
Brother, husband, father, grandpa. Survivor. Now an #Aging baby-boomer, obsessed with ⬆️#Healthspan for both me & my 💰#portfolio
Joined May 2011
- Tweets 487
- Following 551
- Followers 165
- Likes 5,311
23 Photos and videos








Ron Lecours, ex-CFP retweeted

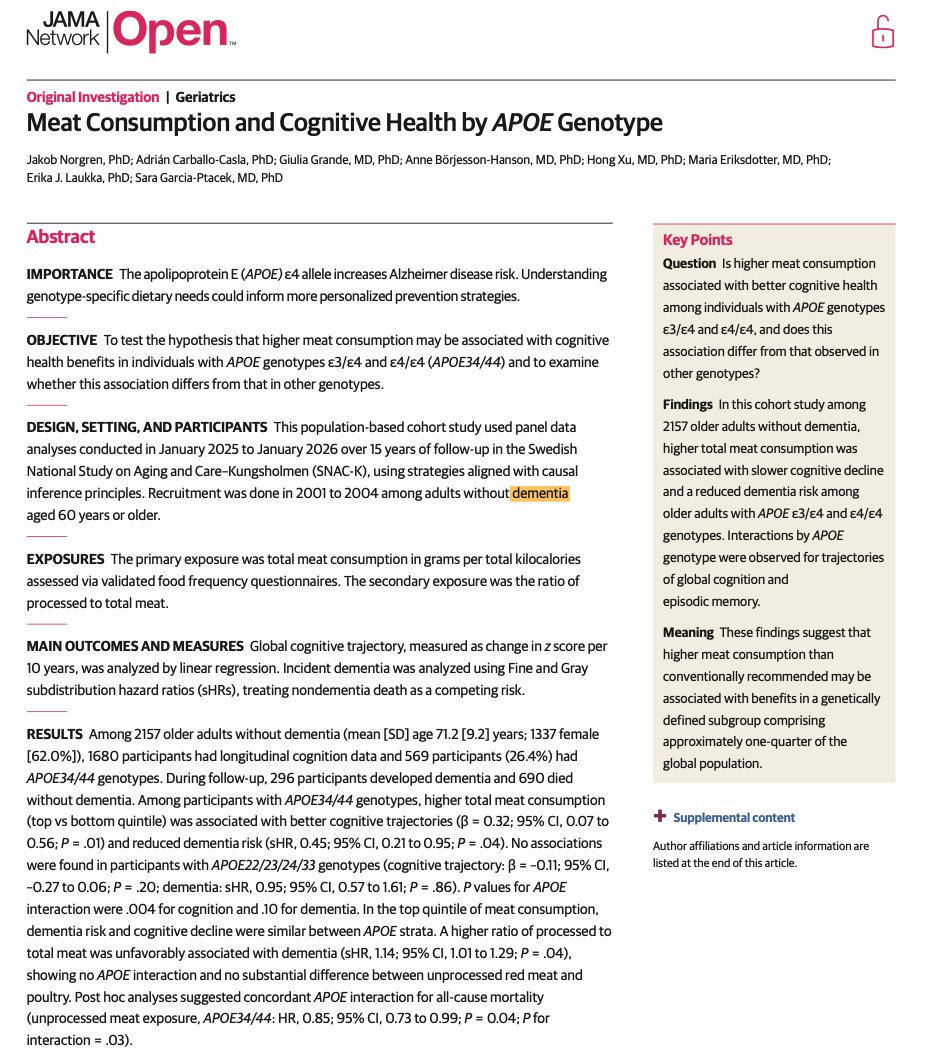
Higher meat intake was associated with less cognitive decline and lower dementia risk in APOE e4 carriers, a group at higher risk of Alzheimer's disease and dementia.
Those who ate ~2 servings of meat per day had a better 10-year cognitive trajectory and a 55% lower dementia risk compared to people eating less than a half a serving per day.
That pattern wasn't seen in the non-APOE e4 carriers and was NOT observed for processed meat. Unprocessed red meat alone was also linked to lower dementia risk in APOE e4 carriers.
My take is not “everyone should eat more meat.”
But a few servings per day of unprocessed meat (as observed in this study) is perfectly healthy for most people.

36
94
776
48,545
Ron Lecours, ex-CFP retweeted

Jun 10
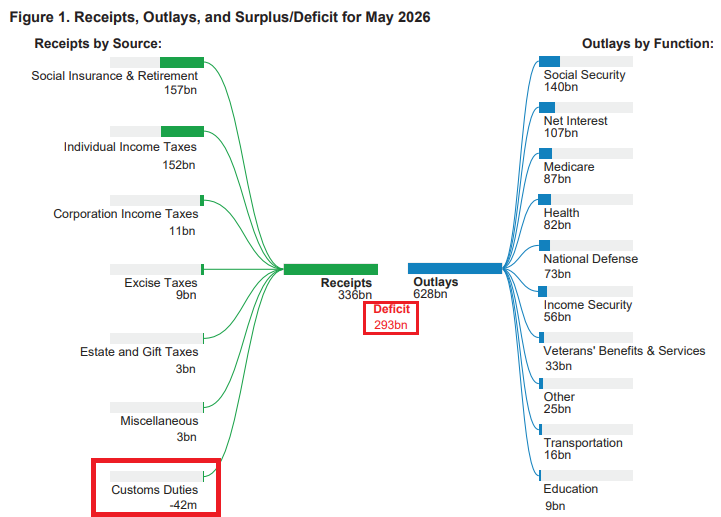
May: The Federal Government took in $336 billion and spent $628 billion. Don't try this at home.
89
333
1,234
119,363
Ron Lecours, ex-CFP retweeted

Jun 14
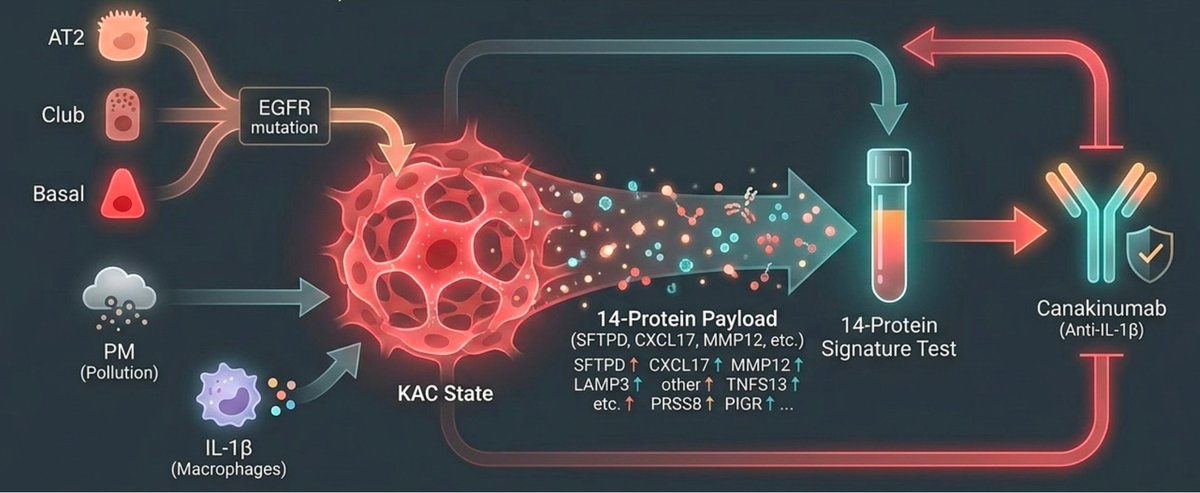
Discovery of a 14-protein biomarker that predicts lung cancer 5.6 years before it is diagnosed, even in non-smokers, and an anti-inflammatory medicine that prevents its progression. And, challenging dogma, the proteins are not coming from cancerous cells!
35
532
2,408
143,540
Ron Lecours, ex-CFP retweeted

Jun 11
Be forgiving with your past self. What's done is done. No sense in beating yourself up about it.
Be strict with your present self. Win the moment in front of you right now.
Be flexible with your future self. There are many paths to success. You don't need life to be a certain way to live well.
101
728
4,644
121,631

Ron Lecours, ex-CFP retweeted

May 29
From a population health perspective... What’s the single most important variable when it comes to exercise for healthspan?
I write a lot about specific workouts... HIIT vs zone 2, power vs strength, how long, how often, or how hard. And to be fair, once you’re in the game, those variables matter.
But…
The single biggest factor in whether exercise improves your health is the decision to do something rather than nothing.
At the population level, the data is so strong it’s almost silly. Going from nothing to something is where the biggest bang for your buck comes from.
-Move daily
-Occasionally walk fast
-Lift heavy things a few times a week.
That's where the massive health gains lie. Not in the optimization, or in the perfect program.
It’s all about showing up.
Everything I write about after that is fine-tuning. Don’t get me wrong… It’s important fine-tuning— but fine-tuning nonetheless.
The gap between doing nothing and doing something is a canyon. The gap between a good program and a perfect one is a crack in the sidewalk.
Sweating the details keeps too many on the couch… let’s focus on getting off the couch first.
20
34
241
24,688
Ron Lecours, ex-CFP retweeted

May 28
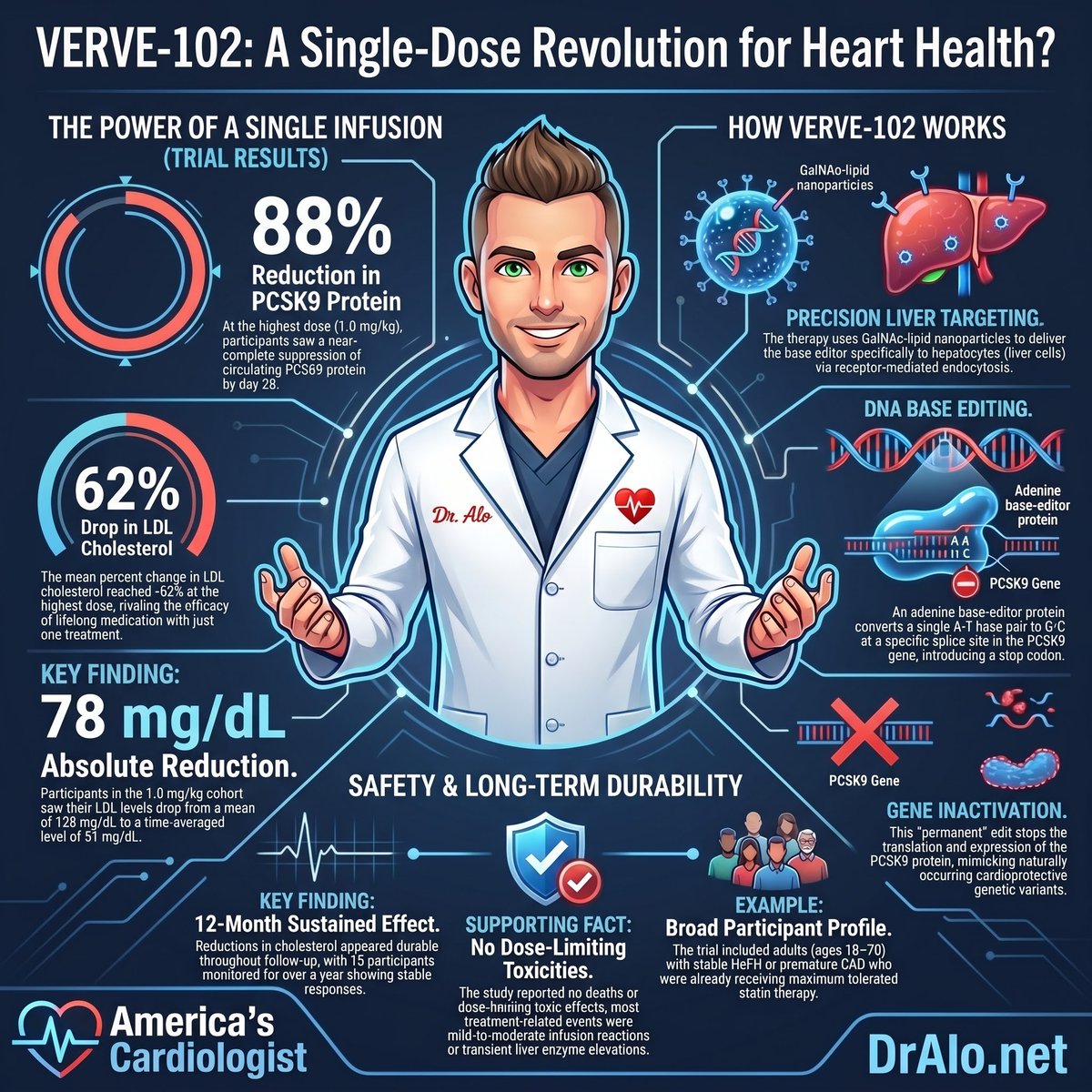
🚨 A single IV injection permanently lowered LDL cholesterol by 62%. No daily pills. No biweekly injections. No adherence problem.
One shot. Done.
But this is not science fiction. This is published data in the New England Journal of Medicine.
I am a cardiologist who has watched patients fail cholesterol therapy not because the drugs don't work, but because life gets in the way. Missed doses. Insurance gaps. Injection fatigue. That is the adherence problem medicine has never solved. Until now.
💓 Here is what the science actually says.
The HEART-2 Trial (VERVE-102) published Phase 1 results on May 25, 2026. A single intravenous infusion of VERVE-102 used base-editing technology to permanently inactivate the PCSK9 gene inside liver cells.
✅ HEART-2 (VERVE-102): LDL cholesterol reduced 62% from a single dose.
That is not a typo. One treatment. Permanent gene-level change.
🔬 Here is the mechanism and why it matters.
PCSK9 is the protein that destroys LDL receptors in your liver. When PCSK9 is active, your liver cannot clear LDL from your blood efficiently. Base editing rewrites a single letter in the PCSK9 gene at the DNA level. The liver cells stop producing PCSK9. LDL receptors stay active. LDL drops.
This mimics what nature already proved works. Humans born with natural PCSK9 loss-of-function mutations carry lifetime LDL levels that run dramatically lower than average, and they show 88% reduction in coronary artery disease risk over a lifetime.
VERVE-102 engineers that same protection into adults who were not born with it.
⚠️ This is still Phase 1 data.
Phase 1 trials establish safety and dosing. The 62% LDL reduction is real and it is remarkable. Long-term cardiovascular outcomes data is not yet available. Off-target editing effects require continued surveillance. This therapy is not approved and is not in clinical use today. But the signal is strong enough that every cardiologist needs to pay attention right now.
🩺 Why PCSK9 Is The Right Target.
PCSK9 inhibitors already have the cardiovascular outcome data. FOURIER (evolocumab) showed 15% reduction in major cardiovascular events. ODYSSEY OUTCOMES (alirocumab) showed 15% reduction in cardiovascular death, heart attack, and stroke. The biology is validated. The target is proven. VERVE-102 goes one step further and eliminates the target permanently at the genetic level.
A patient who takes VERVE-102 once does not need to remember a pill tomorrow. They do not need a refill. They do not need a prior authorization renewal. They do not need a nurse to administer a monthly injection. That is the difference between 62% LDL reduction maintained for a lifetime and 30% LDL reduction that disappears when adherence breaks down.
❤️ Bottom line:
This is not a supplement. It is not a biohack. It is peer-reviewed, gene-level cardiovascular medicine published in the New England Journal of Medicine.
Natural PCSK9 loss-of-function mutations reduce lifetime coronary artery disease risk by 88%. VERVE-102 engineers that same biological state with a single IV dose and produced 62% LDL reduction in Phase 1.
The question is no longer whether gene editing can lower LDL. The question is how fast we can get outcome data and get this therapy to the patients who need it most.
Watch HEART-2 closely. This trial could redefine preventive cardiology for the next generation.
#Cardiology #HeartDisease #HeartHealth #CardiovascularHealth #CRISPR #GeneEditing #PCSK9 #LDLCholesterol #PreventiveCardiology #CardiovascularMedicine
5
6
20
2,393
Ron Lecours, ex-CFP retweeted

AvivRoy continues out out informative, clear and concise posts.
I urge you to follow.

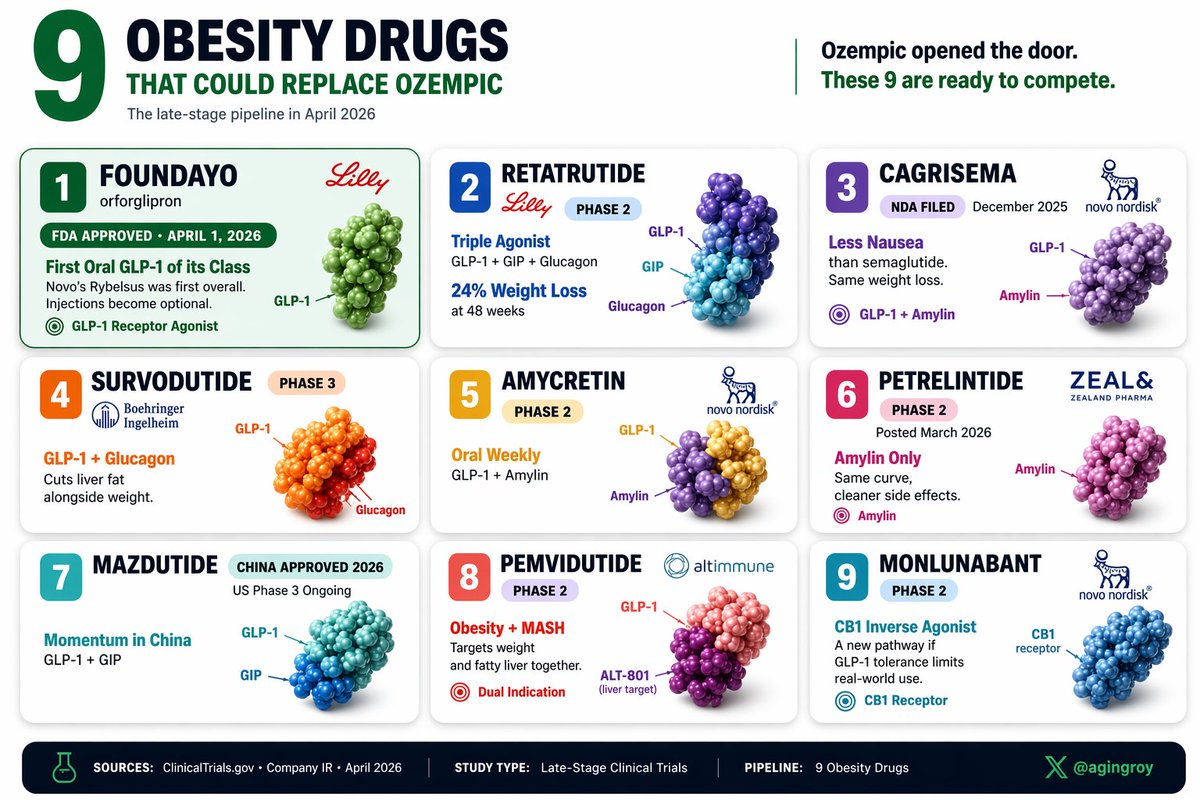
3 years ago, the obesity drug market was basically Ozempic.
Today, it's 9 drugs deep in late-stage. Here's what each one actually adds:
1. Foundayo: latest oral GLP-1. @US_FDA approved April 1, 2026. Injections become optional.
2. Retatrutide: 24% weight loss at 48 weeks (Phase 2). Triple agonist.
3. CagriSema: less nausea than semaglutide. NDA filed December 2025.
4. Survodutide: GLP-1 glucagon. Cuts liver fat alongside weight.
5. Amycretin: oral weekly. GLP-1 amylin. Phase 2.
6. Petrelintide: amylin only. Phase 2 posted March 2026.
7. Mazdutide: China approved 2026. US Phase 3 ongoing.
8. Pemvidutide: obesity MASH dual indication.
9. Monlunabant: CB1 inverse agonist. Phase 2.
The next pharma cycle may not be Novo vs Lilly. It's shaping up as mechanism vs mechanism.
2
2
17
2,432
Ron Lecours, ex-CFP retweeted
May 22
🚨 The 2026 ADA and NICE guidelines now agree on something that would have been unthinkable five years ago.
GLP-1 receptor agonists and SGLT2 inhibitors belong at the front of type 2 diabetes care.
Not as add-ons. As the foundation.
And no, this is not just about lowering blood sugar anymore.
I am a cardiologist. I treat the complications that happen when diabetes goes uncontrolled or undertreated for years. I have seen what late-stage cardiovascular disease looks like in a diabetic patient who spent a decade on metformin alone while their arteries silently failed.
That era is over. Here is what the science actually says.
💓 Why the guidelines changed
The cardiovascular outcomes trials forced this shift. The data became impossible to ignore.
✅ EMPA-REG OUTCOME (empagliflozin): cardiovascular death reduced 38%
✅ LEADER (liraglutide): major adverse cardiovascular events reduced 13%
✅ SUSTAIN-6 (semaglutide): cardiovascular death, nonfatal MI, and nonfatal stroke reduced 26%
✅ DAPA-HF (dapagliflozin): cardiovascular death or worsening heart failure reduced 26%
✅ CANVAS (canagliflozin): major adverse cardiovascular events reduced 14%
These trials enrolled more than 60,000 patients combined. That is not a signal. That is a verdict.
🔬 What these drugs actually do
. Reduce visceral adiposity
. Lower intraglomerular pressure and protect the kidneys
. Reduce systemic inflammation
. Decrease cardiac preload and afterload
. Promote natriuresis and reduce heart failure hospitalizations
. Lower HbA1c, body weight, and blood pressure simultaneously
That matters because no prior diabetes drug class did all of this at once.
⚠️ Where ADA and NICE still differ
The 2026 ADA guidelines recommend initiating GLP-1 receptor agonists or SGLT2 inhibitors based on cardiovascular and renal risk profile, independent of HbA1c thresholds.
NICE in 2026 still places stronger emphasis on cost-effectiveness thresholds and requires more documented comorbidity burden before first-line authorization in some patient groups.
The clinical intent is converging. The implementation pathways still diverge by geography and health system.
🔸 This creates a real problem for patients.
🔸 A diabetic patient in the United States with no documented cardiovascular disease may access semaglutide first-line today.
🔸 A diabetic patient in the United Kingdom with the same risk profile may wait longer due to formulary sequencing requirements.
🔸 Same evidence. Different access. Different outcomes.
🩺 What both guidelines now agree on
Both 2026 frameworks confirm the following.
Metformin is no longer the automatic first choice in patients with established cardiovascular disease, heart failure, or chronic kidney disease.
SGLT2 inhibitors are now recommended independently of glucose control in patients with heart failure with reduced ejection fraction.
GLP-1 receptor agonists are preferred in patients with obesity-driven type 2 diabetes and high atherosclerotic cardiovascular disease risk.
Combination therapy initiated early produces better organ protection than sequential add-on therapy initiated late.
A patient who starts an SGLT2 inhibitor and a GLP-1 receptor agonist early in their diabetes course can reduce their 10-year risk of hospitalization for heart failure by a clinically meaningful margin while losing 10 to 15% of body weight and lowering HbA1c by 2 to 3 percentage points.
That is the difference between managing diabetes and actually reversing its trajectory.
❌ What will not save your heart
❌ Berberine will not save you.
❌ Chromium supplements will not save you.
❌ Cinnamon extract will not save you.
The tools with the strongest data are unsexy, free, and require your participation.
❤️ Bottom line:
Type 2 diabetes treatment is no longer just glycemic management. It is cardiovascular and renal protection delivered through glucose-lowering agents.
The EMPA-REG OUTCOME, LEADER, SUSTAIN-6, DAPA-HF, and CANVAS trials changed everything. More than 60,000 patients across five landmark trials confirmed this drug class saves lives and organs.
Ask your physician whether you qualify for a GLP-1 receptor agonist or SGLT2 inhibitor today. Do not wait for your next complication. Do not accept metformin monotherapy if you carry cardiovascular risk. Understand your HbA1c, your kidney function, and your 10-year ASCVD score.
The question is no longer whether these drugs work. The question is why millions of eligible patients still do not have access to them.
Are you or someone you know with type 2 diabetes on the right therapy in 2026?
#Cardiology #HeartDisease #HeartHealth #CardiovascularHealth #Diabetes #GLP1 #SGLT2 #MetabolicHealth #PreventiveCardiology #LifestyleMedicine

5
11
31
1,794

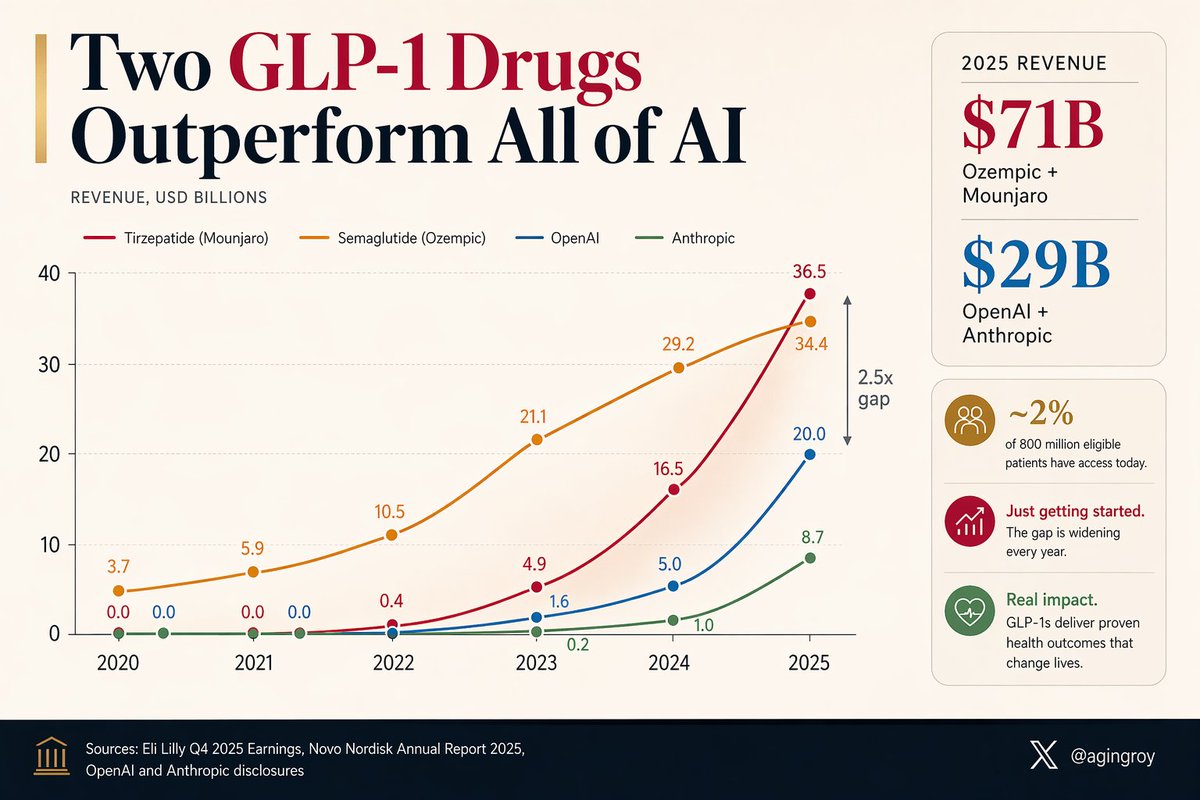
A weekly jab in the belly is generating more revenue than the entire AI industry.
Ozempic Mounjaro: $71B in 2025.
OpenAI Anthropic: $29B.
And they've barely started. ~2% of the 800 million eligible patients can currently access them.
h/t @DrSamuelBHume
57
199
1,117
548,632
Ron Lecours, ex-CFP retweeted

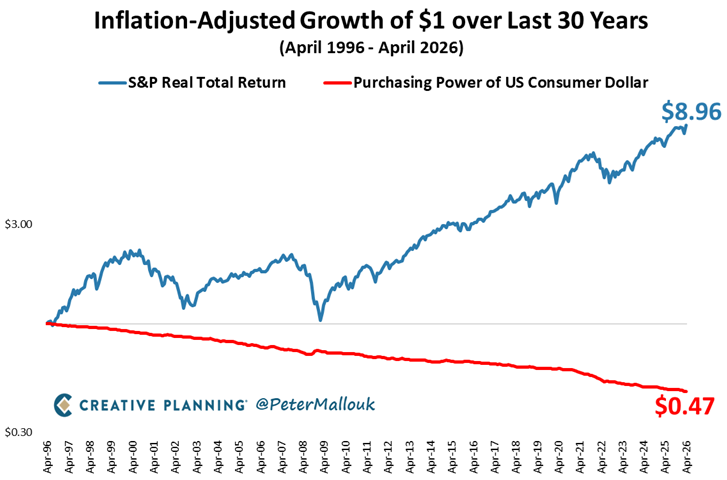
They should plaster this chart throughout hallways of American schools.
Savers lose and investors win.
166
248
1,888
134,592
Ron Lecours, ex-CFP retweeted

Apr 29
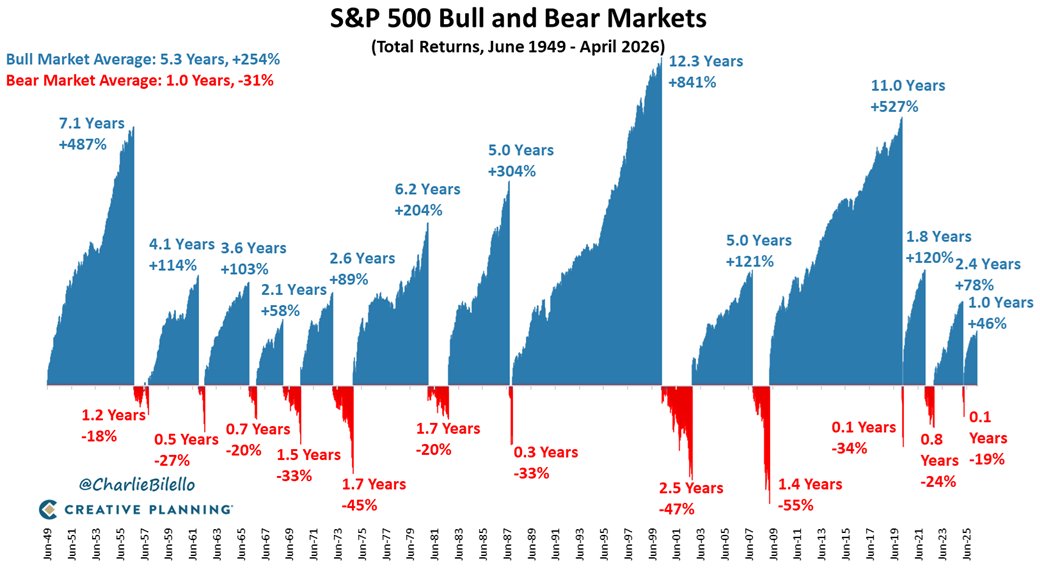
Bear markets pale in comparison to bull markets, both in market movement and duration. A good reminder for every long-term investor.
62
173
793
90,425
Ron Lecours, ex-CFP retweeted
Apr 27
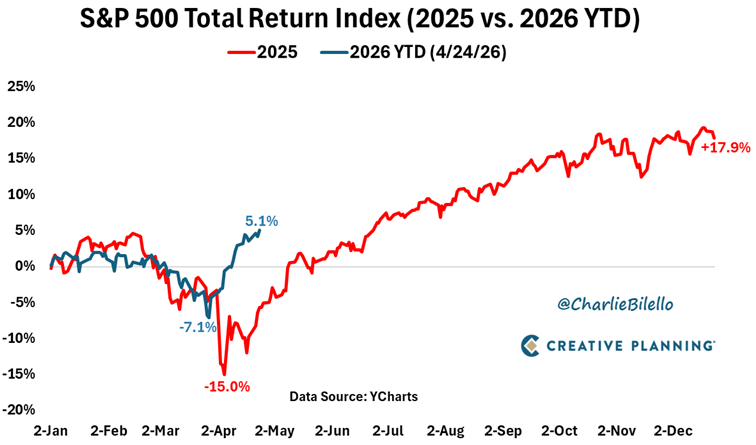
2026 is following the same playbook as 2025. Only difference is traders have become much more immune to extreme rhetoric and have been more confident in buying the dip, sending the stock market quickly back to new all-time highs. $SPX
Video: youtube.com/watch?v=p5e0ThPj…
17
34
251
41,570
Ron Lecours, ex-CFP retweeted

Apr 25
A 2025 Nature study found that lithium deficiency drives early Alzheimer's pathology—and that lithium orotate can prevent or reverse it.
Of 27 metals measured in post-mortem brain tissue, lithium was the only one showing statistically significant reductions in both mild cognitive impairment and Alzheimer's disease. The decline appeared before symptoms, suggesting lithium depletion occurs early in disease progression.
Cortical lithium levels dropped 47–52% in MCI and AD patients compared to healthy controls. Amyloid plaques sequestered lithium like charged sponges, reducing bioavailability in surrounding tissue. More plaques meant less lithium available to brain cells.
When researchers depleted dietary lithium in mice by 92%, brain lithium dropped 47–52%—matching the reduction seen in human Alzheimer's patients. The effects were immediate.
Lithium-deficient mice showed:
• 3–4x increase in amyloid-β deposition
• 3–4x increase in phosphorylated tau
• Loss of synapses, axons, and myelin
• Pro-inflammatory microglial activation
• Accelerated cognitive decline
These changes appeared within 5 weeks and worsened over 9 months. Both Alzheimer's model mice and normal aging mice developed memory deficits on lithium-deficient diets.
Lithium deficiency activated GSK-3β—a regulatory kinase that drives tau phosphorylation and amyloid-β production when overactive. Inhibiting GSK-3β reversed the damage: microglial amyloid clearance restored, tau phosphorylation reduced, oligodendrocyte function improved.
The mechanism operates through GSK-3β suppression, not inositol modulation. This distinguishes physiological lithium from psychiatric doses.
Amyloid plaques trap lithium. Standard lithium carbonate binds strongly to amyloid and becomes sequestered—unavailable to brain tissue. This creates a therapeutic problem in Alzheimer's patients.
Lithium orotate showed 3–4x less binding to amyloid-β fibrils and oligomers compared to lithium carbonate. Lower conductivity correlated with reduced plaque binding across 16 lithium salts tested.
At physiological doses (4.3 µEq/L—similar to endogenous levels), lithium orotate:
• Reduced amyloid plaque burden 60–70%
• Decreased phospho-tau 60%
• Prevented synapse loss
• Maintained myelin integrity
• Suppressed neuroinflammation
• Restored memory function
These effects occurred in both prevention trials (before pathology) and intervention trials (after established disease). Lithium carbonate at the same dose showed no benefit.
In cognitively healthy humans, higher cortical lithium levels correlated with better working memory (P=0.04), higher MMSE scores (P=0.02), and increased expression of complexin 1 and 2—synaptic proteins linked to Alzheimer's resistance.
Human trials confirm lithium engages Alzheimer's biology at sub-psychiatric doses. In Forlenza's MCI trial, lithium carbonate dosed to 0.25–0.5 mmol/L serum reduced CSF phosphorylated tau after 12 months and slowed cognitive decline versus placebo.
In a 2013 trial, Alzheimer's patients received 300 micrograms/day elemental lithium for 15 months. The lithium group remained stable on MMSE. Placebo declined from ~20 to ~14—substantial clinical progression over the same period.
Environmental lithium exposure correlates with longevity. In Oita Prefecture, Japan, tap water lithium ranged from 0.7 to 59 μg/L across 18 municipalities (~1.2 million residents). Higher lithium levels associated with lower all-cause mortality, even after adjusting for suicide rates.
In Caenorhabditis elegans, lithium exposure reduced mortality and extended lifespan up to 36%—suggesting lithium influences conserved pathways linked to stress resistance and aging across species.
Low-dose lithium targets different biology than psychiatric lithium. Psychiatric regimens deliver 150–300 mg/day elemental lithium (targeting 0.5–1.2 mmol/L serum). Low-dose approaches use ~1–10 mg/day, where serum levels run <0.2 mmol/L or "undetectable."
Dietary lithium from food and water averages ~0.5–3 mg/day, with high-lithium water regions reaching ~5 mg/day or more. This means 5–10 mg/day supplementation approximates the upper end of natural exposure—not pharmacologic dosing.
Critical intervention windows may exist in the third and fourth decades, when endogenous lithium begins declining but before pathology emerges. Maintaining physiological lithium during this period may preserve cognitive resilience.
Lithium orotate at physiological doses (4.3 µEq/L) produced no changes in kidney function, creatinine, or thyroid hormones after 12 months in aging mice—minimal toxicity compared to psychiatric doses (1,000x higher).
Disrupted lithium homeostasis is a measurable, modifiable risk factor in Alzheimer's disease. Lithium orotate at near-physiological doses may prevent or slow progression by maintaining GSK-3β regulation, synaptic integrity, and microglial function.
Formulation matters as much as dose—especially when amyloid is present. Lithium orotate was the only salt among 16 tested that avoided plaque sequestration, explaining why older Alzheimer's trials using lithium carbonate produced inconsistent results.
In our Healthspan Research Review, we analyze the cellular mechanisms, human clinical data, and population evidence showing how lithium functions as a brain-relevant micronutrient—and why low-dose lithium orotate represents a distinct biological strategy from psychiatric lithium therapy.
gethealthspan.com/research/a…
2
7
41
2,383
Ron Lecours, ex-CFP retweeted

What can physicians do to promote healthy, life-extending lifestyle changes? see.nf/4lM6dxT

5
11
44
1,987
Ron Lecours, ex-CFP retweeted

Apr 2
The problem with buying core equity index funds and tilting to styles, sectors, or individual stocks, is that you can be wrong for a very long time, and when that happens, you’ll go to the next shiny thing trying to find alpha, which will also eventually stop working. The process
7
4
67
16,520
Ron Lecours, ex-CFP retweeted

Apr 21
Just 9 minutes a day of short, vigorous activity could cut your risk of dying from cancer, heart disease, or any cause by 40-50%
No gym
No weights
Just short bursts of vigorous movement sprinkled throughout the day
That’s enough to meaningfully move the needle on longevity
9
59
661
27,334
Ron Lecours, ex-CFP retweeted

RFK Jr: "I had a full-body MRI a year ago and I went to this doctor who said my organs were covered with visceral fat. I went on his diet, which is the carnivore diet... Thirty days later I had lost 40% of it."
47
297
4,360
379,906
Ron Lecours, ex-CFP retweeted
Apr 16
Another year of training... what worked, what didn't, what had to change... A thread.
Last year, I wrote the most detailed account I've ever published of how I train at 62. Well.. I'm turning 63 — now an update: what held, what broke, what surprised me, and the annoying realities of being an aging athlete.

26
9
357
38,139
Ron Lecours, ex-CFP retweeted

Apr 12
It's a worry
Apr 11

Will our increasing longevity
be enough to save us from
our decreasing fertility?

20
12
222
30,823