
PCCSM physician |MAMC alum l tweets my own 🇮🇳🇺🇸
Joined September 2017
- Tweets 973
- Following 364
- Followers 430
- Likes 6,994
40 Photos and videos










Himanshu Rawal MD retweeted

Jun 11
ARISE-FLUIDS has arrived and it's awesome 🥳
For over a decade, the Surviving Sepsis Guidelines recommended that septic patients get at least 30 cc/kg fluid. In the United States, these guidelines were weaponized into performance metrics, pressuring clinicians to prescribe arbitrary volumes to every patient.
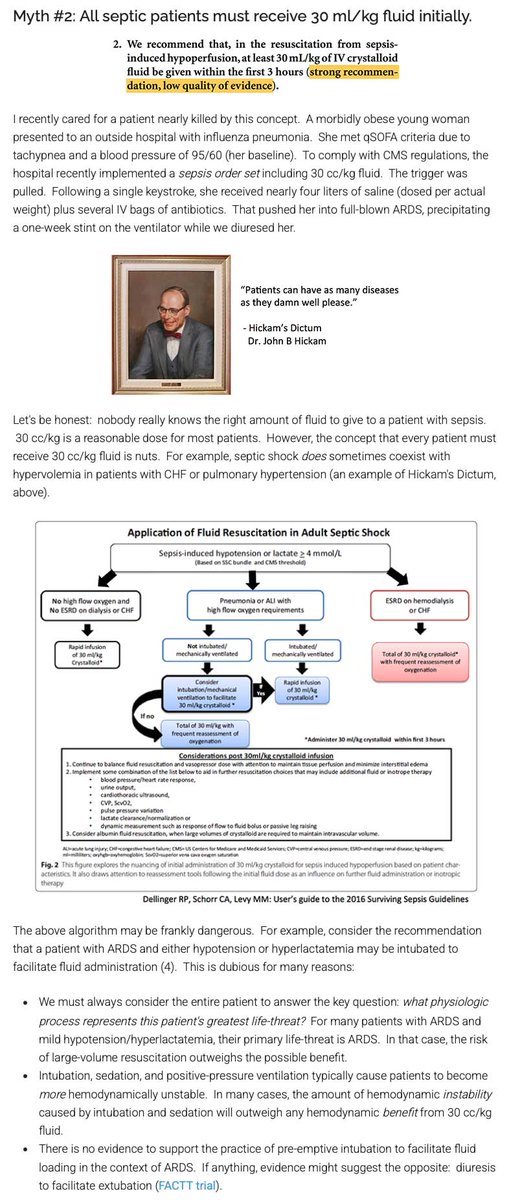
Evidence-based clinicians have LONG known that this guideline lacked evidentiary support. For example, I've attached a picture of a blog I wrote about this back in 2017. Despite the lack of evidentiary support and some evidence of harm, the Surviving Sepsis Guidelines INSISTED on perpetually recommending 30 cc/kg fluid resuscitation.
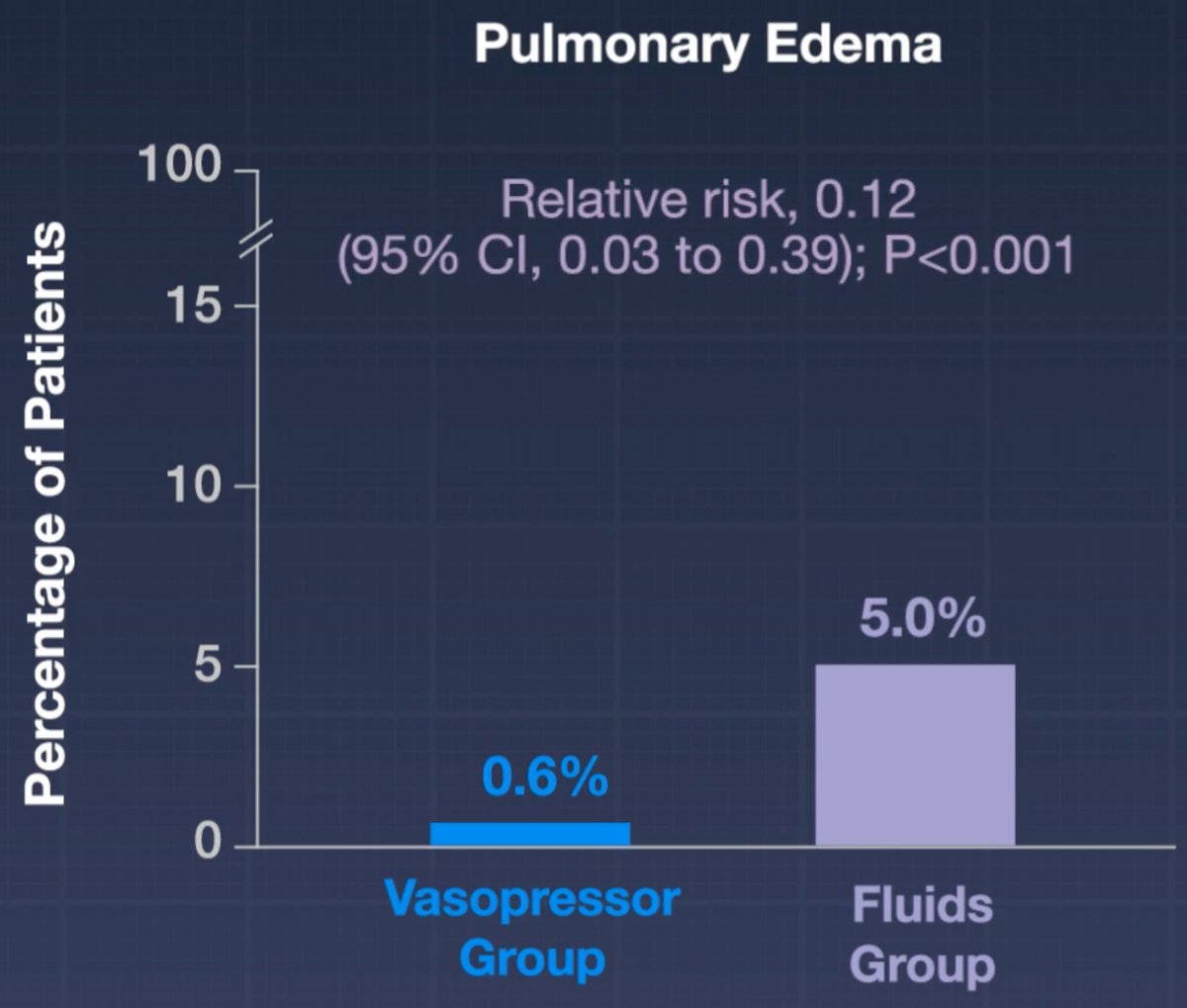
We finally have a prospective RCT demonstrating that mandating early administration of 30 cc/kg fluid (as compared to early vasopressors) doesn't help and may actually cause harm.
It's important to note that all of the hard endpoints in this trial were neutral (e.g., mortality, days free of organ support).
I still think that 30 cc/kg fluid is a pretty reasonable volume of fluid for *most* patients. But the study does suggest that giving too much fluid may promote edema - so we should be *thoughtful* about this intervention rather than mandating it for every septic patient.
Based on the subgroup analysis, the fluid-conservative strategy may have helped the subgroup of pneumonia patients the most. This is statistically nonsignificant but aligns with my expectation. ARDSy patients often don't respond well to fluid. (In contrast, I really doubt that a liter of fluids in either direction matters for most urosepsis patients.)
This is a great example of the over-reach of guidelines and protocoled medicine. People get all upset about practice variation, so sometimes they try to stomp it out using guidelines and protocols. But these guidelines are highly fallible, so what may occur is that you standardize care in a way that harms everyone equally. 🤦♂️


17
146
465
59,241
Himanshu Rawal MD retweeted

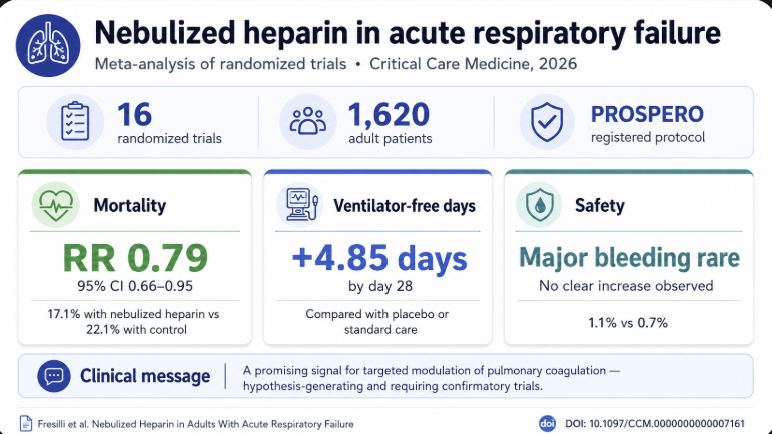
New in @CritCareMed: our meta-analysis of 16 RCTs (1,620 adults) suggests nebulized heparin in acute respiratory failure may lower mortality (RR 0.79, 95% CI 0.66–0.95) and increase ventilation-free days, with no safety signal. pubmed.ncbi.nlm.nih.gov/4214…
19
54
11,968
Himanshu Rawal MD retweeted

🫁 Chest tubes are far more than “just a drain.”
This review is an excellent reminder that successful pleural management depends on understanding physiology, imaging, drainage mechanics, and complications.
Several practical concepts stand out:
📡 Image guidance matters.
Ultrasound is now the standard for pleural drainage, improving success and reducing complications compared with blind insertion. CT guidance becomes essential for loculated, fissural, or complex collections.
📏 Bigger is not always better.
Small bore pigtail catheters are increasingly supported for many pleural effusions and pneumothoraces, often causing less pain and fewer complications. Large bore tubes still retain value in:
• hemothorax
• empyema
• persistent air leak
• mechanically ventilated pneumothorax
⚠️ One of the most misunderstood areas remains chest drainage systems.
The paper clearly explains: • tidaling
• bubbling interpretation
• water seal physiology
• suction management
• digital drainage systems
Importantly, continuous bubbling is not automatically “normal.” It may indicate a persistent air leak, tube malfunction, or incomplete pleural sealing.
Another excellent point: 🧠 excessive suction may sometimes prolong alveolar or bronchopleural fistula healing.
Finally, the review highlights serious complications clinicians must actively anticipate: • tube malposition
• arterial injury
• persistent air leak
• reexpansion pulmonary edema
Chest tube management is not a nursing afterthought. It is dynamic pleural physiology at the bedside.
📖 Ukeh I et al. Seminars in Interventional Radiology. 2022;39:234–247. doi.org/10.1055/s-0042-17512…

ALT
58
199
9,090
Himanshu Rawal MD retweeted
🍽️ ICU nutrition: we’ve been doing it wrong for years?
More calories
More protein
Earlier feeding
Sounds logical
But physiology disagrees
⚠️ The key update
High-quality RCTs now show:
❌ Early full-dose nutrition
→ NO benefit
→ Potential harm
Especially in:
• Shock
• Multiorgan failure
• High metabolic stress
👉 This is not neutral
👉 This is dangerous practice
🧠 Critical illness is not static
It evolves through metabolic phases:
1. Acute catabolic phase
2. Stabilization phase
3. Recovery phase
👉 Feeding must follow physiology
Not protocols
🔥 Phase 1: Acute catabolic
• High inflammation
• Insulin resistance
• Endogenous substrate mobilization
👉 The body is NOT ready for full nutrition
💡 Strategy:
✔️ Permissive underfeeding
✔️ Low protein
Why?
Because early overload leads to:
• Hyperglycemia
• Hepatic dysfunction
• Renal stress
• Impaired autophagy
👉 You are feeding dysfunction, not recovery
⚖️ Phase 2: Stabilization
• Inflammation decreasing
• Organ function improving
👉 Now metabolism starts to tolerate nutrition
💡 Strategy:
✔️ Slow escalation
✔️ Daily reassessment
⚠️ Red flags:
• Hypophosphatemia
• Hyperglycemia
→ Patient is NOT ready
💪 Phase 3: Recovery
• Anabolism returns
• Mobility improves
👉 NOW nutrition matters most
💡 Strategy:
✔️ Higher calories
✔️ Higher protein
✔️ Combine with rehab
👉 This is where you rebuild muscle and function
📊 The real takeaway
Nutrition is NOT:
❌ A fixed prescription
❌ A calorie target
It is:
✔️ A dynamic therapy
✔️ A metabolic intervention
🎯 The new principle
“Start low
Advance judiciously
Individualize throughout”
👉 Precision ICU nutrition
⚠️ Final thought
Overfeeding early harms
Underfeeding late harms
👉 Timing is everything
📚 Stoppe C et al. Curr Opin Clin Nutr Metab Care 2026
DOI: 10.1097/MCO.0000000000001186
ALT
44
117
5,857
Himanshu Rawal MD retweeted
🧠 CO₂ is not just a number...It is a powerful brain modulator.
🚨 In acute brain injury (ABI), PaCO₂ = cerebral blood flow control
Every intensivist knows it…
But we still underestimate it.
👉 PaCO₂ directly regulates cerebral blood flow (CBF)
✔️ ↑ PaCO₂ → vasodilation → ↑ CBF → ↑ ICP
✔️ ↓ PaCO₂ → vasoconstriction → ↓ CBF → ↓ ICP
📊 The physiology is almost linear
🧠 For every 1 mmHg ↑ PaCO₂
➡️ CBF increases ~3–6%
🧠 For every 1 mmHg ↓ PaCO₂
➡️ CBF decreases ~1-3%
⚠️ This is where we get it wrong
Hyperventilation = double-edged sword
✔️ Good → ↓ ICP
❌ Dangerous → ↓ CBF → ischemia
👉 Especially early after injury
🔥 Critical threshold
🚫 PaCO₂ ~25 mmHg
➡️ ↑ glutamate, lactate
➡️ ↓ cerebral perfusion
➡️ ↑ secondary brain injury
👉 Not theoretical. Clinically proven
📉 Outcome data
PaCO₂ follows a U-shaped mortality curve:
⬇️ <32 mmHg → ↑ mortality
⬆️ >45 mmHg → ↑ mortality
🎯 Sweet spot = 35-45 mmHg
🧠 Practical ICU targets
👉 No ICP crisis:
➡️ Aim normocapnia (35-45 mmHg)
👉 Elevated ICP:
➡️ Mild hypocapnia (32-35 mmHg)
➡️ Short-term only
👉 Refractory ICP / herniation:
➡️ Temporary aggressive hyperventilation
⚡ Key mistake to avoid
❌ Prolonged hyperventilation
👉 Leads to:
▪️ Cerebral ischemia
▪️ Worse long-term outcomes
▪️ Hidden hypoxia
🧬 Advanced insight
CO₂ works through:
✔️ CSF pH changes
✔️ Blood-brain barrier diffusion
✔️ Direct vascular tone modulation
👉 Faster and stronger than systemic pH effects
🫀 Clinical reality
Two patients. Same ICP.
But:
▪️ Different compliance
▪️ Different CO₂ reactivity
▪️ Different outcomes
👉 CO₂ must be individualized
🚀 Future direction
▪️ Brain oxygen-guided ventilation
▪️ Multimodal neuromonitoring
▪️ Personalized PaCO₂ targets
🎯 Take-home
CO₂ is not ventilation.
CO₂ is brain perfusion control.
👉 Treat it like a drug
👉 Dose it carefully
👉 Monitor the effect
📚 Taran et al. Intensive Care Med (2025) 51:1256–1259 doi.org/10.1007/s00134-025-0…
ALT
2
48
174
7,435
Himanshu Rawal MD retweeted

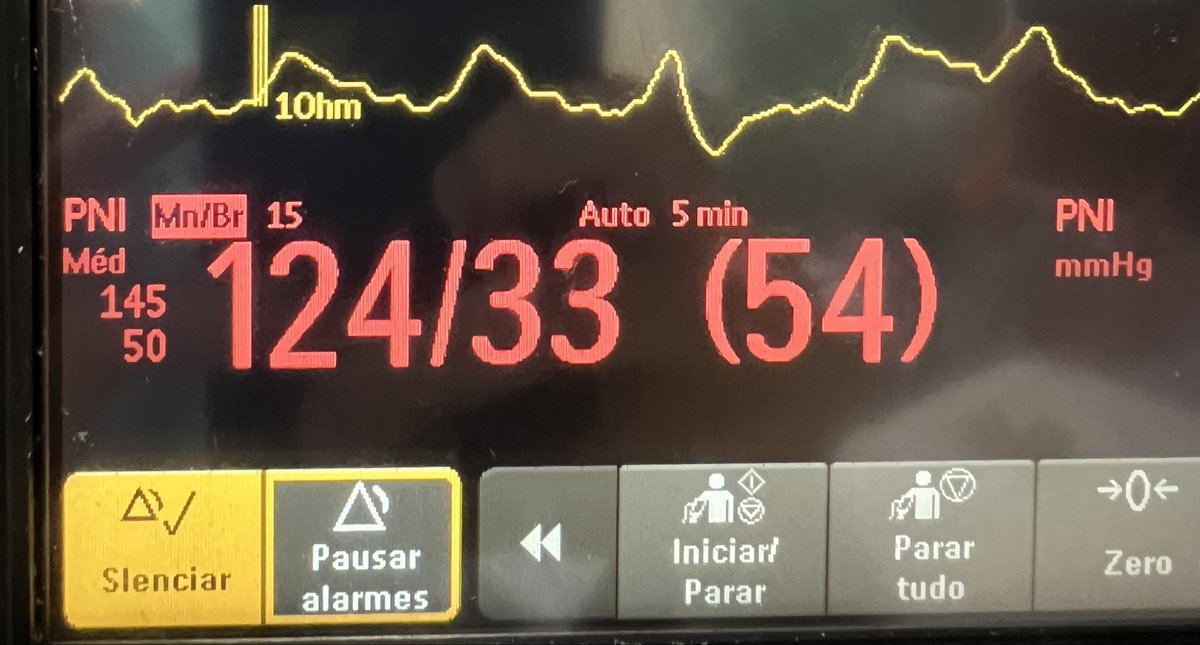
PAD reduzida no choque hemodinâmico é sempre sinônimo de vasoplegia? Nem sempre!
Entenda situações em que a PAD perde acurácia nessa associação.
Segue o fio 🧶
3
21
125
16,097
Himanshu Rawal MD retweeted

10 Oct 2022
[1] #Hemodynamics Tweetorial #2
Heart failure pt in ICU is -3.5L after 2d of aggressive diuresis. On day 3, urine output is ⬇️and BUN/Cr is ⬆️
You personally wedge #PAC at bedside and obtain a mean wedge 17 mmHg (a normal mean wedge is 6-10 mmHg). Admission wedge was 24

29
485
1,327
Himanshu Rawal MD retweeted
🩻Contrast-induced AKI:
one of the biggest myths still shaping clinical decisions
For decades we were taught:
👉 “Contrast damages the kidneys”
👉 “Avoid CT with contrast in CKD”
👉 “Hydrate, protect, delay imaging if needed”
But what if… most of this is wrong?🤔
->The uncomfortable reality
Modern evidence shows:
👉 Low-osmolar contrast rarely causes true nephrotoxicity
👉 Even in CKD, AKI, and ICU patients
👉 The risk is often overestimated—or nonexistent
So where did the fear come from?
📍 1950s high-osmolar contrast (actually toxic)
📍 Poorly controlled observational studies
📍 “Creatinine rise = contrast injury” assumption
👉 Correlation became causation
👉 And the dogma stayed
⚠️What recent data tells us
✔ No difference in AKI rates with vs without contrast
✔ No benefit from bicarbonate, NAC, or aggressive hydration
✔ Even ICU and AKI patients show no worsening outcomes
->Translation to real life
👉 The patient was going to develop AKI anyway...Not because of contrast!!
->The real problem: “Renalism”
👉 Avoiding necessary imaging
👉 Delaying diagnosis
👉 Choosing inferior tests
And that leads to:
❌ Missed PE
❌ Delayed sepsis source control
❌ Worse outcomes
->Clinical mindset shift
Instead of asking:
👉 “Will contrast harm the kidneys?”
We should ask:
👉 “Will NOT doing the scan harm the patient?”
->Who still deserves caution?
✔ eGFR <30
✔ Severe hemodynamic instability
✔ Multiple nephrotoxins
Even then:
👉 Optimize volume
👉 Minimize dose
👉 Don’t delay critical imaging
🤓Bottom line
✔ Contrast nephrotoxicity exists… but is rare
✔ The fear is bigger than the risk
✔ The harm of NOT imaging is often greater
In critical care
👉 We don’t treat creatinine
👉 We treat patients
And sometimes…
👉 The most dangerous thing is NOT the contrast
👉 It’s hesitation.
📃Reference
Florens N, Demiselle J.
Kidney360 7: 445–449, 2026. doi: doi.org/10.34067/KID.0000001…

ALT
20
409
992
224,022
Himanshu Rawal MD retweeted
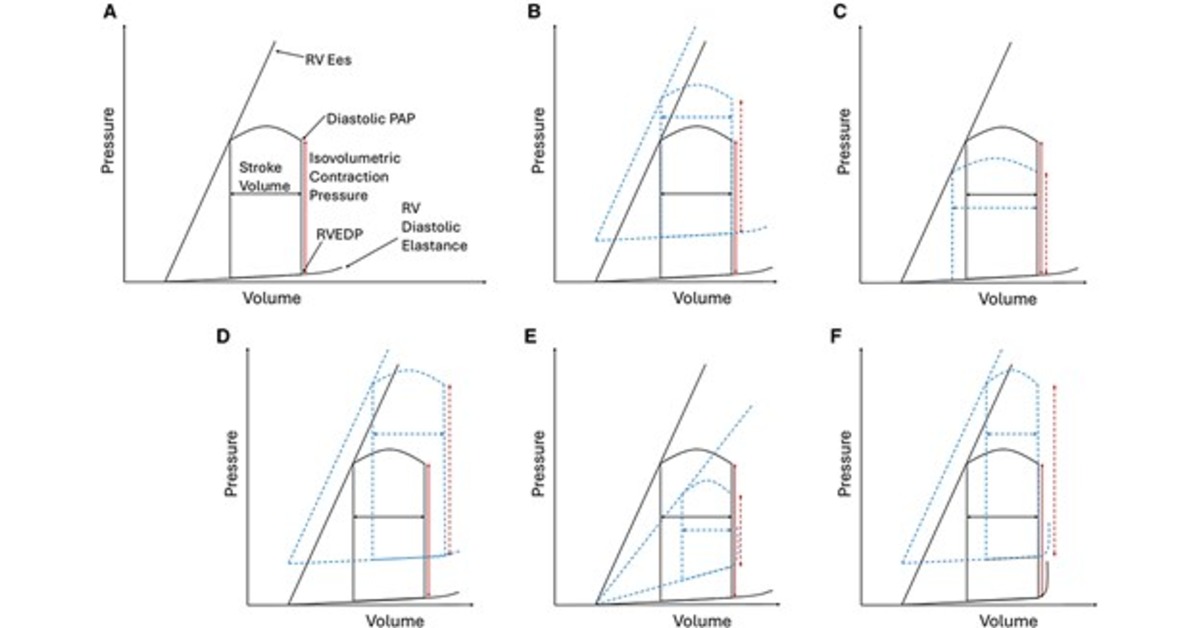
🫀The failing right ventricle:
the most misunderstood chamber in critical care
For years, we focused on the left ventricle.
But in the ICU, the real killer is often the right ventricle.
->What is acute RV failure?
👉 Not just “weak contraction”
It’s a hemodynamic collapse syndrome:
RV dilation
↓ LV preload
↓ cardiac output
↑ venous congestion
➡️ → multi-organ failure
->The key pathophysiology (the vicious cycle)
1. ↑ Afterload (PE, ARDS, PH)
2. → RV dilation
3. → Septal shift → LV underfilling
4. → ↓ CO → hypotension
5. → ↓ RCA perfusion
6. → RV ischemia
👉 And the cycle accelerates
->The most important concept
👉 The RV does NOT tolerate pressure
Handles preload very well
Fails rapidly with afterload
➡️ Even small ↑ PVR → collapse
->Main causes you MUST think first
🔴 Pulmonary embolism
🔴 RV myocardial infarction
🔴 ARDS / mechanical ventilation
🔴 Decompensated pulmonary hypertension
🔴 Post-cardiac surgery
->Diagnosis is NOT obvious
There is no single sign.
👉 It requires suspicion integration:
Clinical: congestion hypoperfusion
ECG biomarkers
POCUS (your best friend 🤓)
Hemodynamics
->Echo mindset (fast ICU approach)
👉 Don’t overcomplicate
Look for:
✔ RV dilation
✔ Septal shift (D-sign)
✔ TAPSE ↓
✔ Venous congestion
The real ICU mistake
❌ Treating RV failure like LV failure
->Management principles
👉 Think in 4 pillars:
1. Preload — “not too much, not too little”
Hypovolemic → small fluid
Congested → REMOVE fluid
👉 CVP is not a target, it’s a warning
2. Afterload, THE key target
✔ Treat PE
✔ Optimize ventilation
✔ Reduce PVR
👉 If afterload stays high → RV will fail
3. Contractility
Dobutamine
Milrinone
Levosimendan
👉 Choose based on context
4. Perfusion pressure
👉 Norepinephrine is your anchor
✔ Maintains coronary perfusion
✔ Supports RV function
->Ventilation: the silent killer
⚠️ Positive pressure = ↑ PVR
👉 Over-ventilate → worsen RV failure
->When nothing works
👉 Think early:
VA-ECMO
RV assist devices
🤓Key insight
This is NOT just a cardiac problem.
👉 It is a ventriculo–arterial coupling failure
When:
Ees / Ea ↓ → RV collapses
🤓Bottom line
✔ RV failure is preload dependent BUT afterload sensitive
✔ Small mistakes → rapid collapse
✔ Early recognition physiology-based treatment saves lives
->Clinical mindset
👉 Don’t ask:
“Is the RV failing?”
👉 Ask:
“Why is the RV failing and, what is driving the afterload?”
📃Reference
Giannakoulas G. et al. European Heart Journal (2025) 00, 1–16 doi.org/10.1093/eurheartj/eh…

ALT
7
257
774
83,247
Himanshu Rawal MD retweeted

Mar 27
If you do outpatient clinical ID, there's an excellent chance you've seen WAY more referrals for latent TB than we used to.
Here's why ⬇️

The number of referrals to ID doctors for latent tuberculosis has exploded. What happened? Read the latest from @PaulSaxMD: voices.nejm.org/doi/full/10.…

ALT Top: On the first visit, a trained health care provider places a TB skin test. Image Credit: Centers for Disease Control and Prevention Bottom: A trained health care provider reads a TB skin test between 48 and 72 hours after placement. Image credit: Centers for Disease Control and Prevention
4
21
113
43,890
Himanshu Rawal MD retweeted
Mar 21
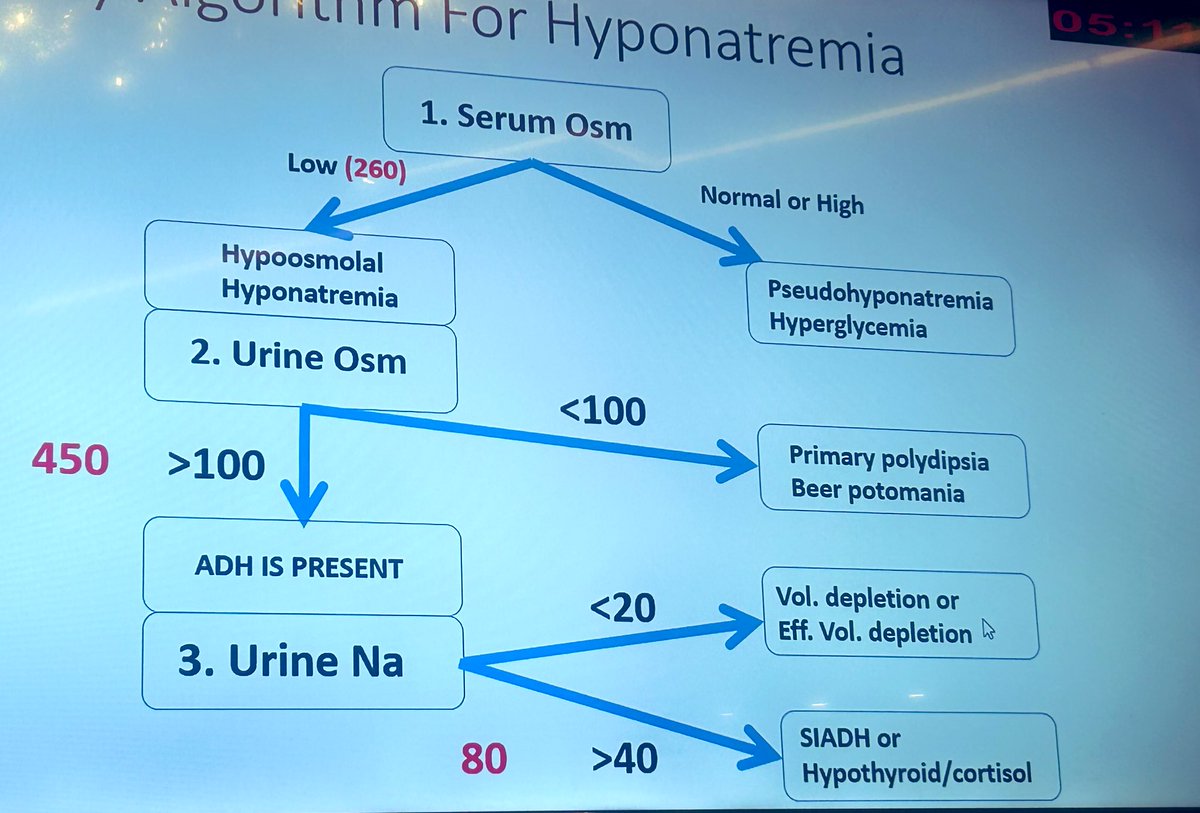
Great schema!
But beware that *any* time you see a diagram like this, it assumes the patient has one disease process.
Our patients are increasingly multimorbid so:
⚠️May have >1 cause of hypoNa
⚠️Fixing one cause may cause dominant physiology to shift (playing wack-a-mol)
Mar 21

🔥Hyponatremia made simple Dr Ajay Kher:
1️⃣ Serum Osm → hypo vs pseudo
2️⃣ Urine Osm → <100 = polydipsia, >100 = ADH present
3️⃣ Urine Na → <20 = volume depletion, >40 = SIADH
🙇♀️Structured thinking = faster diagnosis. #CNSICON2026
@CNSI2026 @VinBhargava @rajdebsaha @drvt87
7
29
177
21,460
Himanshu Rawal MD retweeted

Peripheral vasopressor administration in critically ill adults was associated with a low incidence of adverse events—major events were rare using short peripheral intravenous catheters, and use avoided central venous catheter placement in 60% of cases.
ja.ma/4btNGSr
12
31
3,880
Himanshu Rawal MD retweeted

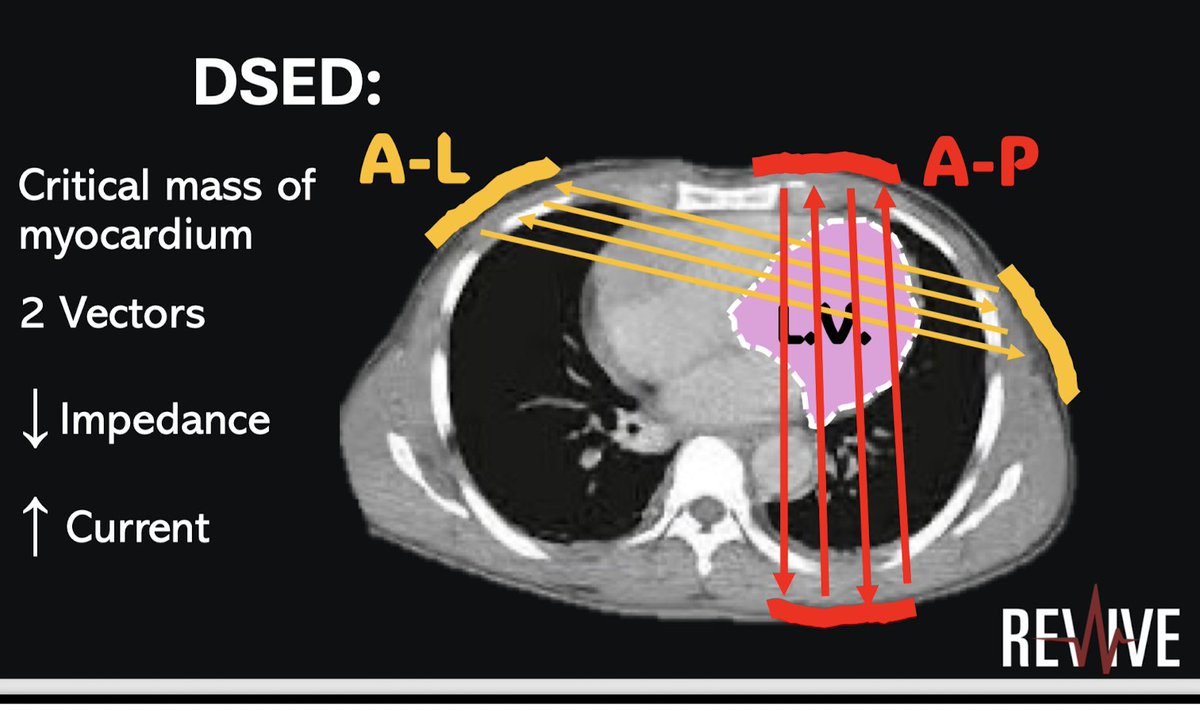
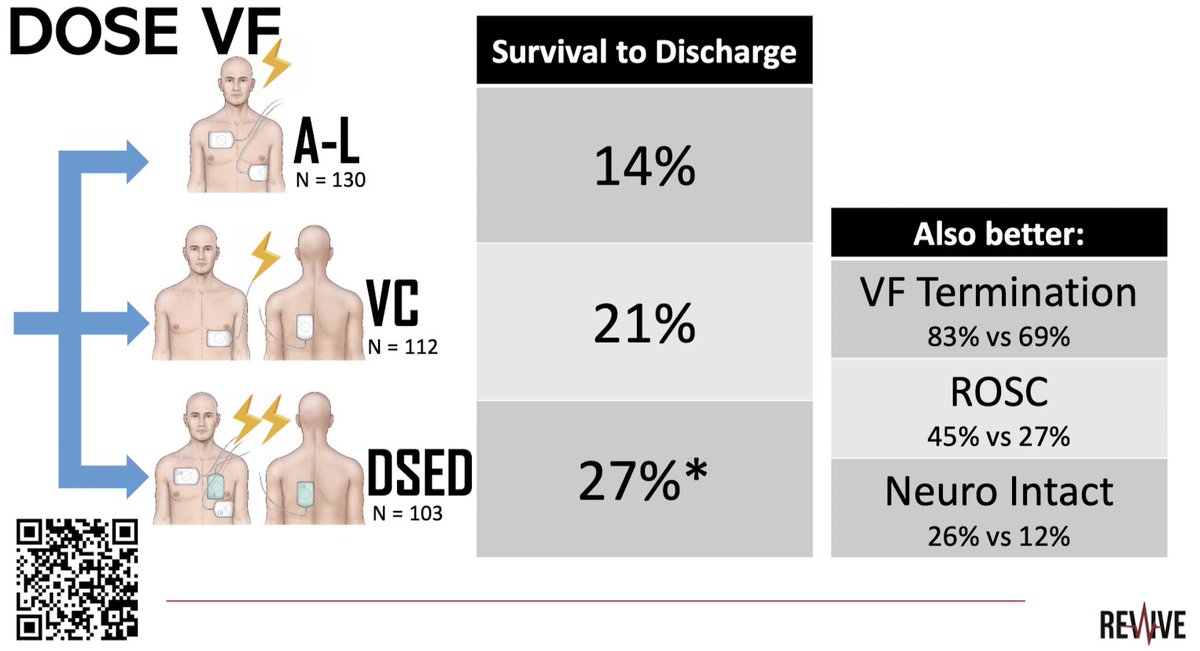
Defibrillation 2.0 by Dr. Corcoran #REVIVE2026
AP pad placement allows
🔺Better vector
🔺 Less impedence
Dual sequential external defibrillation (DSED)
AHA guidelines: Class 2b recom
ILCOR: DSED suggested strategy for VF refractory to shocks
@CardioNerds @OscarJMitchell
1
29
90
10,225

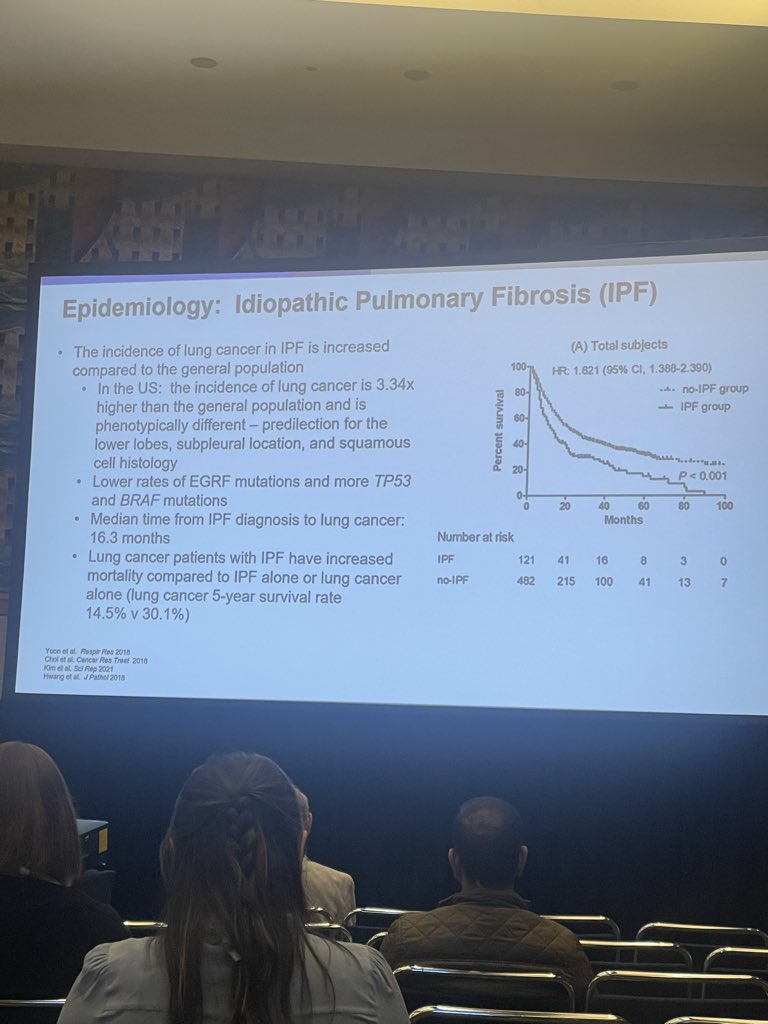
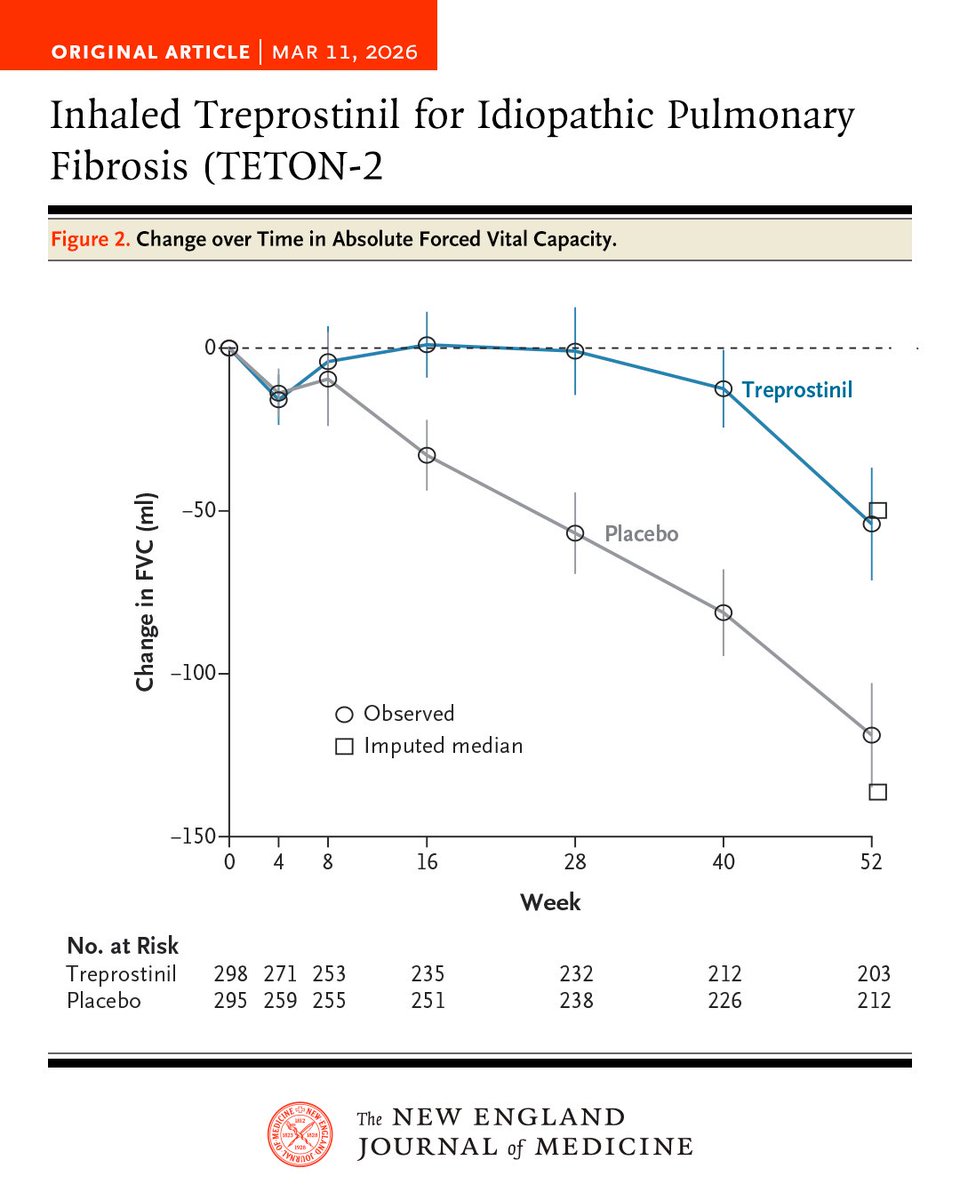
In the phase 3 TETON-2 trial involving patients with idiopathic pulmonary fibrosis, inhaled treprostinil was associated with a smaller decline in forced vital capacity and a lower risk of clinical worsening than placebo over 52 weeks. Full trial results: nejm.org/doi/full/10.1056/NE…
3
38
98
19,615
Himanshu Rawal MD retweeted

Mar 7
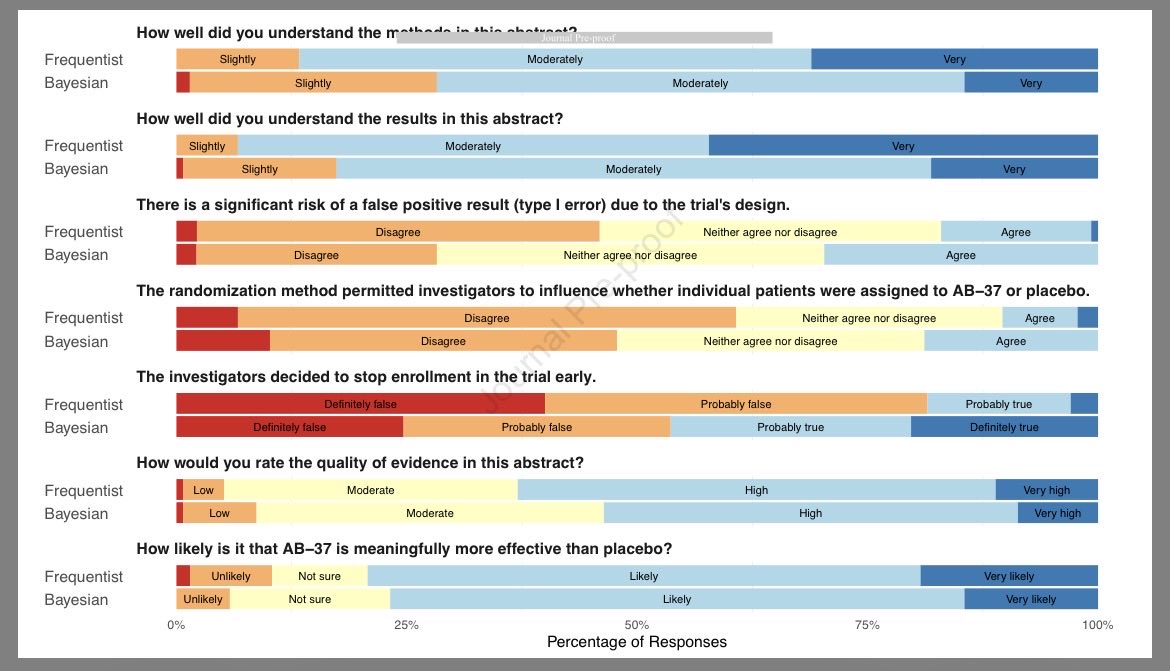
😵💫 Are you confused by Bayesian methods? Do you worry you’re alone? 🫢
Just in #journal_CHESTCritCare, B Malley et al eval how intensivists differently interpret results from Bayesian and frequentist trials…
chestcc.org/article/S2949-78…
…I’m a bit unsettled by their findings 😉
3
9
990
Himanshu Rawal MD retweeted

Mar 2
Great to see this study in press where we show the utility of a sleep positioning device in managing GERD after lung transplant. Novel, safe and cost effective solution to a major problem in this population. Thankful to ACG for the research award! @ScottGabbardMD

1
4
13
2,497
Himanshu Rawal MD retweeted

Mar 1
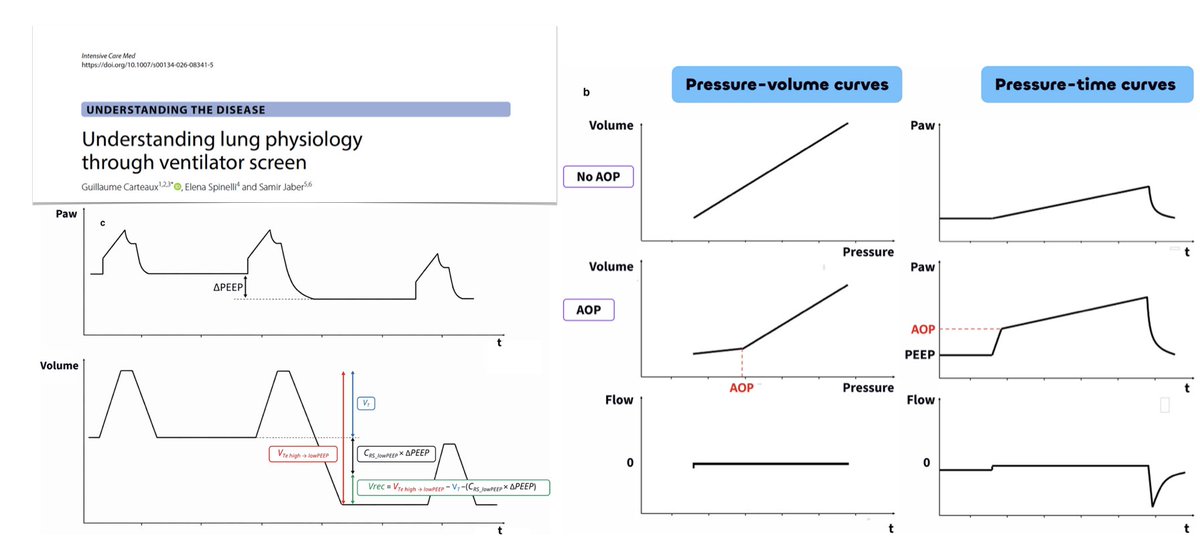
Understanding lung physiology through ventilator screen
🫁 airway pressure waveform at a glance: respiratory system equation of motion, conductive pressure, stress index, driving pressure
🌊 flow waveform during pressure-controlled ventilation
💨 expiratory flow and the time constant of the respiratory system
🛌 dynamic bedside maneuvers: airway opening pressure, recruitability & recruitment-to-inflation ratio
🚧 the way forward
#FOAMcc
🔓 rdcu.be/e6iG6
1
67
211
9,054
Himanshu Rawal MD retweeted

Right Ventricular Hemodynamics in Acute Respiratory Distress Syndrome: Monitoring and Implications for Clinical Management
@atscommunity
🔗 tinyurl.com/4ea9hua2
36
112
7,250
Himanshu Rawal MD retweeted

Feb 2
The time of day for cancer immunotherapy is associated with major outcomes. Early is better. Results from a randomized trial of lung cancer, backs up the importance of our circadian rhythm and immune system
nature.com/articles/s41591-0…

48
327
1,374
544,352

*Pulmonary embolism* versus *Acute myocardial infarction*:
Above and below the pen: the size of the clots in each scenario
I was looking for a picture like this and found it in a lecture by Dr Sripal Bangalore
#foamed #foamcc #meded #MedTwitter

6
55
268
24,893