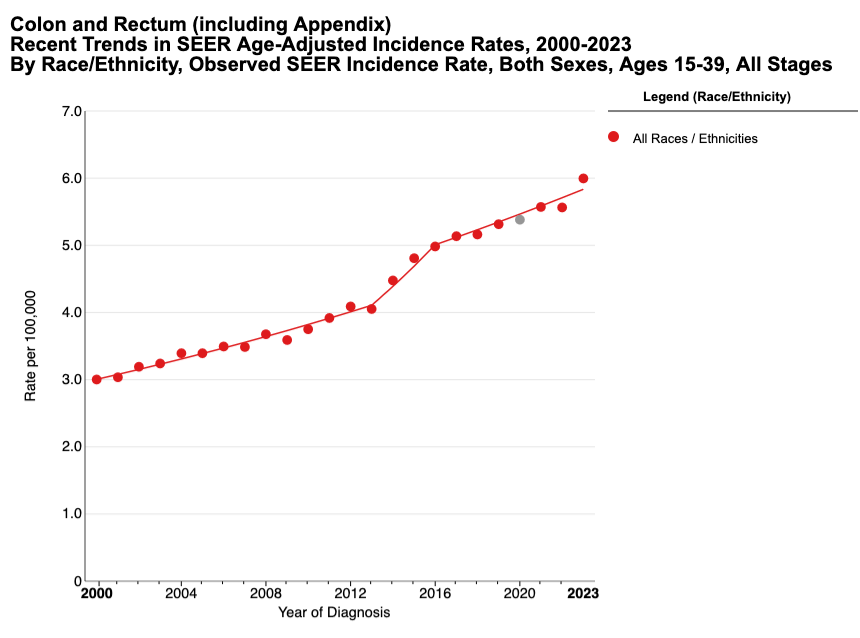
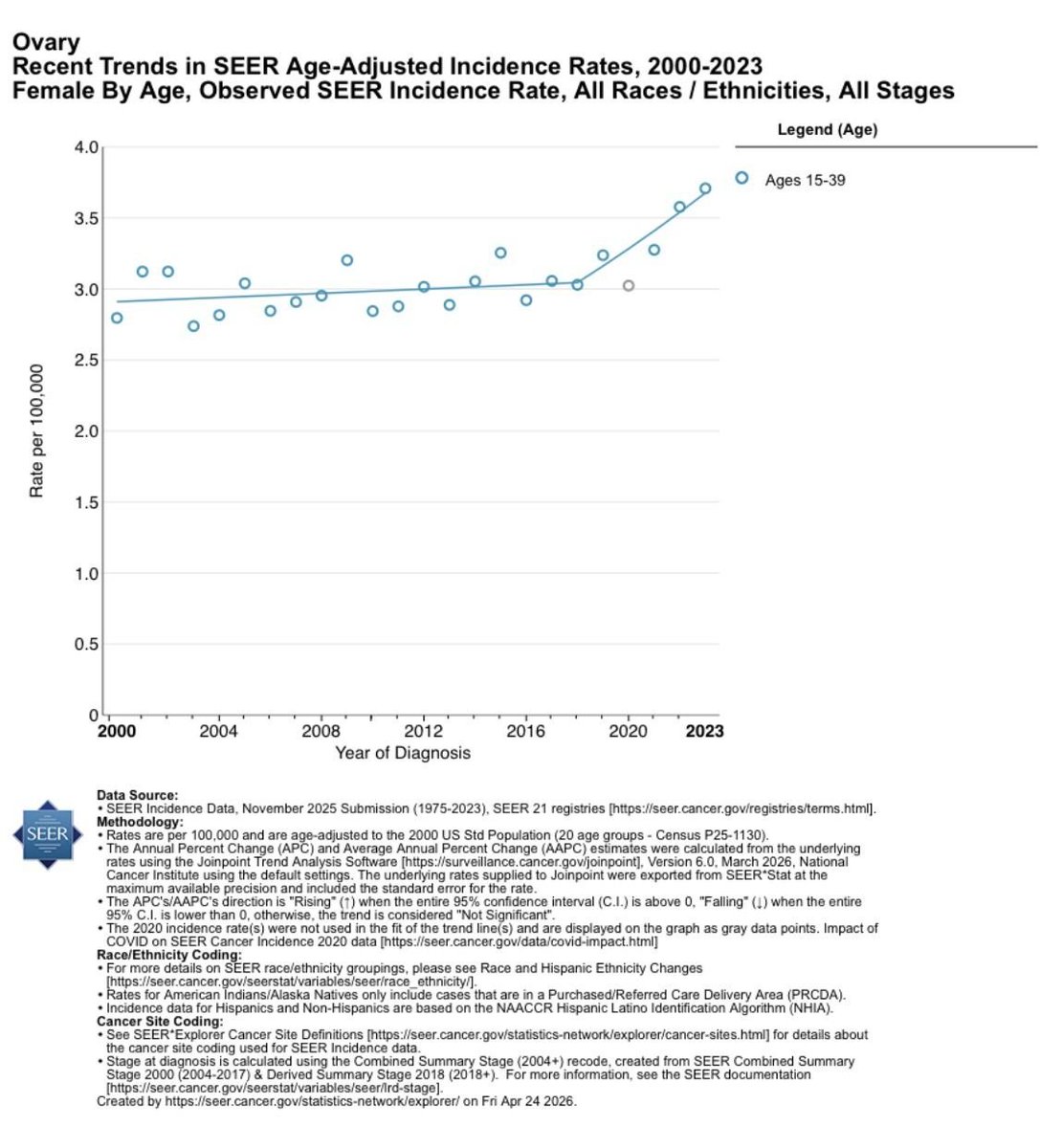
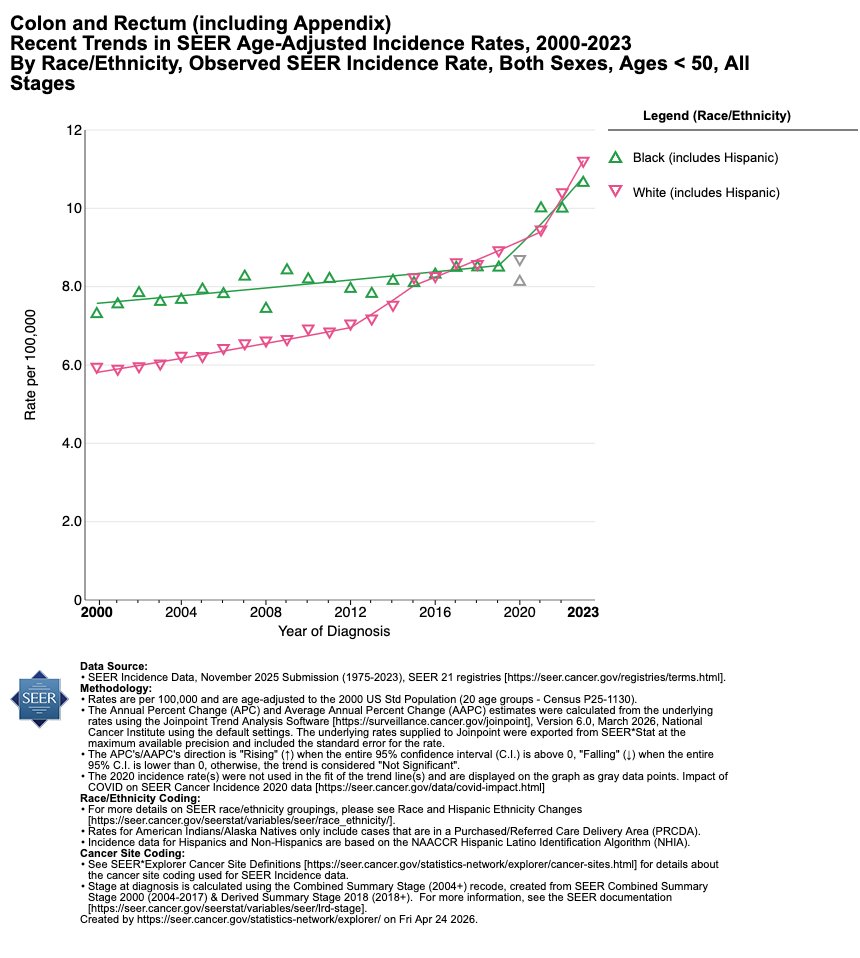
And for the US under 50 data - those trends look even more worrisome.
May 21
It's good news if you had falsely believed COVID vaccines (or COVID) led to measurable replicated rises in cancer worldwide outside of pre-existing trends.
You can always cherry-pick individual cancers that went up or down in individual countries but do we see one measurable signal? No.
Using your reasoning cervical cancer went DOWN in women since 2020 in Norway after a trend up before the pandemic. Do you credit the vaccine?
1
3
17
2,066
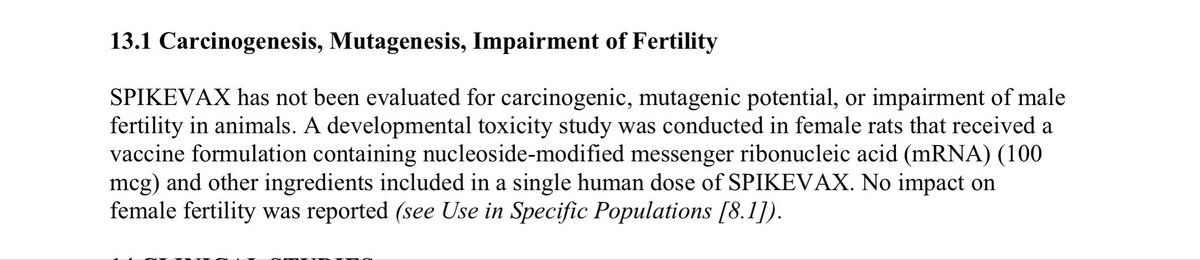
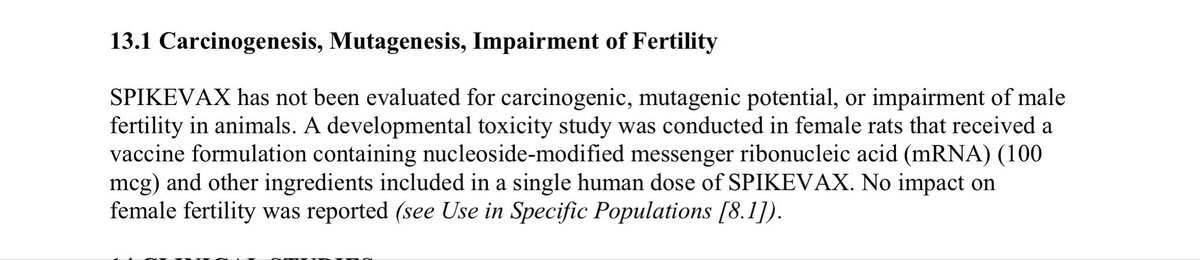
Not until regulatory guidelines are established by the FDA related to the DNA impurities that exist as part of manufacturing these products.
There still are no evidence based thresholds established for LNP- encapsulated DNA …and we still do not know the fate of the LNP-encapsulated DNA in mRNA-LNP vaccines.
Once this data has been made available then we will be in a position to prioritize and fully support this technology.
May 18

This is the kind of work, published today, that should be fully supported and prioritized at the highest level. Currently, there is no vaccine vs the Ebola Bundibugyo virus, the source of a major outbreak pnas.org/doi/10.1073/pnas.25…

2
3
11
1,431
mRNA-LNP vaccines are materially distinct from any other biologics (other than gene therapy). Even the WHO has stated mRNA vaccines need their own regulatory guidance- and they explicitly state such guidance must be established by regulatory bodies of each individual nation. Where is the FDA on this??? It’s been over 6 years…
1
1
122
💯🎯Based on their actions one would think that the FDA believes their job is to protect a public-health narrative, not to protect the public.
And it has been more than 6 years since the rollout of these products and we still do not any guidance or regulation on their manufacturing ...
May 18

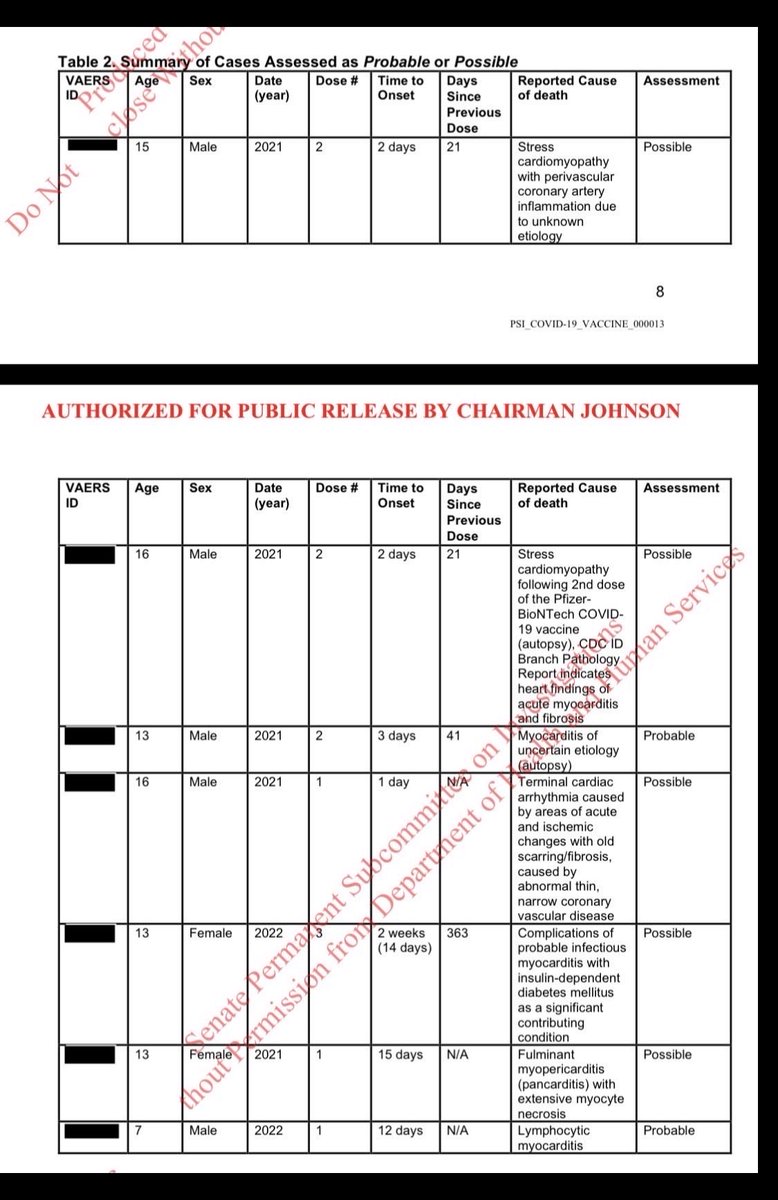
I woke up still thinking about this chart showing 7 pediatric deaths attributed as possibly or probably related to COVID vaccination in the U.S. Senate Permanent Subcommittee on Investigations release of FDA-reviewed VAERS cases.
I wonder what went into the agency’s thinking about labeling and risk communication here. The benefit-risk calculus in this age group is different and may possibly vary depending on underlying risk factors and baseline COVID risk, which is the labeled indication.
At the same time, these vaccines remain widely available in practice. So if FDA reviewers classified even a very small number of pediatric deaths as possible/probable after case-level review, why wasn’t that considered sufficient to better inform the public about a potential very rare but fatal risk?
3
10
677
This response/solution is “whack-a-mole”.
The platform was designed to induce immunity. But biology responded in an unpredictable way...vaccine protein produced by liver cells activated pathways that suppressed CD8 T-cell responses. So rather than viewing this as a potential intrinsic limitation of systemic mRNA-LNP delivery, the proposed solution is to further engineer the platform to bypass or silence the biology responsible for constraining it.
In other words, each newly discovered biological barrier becomes the next target for engineering intervention....
Shouldn't we pause for a moment and be raising the broader question of whether these are isolated obstacles, or signals of deeper platform-level incompatibilities??
May 12

A more “measured and transparent” summary of the paper that avoids some of the big extrapolations and leaps your post makes would be:
“In mice, mRNA-LNPs transfect hepatocytes, and hepatocyte expression of the encoded antigen actually suppresses the CD8 T cell response (partly via PD1/PDL1). Engineering the mRNA to silence hepatocyte expression boosted anti-tumor immunity in a mouse lymphoma model. This suggests an improvable design feature for future mRNA vaccines, particularly cancer vaccines delivered i.v., and raises questions worth investigating about whether hepatic biodistribution dampens clinical mRNA vaccine responses in humans.”
6
3
18
1,908