
May 27
Great thread by @DrJoFranklin 🫡 Says it all about the dangerous everlasting car crash going on with a dumbed down noctor quack-workforce flailing around pretending they're not practicing taskified-pseudo-medicine inflicting increasing institutional harms & deaths upon patients
May 26

Agree 💯
RCN (& presumably HCPC too, though they're v quiet about it all) seem wilfully blind to fact that nurses doing tACP are often anything but experienced nurses, often <2yrs qual & some even applying for tACP when still student. Immed B7 pay Day 1 tACP, course paid for 1/
1
8
18
488

May 20
Of course if we do decide that these elements have core educational value, then it cannot be possible that much of what RDs are doing can be taskified and replaced. I think that would throw a massive spanner in the works of many departments up and down the country.
1
6
145

@wesstreeting has made no secret of his aim to end the GP partnership model.
He & @SKinnock have no idea what GPs do, let alone all the unseen work👇🏼done by partners.
‘Taskified care by a team of non-Drs, w/ an occasional GP thrown in for good measure’ is where we’re heading.
1/

Dear @wesstreeting
It’s past midnight. I’m not only on a non-working day, but I’m actually on annual leave.
Partners work unseen, without fanfare or remuneration, for the best interests of our patients. I am pausing now whilst the caffeine-machine boots, to point out how little you recognise of what we do.
You really need to protect partnerships, for the sake of the wider NHS. You will never find anything as cost effective as us. If I was an NHS employee, my leave would be spent in garden centres, pottery painting, at theme parks and sleeping. Instead it’s an opportunity to catch up on prescribing protocols, a new CDM & medication review process to harness best practice, and a variety of other things that enhance patient care and best use of resources. Annual leave is simply an escape from clinical commitment (partly, we are still contacted about it), to provide a space we can fill with other stuff.
You really, really, REALLY need to support GP partners. There is no cohort who are better value than us.
Give us a contract we can work with.
You really really don’t want to lose us. Honest.
1
17
38
1,238
This is genuinely not a criticism of individual non-GP HCPs.
They are taught algorithms & protocols, & how to give taskified care.
& unlike GPs who have completed vocational training, they’re not trained to offer holistic, expert generalist care, which is very different.
2/
2
6
13
2,029

Mar 11
*rotation used to be compensated. It was never a truly effective way of training but we got away with it for a little while for various reasons.
For some years it inherited some of the patterns, traditions, and practices that had always been in place from the time before that were increasingly incompatible with a rotational workforce, but which took time to be dissolved before new structures, with decreasing reliance on residents to provide the full breadth of medical services (by which they actually learnt), were built to replace them.
Consultants continued, for a little while at least, to do what they had always done, and train how they had been trained, at least within the limitations of the rotational system until they 'learnt' the futility and adapted their working and training patterns.
They, accordingly, increasingly fawned over non-doctors who could be trained into imperfect but functional pattern-recognition result-regurgitation machines in a much shorter time than actually training any SHO to perform the department's operations by understanding and thinking about problems and plans, and were more consistent and reliable at taskified operations than the standard of each of the newly-arriving doctors every 4 months. As consultants were ever more squeezed, endorsing these groups over training doctors was not just desirable, but it was fundamentally the only sane business choice and the one which gave consultants the best lifestyle as well.
There were initially fewer doctors relative to training capacity in the system but also less pressure on time with more leeway to try and consciously compensate for the inadequacies of rotational training in the working day/week/month. It is now not just the norm that resident spend every available minute of their days providing low-to-no-training-value barely medical administrative tasks, but trust management and medical 'leaders' view any unused time in their working days as 'inefficiency' that could be used to improve 'flow' and 'operations', and not actually a normal and vital part of the medical job plan to be able to discuss, teach, learn, read, reflect, and troubleshoot.
Increasingly trusts and senior doctors alike realised that resident doctors were free labour that could be dumped on almost any ward to cover it with minimal investment in training... but that for providing clinics, procedure lists, outpatient clinics and other training-critical services that it made no business sense whatsoever to deliver these services with resident doctors, which would cause re-training requirements every 4-6 months and massive fluctuations in productivity in those services on a regular basis. A CNS, ACP, or PA could be trained just once, to a set standard, and to do things the way the consultant liked it 100% of the time, without any particular expertise but certainly with consistency.
Meanwhile, the 'trainee' doctors are cheap and provided by deaneries, and can be rota'd every day onto whatever ward needs a monkey without any training period, so they are. It's the only logical business plan, and no amount of 'shadowing' or 'scheduled days' in clinic or procedure lists is actually TRAINING (which requires constant regular provision of a service out of necessity to actually achieve) but is the bare minimum token excuse to feed back to deaneries and may as well just be work experience.
Rotation was already very obviously unfit for purpose come the mid-2010s when I graduated, but I then watched it all decompensate further and further over multiple years as more and more time and opportunity was sequentially stripped out of every working day, all time for informal teaching was squeezed out and made an exceptional occurrence, and formal teaching time was rationed and bean-counted down to the bare minimum acceptable to the training programmes.
And all of this, based on the fundamentally flawed foundation of an educationalist delusion that you can strip out all apprenticeship, regular exposure, consistency, trust and longitudinal assessment out and boil down all of training down to a series of uncontextualised and episodic forms, of 'assessments' and 'curriculum items', on a portfolio. You can't, and it's been a few decades of madness trying to prove that we can as the entire profession has gone to shit.
1
3
43
But you said “the vast proportion of ppl support the new GP contract & not the GPs”?
The public have been hoodwinked by Streeting & Kinnock. Access to care in a GP surgery may be improving but access to care by actual GPs is being removed.
Suboptimal taskified care is the norm!
4
78

We can agree to disagree,I don’t suggest it lightly. We are heading towards a private, taskified , disjointed, non continuity model that is bad for all.
I do live in the real world as well as twitter 😊
1
21
336

Feb 20
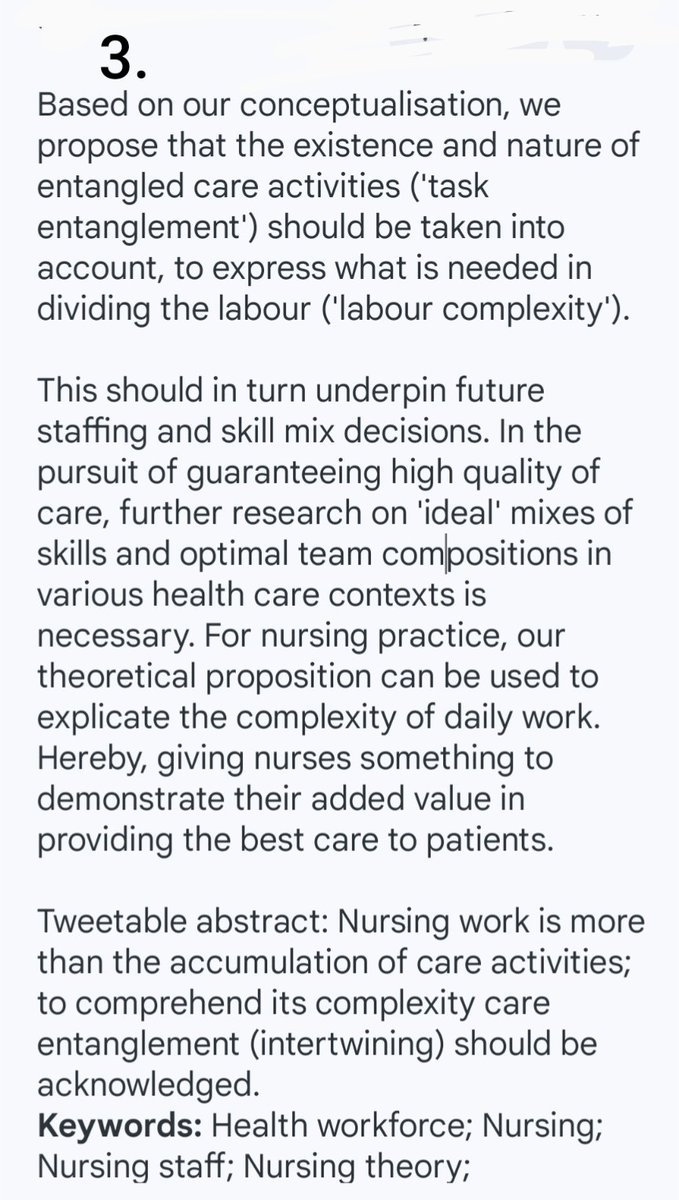
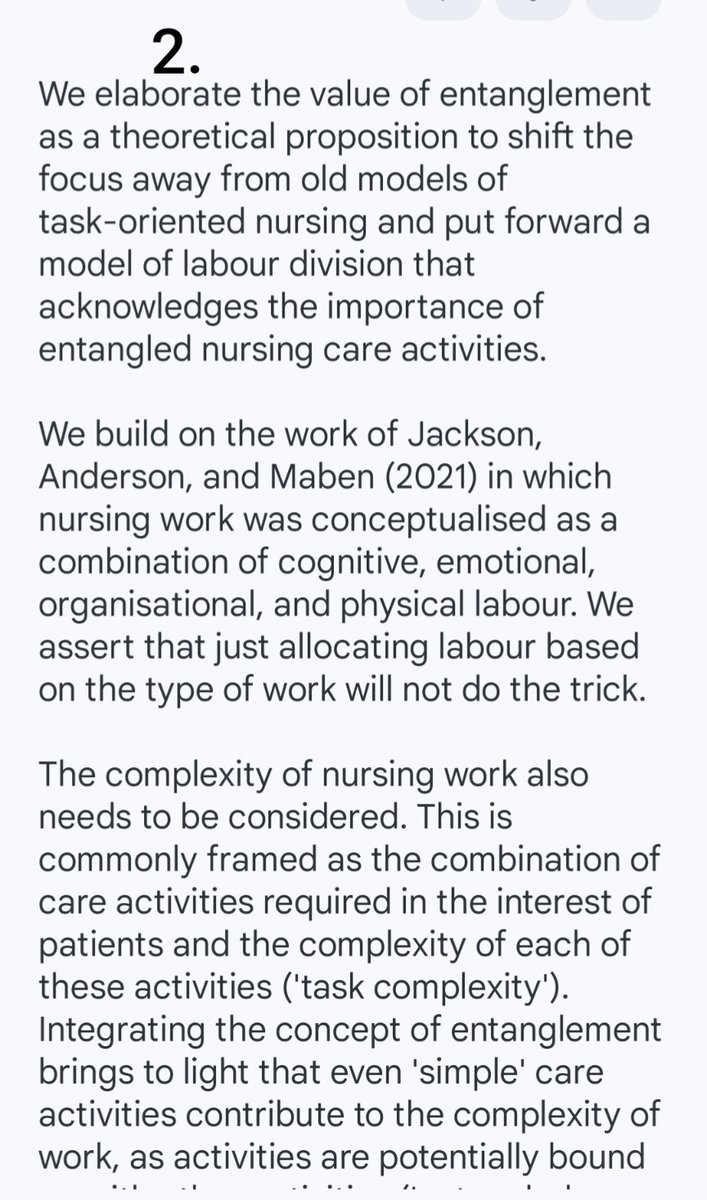
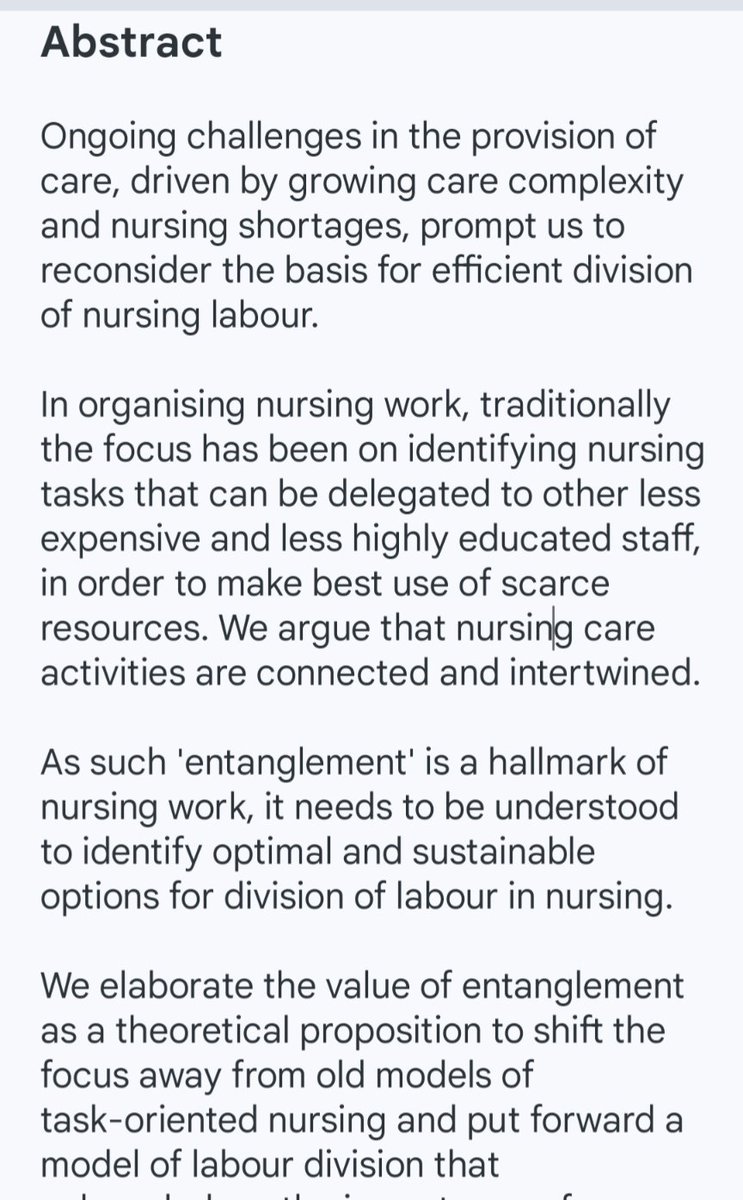
Run ur 👀over this pub on Entanglement in nursing ie. why it can't be taskified hmmm
Strangely silent on work on Indeterminate & Determinate knowledge, cognitive monopolies etc
Larson 1977
Boreham 1983
Abbott 1988
@JaneEBall provides very argument why Medicine can't ⬇️ tasks

1
3
4
130

From what I’m reading @JaneEBall believes that the practise of medicine CAN be taskified and taken over by nurses but nursing practise CANNOT be taskified and taken over by nursing associates
How can these 2 thought processes exist simultaneously?
3
10
55
2,107

Feb 16
same ppl who are excited for "X money" 🤪
more "middle-class" grinding without leverage. eager to normalize taskified, agent-assisted labor mediated by platforms
6
344

Absolutely agree!
But it’s very difficult to get these facts across to ‘the powers that be’ as it’s more convenient to opine that most of general practice can be ‘taskified’ with a protocol sheet and AI. Unfortunately, some doctors - who should know better - facilitate this.
1
5
92

Feb 4
The complexity and humanity of patient care is lost in today's shattered taskified version of medicine
6
183

Jan 6
Modern medicine is becoming “taskified” hence the slow death of clinical medicine.
1
11
430

Framing “task of Medicine” suggests you misunderstand medical practice. It isn’t a task, nor is it a discrete event with finite parameters. It cannot be taskified this way.
Pathology evolves and interacts with other shifting parameters.
To do it right, you need the full training.
1
9
35
598

Don't you see how crazy this tweet is tho?
On the one hand you're saying ACPs can be taskified to do so many things in EM allegedly working to level of ST3, on the other you're saying a CCTd consultant surgeon isn't even good enough.
So why lower the bar even more with ACPs?
1
7
44
2,005

As I have said many time before, the lanyard classes are ushering in two-tier medicine
Those abusing doctors the loudest now will also be the ones having the loudest tantrum when their entire healthcare is delivered by taskified non-medical “advanced practice”
14 Dec 2025

Within the next 20-30 years most healthcare in England will be delivered by non-doctors and bots, blindly following guidelines and pathways.
Doctors will be completely disenfranchised.
The trend of doctors leaving the NHS either to go abroad or to practice privately will accelerate
The only way for most people to get to see a doctor will be to pay.
We’ll have gone back to 4.7.48
The great NHS experiment will have ended.
The circle of change will be complete.
@TheBMA
7
27
78
5,220

A turn primary medical services into ‘taskified’ aliquots of delivery that you can slap blunt targets against, completely missing the point of what made general practice such a success & able to act as such a good gatekeeper and fortune teller (continuity of care for all)
3
8
49
2,026
20 Dec 2025
The alternative of course is that this is what the voting body wants - to have their specialty taskified and broken down, and I'm sure some would welcome under the 'modern ways of working, enough work for everyone' saccharine weirdness that appeals to a select few.
1
2
287
20 Dec 2025
But all under RCS, who have worked heavily on SCP project and not come under much scrutiny for it. But all of these projects basically rely on shortcutting/bypassing medical training in order to achieve a taskified end of some sort.
1
10
282
20 Dec 2025
RCEM and RCGP will be first to 'go' I think, maybe FICM first if it becomes its own College. Any College that has already taskified its own work is vulnerable (RCR maybe somewhere in the middle). Surgery a very broad church with lots of variance.
2
1
13
646