
We help community oncologists stay ahead of breakthroughs that change care - without drowning in promo noise or info overload | Shruti Agarwal | #OncTwitter
Joined November 2023
- Tweets 2,216
- Following 3,536
- Followers 10,188
- Likes 2,351
62 Photos and videos









Together4Cancer retweeted
Quad induction for all, including in many aged > 80 with steroid-sparing approach!
Deciding on myeloma induction now based on whether/not pt may receive ASCT later always felt like putting cart before 🐎…
With new approvals, thankfully these #MMsm gymnastics no longer needed.

❓️ What does "transplant-ineligible" even mean anymore?
@RahulBanerjeeMD, of @fredhutch, reflects on the recent Dara-VRd approval for transplant-ineligible, newly diagnosed #myeloma and how transplant-based trials no longer match real-world care.
📖 buff.ly/eSkgUNj
1
6
21
3,182
Together4Cancer retweeted

Feb 28
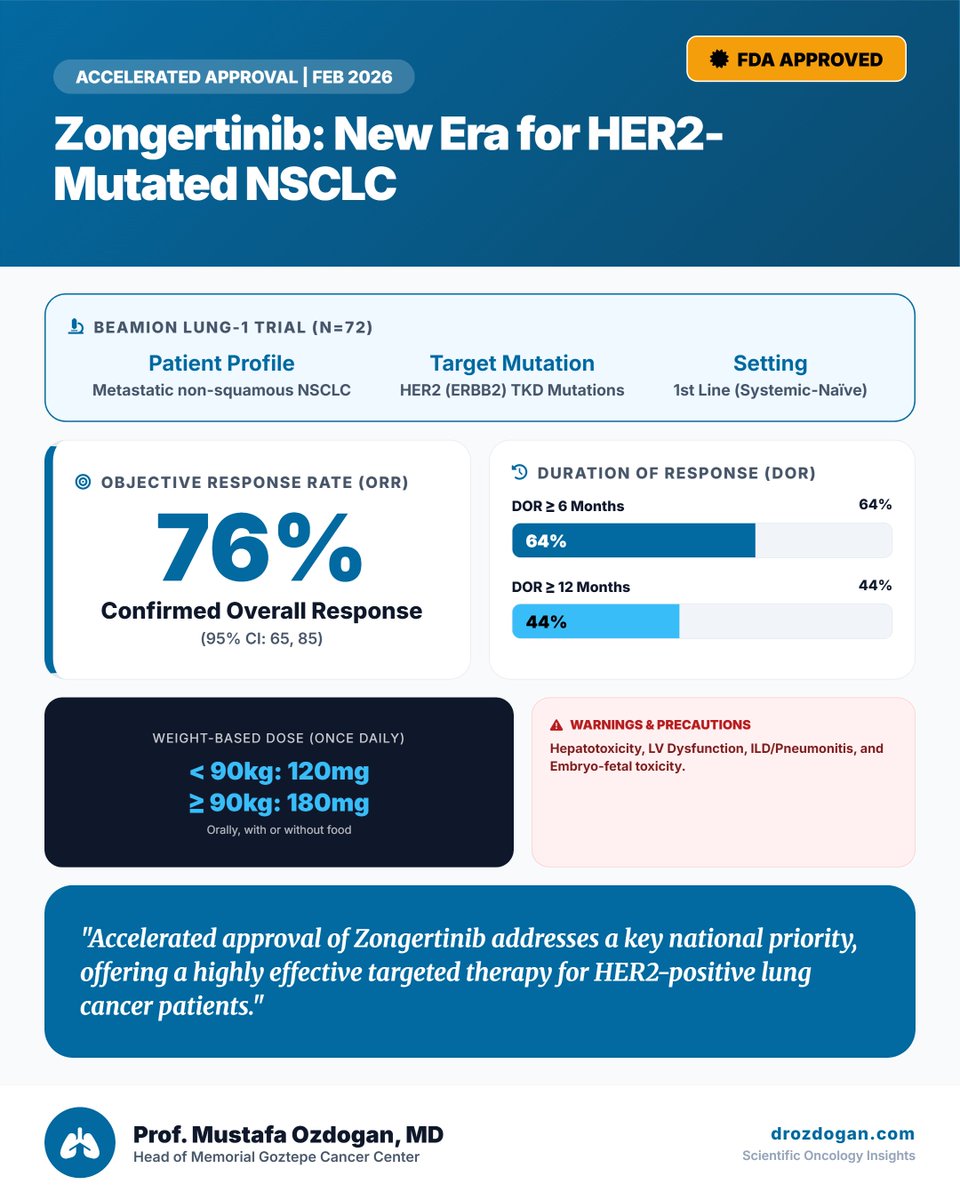
Key Highlights of Zongertinib (Hernexeos) #FDA Approval
1. First Oral Treatment Option: While previous therapies for HER2-mutant lung cancer required intravenous (IV) infusion, Zongertinib is the first FDA-approved oral (pill) treatment for this specific patient group.
2. High Target Selectivity: It is specifically designed as a "HER2-selective" TKI, meaning it targets mutated HER2 receptors without affecting other similar receptors like EGFR.
3. Improved Side Effect Profile: Thanks to its high selectivity, it avoids the severe diarrhea and skin rashes often caused by older generation drugs that also inhibited EGFR, offering a more tolerable treatment for patients.
4. Efficacy Against Brain Metastases: Zongertinib has demonstrated a significant ability to cross the blood-brain barrier, providing a breakthrough treatment option for managing brain metastases in lung cancer patients.
1
10
19
1,253
Together4Cancer retweeted
Feb 28
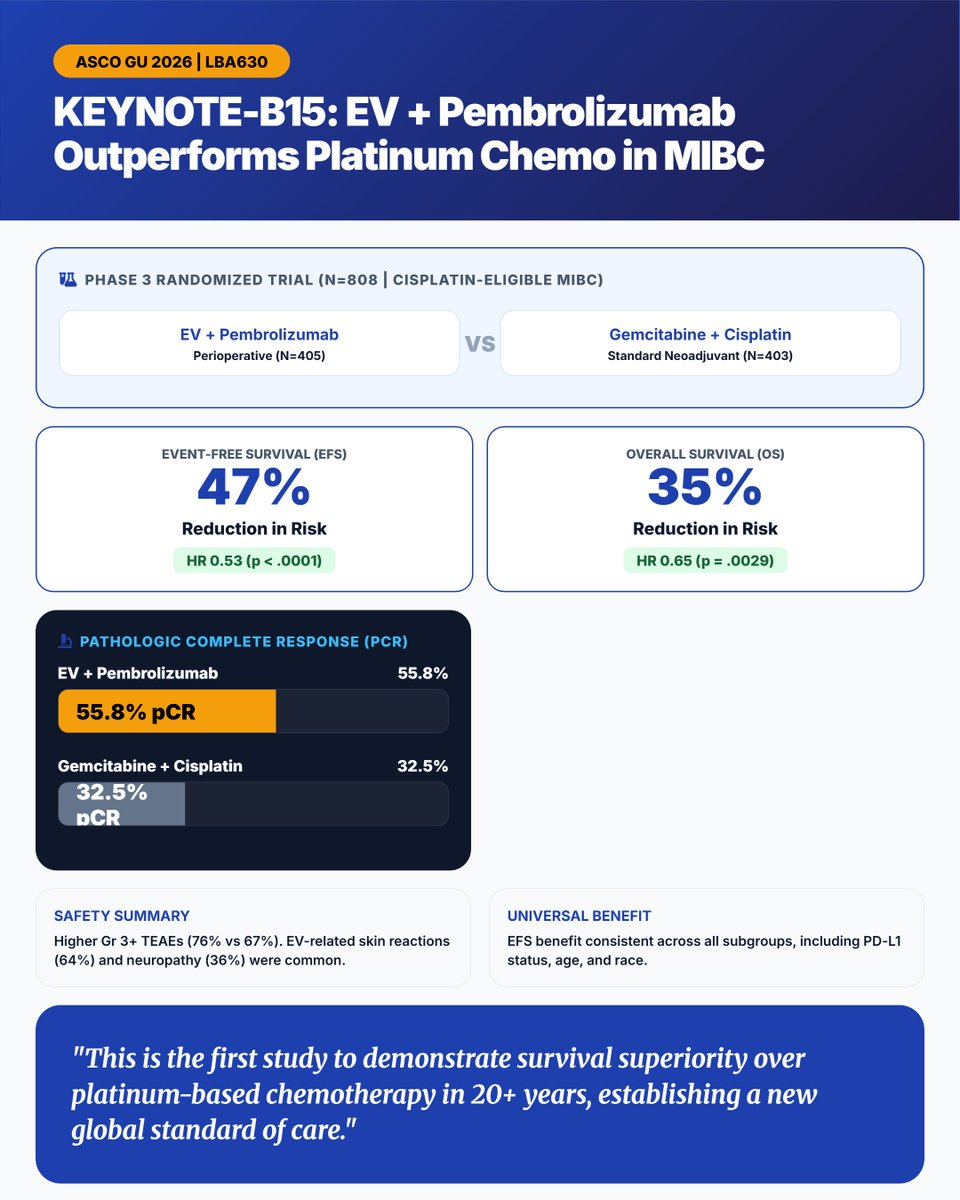
20 years in the making! #ASCOGU26 delivers a historic paradigm shift in Muscle-Invasive Bladder Cancer.
KEYNOTE-B15 (LBA630) demonstrates that perioperative EV Pembrolizumab unequivocally outperforms the platinum chemo standard in cisplatin-eligible MIBC.
A new global standard of care is officially established.
#BladderCancer #MIBC #Oncology #UroOnc #MedTwitter #ASCO @ASCO
7
14
749
Together4Cancer retweeted

Feb 27
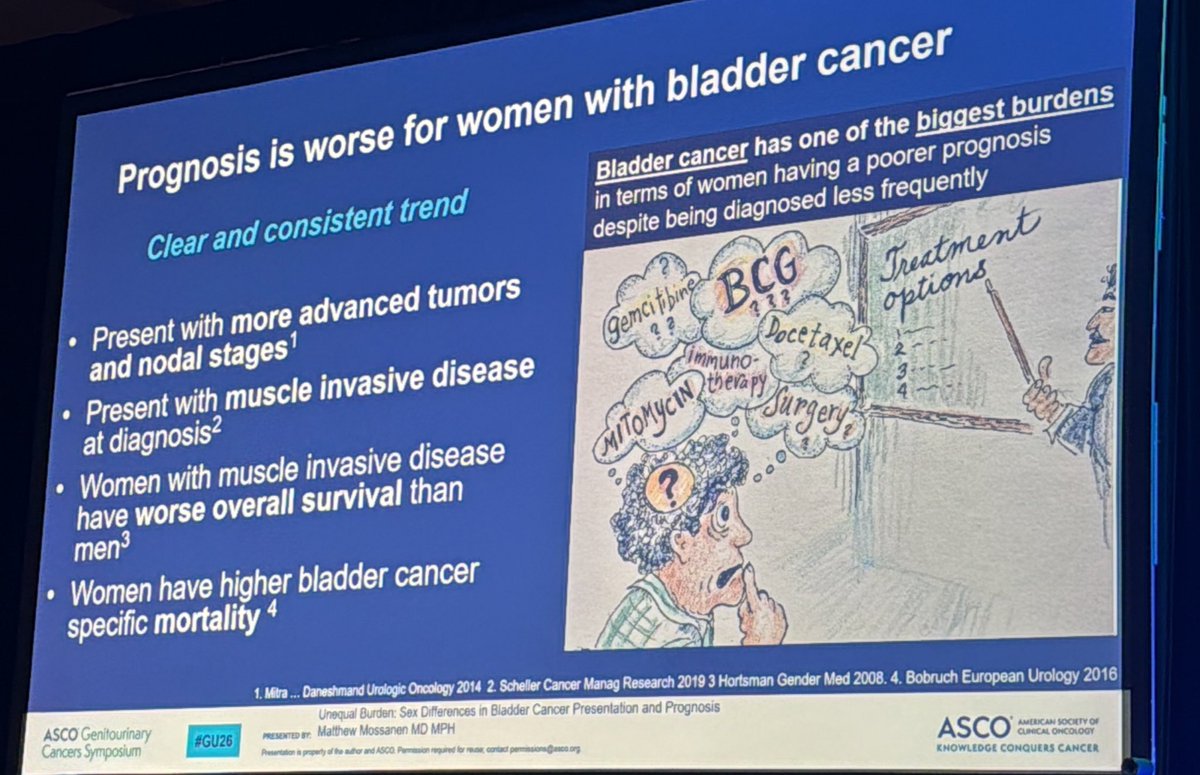
Our own @MattMossanen at #GU26 @ASCO , discussing how we can support women diagnosed with bladder cancer ➡️ stop repeated UTI treatment, refer ASAP to urology for an office cystoscopy takes , it takes less than 5 minutes!!! @DanaFarber_GU @MGBUrology
1
18
45
2,884
Together4Cancer retweeted

Feb 27
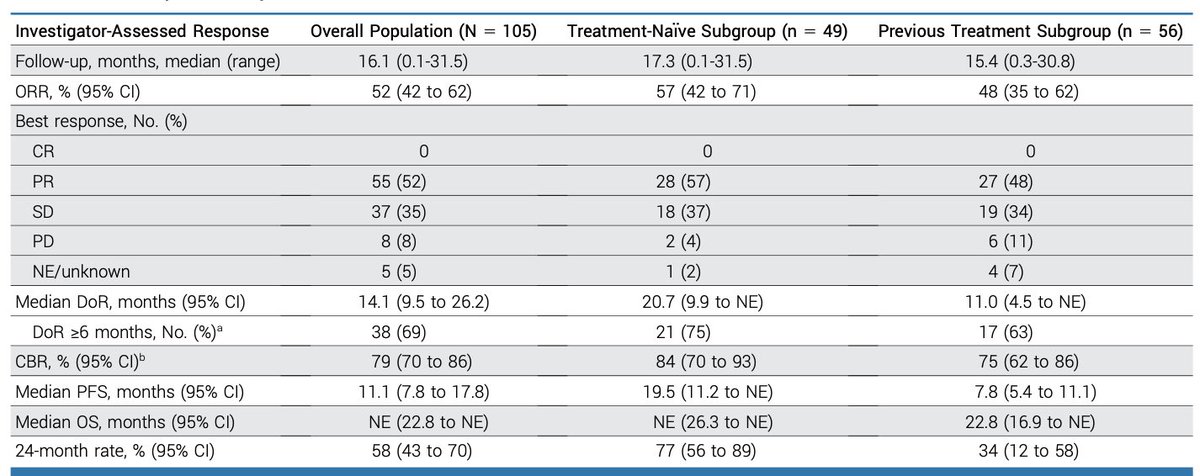
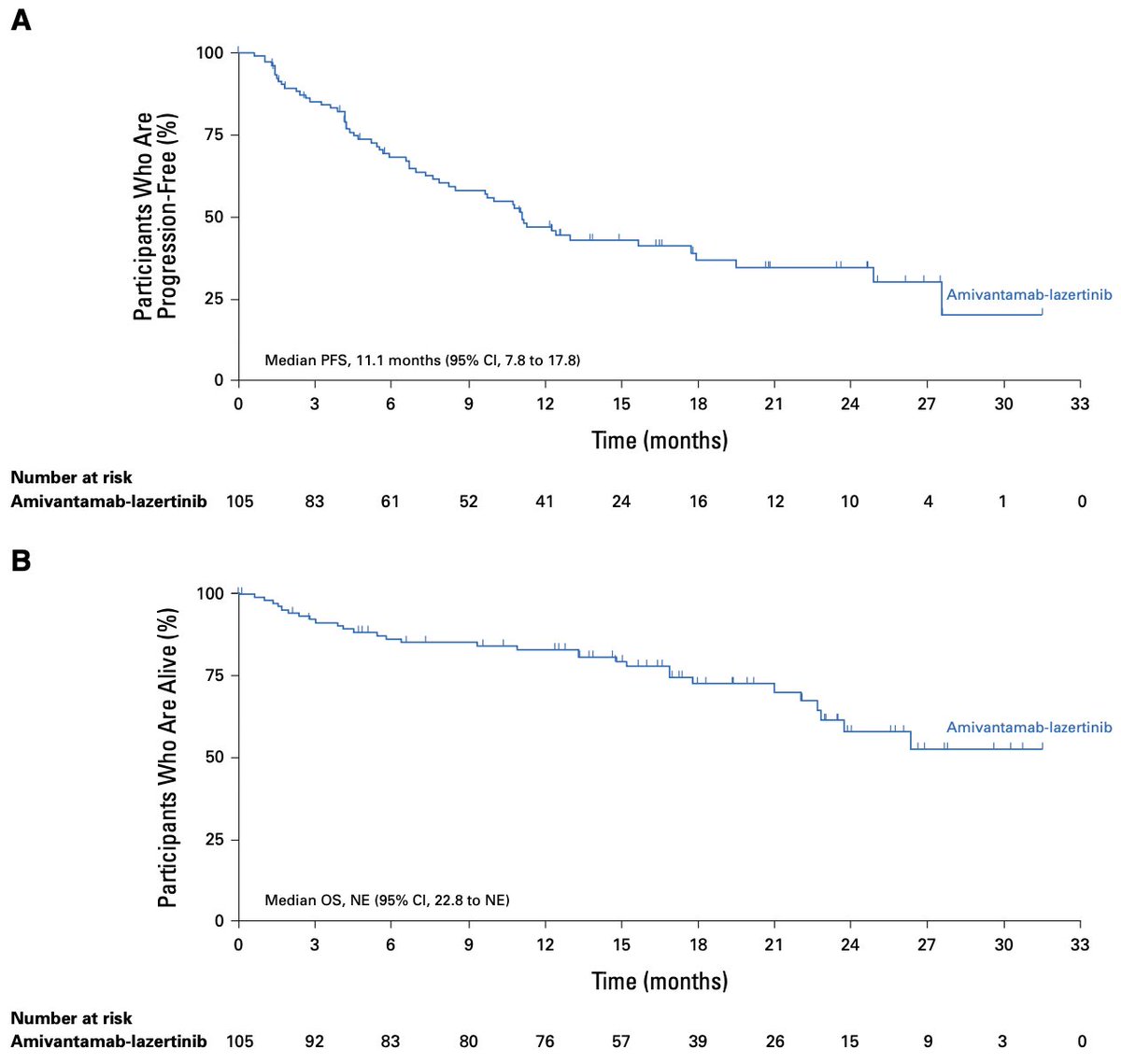
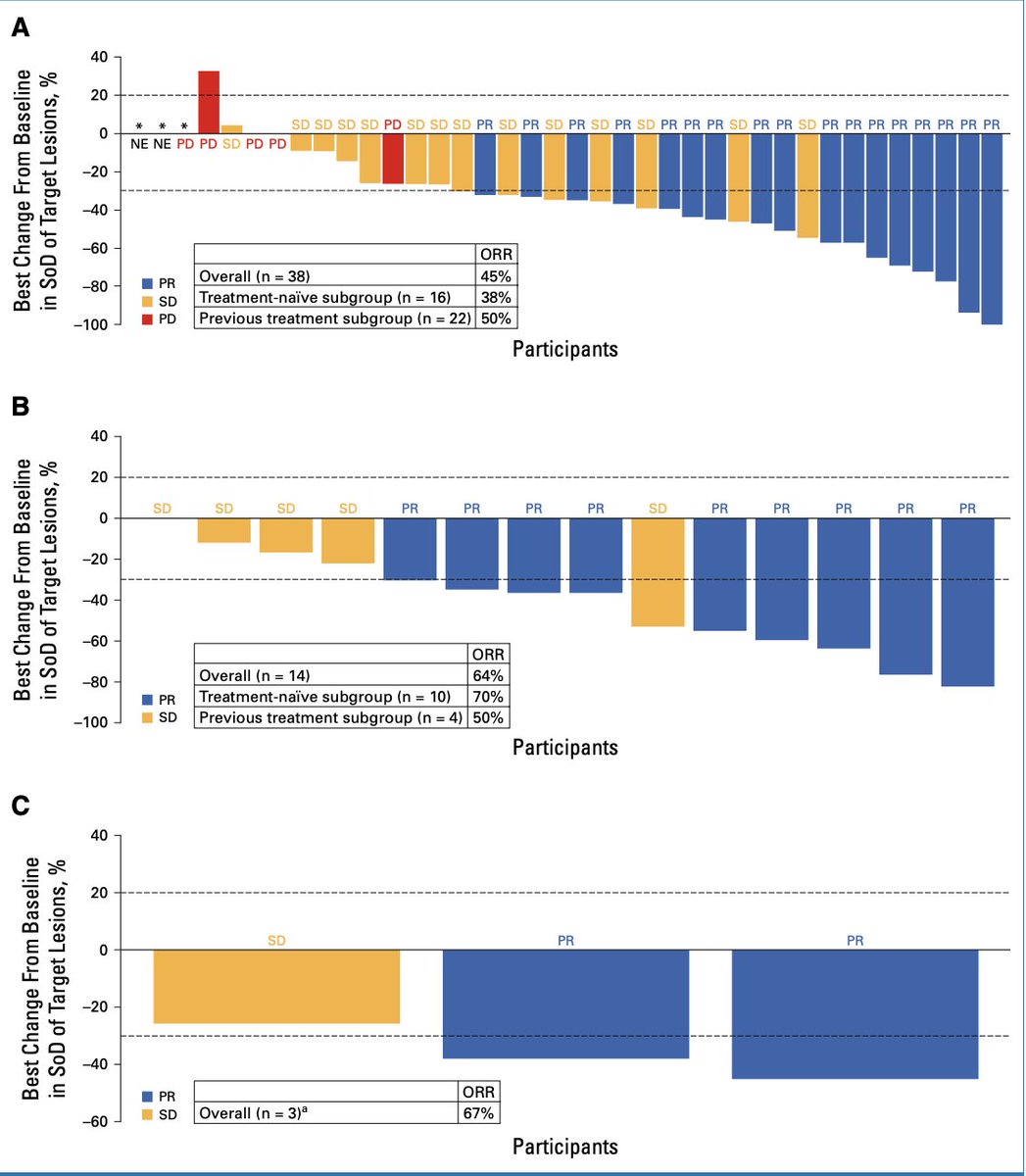
🫁 Amivantamab Lazertinib in Atypical EGFR NSCLC: CHRYSALIS-2.
In 105 pts with advanced NSCLC harboring atypical EGFR mutations (G719X, L861Q, S768I), Amivantamab Lazertinib achieved:
• ORR 52%
• mPFS 11.1 mo
• mDoR 14.1 mo
• mOS NE
Tx-naïve: ORR 57%, mPFS 19.5 mo.
Single-arm study. Meaningful activity in a historically underserved subgroup.
📖 @JCO_ASCO
doi.org/10.1200/JCO-24-02835
#CánCare #NSCLC #EGFR #TargetedTherapy #lcsm

1
18
47
2,945
Together4Cancer retweeted

Feb 25
I am reminded once again that research matters.
My wife’s friend was diagnosed with metastatic ovarian cancer, resistant to our favorite drug Cis/Carboplatin. Genetic testing revealed, among other things, KRAS G12A mutation. She was started on a KRAS inhibitor but unfortunately developed massive myopathy to the point she could barely walk. At that point, she needed bilateral nephrostomy tubes for renal blockage and was given weeks to live. But her mutation panel had also revealed modestly elevated tumor mutation burden (TMB) and CHEK2 mutation, which is involved in DNA damage response. Based on this (though the evidence was limited), she was started on immune checkpoint blockade (ICB) as a last-ditch effort. Since then, her tumors have melted away, and our friend is now strong enough to clear the snow during LAST NIGHT's blizzard in Northeast. Below is a photo she just sent us.
I share not just because this is a miracle, but a SCIENCE IN ACTION! #SpartansWill #ResearchSavesLives
@MSUMD, @MSU_Medicine, @HFH_MSU_HS

91
519
3,684
92,978
Together4Cancer retweeted

Feb 18
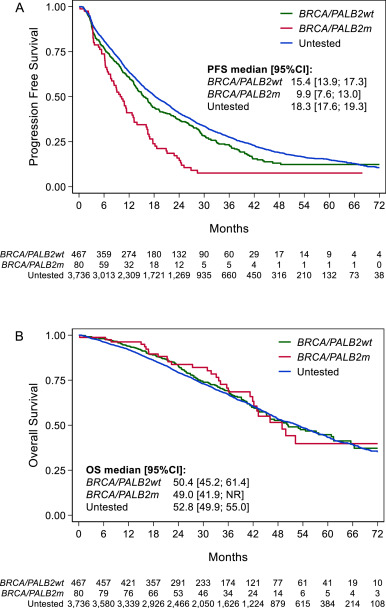
Evidence is accumulating.
Consistent with our meta-analysis presented at #ESMO25, this retrospective cohort shows that first-line CDK4/6 ET leads to shorter PFS in pathogenic BRCA1/2 and PALB2 carriers!
thebreastonline.com/article/…
13 Oct 2025

#ESMO25
My meta-analysis on gBRCA1/2 & CDK4/6i in HR /HER2– MBC
🔹 9 studies
🔹 gBRCA1/2 → shorter PFS & OS vs WT
🔹 Strongest effect in gBRCA2 (possible RB1 link?)
💬 gBRCA1/2 may indicate a negative prognostic profile under CDK4/6i therapy.
Predictive value??
13
44
4,192
Together4Cancer retweeted

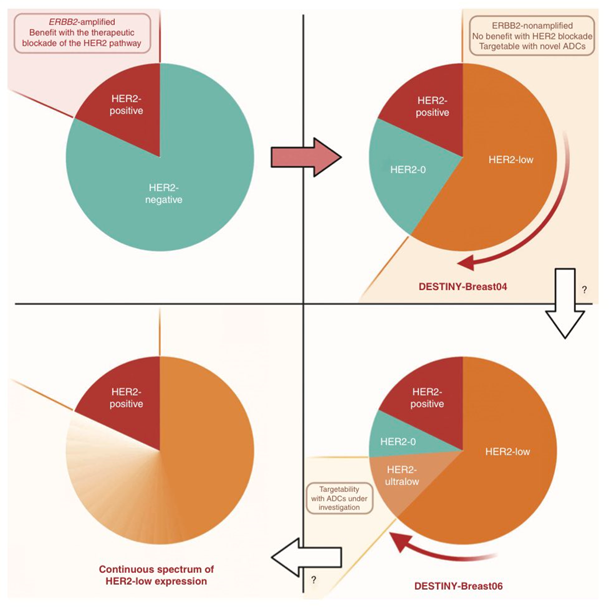
T-DXd has revolutionized the treatment of HER breast cancer, yet predictive biomarkers are critically needed
An exploratory biomarker analysis of DestinyBreast trials is now out in @Annals_Oncology 👇🏻
@OncoAlert

📣A pooled analysis of DESTINY-Breast01/02/03 evaluated the association between best response to T-DXd and baseline characteristics/survival
👉Response was associated with higher HER2 plasma copy number, lower ESR1 expression, lower ctDNA, and better survival
1
16
39
4,240
Together4Cancer retweeted

Jan 29
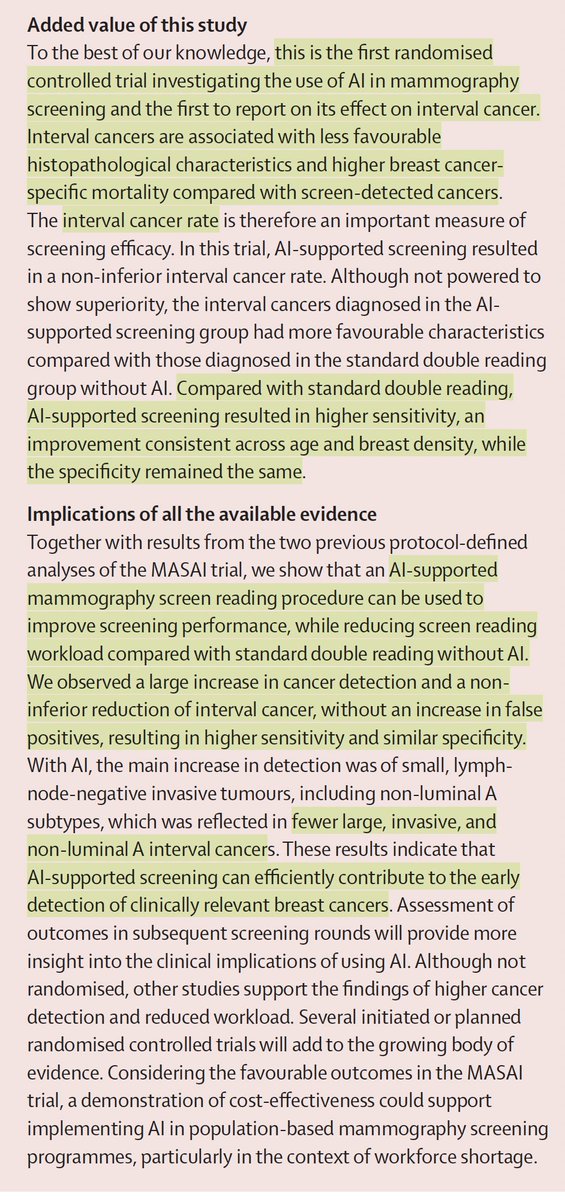
The largest randomized trial of medical A.I.
—Over 100,000 women in Sweden
—radiologist AI vs 2 radiologists, in follow-up
—AI added led to 29% more cancer detected, 44% reduced workload, and
—Less cancer dx in subsequent 2 years, and, when found, less aggressive
thelancet.com/journals/lance…
113
1,296
5,957
1,501,604
Together4Cancer retweeted
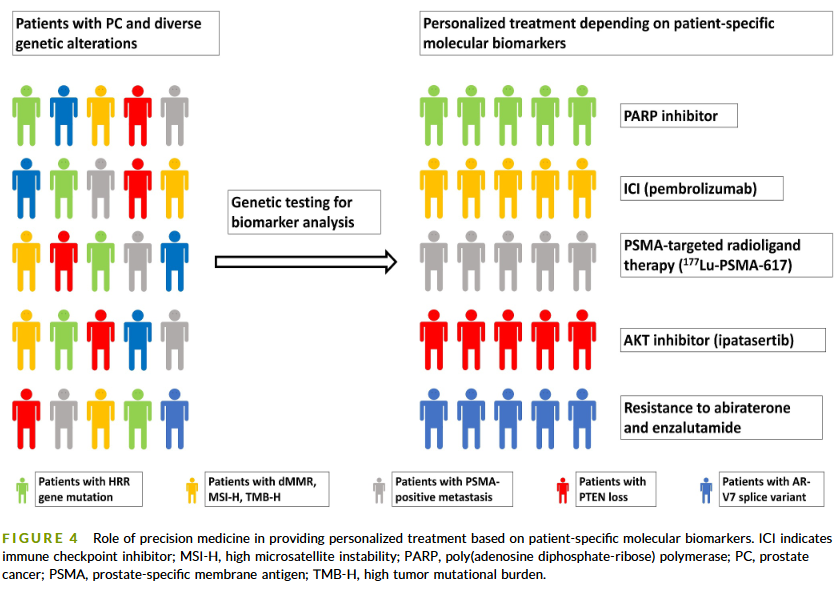
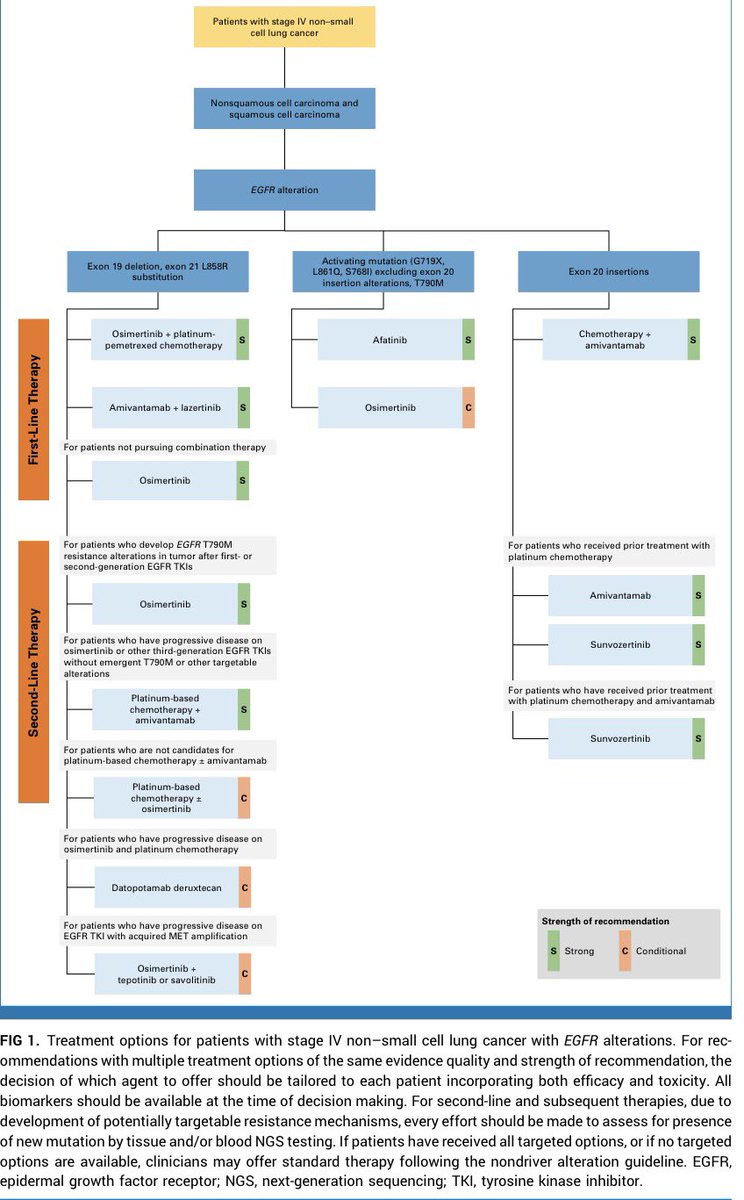
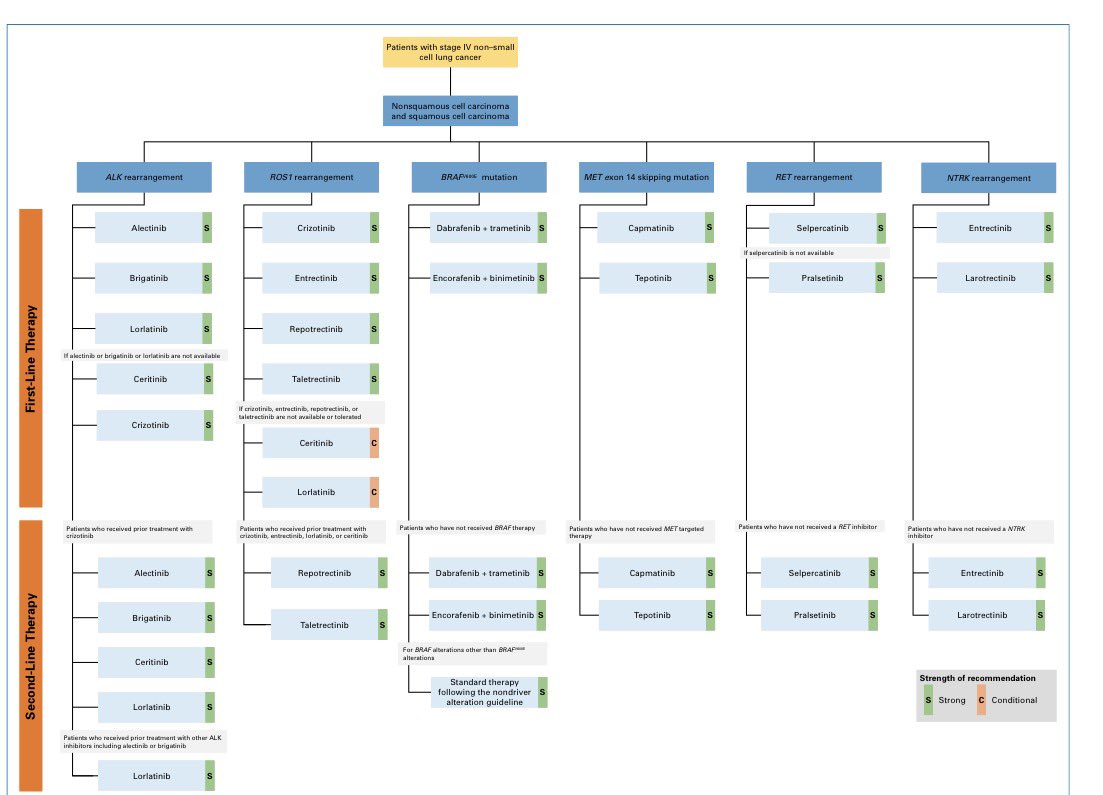
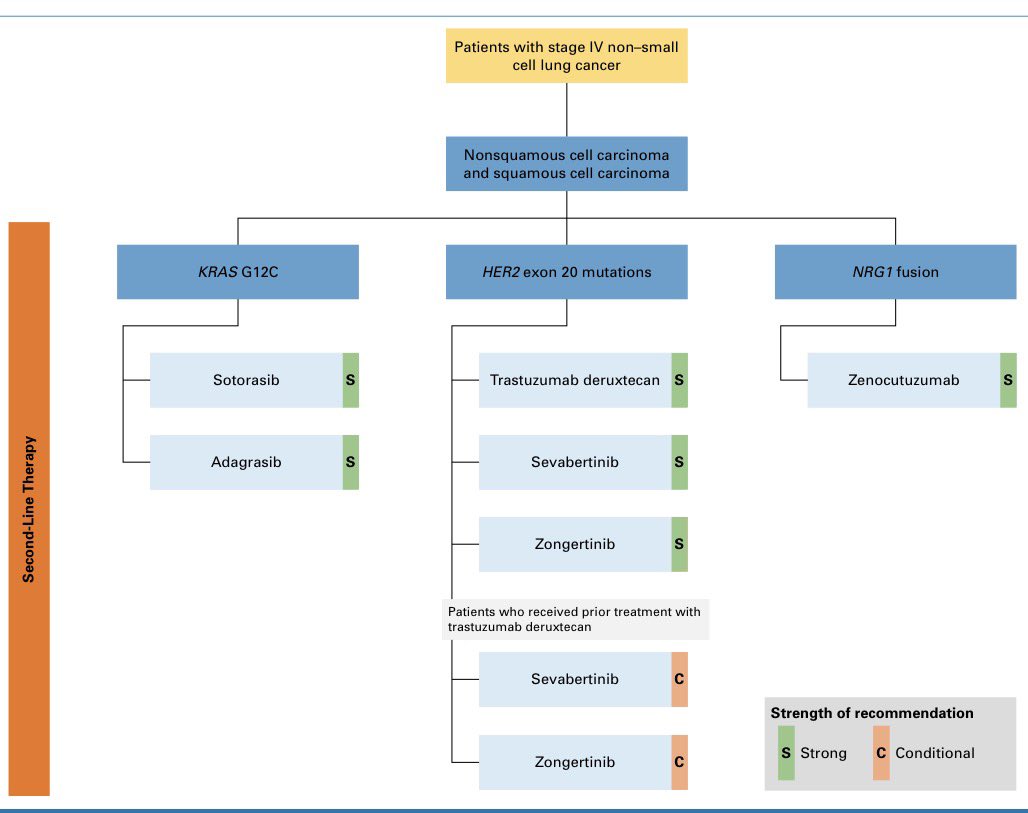
Precision oncology in stage IV NSCLC is no longer optional. It is the backbone of care. 🧬🫁
One diagnosis. Multiple molecular roads. Very different treatments.
What matters first? Broad NGS upfront. Always.
🔹 EGFR alterations
Exon 19 del / L858R: osimertinib ± chemo or amivantamab lazertinib
Exon 20 insertions: chemo amivantamab
Resistance pathways now include MET, T790M, ADCs, bispecifics
🔹 ALK, ROS1, RET, METex14, BRAF V600E, NTRK
Highly effective targeted TKIs upfront
Sequencing matters more than ever after progression
🔹 KRAS G12C, HER2 exon 20, NRG1
Targeted options mainly in later lines
ADCs and next-gen TKIs changing outcomes
Key takeaway 👇
Stage IV NSCLC is not one disease.
Treat the driver, not just the histology.
📌 Broad molecular testing at diagnosis = survival-defining decision.
#OncoTwitter #MedTwitter #LungCancer #NSCLC #PrecisionOncology #TargetedTherapy #CancerGuidelines @asco @JCO_ASCO @myESMO @OncoAlert
2
23
63
13,404


Together4Cancer retweeted

17 Dec 2025
⏱️ Oncologists: save patients time & reduce infusion center overload - infuse pembro in 10 minutes instead of 30. ⏱️
Safety data now out in @JCOOP_ASCO, IRR low (4%) & similar to 30 min infusion. @Oncoalert @JCO_ASCO
ascopubs.org/doi/10.1200/OP-…
2
18
98
11,512

16 Dec 2025
I LOVE “less may be more” trials.
SUPREMO gives us cleaner language for the PMRT gray zone (post-mastectomy, intermediate-risk: pT1N1/pT2N1/pT3N0 or pT2N0 w grade 3/LVI; modern systemic therapy; margins ≥1 mm).
What it found at ~10 years:
• OS: 81.4% w chest-wall RT vs 81.9% w/o (HR 1.04) — no survival benefit
• DFS/DMFS: no meaningful difference
• Chest-wall recurrence: 1.1% vs 2.5% (HR 0.45) — <2% absolute benefit
• LRR: 2.7% vs 4.5% (HR 0.61; CI crosses 1) — directionally better
Takeaway:
In this risk band, chest-wall RT looks like a *small local-control lever*, not a survival lever.
So the real question is: what’s this patient’s baseline 10-year LRR, and is that absolute reduction worth the tradeoffs (reconstruction goals, lung/heart dose, lymphedema, patient priorities)?
Patient perspective: RT mainly lowers a small chance of local recurrence; survival and distant recurrence weren’t improved. Let’s decide if that absolute reduction is worth it for me.
Source: doi.org/10.1056/NEJMoa241222…
76
16 Dec 2025
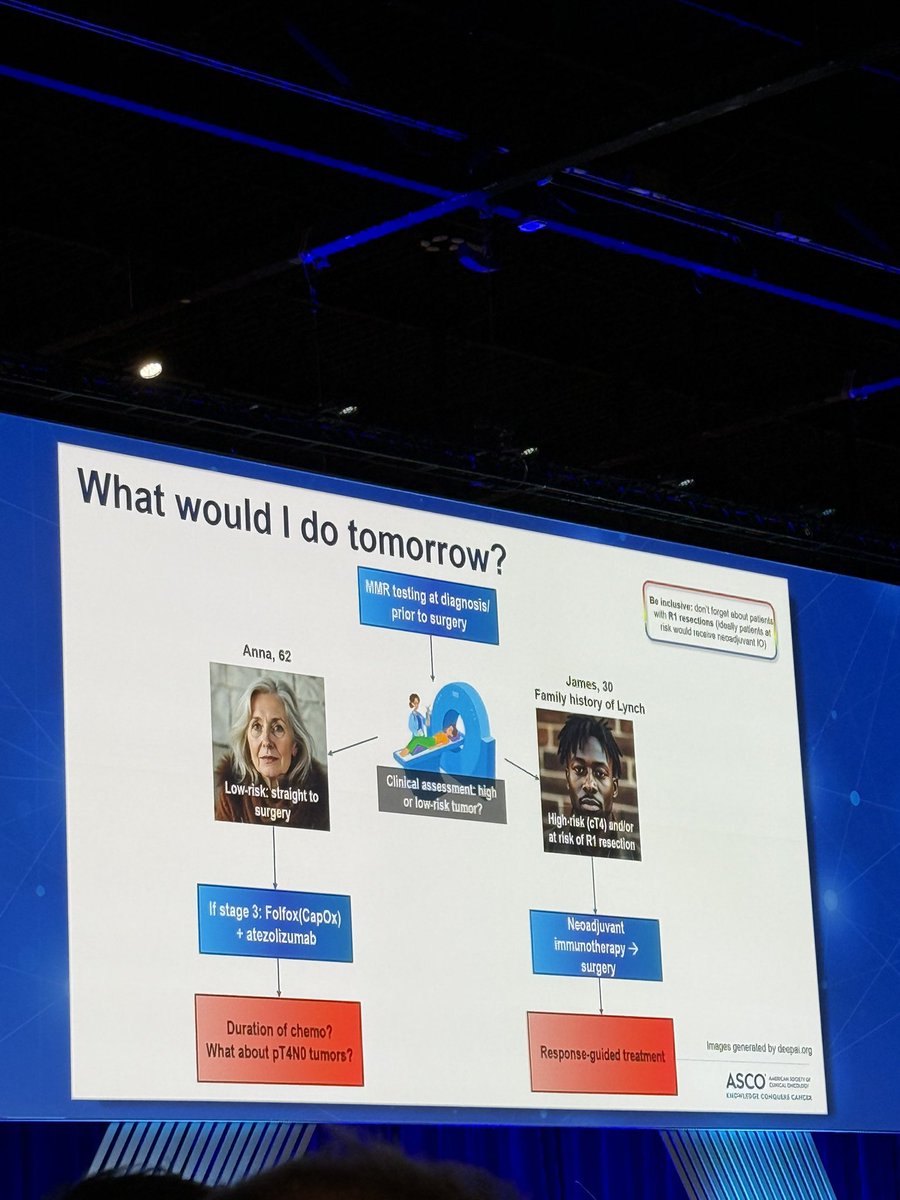
Locally advanced rectal cancer is no longer automatically a trimodality, surgery-first disease. This review pulls together the total neoadjuvant therapy (TNT), watch‑and‑wait, and dMMR‑IO data into one question: for which patients is a stoma now optional—and how safe is that bet in community practice?
Source: doi.org/10.1146/annurev-med-…
106
Together4Cancer retweeted

10 Dec 2025
And dont forget the Five S Rules in #ILD management, as published by my dear friend @PTarantinoMD, wonderful mnemonic for us to remember for our patients, and management guidleines @TumorBoardTues
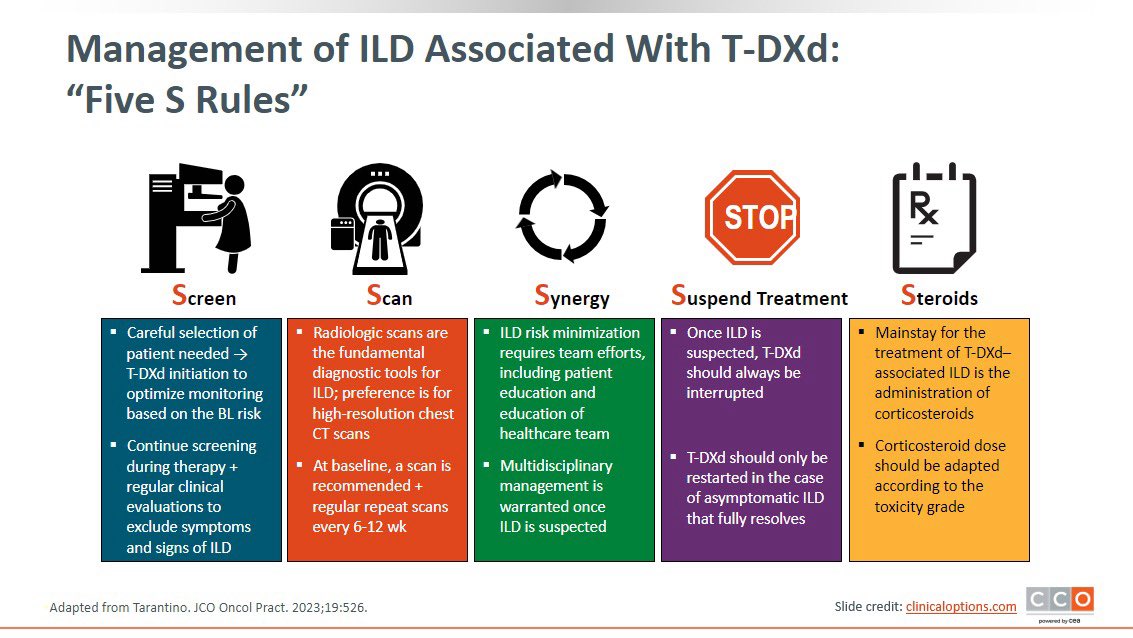
10 Dec 2025

#TumorBoardTuesday
This is where experience is so valuable...by luck of the draw, I have hardly ever used T-DXd and I think my first case of even Grade 1 ILD would make me very nervous to continue therapy even with complete resolution of symptoms😨
7
15
2,050
Together4Cancer retweeted

7 Dec 2025
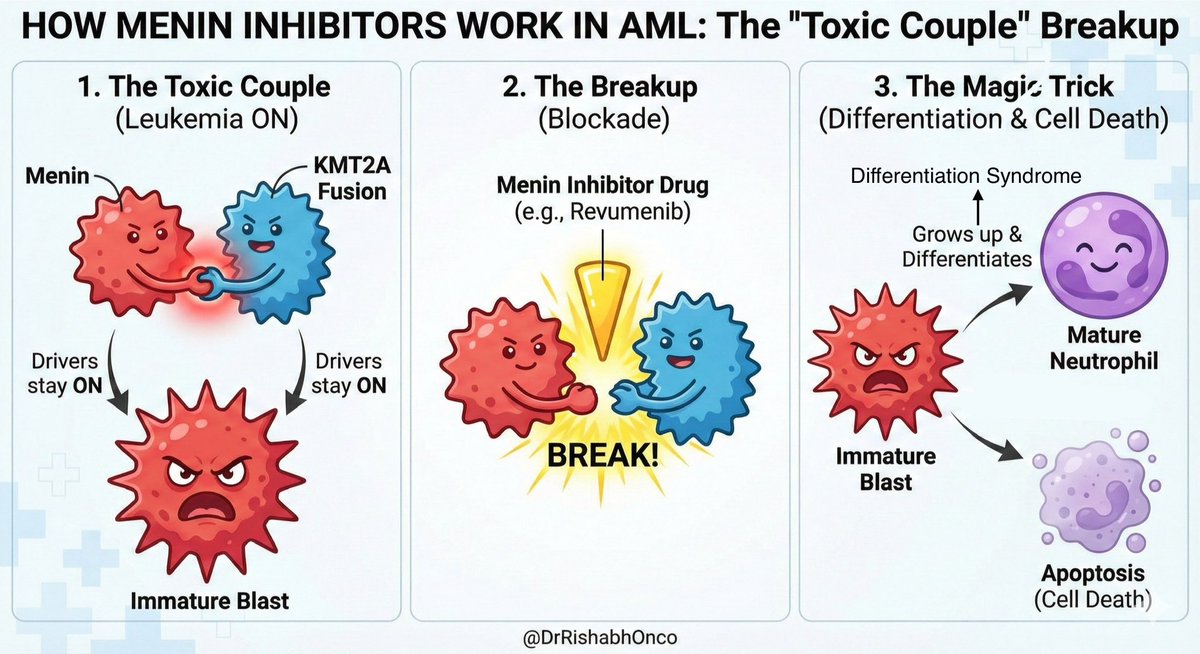
🛑 Stop treating AML like it’s 1990.
We used to just blast the marrow with chemo. Now we are doing molecular micro-surgery.
The star of #ASH25 is the Menin Inhibitor (Revumenib or Ziftomenib).
Here is why this feels like Sci-Fi:
❤️🩹 1. The Toxic Couple
In KMT2A-rearranged leukemia, two proteins cling to each other: Menin KMT2A.
As long as they hold hands, the leukemia program stays ON.
The cell remains an immature, furious blast.
💊 2. The Breakup
The drug does not kill the cell with poison.
It slides between them like a wedge.
Handshake broken.
Switch flipped OFF.
✨ 3. The Magic Trick
The blast realizes it was never meant to be a rebel.
It grows up into a neutrophil.
Does its job.
Then quietly retires.
⚠️ Clinical Pearl
This sudden awakening can trigger Differentiation Syndrome.
Fever, hypoxia, weight gain.
It looks like infection but signals the drug is doing exactly what it should.
Treat with steroids along with supportive care.
Precision Oncology has finally entered AML.
#Leukemia #MedEd #Oncology @OncoAlert @ASCO @myESMO
5
53
207
13,661
Together4Cancer retweeted

8 Dec 2025
Aza Ven >>> IC for select ND-AML 💪🏽
The goal is to get into CR and consolidate with allo. Allo works best if you are fit enough to survive it! Aza-ven gets you there in better shape 💪🏽
Congratulations to Dr. Fathi et al 🙌🏽
#ASH25
7 Dec 2025

#ASH25 #ASHPlenary
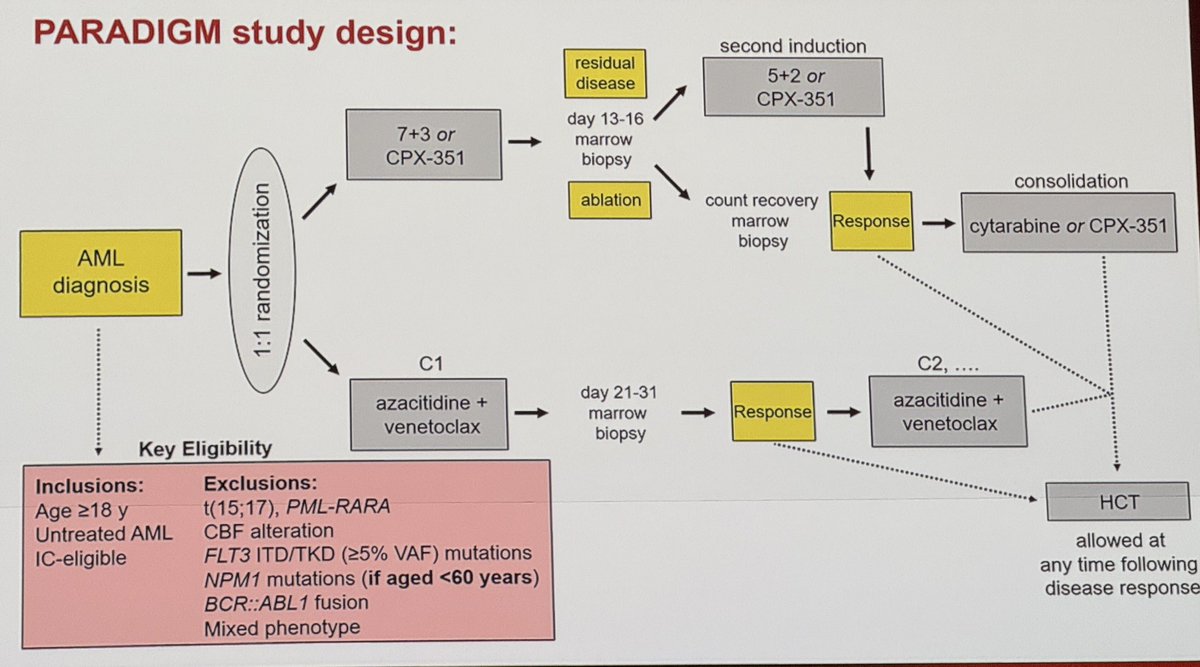
#PARADIGM trial
Great work, congratulations to Dr. Fathi and colleagues! #AML #leusm
Summary:
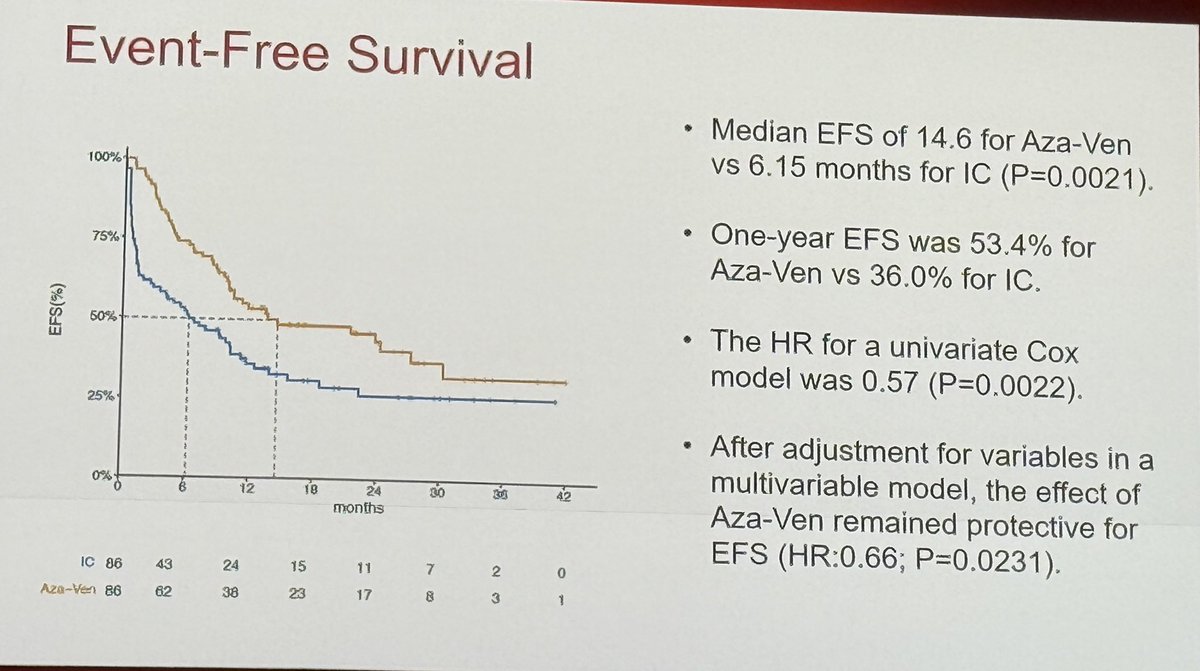
The study met PE for EFS.
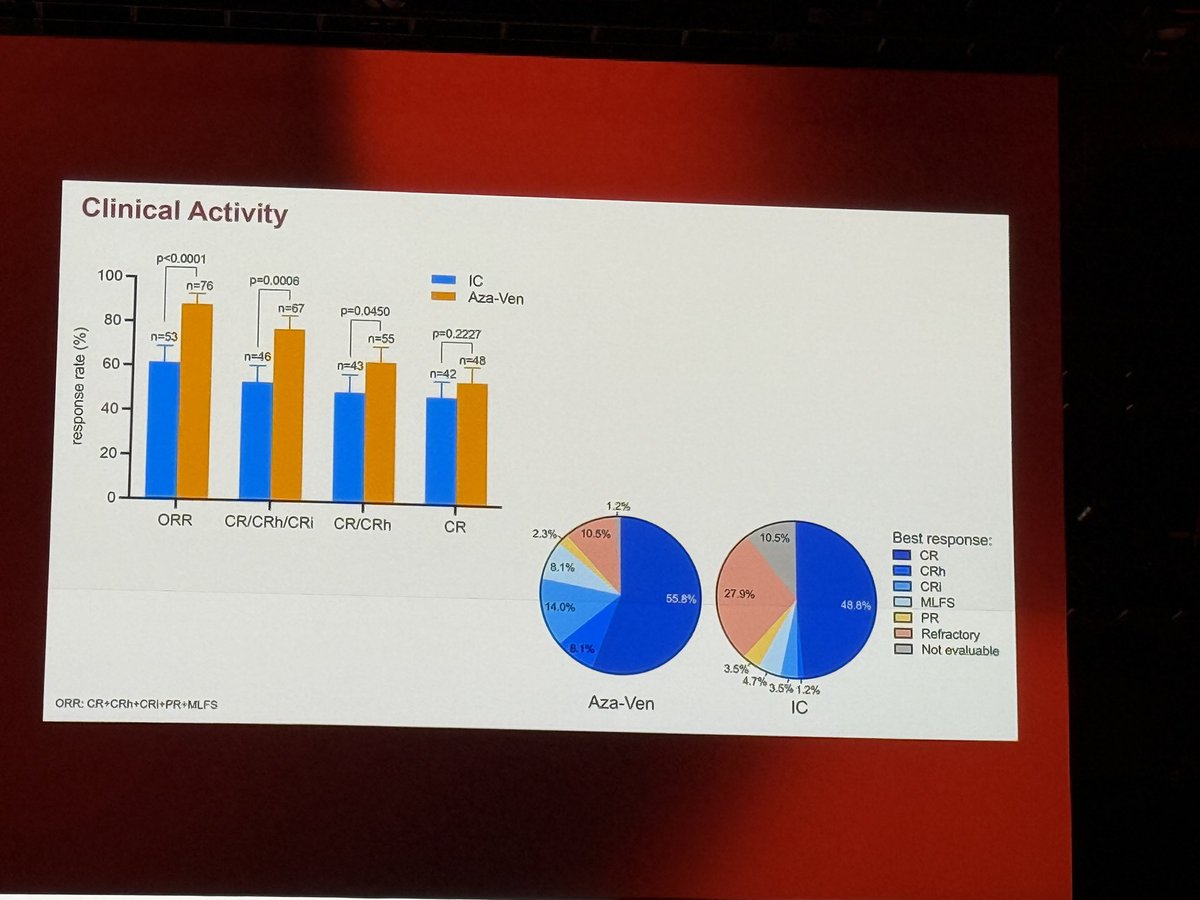
Higher ORR and CR in VEN AZA gp
More pt received transplant in VEN AZA gp
Better QOL
2
13
93
10,368
Together4Cancer retweeted

7 Dec 2025
#ASHkudos to @SLentzsch
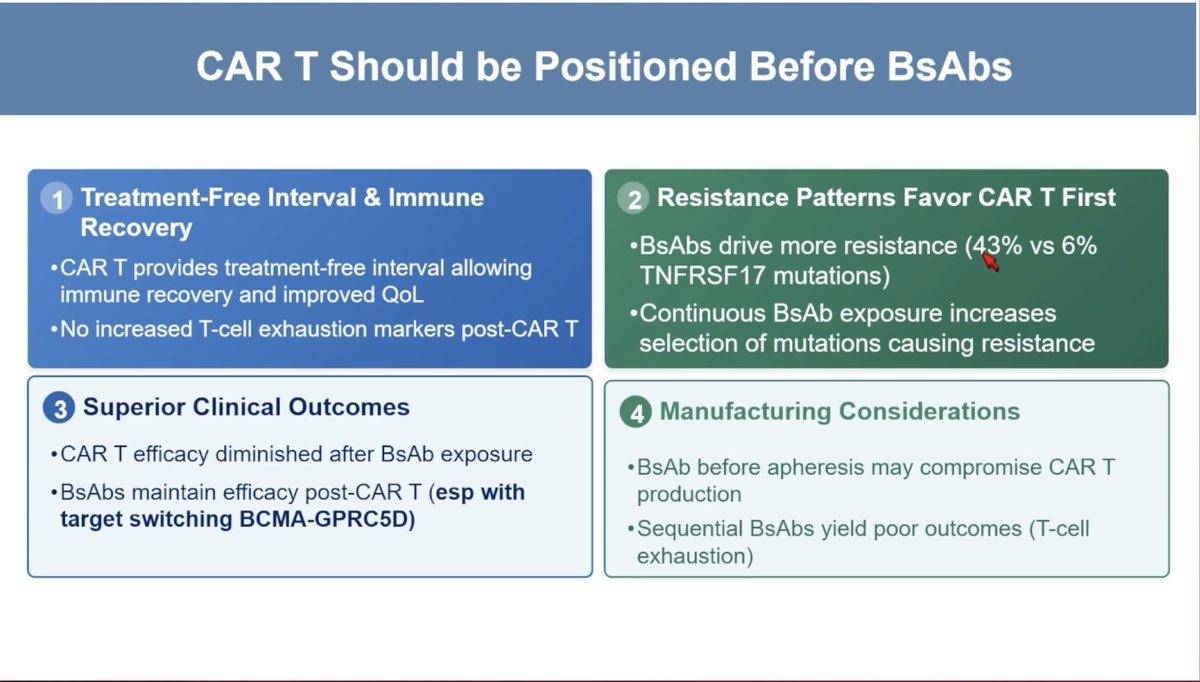
This is the nicest and most succinct explanation I’ve seen for CAR-T before bsAbs in myeloma 👏
And I agree! Even once MajesTEC-3 approved based on #ASH25 results, please make sure #MMsm pts hear about BCMA CAR-T as an option before starting bsAbs!
7 Dec 2025

#ASH25 #mmsm @ASH_hematology
Treatment Refinement in Multiple Myeloma
@SLentzsch
Reasons why CAR-T should be positioned before BsAbs
2
24
99
12,191
Together4Cancer retweeted

24 Nov 2025
24 Nov 2025

Improving communication between healthcare professionals and patients living with advanced breast cancer: a global expert review and call-to-action for 2025–2035 (Goal 5)
sciencedirect.com/science/ar…
Manuscript examines the evolving landscape of communication in advanced #BreastCancer (ABC), emphasizing that while communication skills training for healthcare professionals has expanded in scope, significant gaps remain in meeting the broader communication needs of patients. Drawing on findings from the ABC Global Alliance’s Global Decade Report 2.0, it highlights discrepancies between doctors’ and patients’ preferences for shared decision-making and underscores the importance of empowering patients to express their needs to improve care. These insights have guided the development of the ABC Global Charter 2.0, which sets ten measurable goals for 2025–2035 aimed at enhancing the lives of individuals living with ABC worldwide.
@ABCGlobalAll
@FallowfieldLJ
@franboyleAM
@renatehaidinger
@luzia_travado
@matteolambe @aftimosp @E_de_Azambuja @ErikaHamilton9 @double_whammied @stage4kelly @coffeemommy @itsnot_pink @maryam_lustberg @IBCResearch @kevinpunie @nicolobattisti @raalbany @hoperugo @teamoncology @stolaney1 @LoiSher @jamecancerdoc @JavierCortesMD @JaniceTNBCmets @Prof_Nadia_H @MammaMiaMagazin @itrisabel
#OncoAlertAF
@nataliagandur @acampsmalea @BRicciutiMD
@FernandoOnco
@ElisaAgostinett @to_be_elizabeth @bavilima @realbowtiedoc @Erman_Akkus @Lucarecco @GaiaGriguolo @JankovicK @JooMouta2
@MarioBalsaMD @DrMirallas @GIMedOnc @OscarTahuahua @UOzkerim @DrRishabhOnco @Onco_Cifu88

4
5
528
10 Nov 2025
In cancer care, health literacy doesn’t just shape understanding—it shapes experience.
A population study (PROFILES registry) found that even among high–health literacy patients, those with rare cancers reported lower satisfaction, information access, and quality of life than those with common cancers.
In lower–HL groups, gaps narrowed—but outcomes still fell across the board.
The takeaway: information equity isn’t just about simplifying language. It’s about tailoring communication to context, rarity, and need—especially for those facing cancers that don't get the same share of voice as others.
Source: doi.org/10.1007/s13187-025-0…
#leusm, #MedTwitter, #OncTwitter
1
117