
Joined January 2020
- Tweets 133
- Following 298
- Followers 187
- Likes 399
4 Photos and videos


Thatcher Heumann retweeted

Jun 13
Had the chance to give the colorectal cancer update at Best of ASCO Los Angeles.
Always fun to summarize a year of CRC data in ~20 minutes while pretending that is a normal thing to ask of a human being.
4 takeaways (without getting into some of the really exciting drugs that are coming to CRC soon):
🔹 MSI-H CRC in complete clinical response on PD-1
Stopping at confirmed cCR looks safe. Maintenance may add toxicity without clear benefit.
🔹 BRAF V600E MSS mCRC
Encorafenib cetuximab chemotherapy is now a 1L standard. FOLFIRI is a great option, and FOLFOX is reasonable too. Either way, the targeted therapy backbone is here.
🔹 ctDNA / MRD
Not fully in NCCN yet, but increasingly actionable. I escalate select stage II patients, use it to frame de-escalation discussions, and strongly favor trials when possible.
🔹 Exercise
Prescribe it like we prescribe oxaliplatin.
30 min, 3x/week, ~80% max HR improves DFS/OS and is cost-saving.
CRC is moving fast. The challenge now is not just knowing the data, but figuring out how to apply it thoughtfully in clinic.
Grateful to be part of the conversation.
@TheGutOncLab @Onco_Nexus @OncoAlert @TotalHealthConf


1
18
41
2,172
Thatcher Heumann retweeted

Jun 8
Just insane… this is what we mean when we say that this is just the beginning. 💯 #RASRevolution



13
30
4,848
Thatcher Heumann retweeted

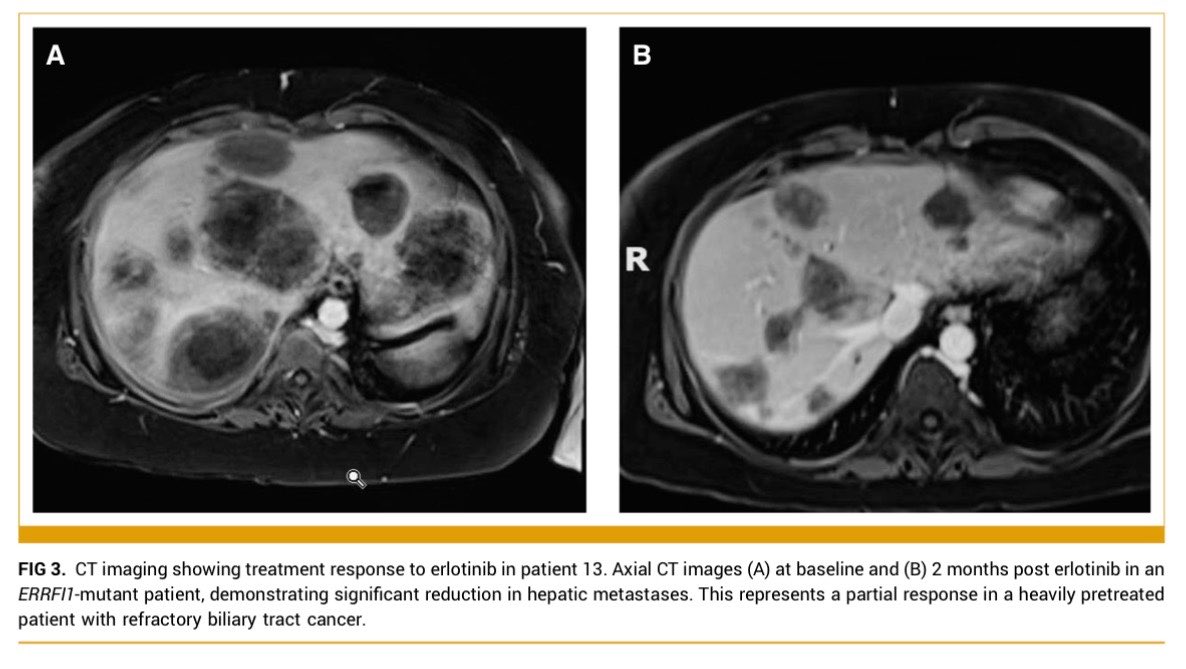
🆕@JCOPO_ASCO
💡Such a beautiful story of real world🌎 precision medicine.
Meet➡️#ERRFI1🎯
📝Time to add➕this to ACTIONABLE Biomarkers🔐for #cholanagiocarcinoma @curecc. @NCCN
👇🏽Patient in paper, I took off hospice to give Erlotinib💊.
@OncoAlert
🔗ascopubs.org/doi/10.1200/PO-…


2
18
29
4,463
Thatcher Heumann retweeted

Jun 5
Outcomes of Y90-radioembolization as downstaging to liver transplantation HCC and tumoral portal vein thrombosis
@HEP_Journal
doi.org/10.1097/HEP.00000000…
👉25% sustained downstaging after TARE
👉15% eventually LTx with good outcome
🧐Downstaging is feasible in MVI pts
@myESMO @ILCAnews @EASLnews

1
36
66
2,759
Thatcher Heumann retweeted

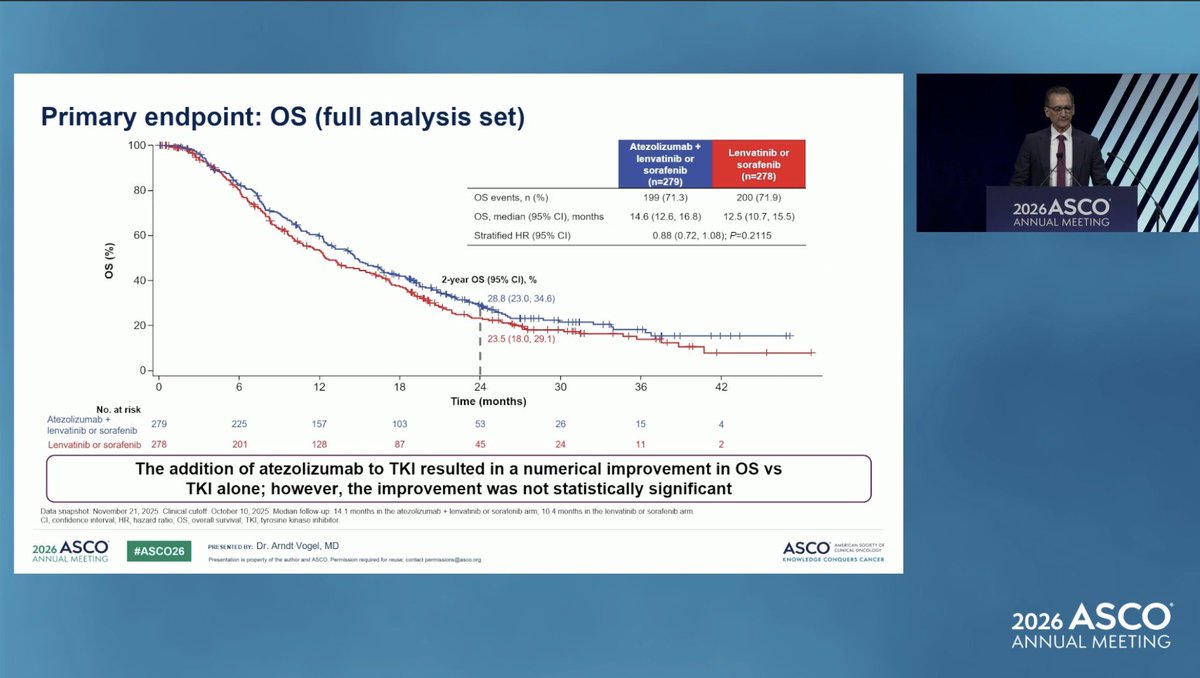
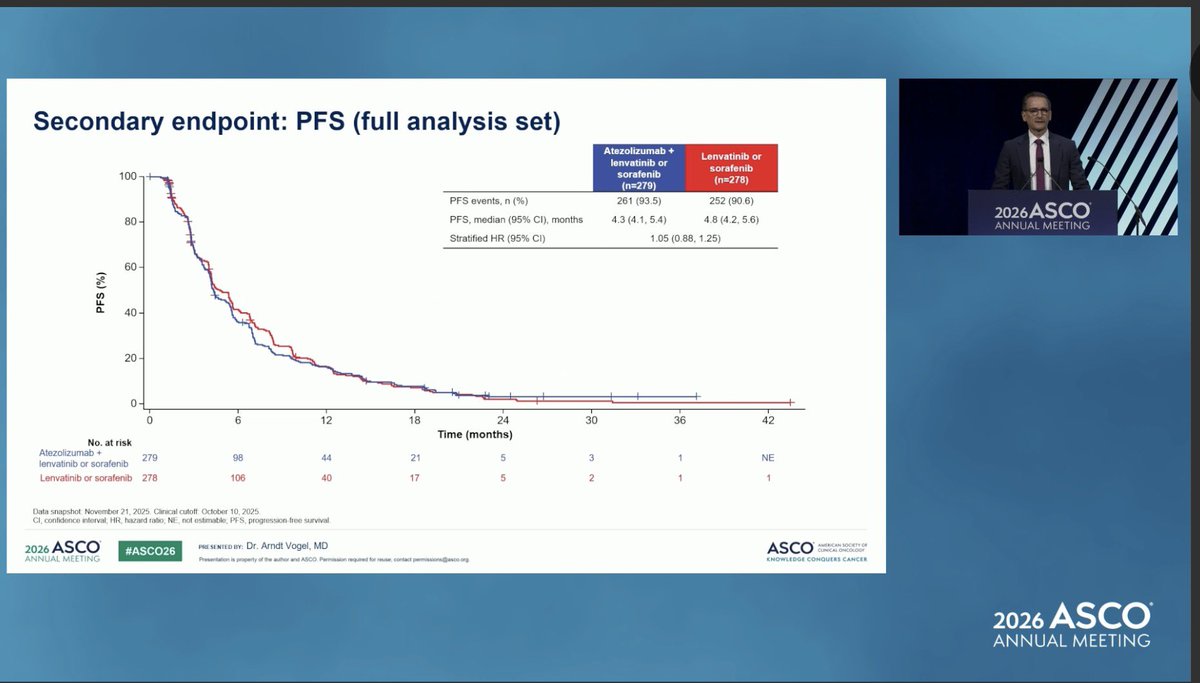
🧬 #ASCO26 | IMbrave251
Atezo lenva/sora vs lenva/sora after atezo bev
📈 OS: 14.6 vs 12.5 mo
• HR 0.88 (NS)
📈 OS from 1L atezo bev: 27.7 vs 25.6 mo, HR 0.85
📈 2-year OS: 28.8% vs 23.5%
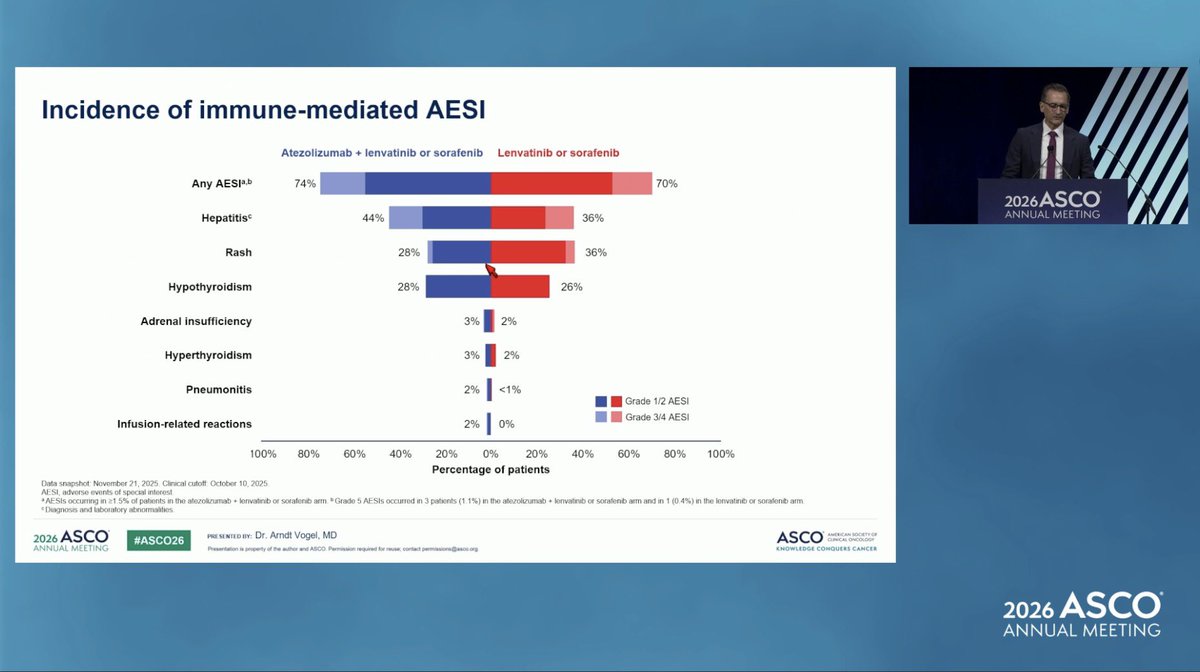
⚠️ Higher toxicity, consistent
🎯 1st phase III sequencing study after atezo bev
@OncoAlert

3
7
367

Thatcher Heumann retweeted
May 31
#ASCO26
Observation vs maintenance PD-1 after cCR in dMMR/MSI-H CRC managed nonoperatively
Abstract #3502
Presentation: May 31, 2026
This is absolutely essential data.
MSI-H CRC has rapidly evolved from aggressive and hard to treat to curable without surgery.
We are suddenly dealing with questions that would have sounded absurd a few years ago:
If a patient with dMMR/MSI-H CRC has a clinical complete response after PD-1 therapy, do we need to keep treating?
This Chinese multicenter cohort looked at exactly that.
Quick hits:
📌 Study design
318 patients with dMMR/MSI-H CRC treated with PD-1 therapy
191 achieved cCR in the presented flow 129 entered non-operative management
👀 Groups
Observation: n=66, stopped PD-1 after cCR
Maintenance: n=63, received ≥2 post-cCR PD-1 cycles
🧬 Included both rectal and colon cancer
Rectal: 58
Colon: 61
Synchronous dual primaries: 10
🔎 cCR assessment was not casual
Endoscopy imaging: 100%
Confirmatory biopsy: 80/129, 62%
Rectal cancer: DRE 100%, pelvic MRI 89.7%
⏱️ Time to cCR
Median cycles to cCR: 8 in both groups
Median treatment duration to cCR: 6 months
69.8% reached cCR within 8 cycles
93.8% reached cCR within 16 cycles
📈 3-year DFS
Observation: 96.4%
Maintenance: 98.2%
P=0.560
🙌 3-year OS
Observation: 100%
Maintenance: 98.4%
P=0.313
🔥 Consistent sensitivity analyses
Overlap-weighted 3-year DFS: 98.5% vs 99.6%
6-week landmark 3-year DFS: 96.0% vs 98.2%
⚠️ The toxicity tradeoff matters
Maintenance did not clearly improve outcomes, but continuing PD-1 means continuing exposure, cost, visits, and immune toxicity risk.
This is the kind of dataset that changes conversations in clinic.
Not definitive. But incredibly useful.
For a patient with dMMR/MSI-H CRC who achieves a high-quality cCR and is being followed closely, observation after stopping PD-1 looks very reasonable.
The remaining question is duration.
Does it depend on colon vs rectum? Localized vs metastatic? Disease burden? Quality of cCR assessment? Patient anxiety?
Almost certainly yes.
But the big message is clear:
In dMMR/MSI-H CRC with cCR after PD-1, more treatment is not automatically better.
Sometimes the win is knowing when to stop.
Plenary-worthy.
@TheGutonclab @UGrewalMD @TimothyJBrownMD @OncoAlert @Onco_Nexus @ASCO
@NazliDizman @LauraAlderMD @DVAraujoMD @DrBarbiOnc @LauraEsfeller @FunchainMD @YGaritaonaindia @DrSAHaddad @jgong15 @iandresmeraz @SakditadMD @RamilaShilpakar @RohitBanwar @lungoncdoc
12
22
1,482
Thatcher Heumann retweeted
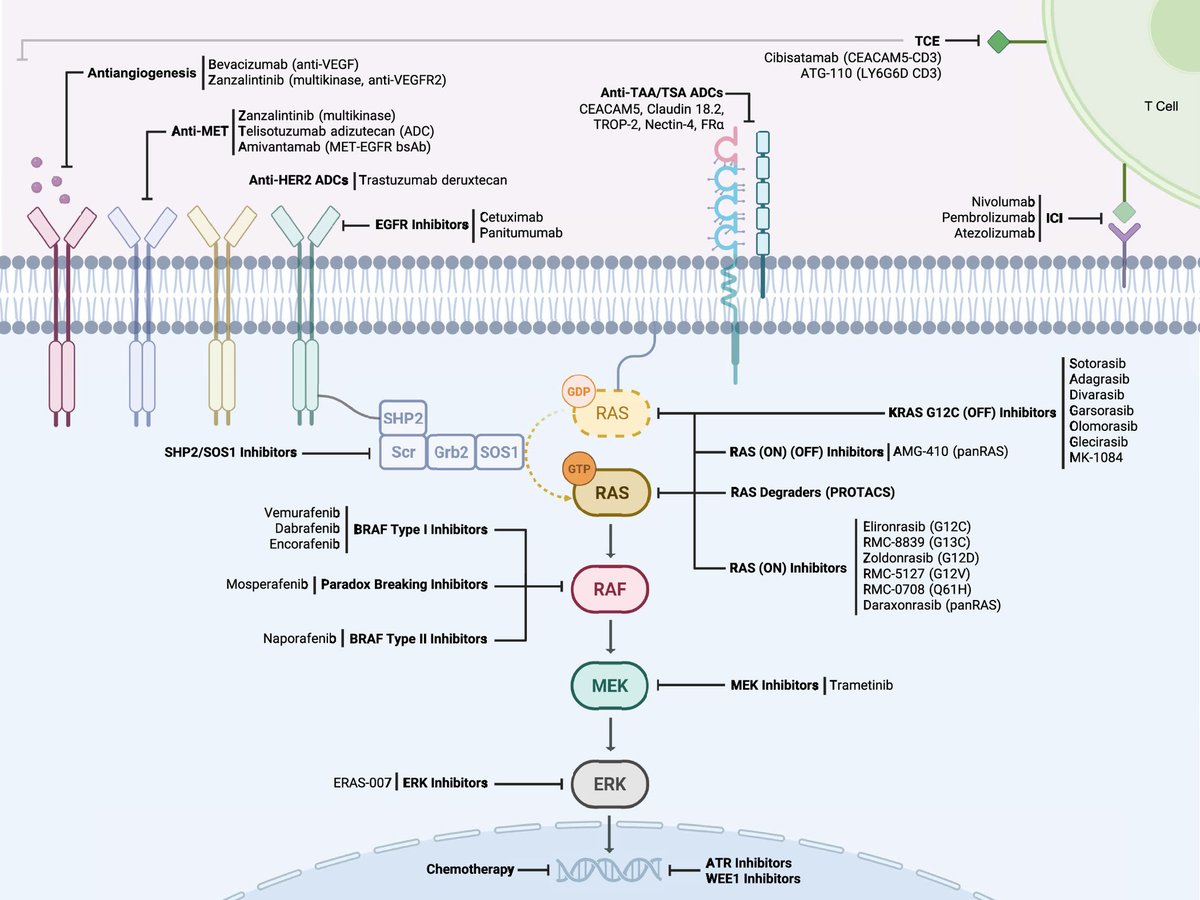
Since ras targeting is so hot right now (there’s a sentence I couldn’t have typed even a few years ago!) I thought this was a great visual of the RAS/RAF/MEK/ERK signaling pathway from the excellent @asco educational book
ascopubs.org/doi/10.1200/EDB…
#ASCO26
6
22
2,598
Thatcher Heumann retweeted
May 31
#ASCO26
This one is special.
This is the hottest paper of 2026 and potentially in the history of pancreatic cancer.
Let’s dive in.
RASolute 302: Daraxonrasib vs investigator’s choice chemotherapy in previously treated metastatic pancreatic cancer
Abstract LBA5 (soon!)
Presentation: May 31, 2026, 3:21-3:33 PM CDT
For decades, pancreatic cancer has been where good ideas go to die.
We have optimized chemotherapy. We have sequenced chemotherapy. We have celebrated modest gains.
But the central driver of PDAC has always been sitting there in plain sight:
RAS.
More than 90% of pancreatic cancers have oncogenic RAS mutations, and until recently, we had essentially nothing direct to do about it.
Daraxonrasib is an oral RAS(ON) multiselective inhibitor targeting the active GTP-bound state of mutant and wild-type RAS.
And in RASolute 302, it delivered.
Quick hits:
📌 Phase 3 international randomized trial 500 patients with previously treated mPDAC Daraxonrasib vs investigator’s choice chemotherapy
🧬 RAS G12 population
91.8% of patients had RAS G12 mutations
📈 OS in RAS G12 population
13.2 vs 6.6 months
HR 0.40
P<0.001
📈 OS in overall population
13.2 vs 6.7 months
HR 0.40
P<0.001
📊 PFS in RAS G12 population
7.3 vs 3.5 months
HR 0.45
P<0.001
📊 PFS in overall population
7.2 vs 3.6 months
HR 0.49
P<0.001
🔥 12-month OS
Overall population: 53.2% vs 17.3%
⚠️ Toxicity matters, but this was not just more efficacy for more toxicity
Grade ≥3 AEs: 61.8% vs 69.6%
TRAEs leading to discontinuation: 1.2% vs 11.2%
This is the kind of survival curve we almost never get to see in pancreatic cancer.
This validates RAS(ON) inhibition in the most RAS-addicted major cancer. It takes a target we have talked about for decades and turns it into a clinically meaningful survival benefit in a randomized phase 3 trial.
The next questions come fast: 1L combinations, maintenance, perioperative disease, sequencing, resistance, toxicity management, and whether this becomes a new backbone.
RAS is here, and it couldn’t have come sooner.
nejm.org/doi/full/10.1056/NE…
@TheGutonclab @UGrewalMD @TimothyJBrownMD @OncoAlert @Onco_Nexus @ASCO
@NazliDizman @LauraAlderMD @DVAraujoMD @DrBarbiOnc @LauraEsfeller @FunchainMD @YGaritaonaindia @DrSAHaddad @jgong15 @iandresmeraz @SakditadMD @RamilaShilpakar @RohitBanwar @lungoncdoc

12
269
911
85,214
Thatcher Heumann retweeted
1
8
26
3,223
Thatcher Heumann retweeted
May 31
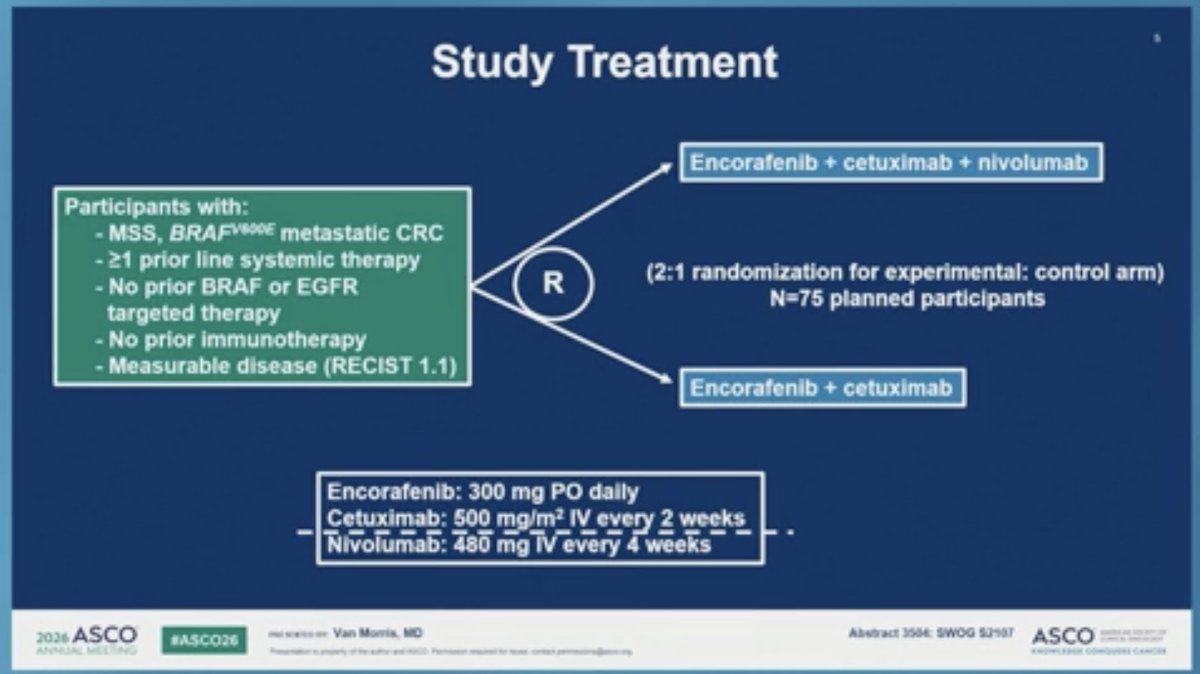
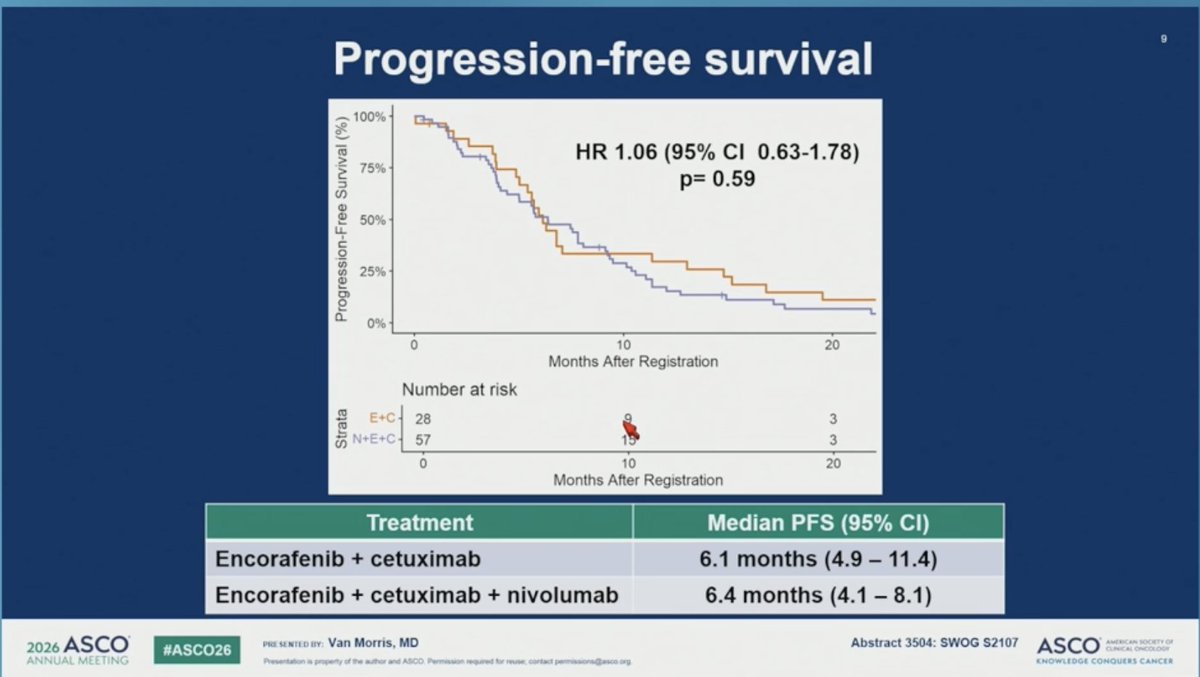
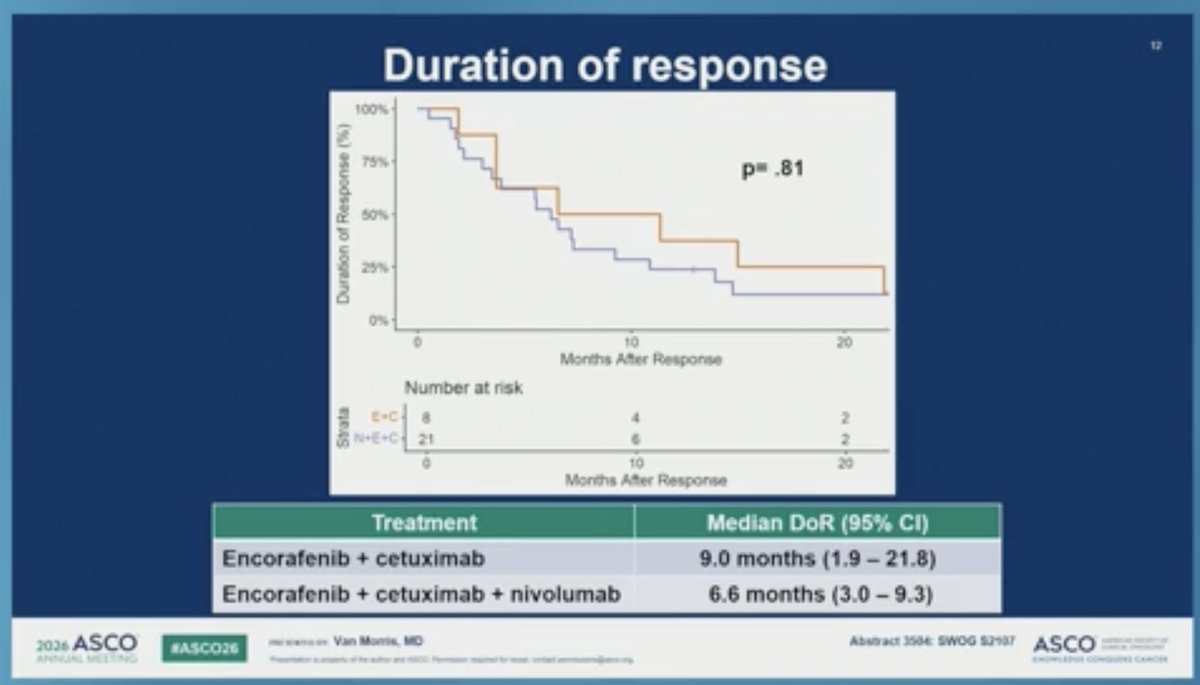
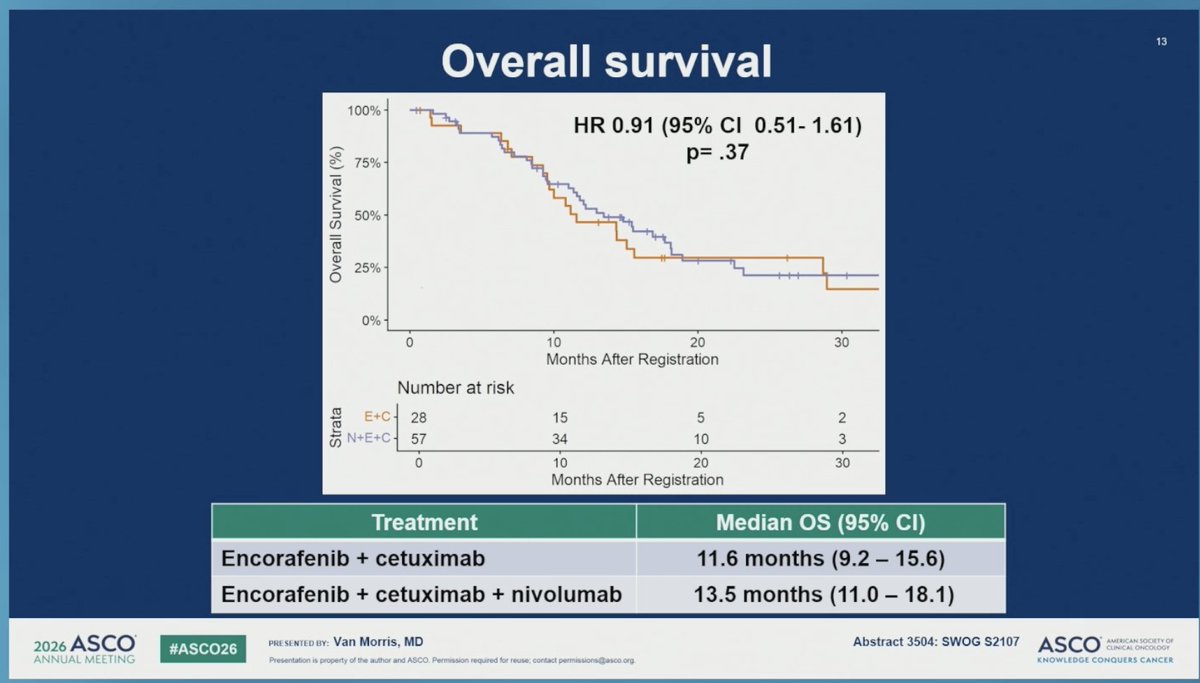
SWOG S2107: Randomized ps II trial of encorafenib and cetuximab with or without nivolumab for patients with previously treated MSS, BRAFV600E mCRC
#ASCO26
👉mPFS 6.1 vs 6.4 mo
👉mOS 11.6 vs 13.5 mo
🧐negative study, no benefit for adding ICI in 2nd line
@myesmo @ASCO
7
16
1,106
Thatcher Heumann retweeted

May 29
The OncoAlert🚨 GI faculty’s TOP 10 abstracts In GI Oncology for #ASCO26 are here — selected by our leads and finalized through a Delphi voting process with our senior experts across #ColorectalCancer #ColonCancer #LiverCancer #PancreaticCancer and more
A snapshot of what will shape GI oncology at #ASCO26 👇
🚨 OncoAlert Top 10 — #GIcancer at #ASCO26
1️⃣ LBA5 | RASOLUTE 302 — Daraxonrasib vs chemo in previously treated metastatic pancreatic adenocarcinoma
2️⃣ #4017 | FIGHT-302 — Pemigatinib in untreated unresectable/metastatic FGFR2-rearranged cholangiocarcinoma (Ph3)
3️⃣ LBA4000 | EMERALD-3 — Tremelimumab durvalumab lenvatinib TACE in unresectable HCC (Ph3)
4️⃣ #3506 | PUMP Trial — Adjuvant HAIP floxuridine in resectable colorectal liver metastases
5️⃣ LBA3500 | CIRCULATE — ctDNA-guided adjuvant therapy in Stage II colon cancer
6️⃣ LBA3503 | BREAKWATER — Encorafenib cetuximab FOLFIRI as 1L in BRAF V600E mCRC (Ph3)
7️⃣ LBA3508 | EPISODE-III — Adjuvant aspirin vs placebo in Stage III CRC post-resection (Ph3)
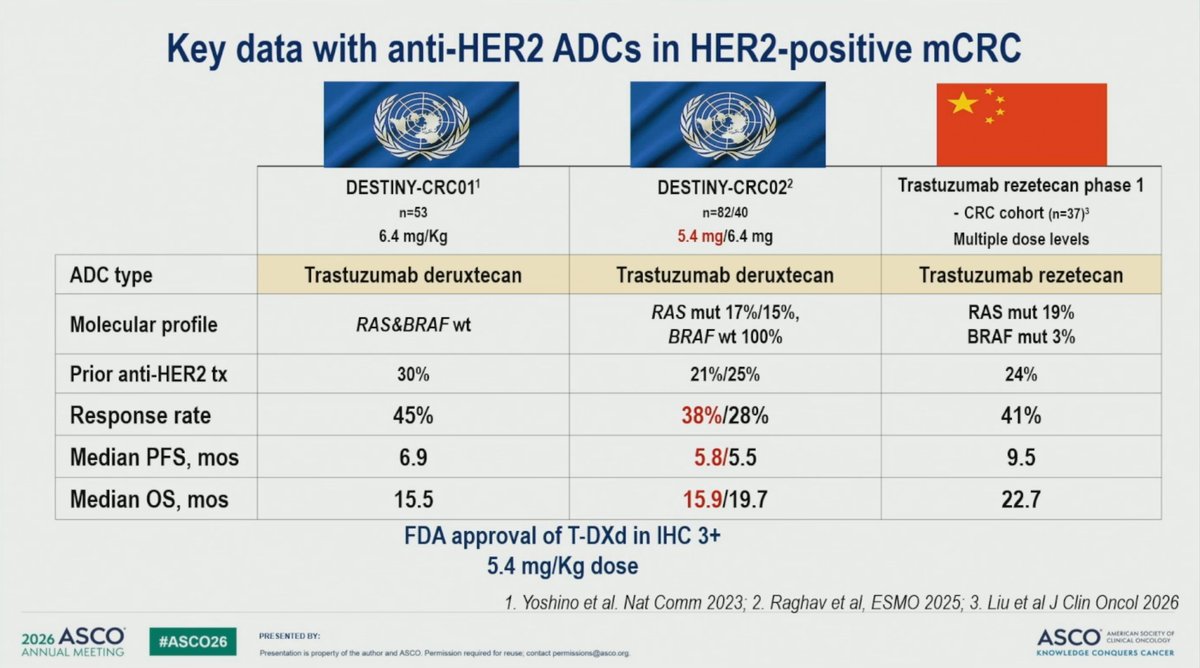
8️⃣ #3505 — Trastuzumab rezetecan vs SOC in chemo-refractory HER2 advanced CRC (Ph3)
9️⃣ #4006 | ATTRACTION-6 — Nivo ipi chemo as 1L in HER2− advanced gastric/GEJ cancer
🔟 #3504 | SWOG S2107 — Encorafenib cetuximab nivo in MSS BRAF V600E mCRC (Ph2)
Leads
@realbowtiedoc
@p_ciracimd
@WeOncologists
Senior faculty
@CathyEngMD @ARosen380 @GillSharlene @BenWestphalen @graokane
Participating AF
@DrVilmaPBarcia @Erman_Akkus @GIMedOnc

19
23
7,107
Thatcher Heumann retweeted
May 18
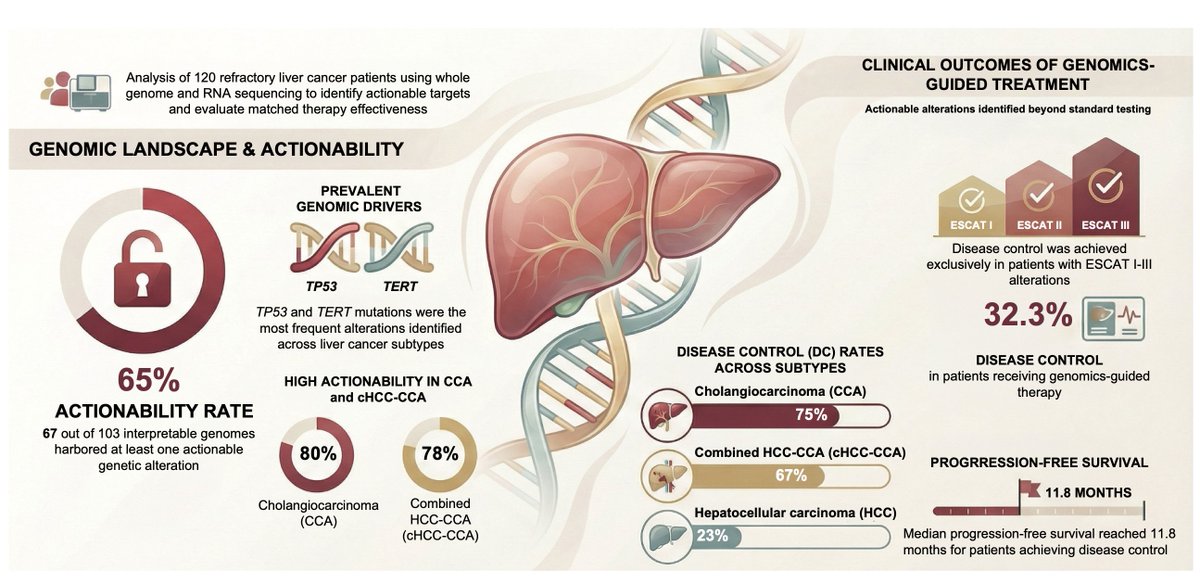
Molecularly guided therapies for advanced primary liver cancers refractory to systemic treatment: Results from the 2025 French genomic medicine initiative
@JHepatology
doi.org/10.1016/j.jhep.2026.…
👉Integrating WGS, WES and RNAseq key to identify actionable genomic alterations
@myESMO @EASLedu @ILCAnews
1
28
50
3,640
Thatcher Heumann retweeted
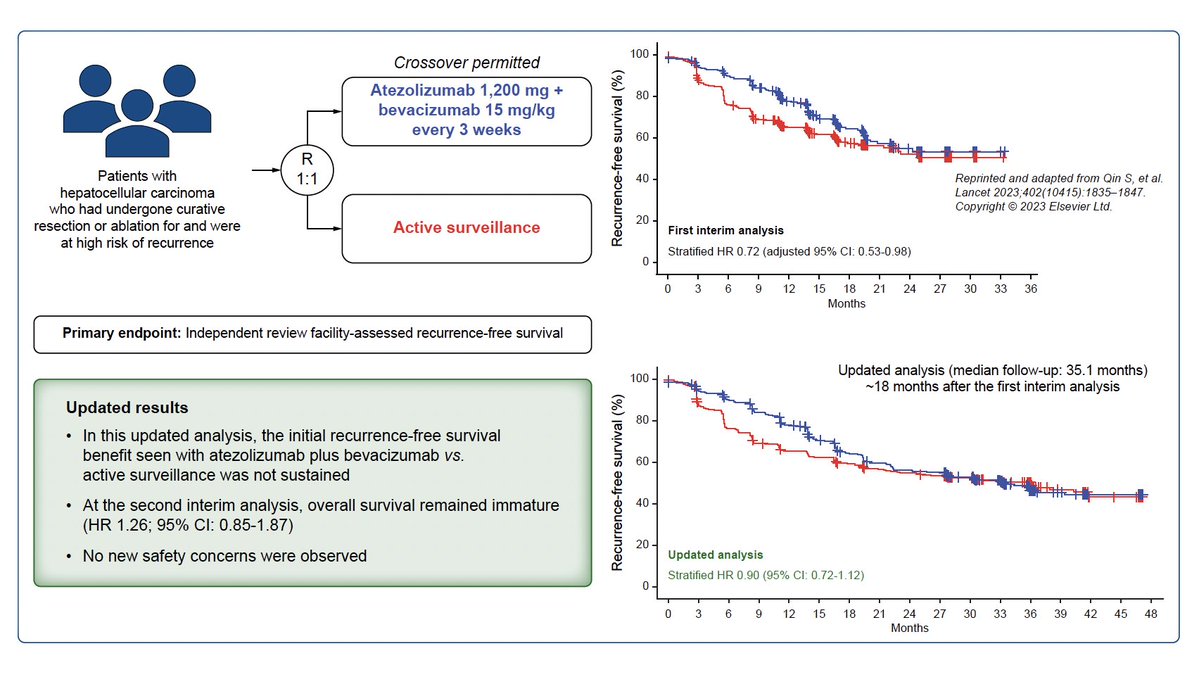
May 18
Updated data from IMbrave050: Adjuvant atezolizumab plus bevacizumab for high-risk hepatocellular carcinoma
@JHepatology
doi.org/10.1016/j.jhep.2026.…
👉Disappointing, we need to do better...
@myESMO @EASLedu @ILCAnews
1
43
82
5,962
Thatcher Heumann retweeted

#ASCO26 is coming soon. Below are the seven GI cancer abstracts that could change the current standard of care if results are positive. Stay tuned.
@ASCO @jgong15 @RevMedicines @SWOG @VanMorrisMD @skopetz @ArndtVogel @GIcancerDoc @ProvSwedish #Daraxonrasib #Pemigatinib #colorectalcancer #HCC #BTC #cholangiocarcinoma #pancreaticcancer #PDAC @curecc

18
32
2,415
Thatcher Heumann retweeted

May 16
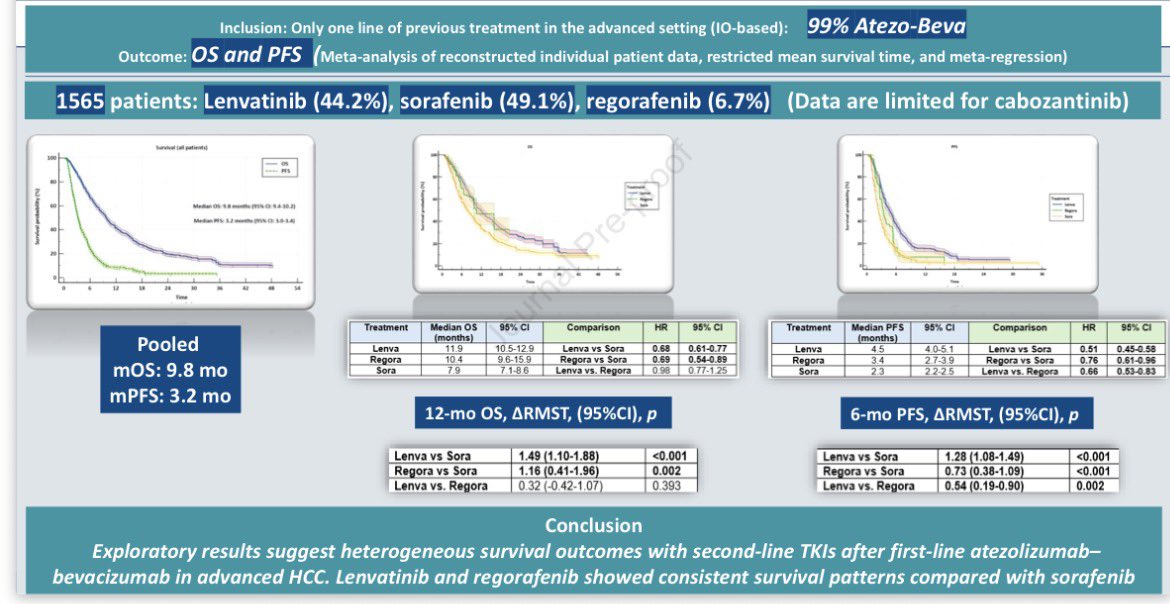
🔵Second-Line TKIs after 1L IO-based Treatment in Advanced HCC
@JHEP_Reports
➡️Our reconstructed IPD meta-analysis
➡️Mainly after atezo-bev
🚨Sorafenib seem to be less effective than lenvatinib and regorafenib
✅Lenvatinib seem to have better efficacy
❓Cabozantinib may be promosing, but needs more data
⚠️Results are exploratory, prospective trials are needed
👉doi.org/10.1016/j.jhepr.2026…
🙏Many thanks to all co-authors and mentors, especially Dr. Bouattour
#cancer #oncology #liver #hcc #hepatocellular #MedX @OncoAlert

1
22
41
5,944
Thatcher Heumann retweeted

May 12
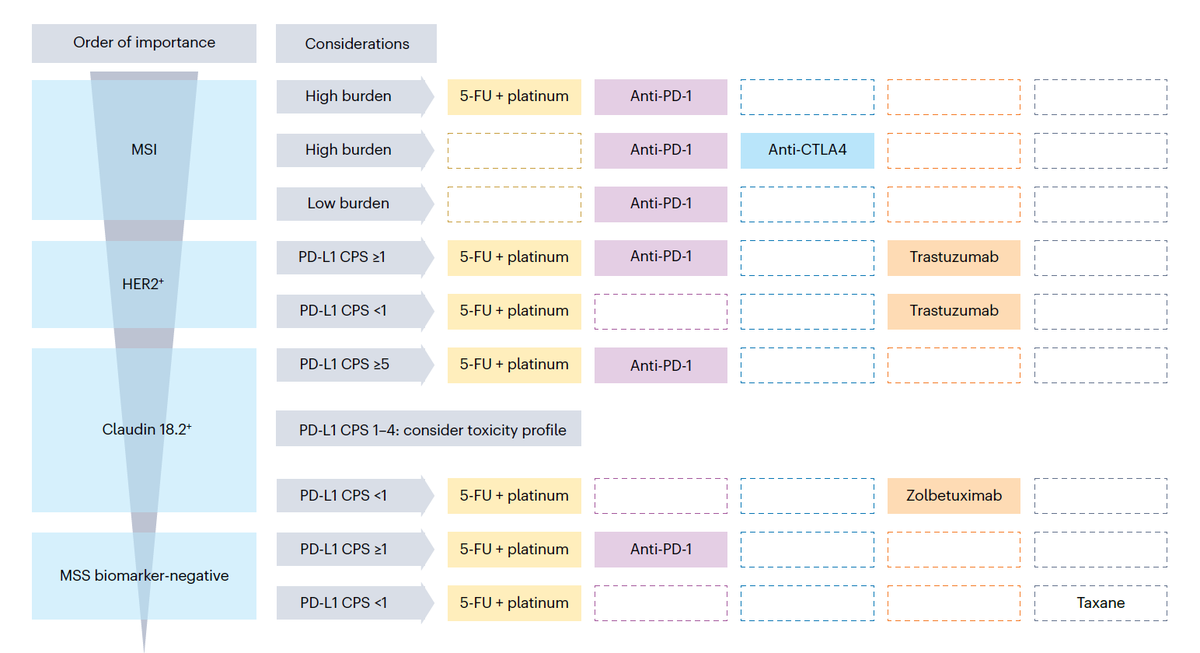
This is an absolutely outstanding review on the management of patients with metastatic gastric cancer.
I may have posted about this review before but it is so good that it deserves another round of applause... Thanks @KlempnerSam @YJanjigianMD @amalsargsyan and all the other co-authors I could not find on X...
Sorry AI, I love you but you are just not there yet. True content experts writing a practical review still beat you easily.
This should be a required read for all who take care of patients with gastric cancer.
nature.com/articles/s41571-0…
3
36
95
6,866
Thatcher Heumann retweeted

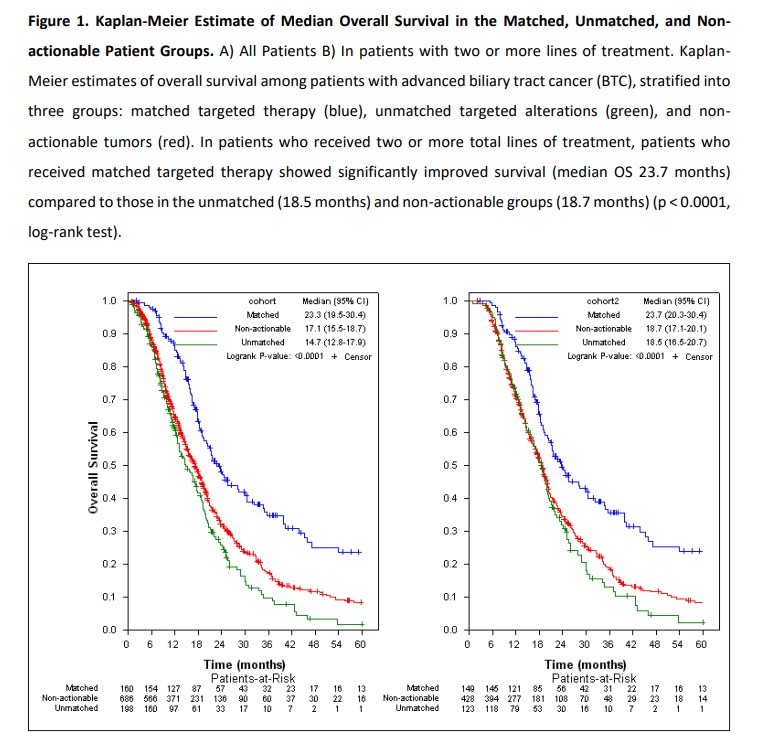
The message in advanced biliary tract cancers is becoming increasingly clear:
NGS should no longer be viewed as an approach reserved only for later lines of treatment.
In this large international cohort (1049 patients):
* Matched targeted therapy achieved a median OS of 23.3 months
* Patients with actionable alterations who did not receive matched therapy had the worst outcomes
* Nearly 45% of patients may never reach second-line treatment
Most common actionable alterations:
* BRCA1/2
* FGFR2 fusion
* HER2 amplification
* IDH1 mutation
One particularly striking point:
Although BRCA1/2 alterations were among the most common actionable findings in this study, they are still not sufficiently emphasized in some routine BTC testing algorithms and guidelines.
Liquid biopsy appears promising, but especially for FGFR2 fusions and HER2 amplifications, it still cannot fully replace tissue-based testing.
In advanced biliary tract cancers, precision oncology is no longer becoming “optional” — it is becoming essential.
nature.com/articles/s41698-0…
@oncodaily @OncBrothers @ilyassahinMD @Nature @tompowles1
2
19
61
4,395